Embed Size (px)
Citation preview

AUSTRAliAN PHYSIOTHERAPY
Andrea MosesJohn Carman
OR IG IN ALAR TI CLE
Anatomy of the cervicalspine: implications for theupper limb tension test
A detailed investigation of the anatomy of thelowercervical nerves andassociated structureswas undertaken, as these structures wouldmost likelybeaffectedbyanystresses generatedin the nerves of the brachial plexus during theupper limb tension test (ULTI). Theinv8stigationused dissection of three adult human spinesandhistological sections ofthree cervical spines.The results support the hypothesis that thelower cervical nerves have a specialisedanatomical arrangement which may protectthem from forces generated in the upper limband cervical spine by the ULIT. The fifth, sixthand seventh cervical nerves are securelyattached to many structures as they emergefromthespinal cord to formthe brachial plexus.Furthermore I theposteri0rlongitudinail igamentanchors the nerve roots to the vertebral bodiesand intervertebral discs. The results suggestthat innervated structures other thanneuromeningeal tissue may also need to beconsidered when evaluating apatient'spositiveULIT response.[Moses AS and Carman JB: Anatomy of thecervical spine: implications for theupperlimbtension test. AustralianJournalofPhysiotherapy42: 31-35]
Key words: Anatomy; BrachialPlexus; Cervical Vertebrae;Spinal Nerves
Moses AS MSc(Hons), ADP(OMT), DipPhty is apart-time lecturerattheSchool ofPhysiotherapy,Faculty of Health Studies,.Auckland Institute ofTechnology.Carman JB BMedSc,MBChB, DPhil(Oxon} isProfessor of Anatomy at theSchoaIof Medicine,University of Auckland.
he upper limb tension test(UL'IT) is a clinical test currentlyused to differentiate between pain
originating from neuromeningealtissue and that originating from otherstructures in the upper limb. The testwas originally described by Elvey(1980) and is a combination ofpassiveshoulder girdle depression,glenohumeral abduction posterior tothe coronal plane, forearm supinationand wrist extension. Cervicalsideflexionmay be added to the basictest position. Neuromeningeal tissue isimplicated if there is reproduction ofthe patient's symptoms once theUL'IT position is adopted. Areduction ofsymptoms with theaddition of ispilateral wrist flexion oran increase in symptoms with cervicalside-flexion to the contralateral sideare further confirmation of a positiveUL'IT result.
The link between the biomechanicsof the UL'IT and the reproduction ofthe patient's symptoms is unclear. It isdifficult to interpret the precise originof the patient's symptoms such as
Correspondence: Andrea Moses, Schoal ofPhysiotherapy, Facu Ity of Health Studies,Akoranga Campus, Auckland Institute ofTechnology, Private Bag, Auckland, NewZealand.This work was supported in part bya Universityof Auckland Post-graduate Scholarship. Thepaper was presented at the.MPAA 8th BiennialConference in Perth 1993.
cervical spinal nerve, dura, or cords ofthe brachial plexus on the basis of theUL'IT.
The biomechanical effects of theUL'IT on the anatomical structures inthe cervical spine have beeninvestigated in a number of studies.Following his observations of cadaversat post-mortem, Elvey (1980) claimedthat the test produces a progressivelygreater tension in the peripheral nerveswhich is transmitted to the cervicalnerve root sheaths. The tension in theperipheral nerves and spinal nerves wasnot measured in .thatstudy.Followingfurther cadaver observations (1983 and1986), Elvey suggested that the C5 andC6 roots of the brachial plexus aremost likely to be subjected to tensilestresses during theUL'IT.
Selvaratnam and co-workers (1988)investigated the strain.at the C5-T1roots of the brachial plexus in fivepost....mortem cadavers. Themovements of the UL'IT werecombined with either contralateralcervical flexion (CLF) or ipsilateralcervical flexion (ILF) and strain at theC5 ,C6, C7,C8 and T1 was assessed.The C5 root showed the greatestdifference in strain between CLF andILF followed by theC6,C7,C8 and T1roots.
Ginn (1988) and Reid (1987)investigated the tension changes in thebrachial plexus of cadavers during theUL'IT. Buckle force transducers wereused to measure the tension changes in-

from page 31the cords of the brachial plexus of thecadavers. Results showed that thelateral cord and therefore the C5 andC6 cervical nerves are subject to thegreatest tension during the UL'IT.
Strain in the lateral cord and thesubclavian artery during theUL'ITwas evaluated quantitatively by Wilsonet al (1994). The investigatorsmeasured the distance betweennominated points on the lateral cordand on the subclavian artery of twoembalmed cadavers. Strain scores werecalculated from the measurements foreach part of the of the artery. Resultsshowed that the UL'IT performedwithCLF produces more strain in thelateral cord and in some parts of thesubclavian artery than with ILF. Strainin the posterior and medial cords ofthe brachial plexus was not measured.
Anatomical studies of the cervicalnerves which may aid in theinterpretation of the effects of forcesgenerated by the ULTT on thecervical spine. and brachial plexus areinconsistent. Studies do not agree onthe precise attachments of the lowercervical nerves to their surroundingstructures. In the 1950s, Frykholmpublished detailed anatomic andhistological studies of the lowercervical vertebrae, intervertebral discs,nerve roots, root pouches and rootsleeves (Frykholm 1951 and 1952).Since then, only a few publishedstudies have specifically described therelations of the emerging cervicalnerves to their surrounding structures(BonneI1984, Herzberg et al 1985,Kikuchi 1982,Kikuchi et al1981Payne and Spillane 19"57, Sunderland1974aand 1974b). These authorsgenerally agree with Frykholm'sfindings on the cervical nerves, duraand dural sleeves. The anterior rootand the posterior root of the nerve exitthe dura separately, each in a separatesleeve of dura. The dura is covereddorsally by thin epidural tissue whichextends out laterally to contribute tothe sheaths of the spinal nerve.Ventrally, the dura is covered bythicker tissue. The posteriorlongitudinal ligament (PLL) has afascia extending laterally to attach to
ORI GIN A L A RII CLE
the dural root sleeves. This fasciacontinues on to take part in theformation of the sheath of the spinalnerve.
There is further inconsistency in theliterature as to the extent to which thecervical nerves are attached to theintervertebral foramina and to theneighbouring zygapophyseal joints.Frykholm (1952) and Bonnel (1984)state that the nerves attach byconnective tissue to the walls of theforamina~However,Sunderland(1974a and 1974b) claimed that therewere virtually no attachments betweenthe nerves and the foramina, althoughanteriorly he found some exchange offibres between the·nerve sheath andthe "capsule ofthe neighbouringintervertebral joint" (presumably theuncovertebral joint), (Sunderland1974b, p. 707).
Frykholm (1952) described a strongattachment of the cervical nerves totheir neighbouring zygapophysealjoints. Others have not described suchattachments at all despite their studiesbeing detailed investigations of theanatomy of the cervical spine (Bonnel1984, Hayashi etal 1977, Herzberg etal 1985, Kikuchi 1982, Kikuchi et al1981, Payne and Spillane 1957).The cervical nerves are anchored to
the gutters of the transverse processes(Bonnel 1984, Frykholm 1952,Herzberget al1985, Kikuchi 1982,,Kikuchi.et al1981,Sunderland 1974aand 1974b), but not all authors agreeon the method ofattachment, or therole of these attachments in preventingtraction to the nerve and nerve roots.The attachments between the fifth,sixth and seventh cervical nerves andthe transverse processes are describedby Frykholm (1952, p.16) as"specialised ligaments",by Sunderland(1974a,p. 757 and 1974b,p. 707) as"fibrous slips"or "fibrous attachments"(Sunderland 1978,p. 875) and byHerzberg et el (1985, p.123) asspecialised "semiconic ligaments". Allthree authors suggest that thisspecialised attachment between thetransverse process and the cervicalnerves serves as the major anatomicalstructure which prevents avulsion ofthe cervical nerve roots.
AUSTRAliAN PHYSIOTHERAPY
The posterior longitudinal ligamenthas a fascial extension which attachesto the dural root pouch and continuesthrough the IVF to take part in theformation of the periradicular sheath(Frykholm 1951 and 1952, Hayashi etal 1977, Kilmchi eta11981, Payne andSpillane 1957,). Kilmchi (1982) foundthat only the superficial (moreposterior) layer of thePLL extendslaterally as a connective tissuemembrane to envelope the nerveswhere it becomes the epiradicularsheath.In summary, there is a degree of
variance in the literature concerningthe precise details of the attachmentsof the lower cervical nerves andparticularly how substantial they are. Itis also not clear which structures in thecervical spine may produce symptomswhen subjected to forces developed inthe upper quadrant during the ULTI.The hypothesis that the UL'ITselectively produces symptoms fromneuromeningeal tissue may not beentirely accurate. To investigate theconnections of the neuromeningealtissue a detailed study of the anatomyof the emerging cervical nerves andassociated nerve roots, and theirrelationship to the dura, theintervertebral foramina (IVF),transverse processes, and thePLL wascarried out.
MethodGross anatomyThe gross anatomical features ofthecervical nerves and their connectionsto the surrounding structures as theyemerge from the vertebral canal andpass laterally over the transverseprocesses were studied by dissection.The dissections were .carried out onfour sides in three embalmed cadaversunder six times and 10 timesmagnification using an.OperatingMicroscope (Leitz, West Germany).Two cadavers were dissected using ananterior approach and one cadaver wasdissected using a posterior approach.
HistologySegments of one side of the vertebralcolumn from three cadavers (two

AUSTRAliAN PHYSIOTHERAPY ORIGINAL ARTICLE
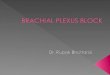
figure 1A horizontal histological section midway through the body of the C4 vertebra. Dorsal is tothe top, lateral is to the left. Magnification: 12.5A group of ventral rootlets are entering their dural sleeve. The lateral extension of theposterior longitudinal ligament (arrow) is seen attaching to the dorsal aspect of thevertebral body of C4 and arching laterally to merge with the ventral and extreme lateralaspect of the dural sleeve. Posteriorly, connective tissue extending from the periosteumof the lamina blends with the dorsal aspect of the dural sleeve. The thick ligamentumflavum blends with the lamina posteriorly.
female, 1 male, aged 69-91 years) wereprepared for histological examination.One provided sagittal sections fromthe midline to beyond the tips of thetransverse processes from C3-Tl; asecond provided horizontal sectionsfrom C3-C7; and a third providedhorizontal sections of the nerves C4C7 and the related soft tissues.
Each specimen was- cut into blocks ofapproximately 5 X 4 X 2 centimetresfor processing~ Specimens weredecalcified for between three and sixweeks, processed routinely for paraffinembedding, and sectioned at 12microns. Ten to 20 sections wererecovered from every hundred cutserially at reasonably regular intervalsand stained with either van Gieson'spicric acid-acid fuschin stain or elasticvan Gieson's stain (Carson 1990).
An assessment of tissue shrinkage wasmade by comparing the processedtissue used in this study with 16 freshfrozen sections of spinal cord and withmeasurements in vivo of spinal corddiameters by MRI (Sherman, Nassuaxand Citrin 1990). Anteroposterior andtransverse diameters at the C5-C7levels of the spinal cord were used forcomparison in each case. Comparedwith fresh frozen spinal cord, there wasa linear shrinkage of 9 per cent, withMRI measurements a linear shrinkageof 13 per cent.
A comparison between processed andfrozen sections was chosen becausemorphological artifacts due to freezingare of "minor significance" accordingto Pech et al (1987, p.782). Theseauthors investigated volume changes,artifacts in tissue and computedtomography (CT) attenuation values infrozen cadavers and animals. Resultsshowed that the nerves, muscles andspinal cord retained their normaltopographic position followingfreezing. It therefore seemedappropriate to compare the processedtissue used in this study with frozensections.

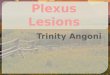
Figure 2A sagittal histological section through the 4th and 5th cervical vertebral bodies andzygapophvseaJ joints. Superior is 10 the top, dorsal is to the left. Magnification 11.5The posterior longitudinal ligament (arrow) is seen running betvveen the posterior aspectof the C4/5intervertebral disc and the vertebral body of C5.The dorsal root lies superiorto the ventral root and each root lies within itsolNn dural sleeve. Multiple strands ofconnective tissue extending from the posterior longitudinal Ugament blend with theanterior and inferior aspects of the ventral root. Fat and small veins fill the space in theintervertebral foramen which is not occupied by the nerve roots.
FromResultsGross anatomyThe course and relations of the nervesCS, C6 andC7 were studied usinganterior, posterior and sagittalapproaches. The course and relationsof CS, C6and C7 within the IVF andin the gutters of the cervical transverseprocesses was essentially identical. Asthese three nerves emerged from theIVF, dense white fibrous tissueconnected much of their circumferenceto the bony margins of their respectiveIVF, including the zygapophyseal jointcapsule posteriorly. The inferiorsurfaces of the nerves lacked this denseconnective tissue attachment. Onlyloose connective tissue connected themto the pedicle below and, forCS ·andC6, to the floor of the gutter of thetransverse process.
A thick fascia, extending laterallythrough the IVF from the posteriorlongitudinal ligament (PLL), blendedinto the epineurium of the anterioraspects of the nerves. As the nervesemerged from the IVF, they becameflattened anteroposteriorlyand passedposteriorly to the vertebral artery.Thick dense irregular connective tissuefibres ran between the nerves find thevertebral artery.
The vertebral artery demonstratedthe following relationship with thenerves: On its medial side, thevertebral artery was connected by slipsofdense irregular connective tissuefrom its adventitial coat hoth to thecervical vertebrae C5,C6andC7,andto the intervertebral discs between C5andC6, and C6 andC7. On its lateralside, connective tissue fibres ranbetween the·adventitia of the arteryand the anterior surface·of the nervesC5, C6 andC7. Pulling laterally on thenerves caused the vertebral artery tomove laterally. Lateral displacement ofthe artery appeared to be limited bythe medial attachments of the artery tothe periosteum of the C5 and C6vertebral bodies and the intervertebraldisc of C5 M C6.
As the nervesC5 and C6 coursedlaterally in the gutter towards the
OR IG IN A L A R TIC LE
periphery, their anterior and posteriorregions were attached to the anteriorand posterior edges of the gutters ofthe transverse processes by connectivetissue bundles. These bundles werediscrete bands of dense connectivetissue. They were most prevalent at theposterior gutter wall and thickest at themedial end ofthe gutter. There wereonly a few delicate strands ofconnective tissue between the floors ofthe bony gutters and· the nerves.HistologyThe histological findings in this studydemonstrate the following attachmentsof the lower cervical nerves as theyemerge from·the.spinalcord andcourse toward the periphery. Theventral and dorsal root of each nervelies within its own dural sleeve andpierces the dura separately. The duralsleeves are attached to theirsurrounding structures. Anteriorly,dense connective·tissue extends fromthe PLL to the anterior dura in the
AUSTRAliAN PHYSIOTHERAPY
region ofthe emergence of the rootsfrom their dural sleeves (Figure 1).The connective tissue extendinglaterally from the ligament consists ofasingle layer ofmembranous tissuewhich attaches to the posterior aspectsof the vertebral bodies andintervertebral discs. The lateralextensions of the PLL sweep under theventral root to attach the nerve root tothe floor of the intervertebral foramen(Figure 2). Posteriorly, connectivetissue fibres extending from theinferior pedicle blend with theposterior aspect of the .dura. Furtherlaterally, the dorsal root ganglion liesimmediately posterior· to the vertebralartery and is firmly connected to it bydense connective tissue irregularlyarranged. Connective tissue fibreswhich are continuous with thePLLattach to the anterior surface of theportion of the dorsal root ganglionwhich lies medial to the vertebralartery.

AUSTRAliAN PHYSIOTHERAPY
DiscussionThe tissue blocks used for histologywere carefully prepared to ensure thatthe nerves and their surroundingstructures were left as undisturbed aspossible. The normal relations of thetissues within the blocks showed onlythe disturbances usual in suchpreparations. This could also beconfirmed by examining serial sectionsfrom neighbouring blocks. There wasno evidence of a disruption to thenormal anatomy in any of the blocks.Likewise the relations were notseriously disturbed by the shrinkagecaused by histological processing. Thetissue used in this·study was fixed,decalcified, processed and impregnatedwith paraffin wax. Each of theseprocedures can cause the tissue toshrink. Itis clear that there was someshrinkage of the soft tissues during theprocessing of the tissue blocks forhistology. However, the purpose ofthis study was to investigate thetopography of the cervical spine, not toassess the amount of tissue present.Shrinkage of about 13 per cent,asexemplified by the shrinkage of thespinal cord, would have little effect onthe relationship between one tissue andanother and so the observations madeof a typical cervical nerve wereconsidered valid.
This study showed that the lowercervical nerves have a significantattachment to the walls of the IVF.Posteriorly, at the medial end of theforamina, the nerves attach to theperiosteum of the inferior pedicles,and, by dense connective tissue, to thecapsules of the zygapophyseal joints.Anteriorly, the nerves are attached tothe vertebral bodies and intervertebraldiscs by the lateral extension of thePLL. Although individual anatomicalvariation is recognised, and the studyused a small sample size, no variationin the cervical anatomy betweenspecimens was observed. The findingsare unlikely to be the result ofanatomical anomalies.
The considerable attachment of thelower cervical nerves to theirsurrounding structures suggests thatpain produced during an ULTT is
OR I GIN A L A Rric LE
unlikely to originate. solely fromneuromeningeal tissue. Many of thestructures to which the lower cervicalnerves are attached are innervated.The sinuvertebral nerve is a mixednerve that is formed from.a somaticroot from a ventral ramus and anautonomic root from a grey ramuscommunicantes {Bogduk 1985). Thesinuvertebral nerve supplies theintervertebral discs, PLL and theperiosteum of the ventrolateral spinalcanal. The zygapophyseal joints receivethe medial branch of a cervical dorsalramus (Bogduk 1985). Theseinnervated structures may also need tobe considered inpatients with apositive ULTT response. Theattachments of the lower cervicalnerves warrant further biomecharucalinvestigation.
ConclusionThe anatomical findings of this studysuggest that the nerves of the lowercervicalspine have numerousattachments to innervated structures intheir course from the spinal cord to theperiphery. The clinical implication isthat these structures, likeneuromeningealtissue, may becomestressed during the ULTT.Neuromeningeal tissue alone may notbe the cause of a positiveULTTresponse. The attachments oEthelower cervical nerves require furtherbiomechanical investigation before theeffects ofthe ULTTcan be fullyunderstood.ReferencesBogduk N (1985): Theinnervation ofthe vertebral
column. Australian Journal.of Physiotherapy31: 89.,.94.
Bonnel F (1984): Microscopic anatomyofthe adulthuman brachial plexus: an anatomical andhistological basis for microsurgery.Microsurgery 5: 107-117.
Carson F (1990): Histotechnology. Selfinstructional text. Chicago: ASCPPress.
Elvey RL (1980): Brachial plexus tension tests andthe pathoanatomical origin of arm pain. InIdozak RM (Ed.): Aspects of ManipulativeTherapy. Melbourne: Lincoln Institute ofHealth Sciences, pp. 105-110.
Elvey RL (1983): The need to test the brachialplexus in painful shoulder and upper quarterconditions. Proceedings of the Neck andShoulder Symposium. ManipulativeTherapists Association ofAustralia. Brisbane,pp.39-52.
ElveyRL (1986): Treatmentofarm pain associatedwith abnormal brachial plexus tension.Australian Journal of Physiotherapy 32: 225231.
Frykholm R (1951): Cervical nerve rootcompression resulring from disc degenerationand root-sleeve fibrosis. A clinicalinvestigation. Acta Chirugia Scandinavica(SuppI160): 1-34.
Frykholm R (1952): Cervical epidural structures,periradicular and epineurial sheaths. ActaChirugia Scandinavica 102: 10-20.
Ginn K (1988): An investigation of tensiondevelopment inupperlimbsoft tissues duringthe upper limb tension test. Proceedings oftheInternational ConferenceofOrthopaedicManipulative Therapists. London, pp. 2526.
HayashiK, Yabuki T, Kurokawa T, Seki H,HogakiM and Minoura S (1977): The anterior andthe posterior .longitudinal ligaments of thelower cervical spine. Journal ofAnatomy 124:633-636.
HerzbergG, Narakas~ComtetJJ, BouchetAandCarretJP (1985): Microsurgical relations ofthe roots of the brachial plexus. Practicalapplications. Annales deChirurgie de la Main4: 120-133.
Kikuchi S, Macnab I and Moreau P (1981):Localisation of the level of symptomaticcervical disc degenerationJournal ofBone andJoint Surgery 63B: 272-277.
Kikuchi S (1982): Anatomical and experimentalstudies ofnerverootinfiltrationJournal oftheJapanese Orthopaedic Association 56: 605-614.
Payne EEand Spillane JD (1957): The cervicalspine. An anatomico.;.pathological study of70specimens (using a special technique) withparticular reference to the problemofcervicalspondylosis Brain 80: 571-596.
Pech P, Bergstrom W,Rauschning and HaughtonVM (1987): Attenuation values, volumechanges and artifacts in tissue due to freezing.Acta Radiologica 28: 779-782.
Selvaramam PJ, GlasgowEFandMatyasTA(1988):Strain effect on the nerve roots of brachialplexus. Journal ofAnatomy 161:260.
ShermanJL, Nassaux PY and Citrin CM(1990):Measurements nfthe normal cervical spinalcord on MR imaging. American Journal ofNeuroradiology 11: 369-372.
SunderlandS (1974a): Meningeal-neural relationsin the intervertebral foramen. Journal ofNeurosurgery 40: 757-763.
Sunderland S (1974b):Mechanisms of cervicalnerve root avulsion in injuries ofthe neckandshoulder. Journal of Neurosurgery 41: 705714.
Sunderland S (1978): Nerve and Nerve Injuries.(2nd ed.) Edinburgh: Churchill Livingstone,pp.870.,.900.
Wilson S, Selvaratnam PJ and .Briggs C (1994):Strain at the subclavian artery during theupper limb tension test. AustralianJournalofPhysiotherapy 40: 243-248.