Embed Size (px)
Citation preview

Update: Uveitis
Prof. Dr. Matthias Becker
http://www.triemli-augenklinik.ch

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Financial Disclosures
• Lecturer: PeerVoice
• Advisor: GLG (Gerson Lehrman Group), AbbVie
• Editor: SwissOphthal
No financial interests

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Pubmed: # publications for „uveitis“
891 918 932
957 954
1085 1124
1190 1211 1207
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Uveitis
• Fifth most common cause of vision loss in high-income countries
• Estimated incidence of 17 to 52 cases per 100‘000
• Highest incidence of disease in the working-age population
• Estimated prevalence 38 to 714 cases per 100‘000
• Overall prevalence is as high as 0.73%
• Accounting for 5% to 20% of legal blindness
• Estimated to cause 10 to 15% of cases of preventable blindness in developed countries and up to 25% of cases in the developing world overall
• Responsible for approximately 30‘000 new cases of legal blindness each year (2.8%–10% of all cases of blindness)
• Socioeconomic impact of uveitis is at least as significant as that of diabetic retinopathy (de Smet et al. 2011)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Horai R, et al. J Interferon Cytokine Res 2011;31:733-44.

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Gomes Bittencourt M, et al. Dev Ophthalmol 2012;51:134-61.

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Recent International Multicenter Studies for Uveitis
Study Drug
MUST Surgical fuocinolone acctonide
implant (Retisert©)
HURON Injectable intravitreal dexamethasone
implant (Ozurdex©)
ENDURE Systemic anti-IL-17 agent
Secukinumab (Cosentyx©)
EYEGUARD Systemic anti-IL1b drug gevokizumab
(XOMA 052©)
VISUAL Systemic anti-TNF adalimumab
(Humira©)
SACURA Injectable intravitreal sirolimus
(Opsiria©)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
VISUAL I+II Systemic anti-TNF adalimumab (Humira©)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Anti-TNF-Inhibitors: Targeting inflammatory cytokines
• Etanercept (Enbrel©; Amgen, Thousand Oaks, CA)
• Infliximab (Remicade©; Janssen Biotech, Horsham, PA)
• Adalimumab (Humira©; AbbVie, North Chicago, IL)
• Golimumab (Simponi©; Janssen Biotech, Horsham, PA)
• Certolizumab (Cimzia©; UCB, Brussels, Belgium)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
To confirm that adalimumab is efficacious in
the studied population versus placebo
Real-world design to provide insight about the
safety and effectiveness of adalimumab in
clinical practice
n=239
n=261
n=424
85% of VISUAL I & II
Active uveitis1
ADA 40 mg or placebo
n=239a
Controlled uveitis2
ADA 40 mg or placebo
n=261a
Open-label extension3
ADA 40 mg
n=424
85% of patients in VISUAL I and II
1. Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43 2. Nguyen QD et al. Lancet. 2016 Sep 17;388:1183-92 3. Suhler EB, et al. IUSG 2016; FP52
RCTs in non-infectious uveitis: The VISUAL program

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
The VISUAL trials
• The VISUAL-I trial was conducted to assess the efficacy and safety of adalimumab (ADA) in patients with active, non-infectious uveitis despite high-dose corticosteroid therapy1
• The VISUAL-II trial was conducted to assess the efficacy and safety of ADA in corticosteroid-dependent patients with inactive, non-infectious uveitis who are at risk of the long-term side effects of corticosteroids2
• The VISUAL-III trial was conducted to evaluate the long-term safety and efficacy of ADA in patients with non-infectious intermediate, posterior, or panuveitis
1. Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43 2. Nguyen QD et al. Lancet. 2016 Sep 17;388:1183-92

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
https://clinicaltrials.gov/show/NCT01138657
https://clinicaltrials.gov/show/ NCT01124838
https://clinicaltrials.gov/show/NCT01148225
Global study sites N = 62 in 21 countries
CH = 2

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
N Engl J Med. 2016;375:932-43
VISUAL-I
• Multinational, phase-III RCT, placebo-controlled
• Active noninfectious intermediate uveitis, posterior uveitis, or
panuveitis
• Randomly assigned 1:1 ratio to receive adalimumab (ADA) or
matched placebo
• All received mandatory prednisone burst followed by tapering of
prednisone over the course of 15 weeks
• PEP: time to treatment failure occurring at or after week 6

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Lancet. 2016;388:1183-92
VISUAL II
• Multicentre, double-masked, randomised, placebo-controlled
• Inactive, non-infectious uveitis controlled by systemic CS
• Controlled by 10–35 mg/day of prednisone
• Randomly assigned 1:1 ratio to receive adalimumab (ADA) or
matched placebo
• PEP: time to treatment failure (multicomponent endpoint)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
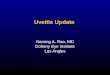
Study design
VISUAL-I
VISUAL-II
1. Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43 2. Nguyen QD et al. Lancet. 2016 Sep 17;388:1183-92

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Composite Primary Endpoint in VISUAL-I and -II
Treatment failure criteria
New lesions
Anterior chamber cells
Vitreous haze
BCVA
Time to treatment failure (TF)
Time to event analysis Multiple triggers
Time to TF is defined as the time from randomization to discontinuation due to any of the given TF criteria
1. Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43 2. Nguyen QD et al. Lancet. 2016 Sep 17;388:1183-92

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Early and sustained effect of adalimumab on the rate of treatment failure compared with placebo
The risk of failing treatment (flare or vision loss) was reduced by almost
half and the time to treatment failure was approximately doubled
PBO ADA
Median time to
treatment
failure
8.3 months >18 months
HR; p-value 0.57; p=0.004
95% CI for HR (0.39–0.84)
PBO ADA
Median time to
treatment failure
3.0 months 5.6 months
HR; p-value 0.50; p<0.001
95% CI for HR (0.36–0.70)
0 2 4 6 8 10 12 14 16 20
Time (months)
Tre
atm
en
t fa
ilu
re
rate
(%
)
20
40
60
80
0 18
placebo (n=111) ADA (n=115)
0 10 20 30 40 50 60 70 80 90 Time (weeks)
Tre
atm
en
t fa
ilu
re
rate
(%
)
20
40
60
80
100
0
placebo (n=107) ADA (n=110)
1. Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43 2. Nguyen QD et al. Lancet. 2016 Sep 17;388:1183-92

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
VISUAL I – Efficacy Primary endpoint: Time to treatment failure
• Hazard ratio for time to treatment failure between ADA and PBO is 0.5 (0.36–0.70), p<0.001, therefore, the risk to fail was reduced by 50% for ADA compared with PBO
• The median time to treatment failure was prolonged by 87% from 13 weeks for placebo to 24 weeks for ADA
HR=0.5 (0.36–0.70), p<0.001
0 10 20 30 40 50 60 70 80 90
Weeks
Tre
atm
en
t fa
ilure
rat
e (
%)
20
40
60
80
100
0
placebo (n=107) ADA (n=110)
87% increase
ADA: Adalimumab; PBO: Placebo
Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
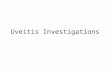
VISUAL II – Efficacy Primary endpoint: Time to treatment failure
HR=0.57 (0.39–0.84, p=0.004)
placebo (n=111) ADA (n=115)
0 2 4 6 8 10 12 14 16 20
Months
Tre
atm
en
t fa
ilure
rat
e (
%)
20
40
60
80
0
18
• Hazard ratio for time to treatment failure between ADA and PBO is 0.57 (0.39–0.84), p=0.004, therefore, the risk to fail was reduced by 43% for ADA compared with PBO
• The median time to treatment failure was 8.3 months for PBO, but was not estimable for ADA, as fewer than half of the ADA-treated patients experienced treatment failure
Denniston A. et al. Lancet_E 2016, S0140-6736(16)31327-7

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Conclusions: VISUAL-I
• In patients with active, non-infectious uveitis uncontrolled with
prednisone ≥10 mg daily, ADA significantly lowered the risk for
uveitic flare or BCVA loss
• Patients on ADA had a lower risk to fail and fewer criteria of
treatment failure were met
• Worsening of AC cell grade, VH grade, and BCVA from best state
achieved, as well as occurrence of new lesions were reduced with
ADA compared with placebo
• Percent change in CRT was significantly smaller with ADA compared
with placebo, and ADA also reduced the risk of developing ME in
patients without pre-existing macular pathology
• Adverse event data were similar between the ADA and placebo
groups. The safety profile was consistent with the known safety profile
of ADA across approved indications
Jaffe GJ et al. N Engl J Med. 2016 Sep 8;375:932-43

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Conclusions: VISUAL-II
• In steroid-dependent patients with inactive, non-infectious uveitis, ADA significantly lowered the risk for uveitic flare or vision loss
• Patients on ADA had a lower risk to experience treatment failure and fewer criteria of treatment failure were met
• Secondary endpoints were numerically in favor of ADA, although significant differences between ADA and placebo were not observed
• Adverse events were similar between the ADA and placebo groups. The safety profile was consistent with the known safety profile of ADA across approved indications.
Nguyen QD et al. Lancet. 2016 Sep 17;388:1183-92

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Strengths
• RCT design
• Large patient population
• Diversity of uveitis diagnosis
• Composite primary endpoint
• Hierarchical statistical analysis of secondary endpoint
Limitations
• Heterogenity of uveitis aetiologies
• Underestimation of time to treatment failure?
• Overestimation of treatment failure?
• Scarcity of established high-quality outcome measures

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
N Engl J Med 2017;376(17):1637
• Children and adolescents 2 years of age or older who
had active JIA-associated uveitis
• Taking a stable dose of MTX
• Randomly assigned in a 2:1 ratio to receive either ADA
(20 mg or 40 mg, BW) or placebo +
• Treatment failures in 27% in the ADA versus 60% in
placebo

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Adalimumab labels
• FDA (approval 30-JUN-2016): «Humira is indicated for the treatment of non-infectious intermediate, posterior and panuveitis in adult patients.”
• 10th approved indication for HUMIRA in the United States
• EMA (approval 24-JUN-2016): «Humira is indicated for the treatment of non-infectious intermediate, posterior and panuveitis in adult patients who have had an inadequate response to corticosteroids, in patients in need of corticosteroid sparing, or in whom corticosteroid treatment is inappropriate.»
• Swissmedic (approval 17-MAY-2017) FDA Humira, www.fda.gov, Date of information: June 2016 EMA Humira, www.ema.europa.eu, Date of information: October 2016 SmPC Humira, www.swissmedicinfo.ch, Date of information: March 2016

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Preis in der Schweiz (compendium.ch)
• Fertigspritze 40 mg = 739 CHF
• Initialdosis von 80 mg (2 Injektionen) und danach 40 mg (1 Injektion) jede zweite Woche beginnend eine Woche nach der Initialdosis als subkutane Injektion

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
SACURA-TRIAL Intravitreal Sirolimus
“Sirolimus study assessing doublemasked uveitis treatment”

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
mTOR-Inhibitors (= mechanistic Target of Rapamycin)
• Tacrolimus (Prograf®)
• Everolimus (Certican®)
• Sirolimus
– Systemisch: Rapamycin (Rapamune®)
– Intravitreal: Opsiria® (Santen, Osaka, Japan)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Ophthalmology.
2016;123:2413-23
• Noninfectious uveitis (NIU) of the posterior segment
• 2nd Phase III, randomized, double-masked, active-
controlled, 6-month
• Vitreous haze (VH) score >1+
• Assigned 1:1:1 at doses of 44, 440, or 880 μg, administered
on days 1, 60, and 120
• PEP: % VH=0 at month 5 without use of rescue therapy
• SEP: VH 0 or 0.5+ response rate, CS tapering success,
changes in BCVA
• N=347

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Results: SACURA-II Trial Nguyen QD et al., Ophthalmology. 2016;123:2413-23
44 μg 440 μg 880 μg
PEP 10.3% 22.8%; P = 0.025 16.4%; P = 0.182
VH score of 0 or
0.5+
35.0% 52.6%; P = 0.008 43.1%; P = 0.228
CS-taper 63.6% 76.9% 66.7%
BCVA maintained throughout the study
in each dose group

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Conclusion: SACURA-II Trial Nguyen QD et al., Ophthalmology. 2016;123:2413-23
• Significantly more patients in the 440 μg group achieved improvement in ocular inflammation than did the 44 μg set
• Opsiria is intended as a 440 µg sirolimus injection
• Demonstrating its safety and maintaining BCVA
• Lack of inducing glaucoma
• Efficacy to treat CME has not been clarified in the SAKURA trial and is likely to be low
• Potential to provide safe long-term care

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich
Sirolimus labels
• FDA (25-APR-17): „FDA Filing Acceptance of New Drug Application (NDA) for Intravitreal Sirolimus (DE-109) in the Treatment of Non-Infectious Uveitis of the Posterior Segment“
• EMA (20-MAY-2016): „Santen officially notified the Committee for Medicinal Products for Human Use (CHMP) that it wishes to withdraw its application for a marketing authorisation for Opsiria“
• Swissmedic: (approval pending)

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich

Prof. Dr. Matthias Becker Augenklinik Triemli Zürich