Embed Size (px)
Citation preview

International Journal of Phonosurgery and Laryngology, July-December 2013;3(2):61-64 61
Urbach-Wiethe Disease: A Rare Cause of Hoarseness of Voice
IJOPL
CASE REPORT
Urbach-Wiethe Disease: A Rare Cause of Hoarseness of VoiceDeepthi Koganti
10.5005/jp-journals-10023-1065
ABSTRACTUrbach-Wiethe disease is a rare, autosomal recessive disorder, characterized by infiltration of periodic acid-Schiff positive hyaline material into the skin, oral cavity, larynx and internal organs. The clinical manifestations include hoarseness of voice, beaded papules along the eyelid margins, skin scarring and an inability to protrude the enlarged and thickened tongue. Laryngeal involvement is typical and causes hoarseness of voice. In this paper, we present a case of a middle-aged female with clinical features suggestive of Urbach-Wiethe disease. This entity is of interest to the otolaryngologist as it is a rare cause of hoarseness of voice.
Keywords: Urbach-Wiethe disease, Lipoid proteinosis, Hyalinosis cutis et mucosae.
How to cite this article: Koganti D. Urbach-Wiethe Disease: A Rare Cause of Hoarseness of Voice. Int J Phonosurg Laryngol 2013;3(2):61-64.
Source of support: Nil
Conflict of interest: None
INTRODUCTION
Urbach-Wiethe disease, also known as lipoid proteinosis or hyalinosis cutis et mucosa, is a rare mucocutaneous disorder reported mainly in patients with a European ancestry. It was first described by Seibenmann in 1908 but the first detailed report was made by Urbach and Wiethe in 1929. Hoarseness is observed in early childhood associated with infiltration and thickening of the skin. It is an autosomal recessive disorder, caused by widespread deposition of a lipoprotein complex in the skin, mucous membranes of the mouth and larynx and occasionally other organs.1 This hyaline-like material is periodic acid-Schiff (PAS) positive and diastase resistant.2
It has been shown that this disease is caused by mutations in the extracellular matrix protein 1 gene (ECM1 gene).3
CASE REPORT
A 35-year-old female presented to the outpatient Department of Otorhinolaryngology of Mahatma Gandhi Medical College and Research Institute, Puducherry, with chief complaints of hoarseness of voice since childhood. A history of weak cry at birth was elicited. The hoarseness of voice had gradually progressed with time but there was no history of speech impairment. The patient developed multiple popular lesions of the skin over the face and extremities at about 5 years of age, which on healing showed scarring. There was
thickening and beading of the margins of the eyelids. The patient gave a history of recurrent episodes of convulsions in childhood not associated with fever. The patient was a product of a consanguineous marriage with an uneventful pregnancy and labor. There was a history of similar complaints in one of her siblings but there was no such history in either of her parents. There was no history of any other neuropsychiatric disturbances or visual impairment. There was no history of photosensitivity, facial edema, joint swellings or joint pains. The patient had no specific nasal or aural complaints. There was no history suggestive of any other systemic complaints.
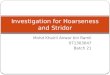
General examination of the patient showed a moderately built and nourished, otherwise healthy female. The patient had a hoarse voice and was pale. Examination of the skin showed multiple waxy skin colored and hyperpigmented papules arranged discretely seen over the extensor aspect of upper limbs, face, chest, trunk and axilla (Fig. 1). Beaded papules were seen along the margins of the upper and lower eye lids (moniliform blepharosis) (Fig. 2). Examination of the oral cavity revealed restriction of mouth opening up to grade II trismus. The patient’s lips were indurated, fissured and drawn inwards. The tongue was enlarged, firm, bald, and the patient was unable to protrude the tongue beyond the lip margins (Fig. 3). The buccal mucosa was pale and indurated. Indirect laryngoscopy revealed nodules in the epiglottis and vocal cords (Fig. 4). Both vocal cords were thickened with normal mobility. No mass lesions were identified. Examination of the nose and ears revealed no abnormalities. Systemic examination of the patient did not reveal any abnormal finding.
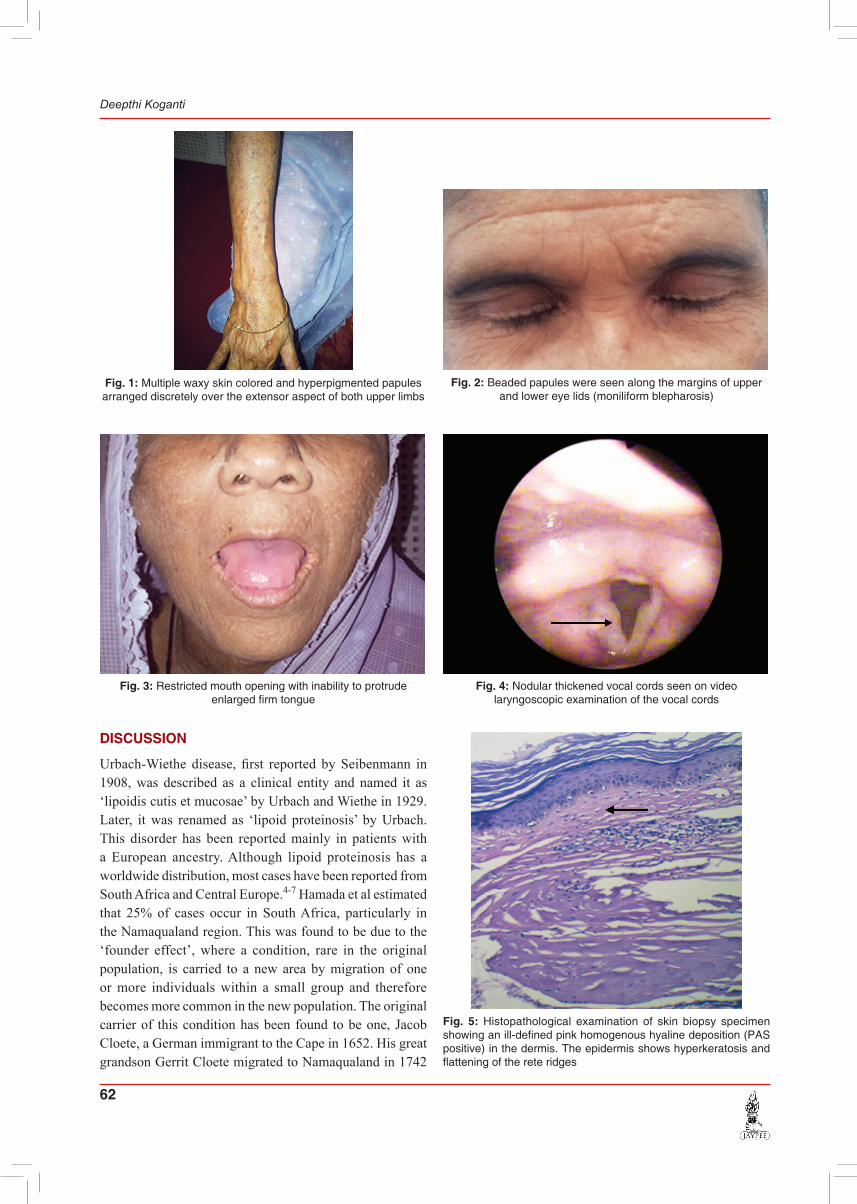
Videolaryngoscopy confirmed the findings of indirect laryngoscopy. Routine laboratory investigations including complete hemogram, urine examination, liver function tests and renal function were within normal limits. CT scan brain was normal. A skin biopsy from one of the papular lesions over the forearm was performed and histopathological examination of the specimen revealed an ill-defined homogeneous hyaline deposition in the dermis. This material was PAS-positive and diastase resistant (Fig. 5). The epidermis showed hyperkeratosis and flattening of the rete ridges. The nodule showed pink hyaline material along the thin-walled blood vessels and adnexal structures and had a lamellar pattern (Fig. 6).
62
Deepthi Koganti
Fig. 1: Multiple waxy skin colored and hyperpigmented papules arranged discretely over the extensor aspect of both upper limbs
Fig. 2: Beaded papules were seen along the margins of upper and lower eye lids (moniliform blepharosis)
Fig. 3: Restricted mouth opening with inability to protrude enlarged firm tongue
Fig. 4: Nodular thickened vocal cords seen on video laryngoscopic examination of the vocal cords
Fig. 5: Histopathological examination of skin biopsy specimen showing an ill-defined pink homogenous hyaline deposition (PAS positive) in the dermis. The epidermis shows hyperkeratosis and flattening of the rete ridges
DISCUSSION
Urbach-Wiethe disease, first reported by Seibenmann in 1908, was described as a clinical entity and named it as ‘lipoidis cutis et mucosae’ by Urbach and Wiethe in 1929. Later, it was renamed as ‘lipoid proteinosis’ by Urbach. This disorder has been reported mainly in patients with a European ancestry. Although lipoid proteinosis has a world wide distribution, most cases have been reported from South Africa and Central Europe.4-7 Hamada et al estimated that 25% of cases occur in South Africa, particularly in the Namaqualand region. This was found to be due to the ‘founder effect’, where a condition, rare in the original population, is carried to a new area by migration of one or more individuals within a small group and therefore becomes more common in the new population. The original carrier of this condition has been found to be one, Jacob Cloete, a German immigrant to the Cape in 1652. His great grandson Gerrit Cloete migrated to Namaqualand in 1742

International Journal of Phonosurgery and Laryngology, July-December 2013;3(2):61-64 63
Urbach-Wiethe Disease: A Rare Cause of Hoarseness of Voice
IJOPL
and intermarried with the inhabitants of the area. As the area is somewhat isolated, consanguineous marriages, resulted in relatively high proportion of homozygous affected individuals.8,9
Urbach-Wiethe disease is a rare, autosomal recessive disorder characterized by generalized thickening of skin, mucosae and certain viscera. Hamada et al mapped LP to chromosome 1q21 at D1S4985 and stated that more severe mucocutaneous LP phenotype is exhibited due to mutations outside exon 7. Pathogenetic loss-of-function mutations were identified in the extracellular matrix protein 1 (ECM1) gene. ECM1 is a glycoprotein with threee varieties: ECM1a, ECM1b and ECM1c. EMC1 is expressed in the dermis, basal keratinocytes, endothelial cells and developing bones linked to keratinocyte differentiation, basement membrane regulation, collagen composition and growth-factor binding. Neurologic features do not show any specific genotype- phenotype correlation. The mutated ECM1 gene leads to deposition of hyaline material in the dermis and around blood vessels and adnexal epithelia.10,11 The patient might present with abnormal scarring and wound healing and premature aging.12 Due to early hyaline material laryngeal infiltration, hoarseness is present at birth or in the early infancy progressing with time.13 Skin changes usually appear in early life, and these initial lesions resemble impetigo, which heal with atrophic scarring. Nodular waxy lesions appear later on the face, hands, elbows and knee. Bead-like papules occur on the lid margins, which coalesce leading to a coarse thickened appearance with scarring.14
Mucosal lesions present early in life. Both the cutaneous and the mucosal portions of the lips are irregularly thickened. Whitish or yellowish nodules appear on the undersurface of
the tongue and on the buccal mucosa, pillars of the fauces, tonsils, uvula and epiglottis. In more severe cases, the lesions coalesce to form diffuse irregular mucosal thickenings. Induration of the frenulum of the tongue leads to restricted movement. Similar involvement of the uvula results in its retraction and near disappearance. Indirect laryngoscopy may be difficult because of the patients inability to open their mouth fully; therefore, direct laryngoscopy has to be performed under general anesthesia. Thickening and nodularity of the vocal cords and of adjacent structures are seen.6 Lesions are found in the interarytenoid areas and on the aryepiglottic folds. Later, the true and false cords may be involved and airway compromise may develop.15,16
The classic and the most easily recognizable sign is the beaded papules on the eyelid margins (moniliform blepharosis) occurring in about two-third of the cases which is said to be pathognomonic.17 These papules are also described as ‘string of beads’ or ‘eyelid beading’.18,19
Few other ocular findings due to hyaline deposits have been described in the conjunctiva, cornea, trabeculum and retina. Later corneal opacities or secondary glaucoma, due to infiltration in the trabeculum, may appear. Deposition of hyaline material in the small bowel may lead to intestinal bleeding. Although autopsy studies have shown lipoid proteinosis to be a generalized disorder with microscopic deposits of hyaline material in practically every organ, symptoms related to other viscera have not been described.20 Some patients may present with extracutaneous and extramucosal features mainly neurological, like epilepsy, memory loss and schizophrenic behavior, sometimes in association with intracranial calcification in the temporal
Fig. 6: Histopathological examination of the skin biopsy specimen showing pink hyaline material along the thin-walled blood vessels and adnexal structures

64
Deepthi Koganti
lobes or hippocampus, easily detected by brain computed tomography (CT).21
Histologically, this entity is characterized by disruption/duplication of the basement membrane with deposition of hyaline material at the level of the basement membrane resulting in its thickening at the dermoepidermal junction. This deposition is also observed in papillary dermis, surrounding capillaries and around adnexal epithelia, especially sweat coils. The hyaline material is eosinophilic, PAS-positive and diastase resistant, indicating the presence of glycoproteins. Acumulations of type IV and V collagen occur around the blood vessels and appendages.2,22
No effective treatment is described for this disease. In a case study, successful clinical and histological improvement was observed with a continuous treatment with D-penicillamine, a chelating agent.23 Another study reported improvement after administration of dimethyl sulfoxide (DMSO) at a dose of 60 mg/kg/day.24 But, a more recent report in three patients from Turkey showed no benefit of DMSO.25 In few studies, oral etretinate have shown promising results.10 Toosi and Ehsani postulated that acitretin helps in improving laryngeal lesions, improving voice when compared to other drugs.26 Although both oral dimethyl sulfoxide and oral etretinate have shown promising results, recent case reports have found them to be ineffective.27
Excision of the lesions using microlaryngoscopy instruments has been shown to improve the airway and quality of the voice. Rarely, tracheostomy has been required to ensure a safe airway.17,28 CO2 laser has been used successfully to treat eyelid deposits in lipoid proteinosis.29
Despite the variety of the reported treatment options for LP, there have been no lasting improvements or total cure.
REFERENCES
1. Black MM. Lipoid proteinosis, Metabolic and nutritional disorders. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors. Rook/ Wilkison/ Ebling Textbook of Dermatology. 6th edn, Oxford: Blackwell Science 1998. p. 2460-2462.
2. Touart DM, Sau P. Cutaneous deposition diseases. Part I. J Am Acad Dermatol 1998;39:149-171.
3. Shivaswamy KN, Thappa DM, Laxmisha C, Jayanthi S. Lipoid proteinosis in two siblings: A report from South India. Dermatol Online J 2003;9:12.
4. Muda AO, Paradisi M, Angelo C, et al. Lipoid proteinosis: clinical, histologic and ultrastructural investigations. Cutis 1995;56:220-224.
5. Farolan MJ, Ronan SG, Solomon LM, Loeff DS. Lipoid proteinosis: case report. Pediatr Dermatol 1992;9:264-267.
6. Grosfild JCM, Spaas J, Vande Staak WJB M, Stradhouders AM. Hyalinosis cutis et mucosae. Dermatologia 1965;130:239-266.
7. Burnett JW, Mercy SM. Lipoid proteinosis. Am J Dis Child 1963;105:81-84.
8. Van Hougenhouck-Tulleken W, Chan I, Hamada T, et al. Clinical and molecular characterizations of lipoid proteinosis in Namqualand, South Africa. Br J Dermatol 2004;151:413-423.
9. Gordon H, Gordon W, Botha V. Lipoid proteinosis in an inbred Namaqualand community. Lancet 1969;1:1032-1035.
10. Hamada T. Lipoid proteinosis. Clin Exp Dermatol 2002;27: 624-629.
11. Hamada T, McLean WH, Ramsay M, et al. Lipoid proteinosis maps to 1q21 and is caused by mutations in the extracellular matrix protein 1 gene (ECM1). Hum Mol Genet 2002;11: 833-840.
12. Ringpfeil F. Selected disorders of connective tissue: pseudoxanthoma elasticum, cutis laxa and lipoid proteinosis. Clin Dermatol 2005;23:41-46.
13. Acar A, Eryılmaz A, Gocer C, et al. Lipoid proteinosis of larynx: review of four cases. Int J Pediatr Otorhinolaryngol 2004;68:1557-1561.
14. Gordon H, Gordon W, Botha V, Edelstein I. Birth defects (Original Article Series), New York: National Foundation - March of Dimes 1971;7(8):164-177.
15. Heyl T. Lipoid proteinosis. Br J Dermatol 1963;75:465-473. 16. Harper JI, Duguid KP, Staughton RC, Moffat DC. Oropharyngeal
and laryngeal lesions in lipoid proteinosis. J Laryngol Otol 1983; 9:877-880.
17. Bozdag KE, Gul Y, Araman A. Lipoid proteinosis. Int J Dermatol 2000;39:203-204.
18. Staut CCV, Naidich TP. Urbach-Wiethe disease (lipoid proteinosis). Pediatr Neurosurg 1998;28:212-214. [9732251] [DOI:10.1159/000028653]
19. Thappa DM, Gupta S. Eyelid beading—a useful diagnostic clue for lipoid proteinosis. Indian Pediatr 2001;38:97. [11175944]
20. Francois J, Bacskulin J. Manifestations oculaires du syndrome d Urbach Wiethe. Ophthalmologica 1968;155:433-438.
21. Friedman L, Mathews RD, Swanepoel PD. Radiographic and computed tomographic findings in lipoid proteinosis: A case report. S Afr Med J 1984;65:734-735.
22. Harper JI, Filipe MI, Staughton RC. Lipoid proteinosis: Variations in histochemical characteristics. Clin ExpDermatol 1983;8:135-141. [6851235] [doi:10.1111/j.1365-2230.1983.tb0 1757.x]
23. Kaya T, Kokturk A, Tursen UI, kizoglu G, Polat A. D-peni-cillamine treatment for lipoid proteinosis. Pediatr Dermatol 2002;19:359-362.
24. Wong C, Lin C. Remarkable response of lipoid proteinosis to oral dimethyl sulphoxide. Br J Dermatol 1988;119:541-544.
25. Gruber F, Maestar D, Stasic A, Grgurevic Z. Treatment of lipoid proteinosis with etretinate. Acta Derm Venereol 1996;76:154-156.
26. Toosi S, Ehsani A. Treatment of lipoid proteinosis with acitretin: a case report. J Eur Acad Dermatol Venereol 2009;23:482-483.
27. Oz F, Kalekoglu N, Karakullukcu B, Ozturk O, Oz B. Lipoid proteinosis of the larynx. J Laryngol Otol 2002;116:736-739.
28. Richards SH, Bull PD. Lipoid proteinosis of the larynx. J Laryngol Otol 1973;87:187-190.
29. Rosenthal G, Lifshitz T, Monos T, et al. Carbon dioxide laser treatment for lipoid proteinosis (Urbach-Wiethe syndrome) involving the eyelids. Br J Ophthalmol 1997;81:253.
ABOUT THE AUTHOR
Deepthi KogantiResident, Department of Otorhinolaryngology, Pinnamaneni Siddhartha Institute of Medical Sciences, Chinoutpalli, Andhra Pradesh, India e-mail: [email protected]