Embed Size (px)
Citation preview

Uohf
Uacprug
nrtrahapcdmpbr1a
PF
t
HP
M
CASE REPORT
©A
URINARY ASCITES WITHOUT HYDRONEPHROSIS IN ANEONATE WITH URETHRAL ATRESIA
ROBERT J. STEIN, PAUL H. NOH, AND HSI-YANG WU
ABSTRACTrethral atresia is a rare and usually fatal cause of prenatal bladder outlet obstruction. We present a casef urethral atresia with urinary ascites to highlight the difficulties in making the diagnosis in the absence ofydronephrosis. We also discuss possible reasons why this patient maintained normal renal and pulmonaryunction. UROLOGY 66: 432.e7–432.e8, 2005. © 2005 Elsevier Inc.
rtranwbbuwmw
lrtfpalpnussawa
svod
rethral atresia commonly causes fetal or neo-natal death unless a patent urachus persists or
vesicoamniotic shunt is placed. Even in the rareases that survive, hydronephrosis and renal dys-lasia often result in end-stage renal disease. Weeport a case of a neonate with urethral atresia,rinary ascites, bladder perforation, and sono-raphically normal kidneys.
CASE REPORT
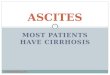
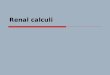
The patient was born at 37 weeks’ gestation witho prenatal testing. He was intubated at birth forespiratory failure and was noted on examinationo have significant ascites. Abdominal ultrasonog-aphy showed normal kidneys, ascites (Fig. 1), andn empty bladder (Fig. 2). No evidence of portalypertension or congenital heart disease was founds the cause of the ascites. A peritoneal drain waslaced and yielded 300 mL of clear fluid. Serumreatinine on the first day after birth was 0.7 mg/L, and the ascites creatinine was 0.8 mg/dL. Place-ent of a urethral catheter was unsuccessful. The
atient did not void during the first 48 hours afterirth. During the next 2 days, the ascites creatinineose to 3.6 mg/dL, and the serum creatinine rose to.6 mg/dL, suggesting drainage of urine into thebdomen. The patient was taken to the operating
resented at the Society for Fetal Urology Biannual Meeting, Sanrancisco, California, October 8, 2004.From the Department of Pediatric Urology, Children’s Hospi-
al of Pittsburgh, Pittsburgh, PennsylvaniaAddress for correspondence: Hsi-Yang Wu, M.D., Children’s
ospital of Pittsburgh, 3705 Fifth Avenue, 4A-424 DeSoto Wing,ittsburgh, PA 15213. E-mail: [email protected]: December 15, 2004, accepted (with revisions):
parch 29, 2005
2005 ELSEVIER INC.LL RIGHTS RESERVED
oom, but a 6F cystoscope could not be passed intohe urethra. A 0.035-in. guidewire would not passetrograde for more than 2 cm. During creation ofvesicostomy, significant bladder hypertrophy wasoted and a 1-cm perforation of the bladder domeas repaired. The urachus was not well visualizedecause of the mature fistulous tract between theladder and peritoneum, but no drainage from thembilicus was noted. The vesicostomy drainedell, and the peritoneal drain was removed. At 4onths of follow-up, the patient was doing wellith a serum creatinine of 0.4 mg/dL.
COMMENT
Our patient presented with a diagnostic chal-enge, as he did not have hydronephrosis or peri-enal urinoma on ultrasonography. The differen-ial diagnosis of fetal ascites includes nonimmuneetal hydrops due to congenital heart disease orortal hypertension, lysosomal storage diseases,nd obstructive uropathy.1 Because imaging andaboratory examination failed to find cardiac or he-atic causes for the ascites, the possibility of uri-ary ascites was revisited. It is likely that prenatalltrasonography would have suggested the diagno-is if hydronephrosis or a distended bladder wereeen before the perforation. The combination ofscites and the inability to catheterize the urethraere clues to the ultimate diagnosis of urethral
tresia and bladder perforation.Urethral atresia is usually fatal, with long-term
urvival requiring either early diagnosis and inter-ention with vesicoamniotic shunt or persistencef a patent urachus to allow normal pulmonaryevelopment. Gonzalez et al.2 reported that in 6
atients with urethral atresia who survived the neo-0090-4295/05/$30.00doi:10.1016/j.urology.2005.03.068 432.e7

naotpcnVccoc
rnucrihtsefspiSsaac
OW
st
b1
t
pv
psfi
ru
f
u
4
atal period, 3 had a vesicoamniotic shunt placed,nd the other 3 had either a vesicocutaneous fistular a patent urachus. Spontaneous bladder perfora-ion is also rare and is most often associated withosterior urethral valves.3–6 It is believed that de-ompression of the urinary tract protects the kid-eys and prevents irreversible renal dysplasia. Deries et al.7 noted that when decompression oc-urs, follow-up serum creatinine and creatininelearance are frequently normal. We believe thatur patient most likely had a patent urachus that
FIGURE 1. Right kidney and ascites.
FIGURE 2. Decompressed bladder.
losed late in gestation, followed by bladder perfo- v
32.e8
ation. Although the concept of a pop-off mecha-ism as protective of renal function in posteriorrethral valves has long been held,8 this has re-ently been challenged. Patil et al.9 reported thatenal function on the side of the pop-off valve ismpaired, and that patients with urinary ascitesave a lower glomerular filtration rate than pa-ients with urinoma. They suggested that the pres-ure required to cause urinary ascites from bladderxtravasation is greater than that required to causeorniceal rupture.9 The outcome in our patientuggests that a large bladder perforation can berotective of renal function, depending on the tim-ng of the urachal closure and bladder perforation.uch a presentation of urethral atresia is rare anduggests that when the degree of hydronephrosisnd lung development do not match the degree ofscites, unusual pop-off mechanisms should beonsidered in the diagnosis.
REFERENCES1. Seashore JH: Distended abdomen, in McMillan JA (Ed):
ski’s Pediatrics, 3rd ed. Philadelphia, Lippincott, Williams &ilkins, 1999, pp 322–323.2. Gonzalez R, De Filippo R, Jednak R, et al: Urethral atre-
ia: long-term outcome in 6 children who survived the neona-al period. J Urol 165: 2241–2244, 2001.
3. Trulock TS, Finnerty DP, and Woodard JR: Neonatalladder rupture: case report and review of literature. J Urol33: 271–273, 1985.4. Johanson L: Neonatal rupture of the bladder secondary
o posterior urethral valves. Pediatr Radiol 12: 304–306, 1982.5. Sahdev S, Jhaveri RC, Vohra K, et al: Congenital bladder
erforation and urinary ascites caused by posterior urethralalves: a case report. J Perinatol 17: 164–165, 1997.
6. Chen C, Shih SL, Liu FF, et al: In utero urinary bladdererforation, urinary ascites, and bilateral contained urinomasecondary to posterior urethral valves: clinical and imagingndings. Pediatr Radiol 27: 3–5, 1997.7. De Vries SH, Klijn AJ, Lilien MR, et al: Development of
enal function after neonatal urinary ascites due to obstructiveropathy. J Urol 168: 675–678, 2002.8. Rittenberg MH, Hulbert WC, Snyder HM, et al: Protective
actors in posterior urethral valves. J Urol 140: 993–996, 1988.9. Patil KK, Wilcox DT, Samuel M, et al: Management of
rinary extravasation in 18 boys with posterior urethral
alves. J Urol 169: 1508–1511, 2003.UROLOGY 66 (2), 2005