Embed Size (px)
Citation preview

Updates in Colorectal Cancer Screening & Prevention
Swati G. Patel, MD MSAssistant Professor of Medicine
Division of Gastroenterology & HepatologyGastrointestinal Cancer Risk and Prevention ClinicUniversity of Colorado Anschutz Medical Center

Disclosures
• None

Objectives
• Review colorectal cancer epidemiology
• Understand colorectal cancer screening options and recommendations
• Understand risk of colorectal cancer based on family history

A few patients…
• I am healthy! I have no symptoms or problems. I don’t think I could have colon cancer.
• I don’t ever want a colonoscopy. Is there another test I can do instead?
• Colonoscopy is too risky for me!!

Colorectal Cancer Incidence & Mortality

Colorectal Cancer Symptoms
•Change in bowel habits/stool caliber
•Blood in stool
•Unintentional weight loss
•Fatigue
•Iron deficiency anemia
•Abdominal pain
NONE!!
•Change in bowel habits/stool caliber
•Blood in stool
•Unintentional weight loss
•Fatigue
•Iron deficiency anemia
•Abdominal pain
NONE!!

Colorectal Cancer Pathogenesis
10-15 years

Importance of Screening

Who Should Get Screened for CRC?


Colorectal Cancer Screening

Colorectal Cancer Screening Options
Stool-based tests
Fecal occult blood testing (FOBT)
Fecal Immunochemical Testing (FIT)
Stool DNA (Cologuard)
Structural Tests
CT Colonography
Barium Enema
Flexible Sigmoidoscopy
Colonoscopy

Colorectal Cancer Screening & Prevention
Structural Test
Stool-Based Test

Colorectal Cancer Screening Options
Stool-based tests
Fecal occult blood testing (FOBT)
Fecal Immunochemical Testing (FIT)
Stool DNA (Cologuard)
Structural Tests
CT Colonography
Barium Enema
Flexible Sigmoidoscopy
Colonoscopy

Stool-Based Tests
• Detect microscopic blood in the stool
• Performed annually
• If positive colonoscopy
• FOBT– Non-specific (human vs non-human
hemoglobin; location in GIT)– Dietary (red meat, poultry, fish, raw
vegetables) & medication restriction (NSAIDs)
– Three successive smears
• FIT– Human globin– No restrictions– Single sample

Stool-Based Testing Performance
Sensitivity CRC
SensitivityAdenoma
Cost Compliance
Hemoccult II 13% - 50% 8% - 20%
Hemoccult SENSA 50% - 79% 21% - 35% $13 49.5%
FIT 75 % - 80% 15% - 44% $28 61.5%

Stool-Based Testing EfficacyTrial Screening Follow-up
(years)N CRC Incidence CRC Mortality All-Cause
Mortality
Nottingham Scholefield et al. 2002
Biennial 11.7 152,303
1.51 vs 1.53/1000 person yr NS 0.87 (0.78-0.97, p=0.010) 1.01 (0.96-1.05) NS
Funen Kronborg et al. 2004
Biennial 17 61,939 1.02 (0.93-1.12) NS 0.84 (0.73-0.96, p<0.05) 0.99 (0.97-1.02) NS
Goteborg Lindholm et al. 2008
Biennial 15.75 23,916 0.96 (0.86-1.06) NS 0.84 (0.71-0.99, p<0.05) 1.02 (0.99-1.06) NS
Minnesota Mandel et al. 1999, 2000
Annual (A) & Biennial (B)
18 46,551 A: 0.8 (0.73-0.94, p<0.001)
B: 0.83 (0.73-0.94, p=0.002)
A: 0.67 (0.51-0.83, p<0.05)
B: 0.79 (0.62-0.97, p<0.05)
342 (334-350)A: 340 (333-348)B: 343 (336-351)NS

Stool-Based Tests
Disadvantages
• Not designed to detect
pre-cancerous lesions
• Requires annual testing
• High false positive rates
• TWO STEP TEST
Advantages
• Low risk, non-invasive
• No bowel preparation
• Home testing
• Inexpensive

Colorectal Cancer Screening Options
Stool-based tests
Fecal occult blood testing (FOBT)
Fecal Immunochemical Testing (FIT)
Stool DNA (Cologuard)
Structural Tests
CT Colonography
Barium Enema
Flexible Sigmoidoscopy
Colonoscopy

Colonoscopy
• Insertion of a flexible scope to visualize the entire rectum and colon
• Can diagnose cancer and perform biopsies
• Can detect and remove potentially pre-cancerous polyps
• Requires a bowel preparation to cleanse the colon– Clear liquids day before procedure– Bowel preparation evening before and day of
procedure (split dose)
• Sedation given during the procedure– Requires day off life/work– Requires escorted transportation

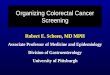
Colonoscopic Polypectomy

Colonoscopy Performance
• Considered the “gold standard”
• Not perfect…– 2-12% of large polyps
are missed
– May not be as protective of cancer on the right side of the colon
OR 0.24 (CI 0.21-0.27)
OR 0.58 (CI 0.53-0.64)

Colonoscopy Quality
• High-definition scopes
• Image enhancement
• Devices (cap, endocuff)
• Chromoendoscopy
• Financial
• Organizational
• Bowel preparation
• Tumor biology
• Specialty/Training
• Personality (vigilance, conscientiousness)
• Procedural/motor skills
• Knowledge base
EndoscopistFactors
Patient factors
Technical factors
System factors

Colonoscopy Quality

Colonoscopy Efficacy
• No randomized controlled trials to date
• Indirect evidence:– National Polyp Study: 76-90% reduction in CRC incidence after
polypectomy– VA study: lower endoscopy within past 6 years associated with
60% reduction in CRC mortality– FOBT & Flexible Sigmoidoscopy trials
• Current trials underway:– VA CONFIRM (Colonoscopy vs FIT)– Spanish trial (Colonoscopy vs FIT)– Nordic-European Initiative (Colonoscopy vs no screening)

Colonoscopy Risks
• Perforation 0.5/1,000
• Bleeding 2.6/1,000
• Death 2.9/100,000





Colonoscopy
Disadvantages
• Invasive, procedural risks
• Sedation required
• Time consuming, expensive
• Full bowel preparation
• Operator, preparation dependent
Advantages
• Can visualize the entire colon
• Diagnose and remove lesions
• Performed every 10 years
• Minimal patient discomfort
• SINGLE STEP TEST

Colorectal Cancer Screening Options
Stool-based tests
Fecal occult blood testing (FOBT)
Fecal Immunochemical Testing (FIT)
Stool DNA (Cologuard)
Structural Tests
CT Colonography
Barium Enema
Flexible Sigmoidoscopy
Colonoscopy

What is the best screening test…?

ACS-MSTF-ACR-AGA
> 50:
FS every 5 years +/- FOBT
every year
-Or-
“High Sensitivity” FOBT/FIT
every year
-Or-
Colonoscopy every 10 years
-Or-
CT Colonography every 5
years
-Or-
Fecal DNA every 3 years
USPSTF50-75:
FS every 5 years with
interval “High Sensitivity”
FOBT/FIT
-Or-
“High Sensitivity”
FOBT/FIT every year
-Or-
Colonoscopy every 10
years

A few patients…
• I am healthy! I have no symptoms or problems. I don’t think I could have colon cancer.
• I don’t ever want a colonoscopy. Is there another test I can do instead?
• Colonoscopy is too risky for me!!

Family history and CRC

Increased Risk Group
Definition Modality Starting Age/ Interval
ACS/MSTF/
ACR
1 FDR > 60
CRC/Adenoma
2 SDR CRC any age
Any 40/Average risk intervals
ASGE 1 FDR > 60
CRC/Adenoma
Colonoscopy 40/Average risk intervals
ACG 1 FDR > 60
CRC/Adenoma
Colonoscopy
Preferred
50/ Average risk intervals
NCCN 1 FDR > 60 CRC
1 SDR < 50 CRC
1 FDR Adv Adenoma
Colonoscopy 50/ q 5-10 yrs

CRC Risk Categories Based on Family History
Average Risk
•No Personal or family history of colon polyps or colorectal cancer (CRC)
Increased Risk
•One first-degree relative with CRC/Adenoma over the age of 60
•Two second degree relatives with CRC any age
High Risk
•One first-degree relative with CRC/Adenoma younger than age 60
•Two or more first degree relatives with CRC/Adenoma, any age
Hereditary Risk
•Three or more family members with colorectal cancer
•Multiple other cancer types in the family
•Young ages of onset of cancers (less than 50)
Age 50, any screening test
Age 40-50, colonoscopy every 5-10 years
Age 40, colonoscopy every 5 years
Referral to Genetics Expert

Take home points
• Colon cancer is common and lethal
• Colon cancer is preventable!
• There are a menu of stool-based and structural CRC screening options– The best option is the one your patient will commit
to!
• Family history of CRC may increase a patient’s risk

Thank you for your attention!