Embed Size (px)
Citation preview

Urine Volume and Change in Estimated GFR in aCommunity-Based Cohort StudyWilliam F. Clark,*† Jessica M. Sontrop,*†‡ Jennifer J. Macnab,‡ Rita S. Suri,*† Louise Moist,*†‡ Marina Salvadori,§ andAmit X. Garg*†‡
SummaryBackground and objectives The effect of increased fluid intake on kidney function is unclear. This studyevaluates the relationship between urine volume and renal decline over 6 years in a large community-basedcohort.
Design, setting, participants, & measurements This prospective cohort study was undertaken in Canadafrom 2002 to 2008. We obtained 24-hour urine samples from adult participants with an estimated GFR(eGFR) �60ml/min per 1.73 m2 at study entry. Percentage annual change in eGFR from baseline was cate-gorized as average decline �1% per year, between 1% and 4.9% (mild-to-moderate decline) or �5% (rapiddecline).
Results 2148 participants provided valid 24-hour urine samples, grouped as �1 L/d (14.5%); 1 to 1.9 L/d(51.5%); 2 to 2.9 L/d (26.3%); and �3 L/d (7.7%). Baseline eGFR for each category of urine volume was 90,88, 84, and 87 ml/min per 1.73 m2, respectively. Overall, eGFR declined by 1% per year, with 10% demon-strating rapid decline and 40% demonstrating mild-to-moderate decline. An inverse, graded relationshipwas evident between urine volume and eGFR decline: For each increasing category of 24-hour urine vol-ume, percentage annual eGFR decline was progressively slower, from 1.3%, 1.0%, 0.8%, to 0.5%, respec-tively; P � 0.02. Compared with those with urine volume 1 to 1.9 L/d, those with urine volume �3 L/dwere significantly less likely to demonstrate mild-to-moderate decline (adjusted odds ratio 0.66; 95% confi-dence interval 0.46 to 0.94) or rapid decline (adjusted odds ratio 0.46; 95% confidence interval 0.23 to 0.92);adjusted for age, gender, baseline eGFR, medication use for hypertension (including diuretics), proteinuria,diabetes, and cardiovascular disease.
Conclusions In this community-based cohort, decline in kidney function was significantly slower in thosewith higher versus lower urine volume.
Clin J Am Soc Nephrol 6: 2634–2641, 2011. doi: 10.2215/CJN.01990211
IntroductionThe message to drink “at least 8 glasses of water aday” is widespread, despite a lack of evidence tosupport it (1– 4). Two major medical journals, theBritish Medical Journal and The Lancet, rightly de-scribe this “fluid craze” as a medical myth propa-gated by the popular press (1,5). Aside from pre-venting kidney stone formation (6,7), few studieshave demonstrated a beneficial effect of increasedfluid intake in adequately hydrated individuals(3,4). Previous research evaluating the relationshipbetween fluid intake and kidney function has pro-duced equivocal results; however, much of this re-search was conducted in animal models (8) or wasrestricted to patients with chronic kidney disease(CKD) (9). To date, no study has prospectively ex-amined the effect of urine volume on kidney func-tion in the general population. The WalkertonHealth Study, a prospective community-based co-
hort study, provided a unique opportunity to eval-uate the relationship between urine volume andrenal decline over 7 years of follow-up.
Materials and MethodsParticipants and Study Design
Participants were from the Walkerton Health Study(2002 to 2008, Canada), a prospective cohort studyevaluating the long-term health sequelae from expo-sure to water contaminated with Escherichia coli O157and Campylobacter. The design and methodology ofthe Walkerton Health Study are described elsewhere(10). Briefly, residents of the Walkerton area wereinvited to participate in the study and attend an an-nual clinic, irrespective of whether they had beenexposed to contaminated water or developed an acuteillness. The study sample has previously been shownto be representative of the target population (11).Written consent was obtained from all participants.
*Division ofNephrology,Department ofMedicine, LondonHealth Sciences Centre,London, Ontario,Canada; †LondonKidney ClinicalResearch Unit, LondonHealth Sciences Centre,London, Ontario,Canada; ‡Departmentof Epidemiology &Biostatistics, Universityof Western Ontario,London, Ontario,Canada; and§Department ofPediatric InfectiousDiseases, Children’sHospital, LondonHealth Sciences Centre,London, Ontario,Canada
Correspondence:Dr. William F. Clark,Victoria Hospital, RoomA2-343, 800Commissioner’s RoadEast, London ON,Canada N6A 5W9.Phone: 519-685-8361;Fax: 519-685-8047;E-mail: [email protected]
2634 Copyright © 2011 by the American Society of Nephrology www.cjasn.org Vol 6 November, 2011
Article

Ethics approval was obtained from the University of West-ern Ontario’s Research Ethics Board for Health Sciences.The present analysis was limited to adult participants �18years who joined the study in 2002 or 2003 (n � 3154),provided a valid 24-hour urine samples at study entry, hadan estimated GFR (eGFR) �60 ml/min per 1.73 m2 atbaseline, and had at least two annual eGFR assessments.
MeasuresParticipants attended an annual clinic and completed a
computer-assisted in-person interview that included ques-tions on family history, past and current medication use,risk factors, and several physician-diagnosed health con-ditions, including diabetes and cardiovascular disease.Questionnaire development was guided by the U.S. ThirdNational Health and Nutrition Survey (NHANES III) andStatistics Canada’s National Population Health Survey.Height and weight were measured by trained study per-sonnel.
Serum creatinine was assessed annually and eGFR wascalculated using the abbreviated Modification of Diet inRenal Disease equation (12). Participants provided a 24-hour urine sample at study entry and again at years 5 and7. Under- or overcollection of 24-hour urine samples wereidentified if 24-hour urine creatinine was less than orgreater than the laboratory’s reference range (7 to 25mmol/d). Serum and urine creatinine were measured bythe modified kinetic method of Jaffe using the Vitros 950autoanalyzer (interassay coefficient of variation �4%)(Johnson and Johnson, Skillman, NJ). Based on evidencethat 24-hour urine protein was systematically overesti-mated in samples with higher urine volumes (13), protein-uria was measured using a urine dipstick (Bayer 8SG Mul-tistix) from a random spot urine sample obtained at studyentry. In 2003, participants were offered an 8-hour fastingplasma glucose test and an oral glucose tolerance test(OGTT), if fasting glucose was 5.5 to 6.9 mmol/L, to in-crease the sensitivity of detecting diabetes.
DefinitionsParticipants were grouped into four categories of urine
volume based on values at study entry (�1 L/d, 1 to 1.9L/d, 2 to 2.9 L/d, and �3 L/d) (14). To calculate the rate ofchange in kidney function over time, we fitted an ordinaryleast-squares regression line to all eGFR measures for eachparticipant. The slope of the regression line describes therate of change in kidney function (eGFR) over time. Whilethe distribution of the absolute annual change was stronglyskewed to the right and susceptible to highly variable ratesof annual decline in those with eGFR �90 ml/min per 1.73m2, the distribution of percentage annual change ([slope/baseline eGFR]�100) was more symmetrically balancedaround the median. Therefore, for our primary analysis,we defined change in renal function as percentage annualchange in eGFR from baseline, categorized as average de-cline �1% per year (reference), between 1% and 4.9% peryear (mild-to-moderate decline), or �5% (rapid decline)(15,16). Cardiovascular disease was defined as a self-re-ported, doctor-diagnosed heart attack, stroke, or conges-tive heart failure. Diabetes mellitus was defined using thecurrent diagnostic criteria based on the presence of fasting
plasma glucose �7.0 mmol/L, random or 2-hour postOGTT plasma glucose �11.1 mmol/L, a medical diagnosisof diabetes, and/or the use of oral hypoglycemic agents orinsulin (17).
Statistical AnalysesNormally distributed data were summarized by the
mean and standard deviation (SD), and skewed distribu-tions by the median and interquartile range (IQR). Bivari-able associations were assessed using the chi-squared test,ANOVA, or the Kruskal–Wallis test, as appropriate. Weperformed a multiple linear regression to compare renaldecline across categories of urine volume while adjustingfor confounders. We performed a multinomial logistic re-gression to estimate odds ratios (ORs) and 95% confidenceintervals (CIs) for rapid decline and mild-to-moderate re-nal decline. The reference category for all analyses wasurine volume 1 to 1.9 L/d, which contained the medianvalue for the population. Age and gender were included inall models. Possible confounders considered for statisticaladjustment included medication use for hypertension andrisk factors for renal progression, including dipstick pro-teinuria (missing for 31), cardiovascular disease, diabetes,smoking, obese body mass index at study entry (�30 kg/m2), and family history of hypertension (missing for 5),diabetes (missing for 2), or kidney failure (missing for 1).Information on risk factors was collected from multiplesources, and in the absence of any evidence, missing dataon risk factors was set to zero (absent), which producedsimilar or more conservative results than a complete caseanalysis. Models were reduced using backward elimina-tion at alpha � 0.15 (18,19) unless elimination changed theexposure-outcome association by �10% (19,20). Modelswere run with and without outliers, with no appreciableeffect on results. To assess the potential impact of informa-tion bias from differential follow-up times, we examinedthe change in risk when (1) follow-up time was enteredinto the model, and (2) number of annual eGFR assess-ments was entered into the model. In addition, we exam-ined whether the main results differed when renal declinewas defined using a minimum of three versus two annualeGFR assessments. Additional sensitivity analyses wererun to confirm that results were robust to differing variabledefinitions and modeling techniques.
ResultsOf 3371 participants �18 years, 2148 provided valid
24-hour urine samples at study entry and had at least twoannual eGFR assessments (Figure 1). Participants were56% female, with an average age of 46 years. At baseline,median urine volume was 1.8 L/d (IQR 1.2 to 2.2) andmean eGFR was 87 ml/min per 1.73 m2. Participants re-ceived a median of 6 (IQR 4 to 7) annual eGFR assessments,and 82% received at least four annual assessments. Partic-ipant characteristics overall, and by 24-hour urine volume,are shown in Table 1. Those with higher urine volumestended to be older and were more likely to be obese,smokers, or taking medication for hypertension, whichincluded diuretics. Baseline eGFR for each category ofurine volume (�1 L/d, 1 to 1.9 L/d, 2 to 2.9 L/d, and �3L/d) was 90, 88, 84, and 87 ml/min per 1.73 m2, respec-
Clin J Am Soc Nephrol 6: 2634–2641, November, 2011 Urine Volume and Renal Decline, Clark et al. 2635

tively. The median number of annual eGFR assessments (6)was similar across categories of urine volume.
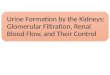
The annual change in eGFR was �0.83 ml/min per1.73m2/yr (�0.81 ml/min per 1.73m2/yr for men and�0.84 ml/min per 1.73m2/yr for women). The annualizedchange in reciprocal serum creatinine was �0.005 (mg/dl)�1 per yr (�0.004 (mg/dl)�1 per yr for males and�0.006 (mg/dl)�1 per yr for females). Overall, eGFR de-clined by 1.0% per year, with 10% demonstrating rapiddecline (eGFR decline �5%) and 40% demonstrating mild-to-moderate decline (eGFR decline between 1% and 4.9%).The difference in eGFR between the first and last assess-ment was 5.1 ml/min per 1.73 m2, and eGFR fell below 60ml/min per 1.73 m2 for 9.6% of participants. Despite hav-ing similar levels of renal function at baseline (87 ml/minper 1.73 m2), eGFR fell below 60 ml/min per 1.73 m2 fortwice as many participants with urine volume �3 L/dcompared with those with urine volume �3 L/d (10.0%versus 5.5%; P � 0.07). An inverse, graded relationship wasevident between urine volume and renal decline: For eachincreasing category of 24-hour urine volume (�1 L/d, 1 to1.9 L/d, 2 to 2.9 L/d, and �3 L/d), percentage annualdecline in eGFR was progressively slower (1.3%, 1.0%,0.8%, and 0.5%, respectively; P � 0.02). A similar patternwas seen for reciprocal serum creatinine, where the annu-alized change was: �0.007, �0.006, �0.005, �0.002 (mg/dl)�1 per yr, respectively, P � 0.06. In terms of absoluteeGFR decline, Figure 2 shows the difference in eGFR be-tween the first and last assessment (median 5.7 years); thedecrease in eGFR was nearly three times greater in thosewith the lowest versus highest urine volumes: 6.4 ml/minper 1.73 m2 versus 2.3 ml/min per 1.73 m2; P � 0.01. Theincrease in serum creatinine between the first and last
assessment showed a similar pattern, with the increasebecoming progressively smaller across increasing catego-ries of urine volume: 0.03 mg/dl, 0.03 mg/dl, 0.02 mg/dl,and 0.01 mg/dl; respectively; P � 0.04. Overall, the age-and gender-adjusted average annual eGFR decline was 0.6ml/min per 1.73 m2/yr slower in those with urine volume�3 L/d compared with those with smaller urine volumes(P � 0.01). As shown in Table 2, percentage annual declinein eGFR remained significantly slower in adults with urinevolume �3 L/d compared with those in the referencecategory (1 to 1.9 L/d) after adjusting for age, gender,medication use for hypertension, dipstick protein, and car-diovascular disease (difference � 0.9%/yr; P � 0.02).
As shown in Table 3 and Figure 3, an inverse, gradedrelationship was evident between urine volume and therisk for mild-to-moderate and rapid renal decline. Com-pared with those with urine volume 1 to 1.9 L/d, thosewith urine volume �3 L/d were significantly less likely todemonstrate mild-to-moderate renal decline (adjustedOR � 0.66; 95% CI 0.46 to 0.94; P � 0.02) or rapid decline(adjusted OR � 0.46; 95% CI 0.23 to 0.92; P � 0.03).
Sensitivity AnalysesResults of the regression analyses did not change after
controlling for number of eGFR assessments, follow-uptime, baseline eGFR, diabetes, and urine creatinine, orwhen renal decline was modeled as absolute versus per-centage change or as the inverse of serum creatinine.Change in measured creatinine clearance between first andlast assessment did not significantly associate with urinevolume; however, measurement of serum creatinine wasnot timed to the 24-hour urine collection and thereforecannot be assumed to reflect the true clearance. When we
Figure 1. | Flow of participants from recruitment to analysis.
2636 Clinical Journal of the American Society of Nephrology

restricted the analysis to those with a minimum of threeannual eGFR assessments (n � 1865) and sustained poly-uria (urine volume �3 L/d for at least two annual assess-ments; n � 95), percentage annual decline in eGFR was0.6%/yr slower in those with sustained polyuria (P �0.047). When 24-hour urine volume was averaged over thethree follow-up assessments (intraclass correlation coeffi-cient: 0.78; P � 0.001), the inverse relationship betweenaveraged urine volume and renal decline remained thesame; however, polyuria lost statistical significance (differ-ence � 0.5%/yr; P � 0.28), and renal decline for those withthe smallest urine volumes (�1 L/d) was significantlyfaster (difference � �0.7%/yr; P � 0.04) compared withthe reference group (urine volume 1 to 1.9 L/d).
DiscussionIn this prospective, community-based cohort study of
adults with normal kidney function, decline in kidneyfunction was significantly slower in those with higher ver-sus lower urine volumes. The age- and gender-adjustedaverage annual decline in eGFR was 0.6 ml/min per 1.73m2/yr slower for those with urine volume �3 L/d com-pared with those with smaller urine volumes. Over 10
years, this translates into a difference of 6 ml/min per 1.73m2. The fastest rate of decline was observed for those withthe smallest urine volumes (�1 L/d). Those with the larg-est urine volumes (�3 L/d) were least likely to demon-strate mild-to-moderate renal decline or rapid decline. Theinverse, graded relationship between urine volume andrenal decline remained significant after controlling for age,gender, baseline eGFR, medication use for hypertension(including diuretics), dipstick proteinuria, diabetes, andcardiovascular disease.
Our findings are consistent with Strippoli et al., whorecently reported a protective effect of higher self-reportedfluid intake on kidney function in a large community-based cohort (21). These findings contrast with earlierstudies showing no association or possible harm of greaterfluid intake; however, much of this research was con-ducted in animal models (8) or CKD patients (9). In anobservational study of CKD patients, higher urine volumeand low urine osmolality were associated with faster de-cline in renal function (9). However, this association maybe explained, in part, by greater diuretic use among thosewith higher urine volumes and the decreased ability of thekidneys to concentrate urine as function declines; and,
Table 1. Characteristics of participants, overall and by 24-hour urine volume at baseline
Overall(n � 2148)
24-hour Urine Volume
Pa
�1 L (n � 312) 1 to 1.9 L(n � 1107)
2 to 2.9 L(n � 564)
�3 L(n � 165)
Female gender 1207 (56.2%) 182 (58.3%) 607 (54.8%) 328 (58.2%) 90 (54.5%) 0.48Age at entry (years),
mean (SD)46.3 (15.0) 39.2 (14.5) 46.0 (15.3) 50.2 (13.6) 48.4 (13.9) �0.001
Age at last follow-up(years), mean (SD)
51.5 (15.3) 44.3 (14.7) 51.2 (15.6) 55.6 (13.9) 53.9 (14.0) �0.001
Years followed, median(IQR)
5.7 (3.9, 6.0) 5.6 (3.8, 6.0) 5.7 (3.8, 6.0) 5.8 (4.1, 6.0) 5.8 (4.3, 6.1) 0.001
Number of eGFRassessments, median(IQR)
6.0 (4, 7) 6 (4, 7) 6 (4, 7) 6 (5, 7) 7 (5, 7) 0.001
24-hour urine volume(L), median (IQR)
1.8 (1.2, 2.2) 0.8 (0.65, 0.9) 1.4 (1.2, 1.7) 2.3 (2.2, 2.6) 3.3 (3.1, 3.8) �0.001
eGFR ml/min per1.73 m2, mean (SD)
86.9 (15.2) 90.3 (15.5) 87.6 (15.6) 83.8 (14.1) 86.5 (13.9) �0.001
Serum creatinine(mg/dl), mean (SD)
0.88 (0.15) 0.88 (0.15) 0.88 (0.15) 0.89 (0.14) 0.88 (0.14) 0.61
Dipstick protein �1 g/L 41 (1.9%) 9 (2.9%) 18 (1.6%) 11 (2.0%) 3 (1.8%) 0.02Obese (BMI �30 kg/m2) 783 (36.5%) 97 (31.1%) 402 (36.3%) 214 (37.9%) 70 (42.4%) 0.07Family history
hypertension 955 (44.5%) 128 (41.0%) 492 (44.4%) 255 (45.2%) 80 (48.5%) 0.44kidney failure 52 (2.4%) 10 (3.2%) 21 (1.9%) 13 (2.3%) 8 (4.8%) 0.10diabetes 584 (27.2%) 68 (21.8%) 311 (28.1%) 162 (28.7%) 43 (26.1%) 0.12
Smoker 970 (45.2%) 113 (36.2%) 502 (45.3%) 271 (48.0%) 84 (50.9%) 0.003Medications for
hypertension(including diuretics)
601 (28.0%) 50 (16.0%) 306 (27.6%) 189 (33.5%) 56 (33.9%) �0.001
Diabetes 270 (12.6%) 31 (9.9%) 132 (11.9%) 83 (14.7%) 24 (14.5%) 0.15Cardiovascular disease 175 (8.1%) 15 (4.8%) 92 (8.3%) 57 (10.1%) 11 (6.7%) 0.05
Values are numbers (percentages) unless stated otherwise (n � 2148). IQR, interquartile range; eGFR, estimated GFR; BMI, body massindex.aVariables were compared using the chi-squared test, analysis of variance, or the Kruskal-Wallis test, as appropriate.
Clin J Am Soc Nephrol 6: 2634–2641, November, 2011 Urine Volume and Renal Decline, Clark et al. 2637

thus, in CKD patients, high urine volume with low osmo-lality could be the result, not the cause, of faster decline(9,22). Evidence supporting the latter conclusion is pro-vided by highly controlled studies in rats in which highhydration shows a persistent benefit in preserving renalfunction (8,22–25). Furthermore, an experimental studythat randomized elderly men to increase fluid intake sawno change in eGFR over a 6-month follow-up (26), al-though a longer follow-up may be necessary to discern anappreciable effect on kidney function. In two small studiesof acute water loading in healthy adults, a transient in-
crease in albumin excretion was observed in one (27), andthe other showed that the effect of fluid loading on GFRwas dependent on whether participants had consumed ahigh-protein meal or were in a fasting state (28). Anastasioet al. underlined the acute nature of these experiments,which cannot be generalized to the effects of chronic highhydration (28). We previously noted an association be-tween polyuria and 24-hour urine protein, but a subse-quent investigation revealed that laboratory measurementerror was the most likely explanation for these results(13,29).
Figure 2. | Decline in kidney function between first and last assessment over 5.7 years (n � 2148). eGFR, estimated GFR.
Table 2. Percentage annual change in kidney function in relation to 24-hour urine volume at baseline (n � 2145a)
Age and GenderAdjusted Fully Adjusted
Changeb P Changeb P
Intercept �0.83 0.08 �1.03 0.03Age �0.01 0.01 0.01 0.50Gender (reference: male) 0.06 0.76 �0.08 0.71Urine volume (reference: 1 to 1.9 L/day)
�1 L/day �0.22 0.45 �0.20 0.512 to 2.9 L/day 0.11 0.64 0.12 0.62�3 L/day 0.87 0.02 0.86 0.02
Dipstick protein �1 g/L �2.56 �0.01Medications for hypertension (including diuretics) �0.63 0.01Cardiovascular disease �1.23 0.01
aExcludes three outliers with strong positive skew in estimated GFR decline.bMultiple linear regression: models were reduced using backward elimination at alpha � 0.1518,19 unless elimination changed theassociation with urine volume by �10%;19,20 age and gender were forced into all models.
2638 Clinical Journal of the American Society of Nephrology

The kidneys play a key role in regulating fluid balance,which is guided by tight homeostatic control of plasmaosmolality. Whereas increased plasma osmolality stimu-lates the release of arginine vasopressin, causing the kid-ney to retain water and decrease urine production, de-creased plasma osmolality inhibits the excretion ofvasopressin, causing the kidney to increase urine output(30,31). In addition to regulating fluid balance, the kidneysfilter waste from the blood and require a minimum obli-gate urine volume to remove the solute load (31,32). Kid-neys may function more efficiently in the presence of anabundant supply of water (33). Higher fluid intake in-creases the clearance of sodium, urea, and osmoles
(4,28,34), and high fluid intake is the most effective thera-peutic measure to prevent kidney stones (6,7,35). If thekidneys are made to economize on water and producemore concentrated urine to maintain plasma osmolality,they may incur greater metabolic demand, as demon-strated in studies of rats (23,32,36,37).
Osmolar excretion and urine volume are affected bygender and race. Some argue that the greater food con-sumption among men compared with women, and theirconsequent higher daily osmolar loads and higher argi-nine vasopressin, might contribute to their increasedsusceptibility to kidney disease and salt-sensitive hyper-tension. Similarly, black individuals excrete similar
Figure 3. | Urine volume and risk for renal decline in the general population (n � 2148). eGFR, estimated GFR; OR, odds ratio; CI,confidence interval.
Table 3. Association between urine volume and renal decline in the general population (n � 2148)
Mild to Moderate Renal Declinea Rapid Renal Declineb
24-hourUrine Volume n � 861
ORc (95% CI)
n � 214
ORc (95% CI)
Age and GenderAdjusted
MultivariateAdjusted
Age and GenderAdjusted
MultivariateAdjusted
�1 L/day 146 1.30 (1.00 to 1.70) 1.33 (1.01 to 1.75) 31 1.26 (0.81 to 1.97) 1.32 (0.83 to 2.09)1 to 1.9 L/day 454 1.0 1.0 111 1.0 1.02 to 2.9 L/day 205 0.82 (0.66 to 1.02) 0.84 (0.67 to 1.05) 62 0.97 (0.68 to 1.36) 1.01 (0.70 to 1.44)� 3 L/day 56 0.67 (0.47 to 0.96) 0.66 (0.46 to 0.94) 10 0.48 (0.24 to 0.94) 0.46 (0.23 to 0.92)
OR, odds ratio; CI, confidence interval.aMild to moderate renal decline: eGFR decline from baseline between 1% and 4.9%.bRapid renal decline: estimated GFR decline from baseline �5%.cOdds ratios were estimated using multinomial regression.dAdjusted for age (in 1-year increments), gender, baseline estimated GFR, dipstick protein �1 g/L, medication use for hypertension(including diuretics), diabetes, and cardiovascular disease.
Clin J Am Soc Nephrol 6: 2634–2641, November, 2011 Urine Volume and Renal Decline, Clark et al. 2639

daily osmolar loads as white individuals, but with lessurine volume, which may, in part, explain their higherrate of kidney disease and salt-sensitive hypertension(38 – 40). Accelerated loss of kidney function can have anumber of adverse consequences, including, but notlimited to, poor BP control, various biochemical abnor-malities, and higher levels of uraemic toxins (41).
We measured 24-hour urine volume in over 2000 indi-viduals from the general community. To our knowledge,this is the largest study of its kind. We excluded partici-pants with urine creatinine levels outside the specifiedlaboratory reference ranges, minimizing over- or undercol-lection as a source of misclassification bias. We obtainedaccurate comorbidity and medication information throughstructured interviews, blood tests, and medical chart re-views; controlled for age, gender, presence of proteinuria,smoking, cardiovascular disease, and medication use forhypertension; and used a highly sensitive algorithm todetect the presence of diabetes. Estimated renal declinewas calculated over a median follow-up time of 6 years.High variability in absolute change among those witheGFR �90 ml/min per 1.73 m2 made percentage change abetter measure of renal decline in this general populationsample (15). In addition, since percentage change adjustsfor baseline eGFR, this method effectively adjusts for dif-ferences in baseline renal reserve, giving greater weight tosmall changes in the presence of reduced renal reserve andless weight to small changes at higher levels kidney func-tion. However, results were similar when we analyzed theabsolute annual change rather than percentage change.True decline in renal function may be underestimatedwhen eGFR is used in place of measured GFR (42); how-ever, this should not affect the difference between compar-ison groups. Although we did not measure fluid intakedirectly, urine volume is an excellent proxy since it isdirectly proportional to fluid intake (6). Moreover, we didnot query participants on fluid consumption, and we donot know whether the type of fluid intake varied acrosscategories of urine volume. For instance, a recent analysisof NHANES data showed a positive association betweenconsumption of sugar-sweetened soft drinks and mi-croalbuminuria (43). We did not measure use of lithium,which may be associated with polyuria; however, the prev-alence of lithium use in the general population is extremelylow and is unlikely to explain the inverse association be-tween polyuria and renal decline. Finally, because thepresent study took place after the occurrence of an envi-ronmental disaster in which a substantial number of thisstudy’s participants were exposed to contaminated watercontaining E. coli O157 and Campylobacter, we consideredthe possibility that this exposure may have affected theresults. However, the presence of acute illness at the timeof the outbreak was not associated with polyuria or renaldecline (data not shown).
In this prospectively followed community-based cohort,renal decline was significantly slower in adults with higherversus lower urine volume. Our results do not supportaggressive fluid loading with its attendant risk for hypona-traemea (44,45) but are consistent with the popular belief inthe benefits of a moderately increased fluid intake. This isthe first large study of the general population to system-
atically study the relationship between urine volume andchange in kidney function over time. Although this is anobservational study and conclusions regarding causalitymust be cautious, these findings represent important initialevidence that higher fluid intake (2 to 3 L/d) may in factbenefit the kidney; however, it remains to be determinedwhether these results generalize to patients with CKD, thesegment of the population where preservation of renalfunction is most crucial.
AcknowledgmentsAn abstract of this work was presented at the North American
Congress of Epidemiology, Montreal, Canada, June 21 to 24, 2011.
DisclosuresThe funding source for this study was The Ontario Ministry of
Health and Long-term Care. The funding source had no role indesign and conduct of the study; in the collection, analysis, andinterpretation of the data; or in the preparation, review, or ap-proval of the manuscript.
All authors have completed the Unified Competing Interestform at http://www.icmje.org/coi disclosure.pdf (available, onrequest, from the corresponding author) and declare that (1) noauthors have received support from any companies for the sub-mitted work; (2) no authors have any relationships with anycompanies that might have an interest in the submitted work inthe previous 3 years; (3) their spouses, partners, or children haveno financial relationships that may be relevant to the submittedwork; and (4) no authors have nonfinancial interests that may berelevant to the submitted work.
References1. Vreeman RC, Carroll AE: Medical myths. BMJ 335: 1288–
1289, 20072. Wenzel UO, Hebert LA, Stahl RA, Krenz I: My doctor said I
should drink a lot! Recommendations for fluid intake in pa-tients with chronic kidney disease. Clin J Am Soc Nephrol 1:344–346, 2006
3. Valtin H: “Drink at least eight glasses of water a day.” Really?Is there scientific evidence for “8 x 8”? Am J Physiol RegulIntegr Comp Physiol 283: R993–R1004, 2002
4. Negoianu D, Goldfarb S: Just add water. J Am Soc Nephrol19: 1041–1043, 2008
5. Lette F, Dwyer JP: The fluid craze. Lancet 372: 782, 20086. Siener R, Hesse A: Fluid intake and epidemiology of urolithi-
asis. Eur J Clin Nutr 57 Suppl 2: S47–S51, 20037. Curhan GC, Willett WC, Speizer FE, Stampfer MJ: Beverage
use and risk for kidney stones in women. Ann Intern Med128: 534–540, 1998
8. Nagao S, Nishii K, Katsuyama M, Kurahashi H, MarunouchiT, Takahashi H, Wallace DP: Increased water intake de-creases progression of polycystic kidney disease in the PCKrat. J Am Soc Nephrol 17: 2220–2227, 2006
9. Hebert LA, Greene T, Levey A, Falkenhain ME, Klahr S: Highurine volume and low urine osmolality are risk factors forfaster progression of renal disease. Am J Kidney Dis 41: 962–971, 2003
10. Clark WF, Sontrop JM, Macnab JJ, Salvadori M, Moist L, SuriR, Garg AX: Long term risk for hypertension, renal impair-ment, and cardiovascular disease after gastroenteritis fromdrinking water contaminated with Escherichia coli O157: H7:A prospective cohort study. BMJ 341: c6020, 2010
11. Garg AX, Macnab J, Clark W, Ray JG, Marshall JK, Suri RS,Devereaux PJ, Haynes B: Long-term health sequelae follow-ing E.coli and Campylobacter contamination of municipalwater. Population sampling and assessing non-participationbiases. Can J Public Health 96: 125–130, 2005
2640 Clinical Journal of the American Society of Nephrology

12. Levey AS, Greene T, Kusek JW, Beck GJ: A simplified equa-tion to predict glomerular filtration rate from serum creati-nine. J Am Soc Nephrol 11: 155A, 2000
13. Ortho-Clinical Diagnostics. Vitros UPRO Materials Sheet. No.J04089 EN Version 3.0. 2003. Rochester, New York, Ortho-Clinical Diagnostics, Inc.
14. Sadjadi S: Genitourinary Disorders: Polyuria. In: The MerckManuals: Online Medical Library, edited by Porter R, KaplanJ, Whitehouse Station, New Jersey, Merck Sharp & DohmeCorp., 2009
15. Matsushita K, Selvin E, Bash LD, Franceschini N, Astor BC,Coresh J: Change in estimated GFR associates with coronaryheart disease and mortality. J Am Soc Nephrol 20: 2617–2624, 2009
16. Clark W, Macnab J, Sontrop J, Moist L, Jain A, Salvadori M, Suri R,Garg A: Dipstick proteinuria as a screening strategy to identify rapidrenal decline. J Am Soc Nephrol, 2011, in press
17. Expert Committee on the Diagnosis and Classification of Dia-betes Mellitus: Report of the expert committee on the diagno-sis and classification of diabetes mellitus. Diabetes Care26[Suppl 1]: S5–S20, 2003
18. Mickey RM, Greenland S: The impact of confounder selec-tion criteria on effect estimation. Am J Epidemiol 129: 125–137, 1989
19. Maldonado G, Greenland S: Simulation study of confounder-selection strategies. Am J Epidemiol 138: 923–936, 1993
20. Greenland S, Rothman K: Introduction to stratified analysis.In: Modern Epidemiology, 2nd ed., edited by Rothman K,Greenland S, Philadelphia, PA, Lippincott-Raven, pp 253–279, 1998
21. Strippoli GF, Craig JC, Rochtchina E, Flood VM, Wang JJ,Mitchell P: Fluid and nutrient intake and risk of chronic kid-ney disease. Nephrology (Carlton) 16: 326–334, 2011
22. Torres VE: Water for ADPKD? Probably, Yes. J Am Soc Neph-rol 17: 2089–2091, 2006
23. Bouby N, Bachmann S, Bichet D, Bankir L: Effect of waterintake on the progression of chronic renal failure in the 5/6nephrectomized rat. Am J Physiol- Renal Physiology 258:F973, 1990
24. Grantham JJ: Therapy for polycystic kidney disease? It’s wa-ter, stupid! J Am Soc Nephrol 19: 1–7, 2008
25. Wang X, Wu Y, Ward CJ, Harris PC, Torres VE: Vasopressindirectly regulates cyst growth in polycystic kidney disease.J Am Soc Nephrol 19: 102–108, 2008
26. Spigt MG, Knottnerus JA, Westerterp KR, Olde Rikkert MG,Schayck CP: The effects of 6 months of increased water in-take on blood sodium, glomerular filtration rate, blood pres-sure, and quality of life in elderly (aged 55–75) men. J AmGeriatr Soc 54: 438–443, 2006
27. Viberti GC, Mogensen CE, Keen H, Jacobsen FK, Jarrett RJ,Christensen CK: Urinary excretion of albumin in normal man:The effect of water loading. Scand J Clin Lab Invest 42: 147–157, 1982
28. Anastasio P, Cirillo M, Spitali L, Frangiosa A, Pollastro RM,De Santo NG: Level of hydration and renal function inhealthy humans. Kidney Int 60: 748–756, 2001
29. Clark WF, Kortas C, Suri RS, Moist LM, Salvadori M, WeirMA, Garg AX: Excessive fluid intake as a novel cause of pro-teinuria. CMAJ 178: 173–175, 2008
30. Ramsay D: Homeostatic control of water balance. In: Hydra-tion throughout Life, edited by Arnaud MJ, Montrouge,France, John Libbey Eurotext, pp 9–18, 1998
31. Berl T: Impact of solute intake on urine flow and water ex-cretion. J Am Soc Nephrol 19: 1076–1078, 2008
32. Popkin BM, D’Anci KE, Rosenberg IH: Water, hydration, andhealth. Nutrition Reviews 68: 439–458, 2010
33. Nicolaidis S: Physiology of thirst. In: Hydration throughoutLife, edited by Arnaud MJ, Montrouge, France, John LibbeyEurotext, pp 3–9, 1998
34. Pitts RF: Physiology of the kidney and body fluids: An intro-ductory text, Chicago, Illinois, Year Book Medical Publishers,1974
35. Consensus Conference. Prevention and treatment of kidneystones. J Am Med Assoc 260: 977–981, 1988
36. Bankir L, Bouby N, Trinh-Trang-Tan MM: Vasopressin-de-pendent kidney hypertrophy: role of urinary concentrationin protein-induced hypertrophy and in the progressionof chronic renal failure. Am J Kidney Dis 17: 661– 665,1991
37. Sugiura T, Yamauchi A, Kitamura H, Matsuoka Y, Horio M,Imai E, Hori M: High water intake ameliorates tubulointersti-tial injury in rats with subtotal nephrectomy: Possible role ofTGF-[bgr]. Kidney Int 55: 1800–1810, 1999
38. Adrogue HJ, Madias NE: Sodium and potassium in the patho-genesis of hypertension. N Engl J Med 356: 1966–1978,2007
39. Luft FC: Vasopressin, urine concentration, and hypertension:A new perspective on an old story. Clin J Am Soc Nephrol 2:196–197, 2007
40. Bankir L, Perucca J, Weinberger MH: Ethnic differences inurine concentration: Possible relationship to blood pressure.Clin J Am Soc Nephrol 2: 304–312, 2007
41. Kovesdy CP: Rate of kidney function decline associates withincreased risk of death. J Am Soc Nephrol 21: 1814–1816,2010
42. Xie D, Joffe MM, Brunelli SM, Beck G, Chertow GM, Fink JC,Greene T, Hsu CY, Kusek JW, Landis R, Lash J, Levey AS,O’Conner A, Ojo A, Rahman M, Townsend RR, Wang H,Feldman HI: A comparison of change in measured and esti-mated glomerular filtration rate in patients with nondiabetickidney disease. Clin J Am Soc Nephrol 3: 1332–1338, 2008
43. Shoham DA, Durazo-Arvizu R, Kramer H, Luke A, VupputuriS, Kshirsagar A, Cooper RS: Sugary soda consumption andalbuminuria: Results from the National Health and NutritionExamination Survey, 1999–2004. PLoS One 3: e3431, 2008
44. Gardner J: Death by water intoxication. Military Medicine167: 432–434, 2002
45. Noakes TD: Overconsumption of fluids by athletes. BMJ 327:113, 2003
Received: February 28, 2011 Accepted: July 24, 2011
Published online ahead of print. Publication date available atwww.cjasn.org.See related editorial, “Fluid Intake for Kidney DiseasePrevention: An Urban Myth,” on pages 2558–2560.
Clin J Am Soc Nephrol 6: 2634–2641, November, 2011 Urine Volume and Renal Decline, Clark et al. 2641