Embed Size (px)
Citation preview

Updates in Obstructive Sleep Apnea
Rose A. Franco, MD, FCCPAssociate Professor Pulmonary, Critical Care and Sleep MedicineMedical College of Wisconsin

Disclosures• I have no conflicts to disclose

OBJECTIVES• Review OSA prevalence, update statistics• Discuss Comorbid conditions• Discuss state of art pathophysiologic mechanisms • Review American Society Anesthesiology recommendations for
screening• Discuss evidence around CPAP for medical conditions• Discuss evidence of cpap for risk reduction in perioperative
care
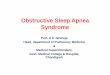
MILD OSA: Apnea Hypopnea index (AHI) >5 + symptoms
MODERATE OSA: Apnea Hypopnea index >15
SEVERE OSA: Apnea Hypopnea index >30
Epstein. J Clin Sleep Med. 2009
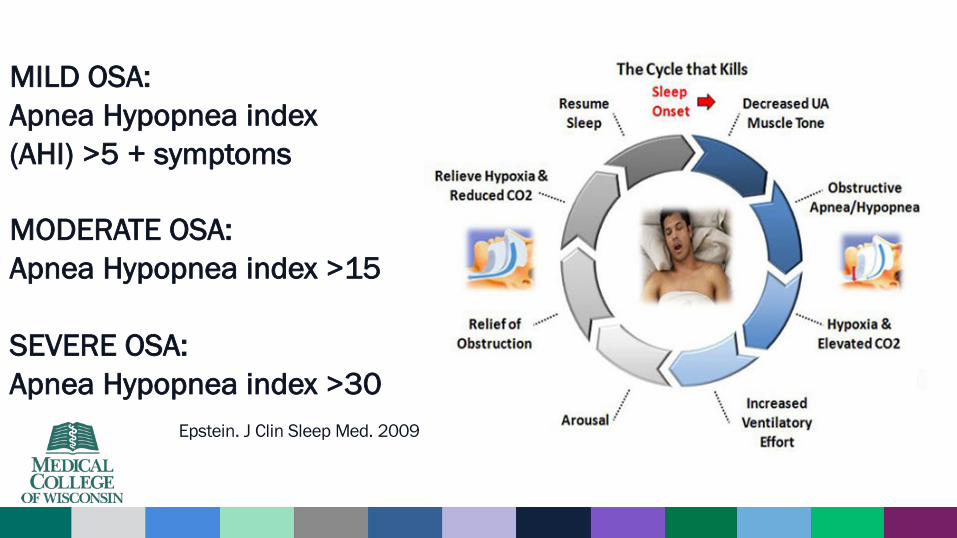
United States Prevalence of OSA• Using AHI >5
– 20-30% men, 10-15% women in US• Using AHI >5 with symptoms or AHI >15
– 15% men, 5% women in US• Ethnicity plays a role
– Higher AHI, AA males age <39 vs. Caucasians of same age• Age
– steady increase in prevalence with age up to about age 60 with plateau• Gender
– Men 2-3 times more likely that women
Young. WMJ 2009Redline. Am J Respir Crit Care Med 1997Peppard. Am J Epidemiol 2013

Population HEALTH burden of OSA
National Health and Nutrition Examination Survey (NHANES) BMI data combine with data from the North American Sleep study cohort • In 20 years (1990 to 2010)
Overall prevalence of OSA has increased from 11% to 14%
• Young T. WMJ 2009; 108:246.

Major RISK FACTOR: WEIGHT• 2010 Prospective study over 4 years in 700 subjects:
Increasing weight by 10% =6 fold increase in risk for OSAPepperd JAMA 2000
• 2010 Population based study with Polysomnography: 1000 people with Moderate to Severe OSA
BMI ORNormal 1Overweight 2.6Obese 10.5
Tufik. Sleep Med. 2010
• 2015, retrospective review of Obese with Hypoxemia, – 80% had OSA.
Povitz. Ann Am Thorac Soc 2015
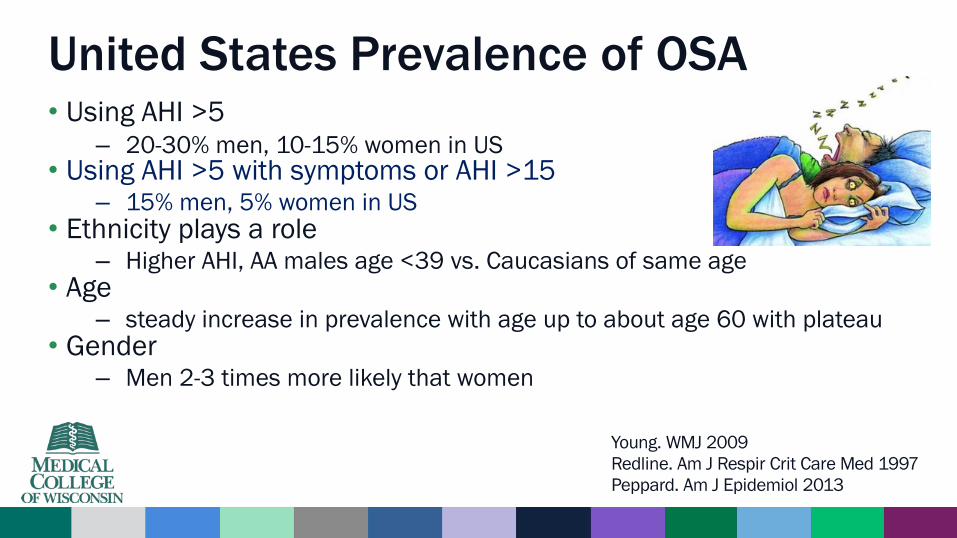
High Prevalence of OSA: COMORBID CONDITIONS
• Atrial Fibrillation 32-49% (5 X)• Coronary Artery Disease 30% (11X M/M post MI)• Hypertension 35-80%*• Congestive Heart Failure 12-53%• Stroke and TIA 60% (1.76 X mortality) • Diabetes (type 2) 50%• Polycystic Ovary Syndrome 30X• Chronic lung diseases 2X
CONDITION OSA PREVALENCEGami.Nat Clin Pract Cardiovasc. 2005Mehra. AJRCCM 2006Peker. ERJ 1999. Young. Sleep 2008Sjostrom. Thorax. 2002Yumino. J Card Fail. 2009Ferrier Chest 2005Vazir Eur J Heart Fail. 2007Yumino. Cardiol. 2007Gottlieb. Circulation 2010Kaneko. Sleep 2003Einhorn. Endocr Pract 2007Heffner Chest 2012.Greenberg-Dotan. Sleep and breathing 2014Vgontsez. J Clin Endocrine Metab. 2001.Sahlin. Arch Intern Med. 2008.

ASSOCIATION VS CAUSATION?
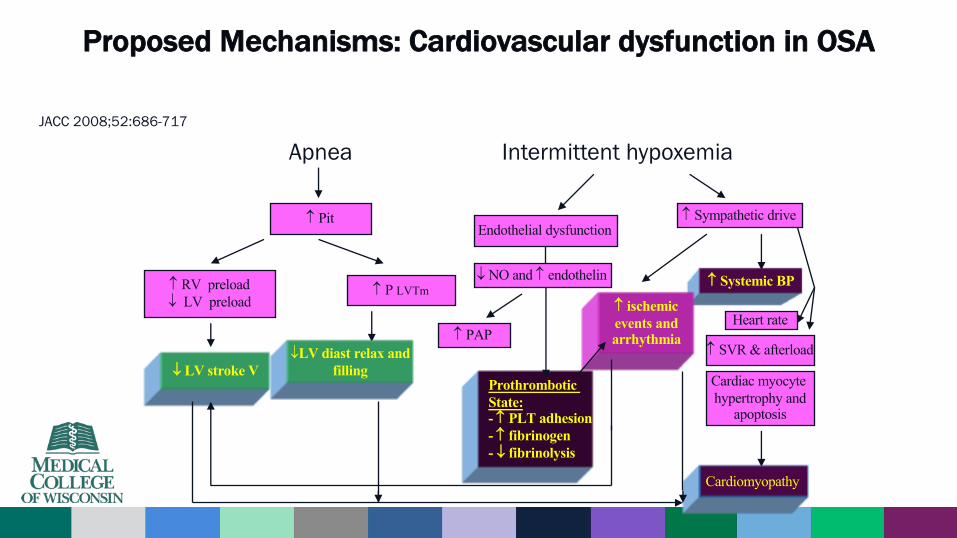
Proposed Mechanisms: Cardiovascular dysfunction in OSA
Apnea Intermittent hypoxemia
Pit
RV preload¯ LV preload
P LVTm
¯ LV stroke V¯LV diast relax and
filling
Sympathetic drive
Systemic BP
Heart rate
SVR & afterload
Cardiac myocyte hypertrophy and
apoptosis
Cardiomyopathy
ischemic events andarrhythmia
Endothelial dysfunction
¯ NO and endothelin
PAP
ProthromboticState:- PLT adhesion- fibrinogen - ¯ fibrinolysis
JACC 2008;52:686-717
0.7
0.8
0.9
1.0
Surv
ival
Pro
babi
lity
0 1 2 3 4 5 6 7 8 9 10Years
< 5.05.0 – 14.9
15.0 – 29.9> 30.0
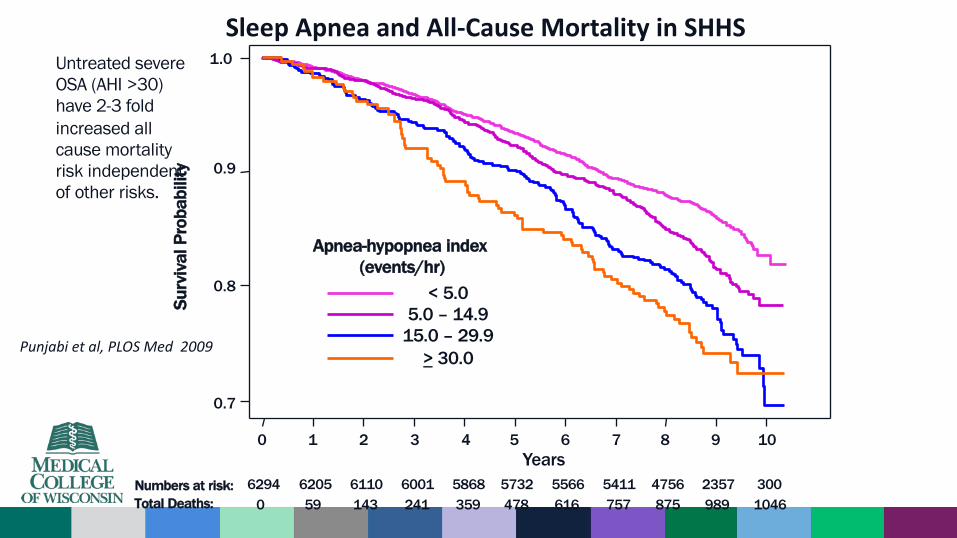
Numbers at risk: 6294 6205 6110 6001 5868 5732 5566 5411 4756 2357 300Total Deaths: 0 59 143 241 359 478 616 757 875 989 1046
Apnea-hypopnea index (events/hr)
Sleep Apnea and All-‐Cause Mortality in SHHS
Punjabi et al, PLOS Med 2009
Untreated severe OSA (AHI >30) have 2-3 fold increased all cause mortality risk independent of other risks.
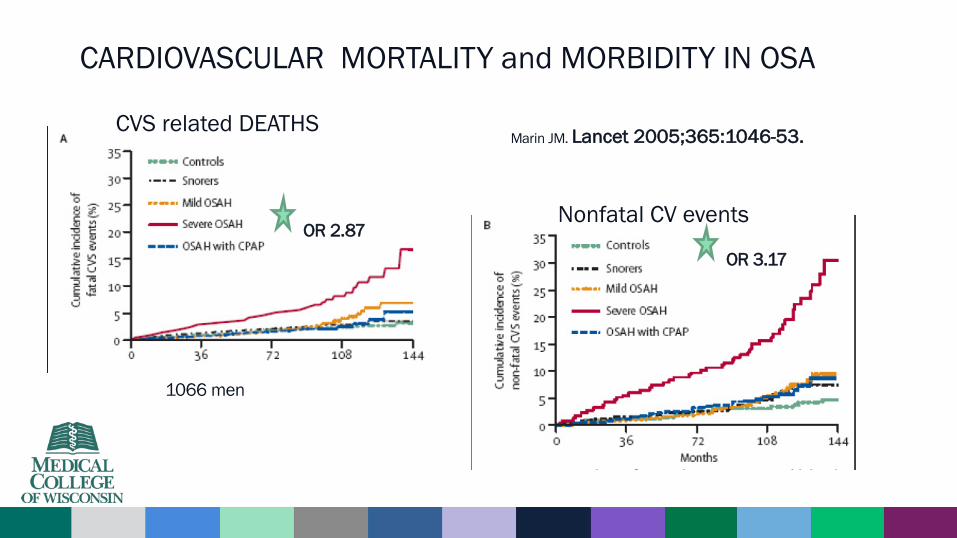
1066 men
Marin JM. Lancet 2005;365:1046-53.
CARDIOVASCULAR MORTALITY and MORBIDITY IN OSA
OR 3.17OR 2.87
CVS related DEATHS
Nonfatal CV events

Sleep Apnea
Intermittent HypoxiaSleep Fragmentation
Increased. Catecholamines
Increased Cortisol
Increased. IL-6, and TNF alpha
Increased LeptinFall in adiponectin
Beta cell dysfunctionInsulin resistance
Glucose intolerance
Metabolic consequences

Diabetes association to OSA
• Type 2 Diabetes and OSA– Animal and Human experimental models
• Intermittent hypoxemia plus sleep fragmentation provide evidence of alteration in glucose metabolism– Baud. J Sleep Res. 2013;22:3-12– Liyori. Am J Respir Crit Care Med 2007;175:851-857.– Stamatakis. Chest 2010; 137:95-101
– INCIDENT DIABETES in SEVERE OSA (AHI >30) 30% higher risk • Of 736 men followed, 9% developed diabetes over 4 years
• Kendzerska T. Am J Respir Crit Care Med 2014; 190:218.

Schematic diagram summarising the functional consequences of visceral obesity in adipocytes, skeletal muscle, the liver and the vessel wall.
M.R. Bonsignore et al. Eur Respir J 2012;;39:746-767
OSA association with Nonalcoholic fatty liver diseaseMeta-analysis of 18 studies with >2000 subjects• OSA present
– 2-3 fold increased risk for NAFLD – independent from age, weight, gender.
• Musso G. Obes Rev 2013; 14:417.
• OSA + higher Transaminases, higher prevalence of NAFLD and fibrosis• Sookoian, Pirola. Obes Surg 2013; 23:1815.
Proposed mechanism• Intermittent hypoxia causes hypoxia inducible factor 1 and 2 (HIF-1, HIF-2), nuclear factor-
kappa B, unfolding protein response and hypoxic adipose tissue inflammation leading to unchecked inflammation.
• Türkay C. Respir Care 2012; 57:244.• Minville C. Chest 2014; 145:525.

OSA and Perioperative riskUsing ICD-9 codes in surgical patients—
– OSA prevalence 7-10%.
UNDIAGNOSED OSA is common.– Cardiac surgery 48%– Bariatric Surgery 70%
Memtsoudis. Anesth Analg. 2014;118:407-18.Mokhlesi. Chest 2013;144:903-14.Frey. Obes Surg. 2003;13:676-83.Hallowell. Am J Surg. 2007;193:910-916.

PERIOP Cardiopulmonary complications with OSA• 2012, 2013 meta-analyses
– INCREASED periop Cardiac complications• Myocardial Infarction • Cardiac arrhythmias (esp Atrial fibrillation)
• 2011 database review of 6 million surgical cases– INCREASED Respiratory complications
– General Surgery• Intubation/Mechanical Ventilation rates almost DOUBLE (10.8 vs 5.94%)• Aspiration Pneumonia (2.79 vs 2.05%)• Acute respiratory distress syndrome (3.79 vs 2.44%).
• 2014 meta-analysis 17 studies – OR 2.4 for acute respiratory failure– OR 2.46 ICU transfers– OR 1.63 Cardiac events
Kaw R, et al. Br J Anaesth 2012Memtsoudis, Anesthe Analg. 2011Hai et al. J Clin Anesth. 2014

ADDITIONAL Periop Risks in OSA
• Acute Renal Failure (OR 2.43)•Wound hematomas/seromas (OR 1.36)• Delirium postoperatively (OR 4.3)• ICU transfer (OR 2.81)
• Longer hospital stay 6.8 vs 5.1 days for joint arthroplasty
2012 meta-analysis (Kaw R, et al. Br J Anaesth 2012)
2012 J. Arthroplasty. D’Apuzzo et al.
2012 Anesthesiology. Flink et al.
PERIOPERATIVE MEDICINE: NEW STANDARDS • OSA Preoperative screening is recommended
– by the American Society of Anesthesiologists, the American Academy of Sleep Medicine, and other international health safety organizations
• Most critical populations are:– OBESE (BMI >30)– Those undergoing bariatric surgery– Those with history of difficulty intubation or upper airway anatomy predicting
difficulty intubation*– Medical Comorbidities with high association with OSA:
• Diabetes• Hypertension• Congestive Heart Failure• Stroke• Hypothyroidism

QUICK SCREEN: STOPBang• Do you SNORE loudly?• Do you often feel TIRED, fatigued, or sleepy during the daytime?• Has anyone OBSERVED you stop breathing (obstruction) during
your sleep?• Do you have or are you being treated for high blood
PRESSURE?• Are you obese/ very overweight – BMI more than 35
kg/m2?• AGE over 50 years old?• NECK Circumference >16 inches?• Are you male (GENDER)?
Chung F et al Anesthesiology 2008 and BJA 2012
>3 buys a screening test

Are we making a difference with CPAP

Benefits of CPAP for Hypertension
Yes Maybe• Meta-analysis finds reduction Net
-2.6 mmHg • Treatment Resistant HTN may
benefit (MAP & DBP -3.2mmhg)• Severe OSA (hypoxemia) more
likely to show improved BP• Longer trials demonstrate benefit
(36 months)
Not really• Only seemed to help those with
coexisting uncontrolled HTN• No change in SBP in same
population• Trials are too short (2-3 months) to
see benefit of combination therapy• Population heath benefit
extrapolated from medication studies
Fava. CHEST 2014;145:762.Becker Circulation 2003;107:68-73.Duran-Cantolla. BMJ 2010;341:c5991Barbe Am J Resp Crit Care Med. 2010;181:718-726Robinson. Eur Respir J. 2006;27:1229-1235

Benefits in Coronary Artery Disease and CPAP
Yes Maybe
• Longer terms studies, decrease in fatal and nonfatal events on cpapover 10 years
• CPAP can alleviate ischemic changes on EKG, reduce nocturnal angina
Not really
• No randomized trials.
Marin. Lancet 2055;365:1046Milleron. Eur Heart J. 2004;25:728-34.Cassar. J Am Coll Cardiol. 2007;50:1310-14.
Benefits in Heart Failure and CPAP
Yes Maybe
• Improves LVEF by 5%• Improves walk distance, and
catecholamine levels.
Not really
• No difference in overall survival• Treating treatment emergent CSA
with Adaptive Servo Ventilation increased all cause mortality (30 vs 24%)
Bradley. N Engl J Med 2005;353)2025Mansfield. Am J Respir Crit Care Med 2004; 169:361.Cowle. N Engl J Med 2015; 373:1095.
Benefits in Atrial Fibrillation and CPAP
Yes Maybe
• Cardioversion failure reduced by 50%
(82 vs 42%)• CPAP use with Ablation (pulmonary
vein isolation) reduced recurrence (63 vs 28%)
• Higher arrhythmia free survival rate off meds
(66 vs 33%)
Not really
• Observational studies
• Need prospective studies.
Ghias. J AM Coll Cardiol. 2009;54:2075-83Ng Am J Cardiol. 2011;108:47-51.Hoyer. J Interv. Card. Electrophysiol. 2010;29:37-42Kanagala. Circulation. 2003;107:2589-2594.

CPAP benefits for Diabetes
Yes maybe
• Nondiabetics improve glucose tolerance with cpap• Short term study improved
glucose tolerance in PREdiabetes
Not really
• No consistent improvement in glucose control in DM•Well designed long term
studies are needed
Yang. Sleep Breath. 2013;17:33-38.Iftikhar. Lung 2012; 190:605-11.Hecht. Ger Med Sci. 2011;9:Doc 20.Pamidi. Am J Respir Crit Care Med. 2015;192:96-105.

OSA PERIOPERATIVE RISK and CPAP
Yes Maybe
• Meta-analysis. Decreased rate of ICU/respiratory events. NNT 45• Decrease atrial arrhythmia• Decreases rostral fluid shifts• Offsets effects of
sedatives/narcotics on airway tone• Shorter hospital stay (0.4 days)
Not really
• Risk most pronounced 3 days after operation• No study confirms negative
effect specific to OSA patients• Adherence in postop period is
low
Nagappa. Anesth Analg. 2015;120:1013-1023Ferreyra GP Ann Surg.2008;247(4):617-626.

Take Home points• OSA prevalence is on the rise
• Comorbid medical conditions increase likelihood OSA
• Severe OSA is associated w. CV morbidity and mortality
• Diabetes, like metabolic syndrome more common in OSA
• Severe OSA look for NALD, risk for progression to cirrhosis
• Preoperative assessment for OSA now a new MANDATE
• Medical Benefits from Treatment best established in severe sleep apnea

Thank you