Embed Size (px)
Citation preview
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D. July, 2003
Visualizing the Venous System: Upper Extremity & Thorax
Heather E. Gunter, Harvard Medical School Year IIIGillian Lieberman, M.D.
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
2
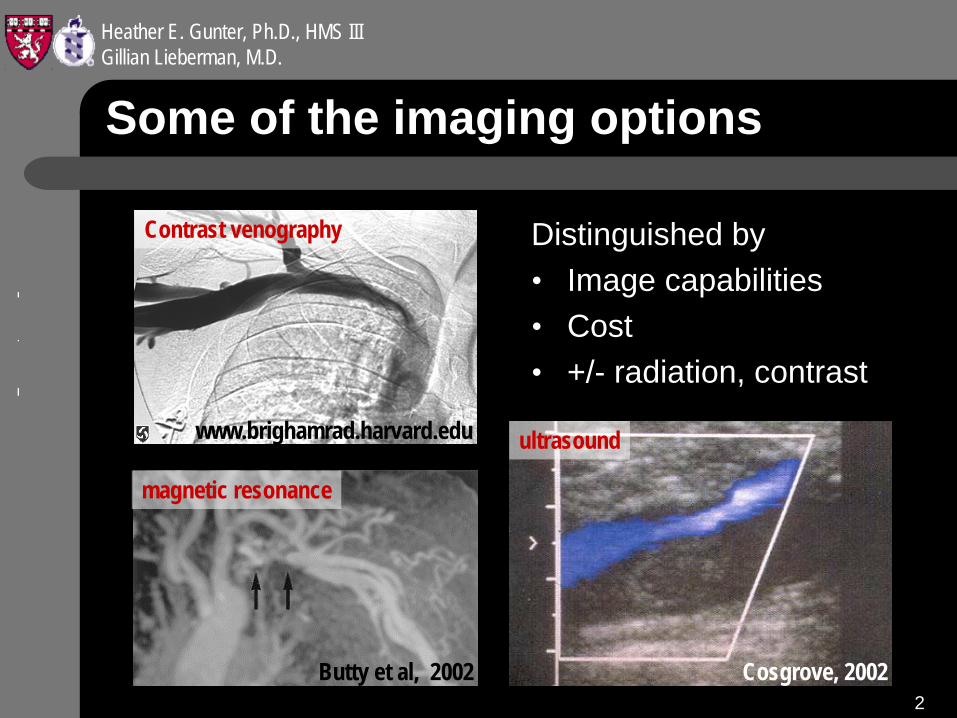
Some of the imaging options
Distinguished by• Image capabilities• Cost• +/- radiation, contrast
www.brighamrad.harvard.edu
Butty et al, 2002 Cosgrove, 2002
Contrast venography
magnetic resonance
ultrasound
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
3
Patient H.V. will guide our discussion
• 52 year old woman with end stage renal failure • Dialysis access through a catheter placed in the
left internal jugular vein since August, 2002
indication: Confirm catheter location in SVC
study:
Chest X-ray
Ultrasound
Trad. venography
MRI
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
4
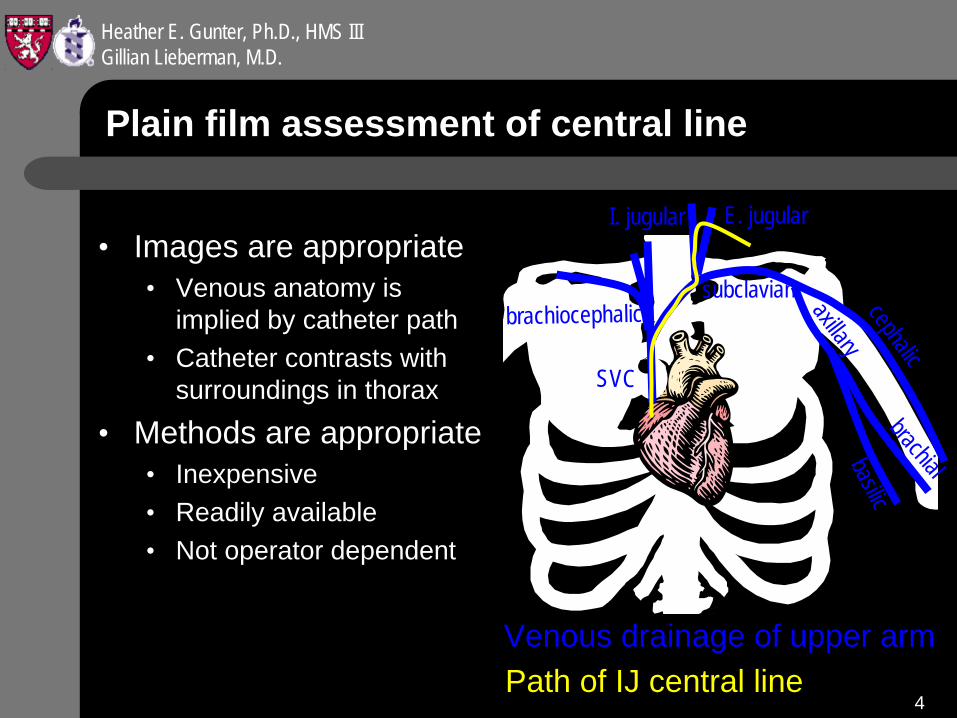
Plain film assessment of central line
• Images are appropriate• Venous anatomy is
implied by catheter path• Catheter contrasts with
surroundings in thorax
• Methods are appropriate• Inexpensive• Readily available• Not operator dependent
cephalic
axillary
subclavian
I. jugular E. jugular
brachiocephalic
SVC
basilicbrachial
Venous drainage of upper armPath of IJ central line
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
5
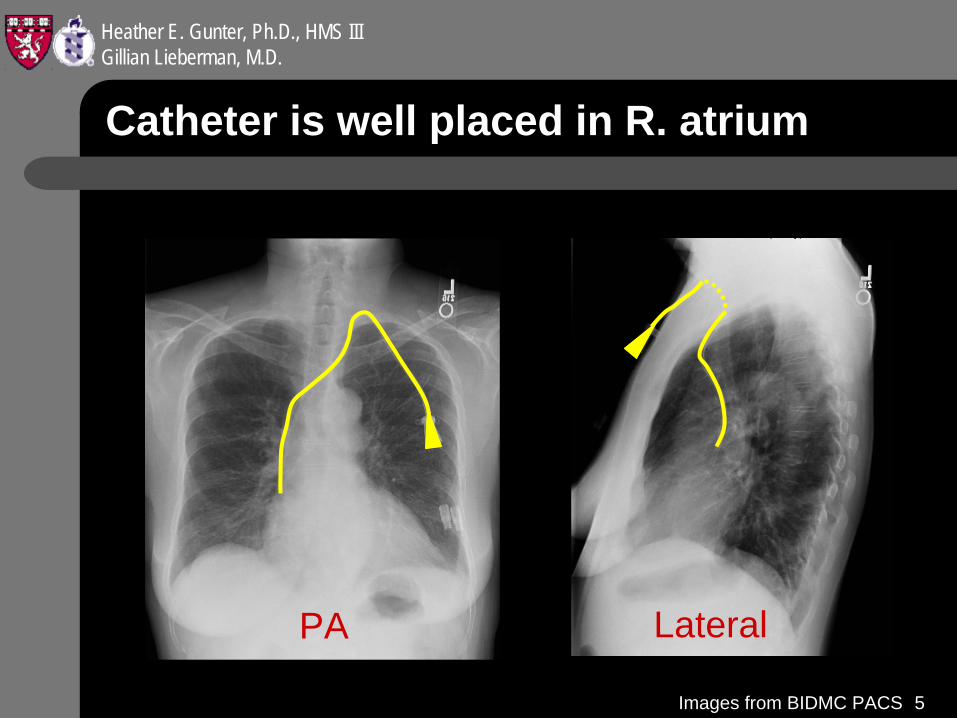
Catheter is well placed in R. atrium
PA Lateral
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
6
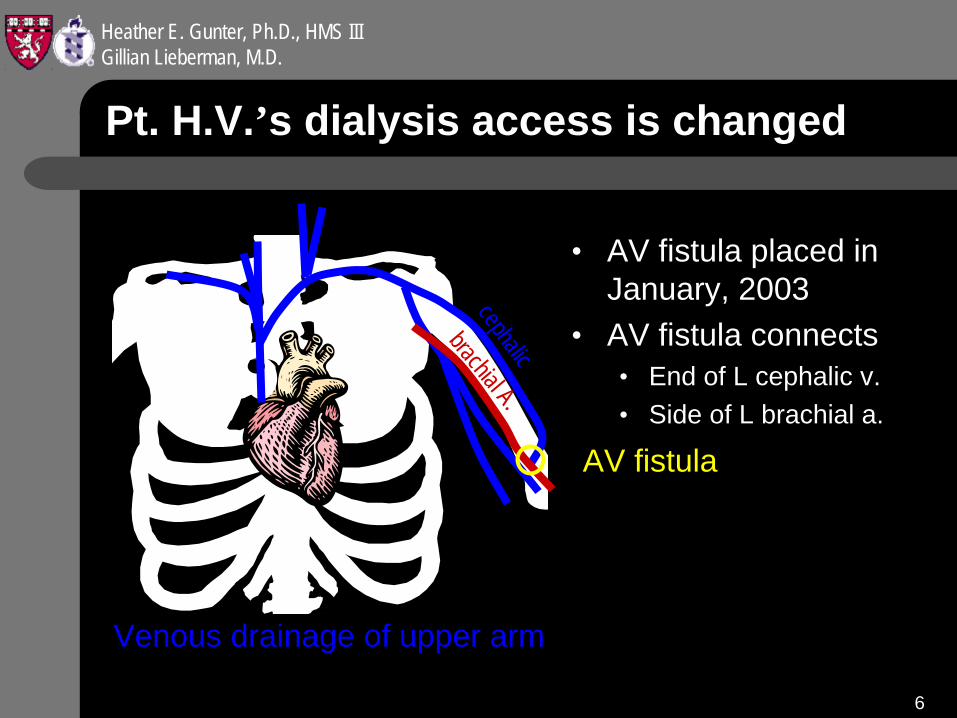
Pt. H.V.’s dialysis access is changed
• AV fistula placed in January, 2003
• AV fistula connects• End of L cephalic v.• Side of L brachial a.
cephalic
Venous drainage of upper arm
brachial A.AV fistula
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
7
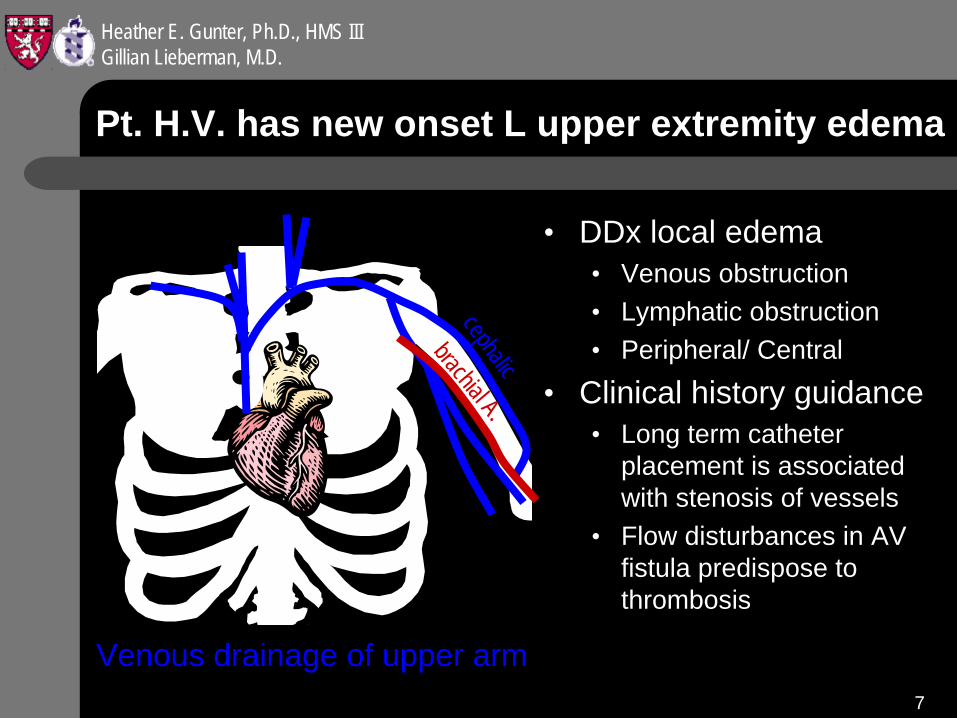
Pt. H.V. has new onset L upper extremity edema
• DDx local edema• Venous obstruction• Lymphatic obstruction• Peripheral/ Central
• Clinical history guidance• Long term catheter
placement is associated with stenosis of vessels
• Flow disturbances in AV fistula predispose to thrombosis
cephalic
Venous drainage of upper arm
brachial A.
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
8
First look for peripheral occlusion
• Turbulence in brachiocephalic AV fistula may have led to thrombotic occlusion
• Catheter placement may have led to stenosis along its path (i.e. left internal jugular vein-)
indication: Evaluate for peripheral venous occlusion
study:
Chest X-ray
Ultrasound
Trad. venography
MRI
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
9
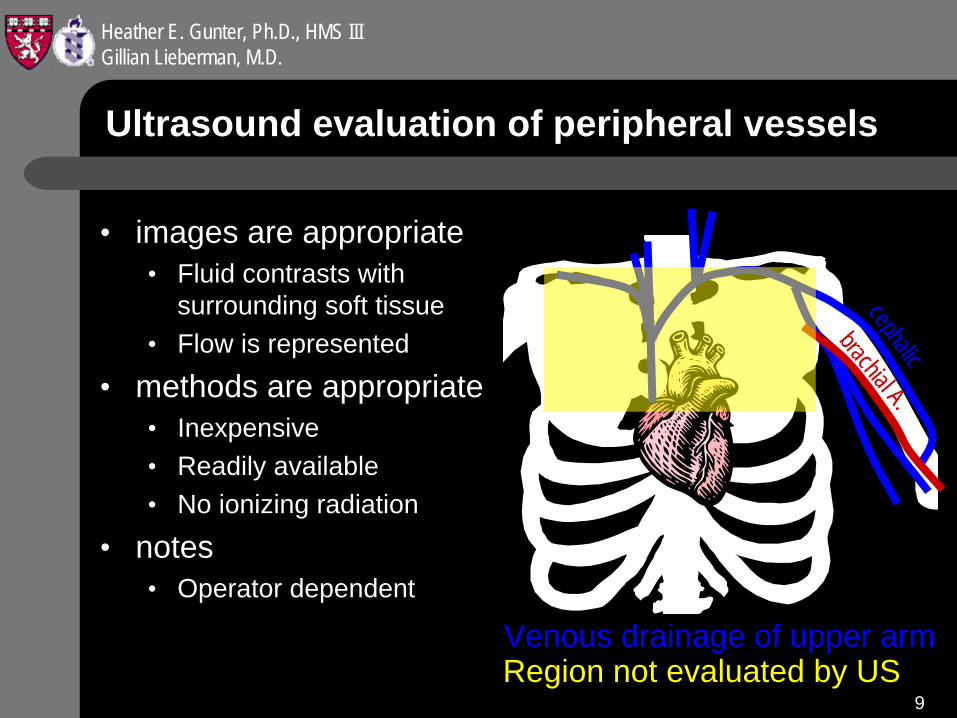
Ultrasound evaluation of peripheral vessels
• images are appropriate• Fluid contrasts with
surrounding soft tissue• Flow is represented
• methods are appropriate• Inexpensive• Readily available• No ionizing radiation
• notes• Operator dependent
cephalic
Venous drainage of upper arm
brachial A.
Region not evaluated by US
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
10
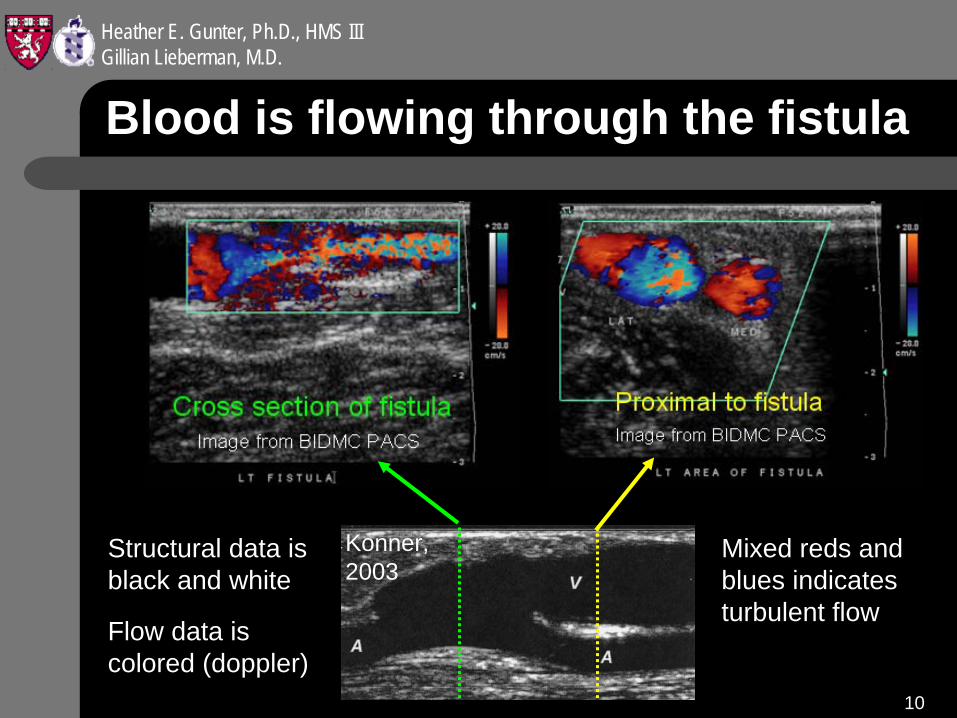
Blood is flowing through the fistula
Konner, 2003
Mixed reds and blues indicates turbulent flow
Structural data is black and white
Flow data is colored (doppler)
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
11
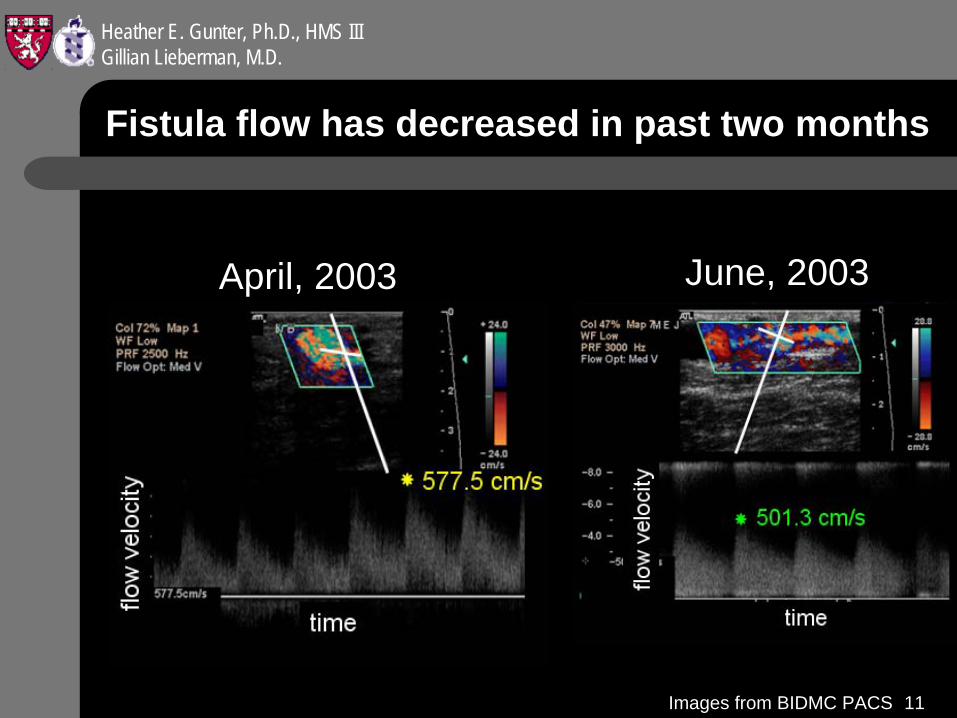
Fistula flow has decreased in past two months
April, 2003 June, 2003
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
12
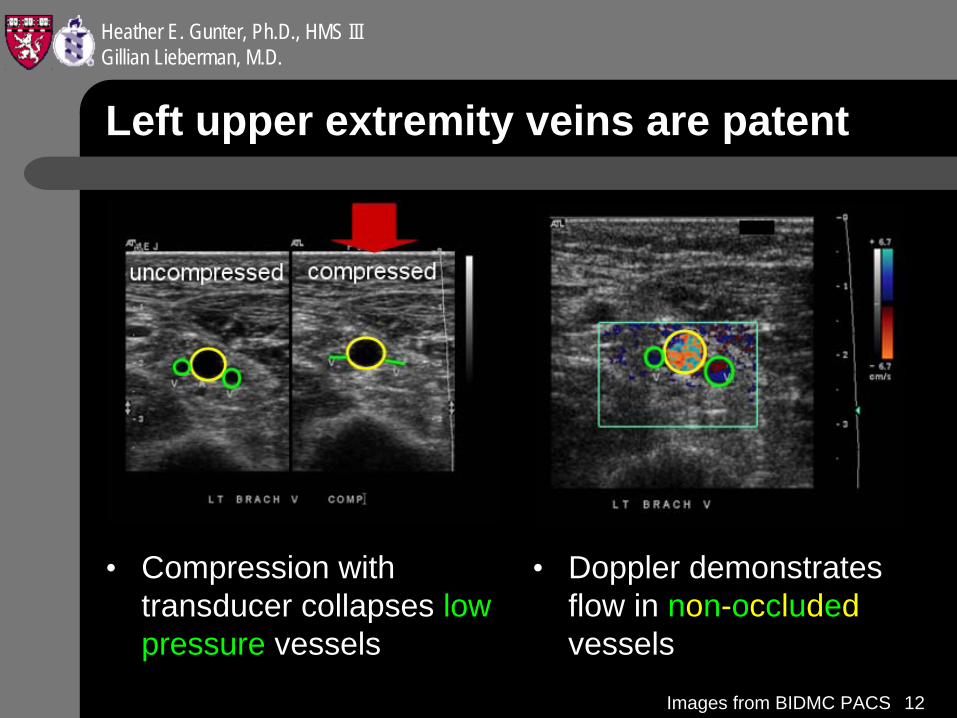
Left upper extremity veins are patent
• Compression with transducer collapses low pressure vessels
• Doppler demonstrates flow in non-occluded vessels
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
13
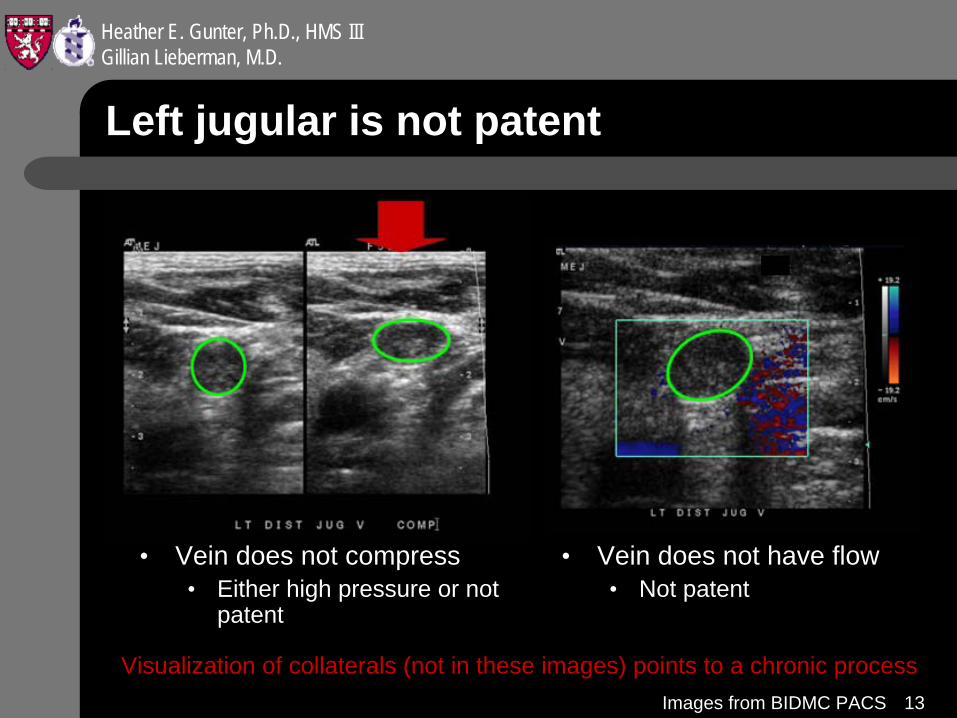
Left jugular is not patent
• Vein does not compress• Either high pressure or not
patent
• Vein does not have flow• Not patent
Visualization of collaterals (not in these images) points to a chronic processImages from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
14
Second, look for central occlusion
• Distal obstruction ruled out with US• US demonstrated blockage in peripheral path of
catheter, which may continue centrally
indication: Evaluate for central venous occlusion
study:
Chest X-ray
Ultrasound
Trad. venography
MRI
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
15
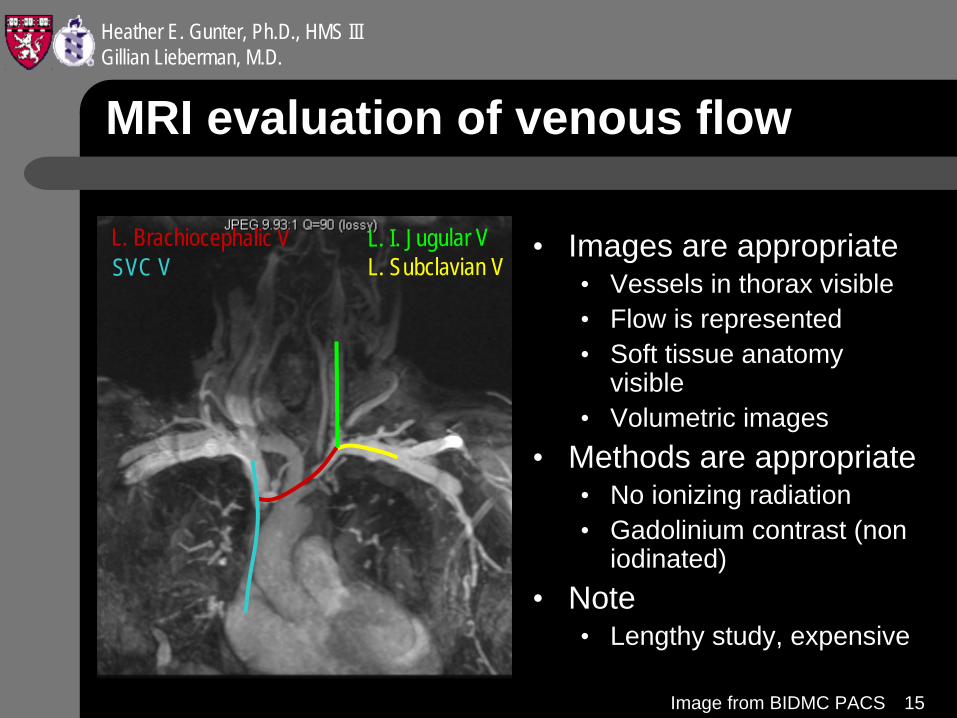
MRI evaluation of venous flow
• Images are appropriate• Vessels in thorax visible• Flow is represented• Soft tissue anatomy
visible• Volumetric images
• Methods are appropriate• No ionizing radiation• Gadolinium contrast (non
iodinated)• Note
• Lengthy study, expensive
L. Subclavian VL. I. Jugular VL. Brachiocephalic V
SVC V
Image from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
16
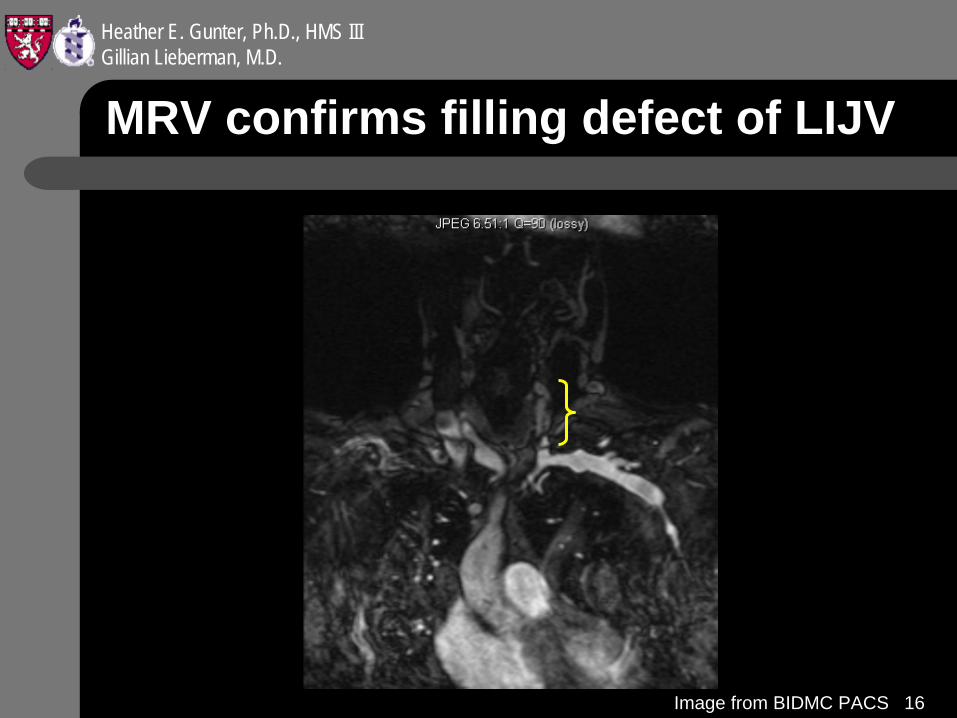
MRV confirms filling defect of LIJV
Image from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
17
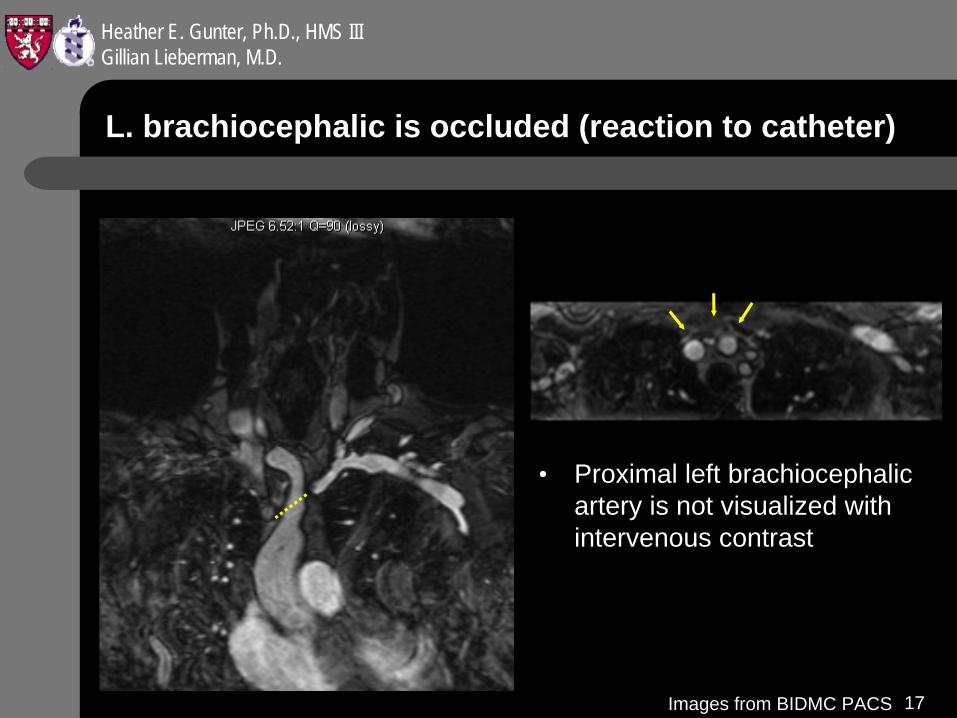
L. brachiocephalic is occluded (reaction to catheter)
• Proximal left brachiocephalic artery is not visualized with intervenous contrast
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
18
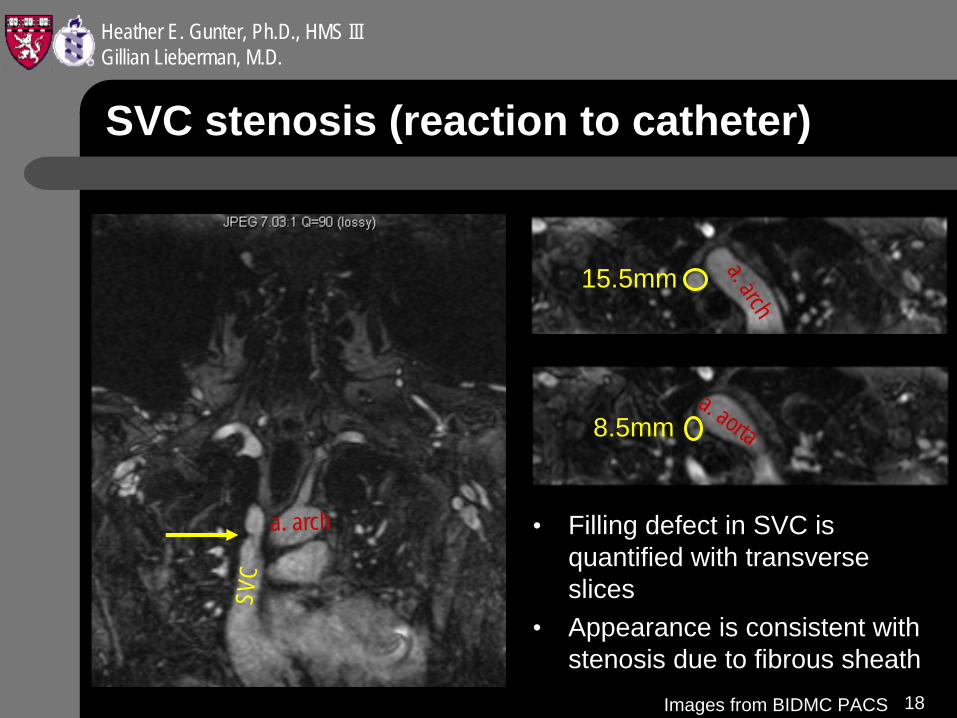
15.5mm
8.5mm
SVC stenosis (reaction to catheter)
• Filling defect in SVC is quantified with transverse slices
• Appearance is consistent with stenosis due to fibrous sheath
a. arch
a. aorta
SVC
a. arch
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
19
Recanalization of LBCV to improve circulation
Fibrous reaction to previous catheter placement has resulted in a L. brachiocephalic occlusion and SVC stenosis.
indication: Recanalize the obstructed vein
study:
Chest X-ray
Ultrasound
Trad. venography
MRI
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
20
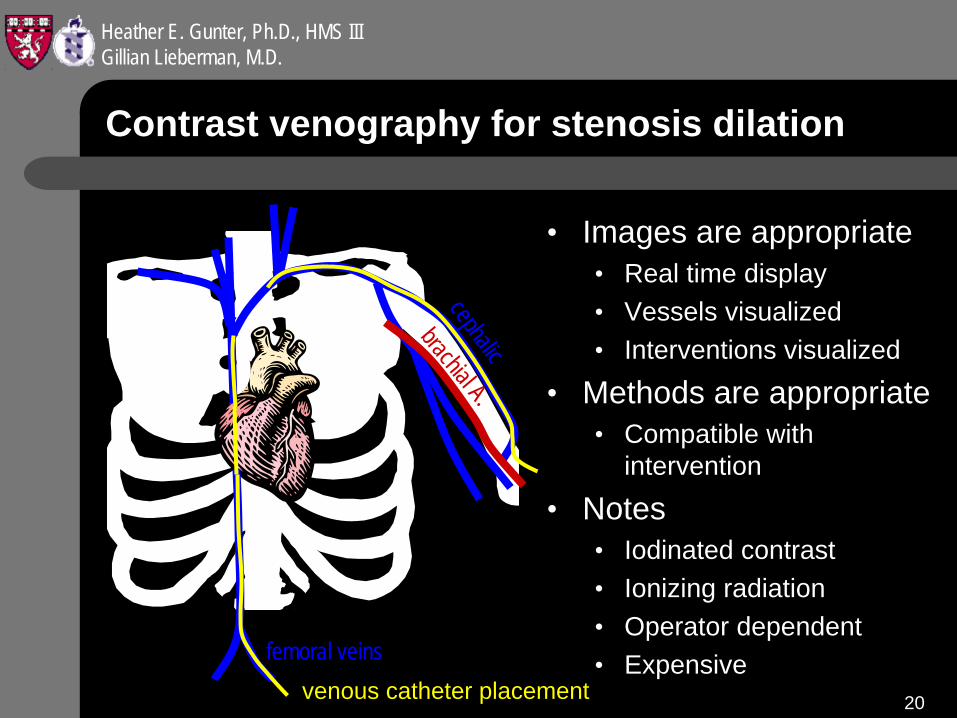
Contrast venography for stenosis dilation
• Images are appropriate• Real time display• Vessels visualized• Interventions visualized
• Methods are appropriate• Compatible with
intervention
• Notes• Iodinated contrast• Ionizing radiation• Operator dependent• Expensive
cephalic
brachial A.
femoral veinsvenous catheter placement
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
21
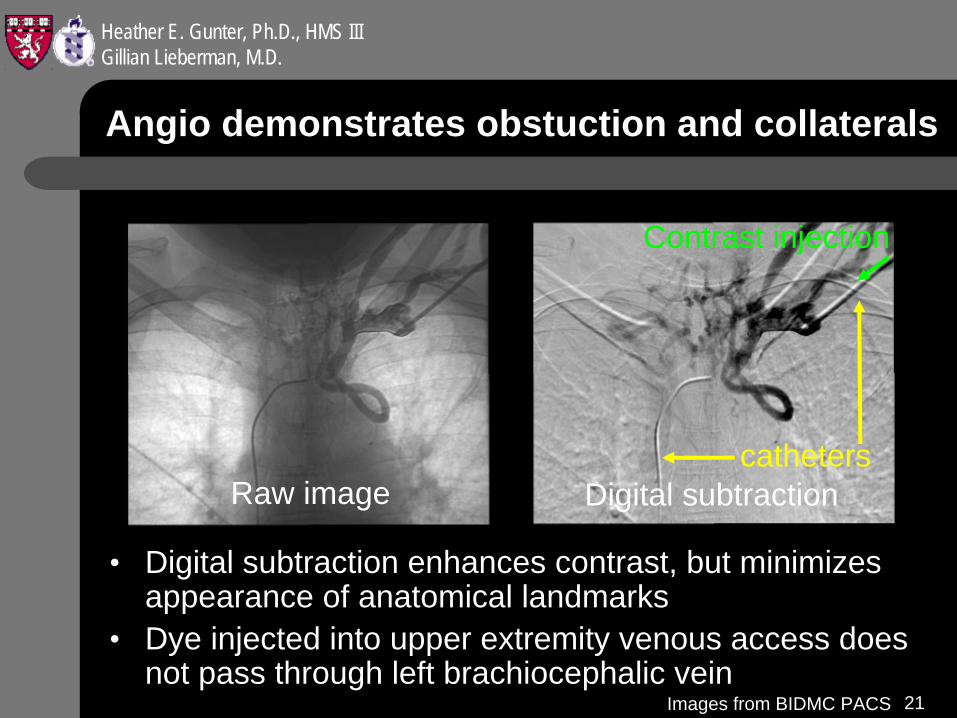
Angio demonstrates obstuction and collaterals
• Digital subtraction enhances contrast, but minimizes appearance of anatomical landmarks
• Dye injected into upper extremity venous access does not pass through left brachiocephalic vein
Digital subtractionRaw imagecatheters
Contrast injection
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
22
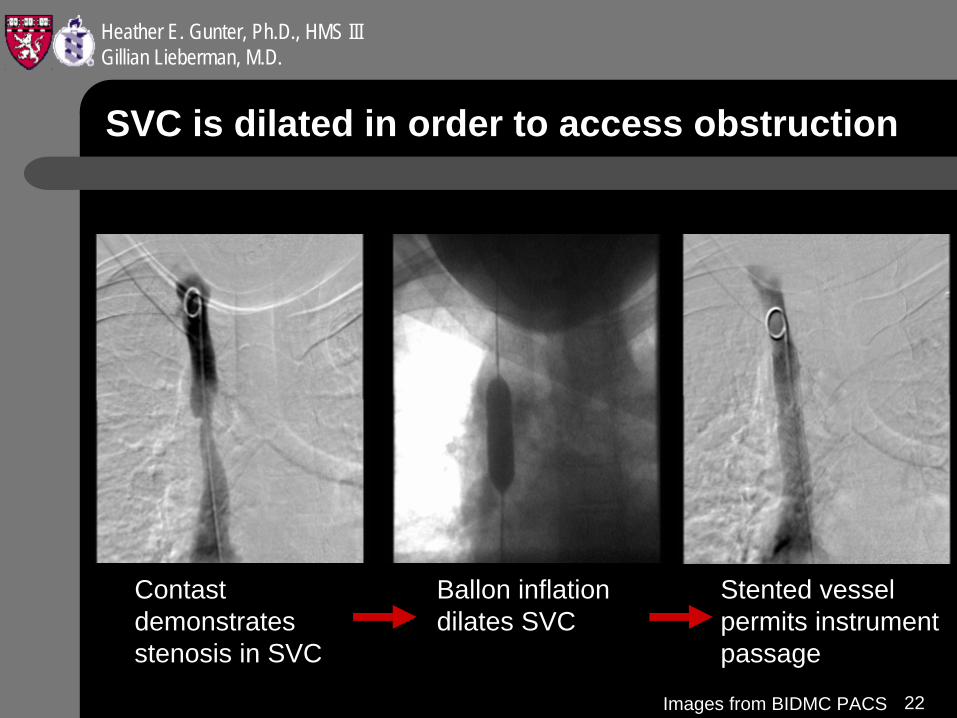
SVC is dilated in order to access obstruction
Contast demonstrates stenosis in SVC
Ballon inflation dilates SVC
Stented vessel permits instrument passage
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
23
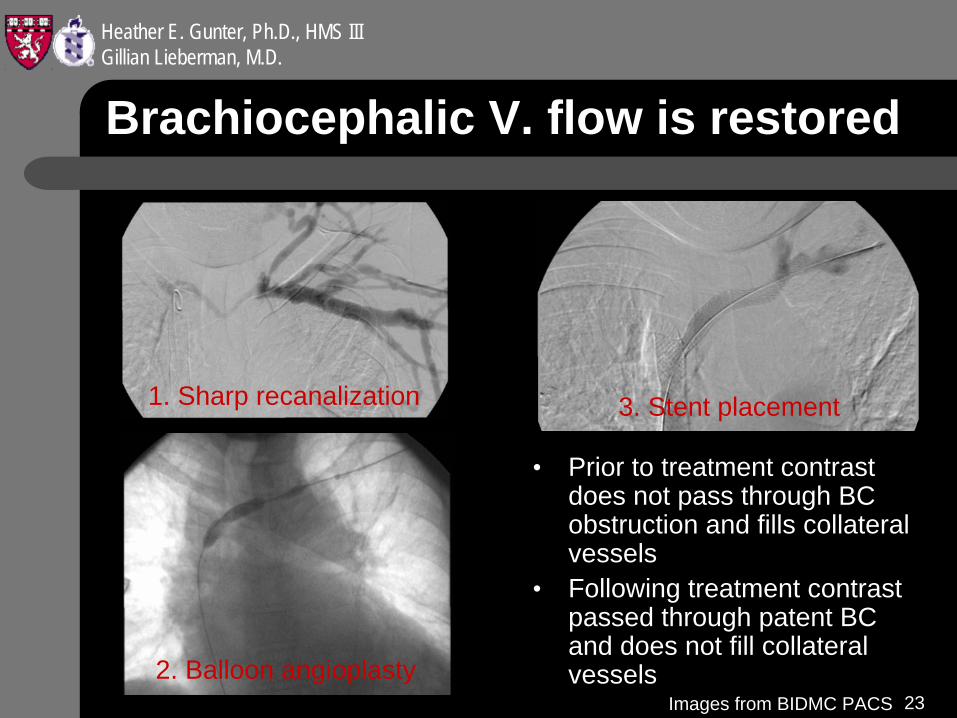
Brachiocephalic V. flow is restored
• Prior to treatment contrast does not pass through BC obstruction and fills collateral vessels
• Following treatment contrast passed through patent BC and does not fill collateral vessels
1. Sharp recanalization
2. Balloon angioplasty
3. Stent placement
Images from BIDMC PACS
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
24
Patient H.V. follow up
• L upper extremity edema resolved following recanalization procedure
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
25
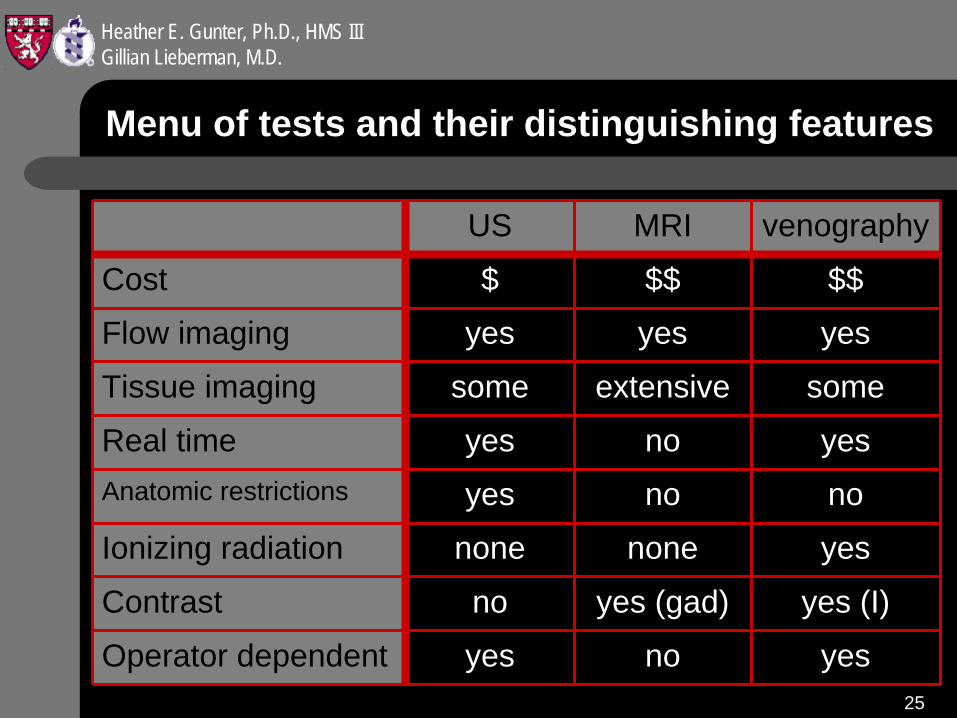
Menu of tests and their distinguishing features
US MRI venography
Cost $ $$ $$
Flow imaging yes yes yes
Tissue imaging some extensive some
Real time yes no yesAnatomic restrictions yes no no
Ionizing radiation none none yes
Contrast no yes (gad) yes (I)
Operator dependent yes no yes
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
26
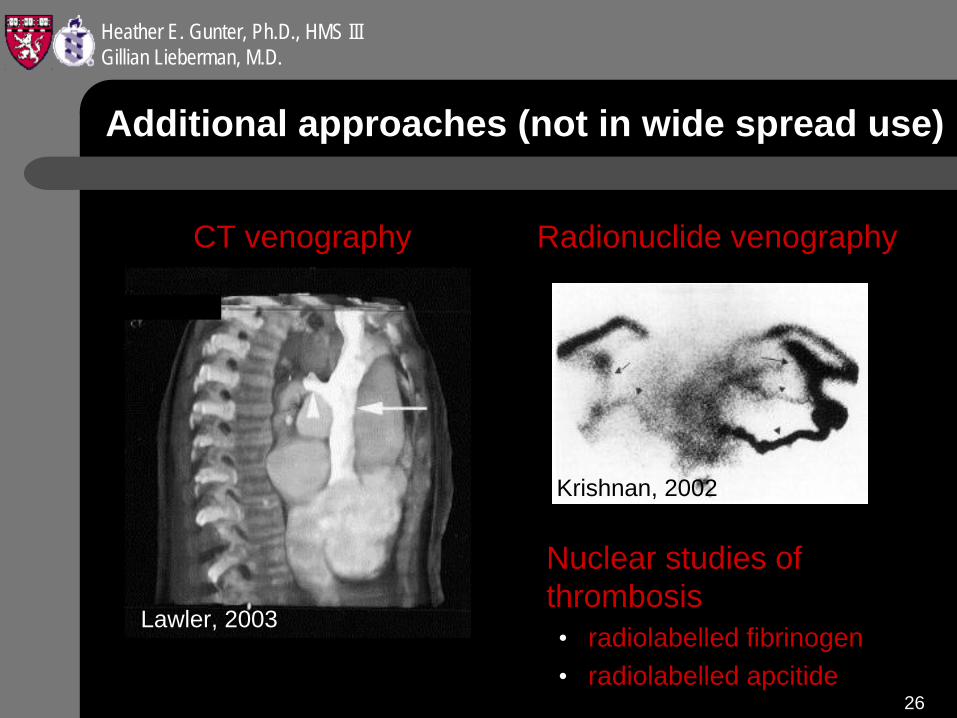
Additional approaches (not in wide spread use)
Nuclear studies of thrombosis• radiolabelled fibrinogen• radiolabelled apcitide
Lawler, 2003
Radionuclide venographyCT venography
Krishnan, 2002
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
27
References
• (1999). The diagnostic approach to acute venous thromboembolism. Clinical practice guideline. Am J Respir Crit Care Med 160:1043
• Butty, S. et al. (2002). Body MR venography. Rad Clin N Am. 40 (4) 899- 919.
• Konner, K. (2003). The arteriovenous fistula. J Am Soc Nephrol. 14(6): 1669-80.
• Krishnan, P. (2002). Venous dilatation seen on routine mammography: a clue to superior vena cava obstruction. Chest 121(4): 1361-3.
• Lang, E. et al. (2003). Sharp racanalization for chronic central venous occlusions. In From Bench to Bedside: Emergency Revascularization.
• Lawler, L.P. (2003). Thoracic venous anatomy: multidetector row CT evaluation. Radiol Clin North Am. 41(3): 545-60.
• Meire, H., & Cosgrove D., (2001). Vascular Ultrasound. in Cosgrove in Grainger & Allison’s Diagnostic Radiology: A Textbook of Medical Imaging, 4th Ed. pp. 59-80.
Heather E. Gunter, Ph.D., HMS IIIGillian Lieberman, M.D.
28
Acknowledgements
• Phoebe Lewit Olhava, M.D.• Elvira Lang, M.D.• Pamela Lepkowski• Larry Barbaras