Embed Size (px)
Citation preview
Update on Tuberculosis contact investigation
Dr David ShitritMaccabi Health ServiceRehovot
TB Contact investigation
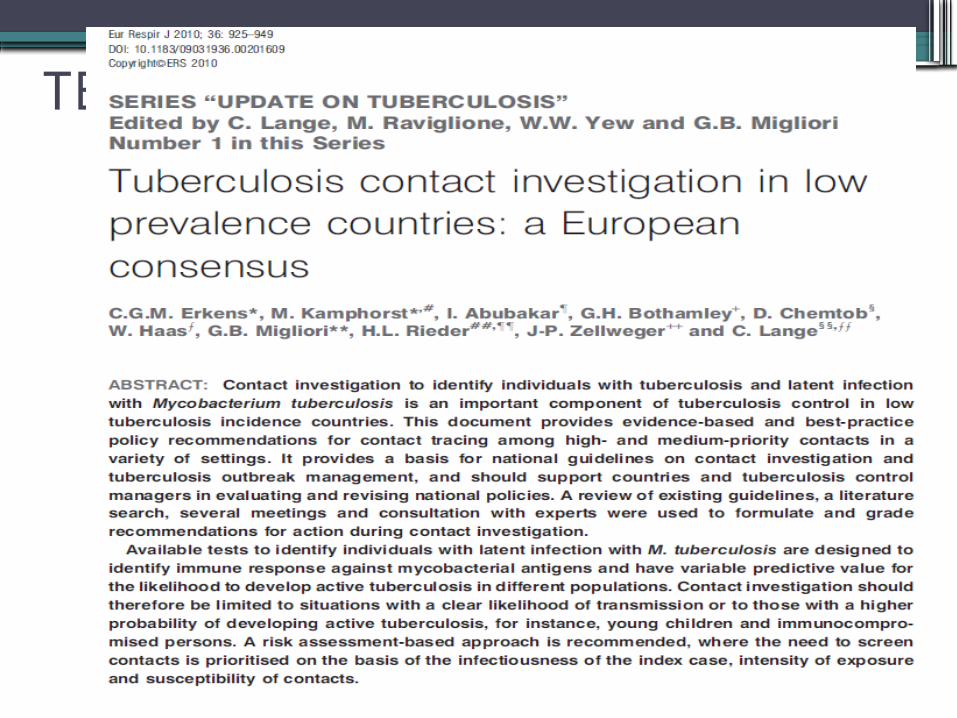
Conditions increasing the risk for progression to tuberculosis and relative odds (OR, from retrospective studies) or relative risk (RR, from prospective studies)
Condition OR or RR
1. Immune suppression
a. HIV-positive and tuberculin skin test-positive 65-67 [C]
b. AIDS68, 69 [C]
c. Solid organ transplantation related to immunosuppressant therapy 70 71, 72[D]
d. Receiving anti-TNF-alpha treatment 73-75 [B]
e. Corticosteroids >15mg prednisolone equivalent per day for >2-4 wks 76, 77 [D*]
2. Malignancy
a. Haematological malignancy (leukemias, lymphomas) 78
b. Carcinoma of the head or neck and lung 79
3. Gastrectomy 80, 81
4. Jejunoileal bypass 82, 83
5. Silicosis 84-86
6. Chronic renal failure / haemodialysis 87, 88
7. Diabetes mellitus 89-92
8. Smoking 93-97
9. Underweight 98, 99
10. Age < 5 years (see table 3) 27
50-110
110-170
20-74
1.5-17
4.9
4-8
16
2.5-6.3
2.5
27-63
30
10-25
2-3.6
2-3
2.0-2.6
2-5
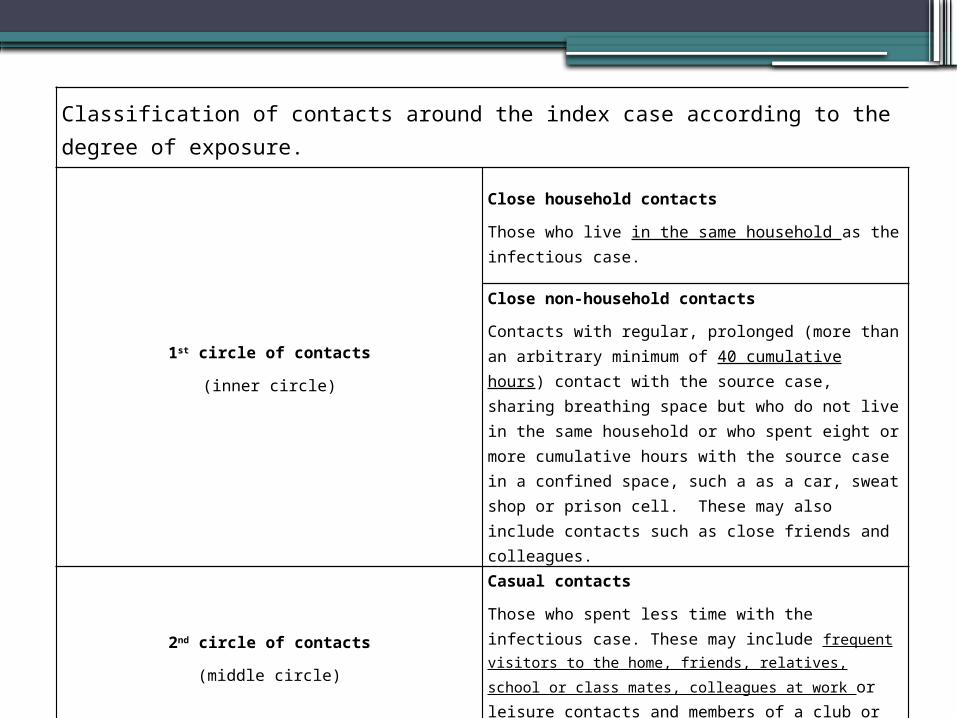
Classification of contacts around the index case according to the degree of exposure.
1st circle of contacts
(inner circle)
Close household contacts
Those who live in the same household as the infectious case.
Close non-household contacts
Contacts with regular, prolonged (more than an arbitrary minimum of 40 cumulative hours) contact with the source case, sharing breathing space but who do not live in the same household or who spent eight or more cumulative hours with the source case in a confined space, such a as a car, sweat shop or prison cell. These may also include contacts such as close friends and colleagues.
2nd circle of contacts
(middle circle)
Casual contacts
Those who spent less time with the infectious case. These may include frequent visitors to the home, friends, relatives,
school or class mates, colleagues at work or leisure contacts and members of a club or team.
3rd circle of contacts
(outer circle)
Community contacts
Those living in the same community or attending the same school, sports club or workplace who may have had sporadic contact.
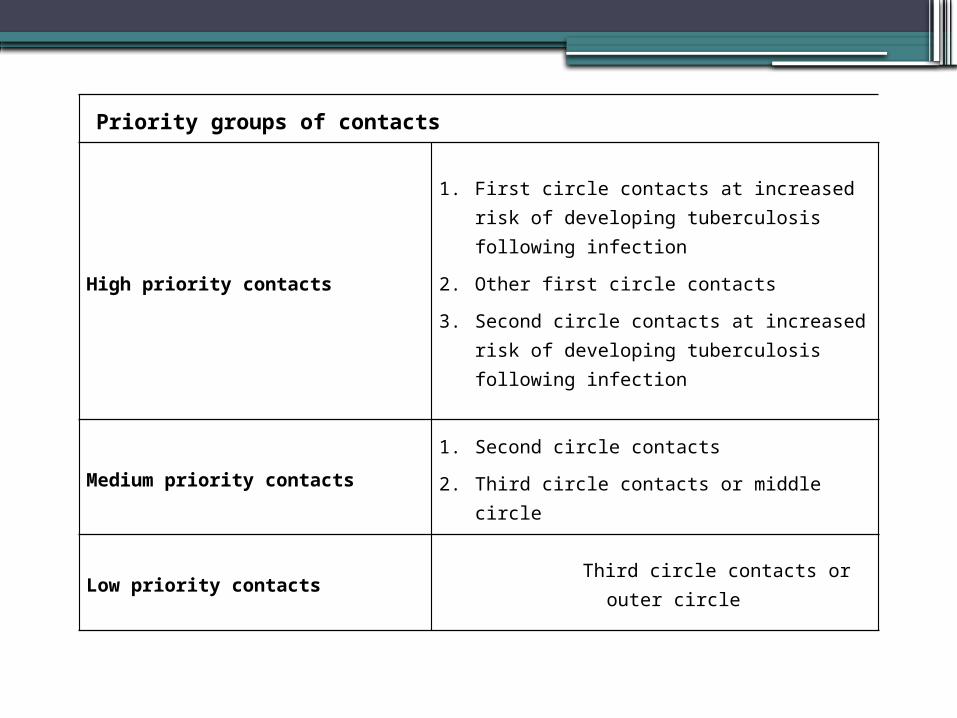
Priority groups of contacts
High priority contacts
1. First circle contacts at increased risk of developing tuberculosis following infection
2. Other first circle contacts
3. Second circle contacts at increased risk of developing tuberculosis following infection
Medium priority contacts1. Second circle contacts
2. Third circle contacts or middle circle
Low priority contacts Third circle contacts or outer circle
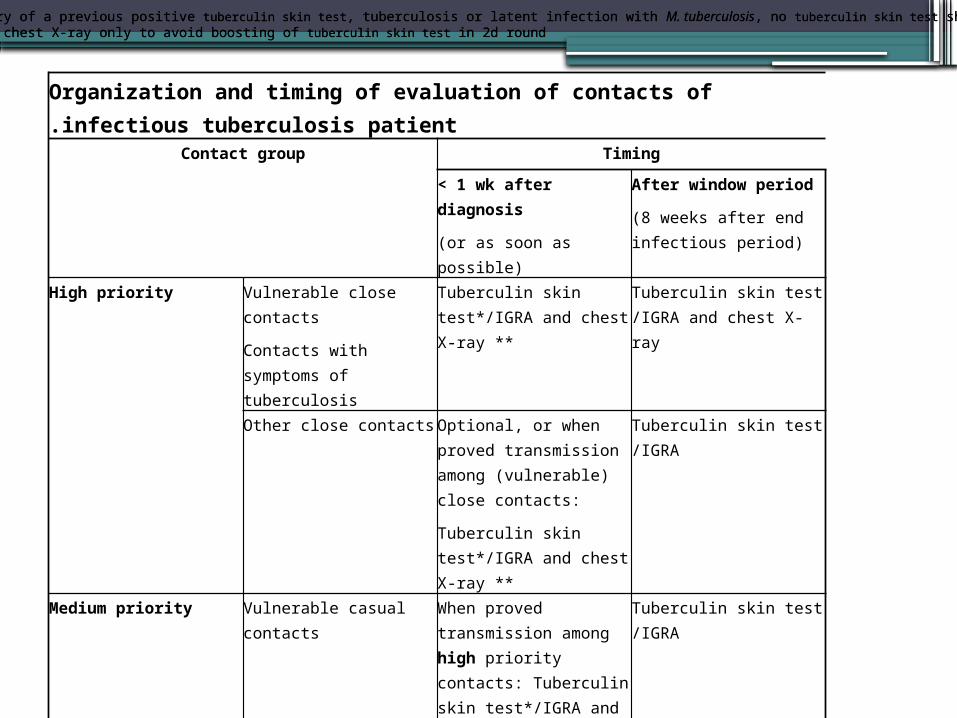
Organization and timing of evaluation of contacts of infectious tuberculosis patient.Contact group Timing
< 1 wk after diagnosis
(or as soon as possible)
After window period
(8 weeks after end infectious period)
High priority Vulnerable close contacts
Contacts with symptoms of tuberculosis
Tuberculin skin test*/IGRA and chest X-ray **
Tuberculin skin test /IGRA and chest X-ray
Other close contacts Optional, or when proved transmission among (vulnerable) close contacts:
Tuberculin skin test*/IGRA and chest X-ray **
Tuberculin skin test /IGRA
Medium priority Vulnerable casual contacts When proved transmission among high priority contacts: Tuberculin skin test*/IGRA and chest X-ray
Tuberculin skin test /IGRA
Medium priority Other medium priority contacts
When proved transmission among high priority contacts:
Tuberculin skin test /IGRA
Low priority When proved considerable transmission among medium priority contacts: Tuberculin skin test /IGRA
*When there is a history of a previous positive tuberculin skin test, tuberculosis or latent infection with M. tuberculosis, no tuberculin skin test should be administered** BCG-vaccinated: chest X-ray only to avoid boosting of tuberculin skin test in 2d round
*When there is a history of a previous positive tuberculin skin test, tuberculosis or latent infection with M. tuberculosis, no tuberculin skin test should be administered** BCG-vaccinated: chest X-ray only to avoid boosting of tuberculin skin test in 2d round
The risk of progression to TB among contacts•A median incubation time of 6 weeks •Highest immediately after incubation time•Exponentially decline during the first 7
years▫60% in the first year▫80% < 2 years
•After 7 years: 1 per 1000 person-yrs•Determined by the age:
▫30-40% among infant▫2% primary school children
Likelihood and risk of transmission
•Every TB patient should be interviewed promptly after diagnosis
•Isolated extra pulmonary TB require CXR and sputum examination to exclude concomitant pulmonary disease.
•The largest number of AFB is found in cavitary lesions
•Smear negative, culture positive: 13% of all transmissions
Parameters to assess the infectiousness of the index patient
Anatomical site: pulmonary TBThe production of sputumResults of sputum smear examinationResults of sputum cultureCavitationcoughing
Infectious period
•Onset of cough (or other respiratory symptom determine the onset of infectiousness
•Pulmonary cases with positive smear: maximum of 3 months
•Pulmonary cases with positive culture and 2 negative smear: 1 month
•Until 2 weeks of appropriate treatment
Locations of transmission
•Outdoors vs. Indoors•Specific investigation, preferably a visit is
important
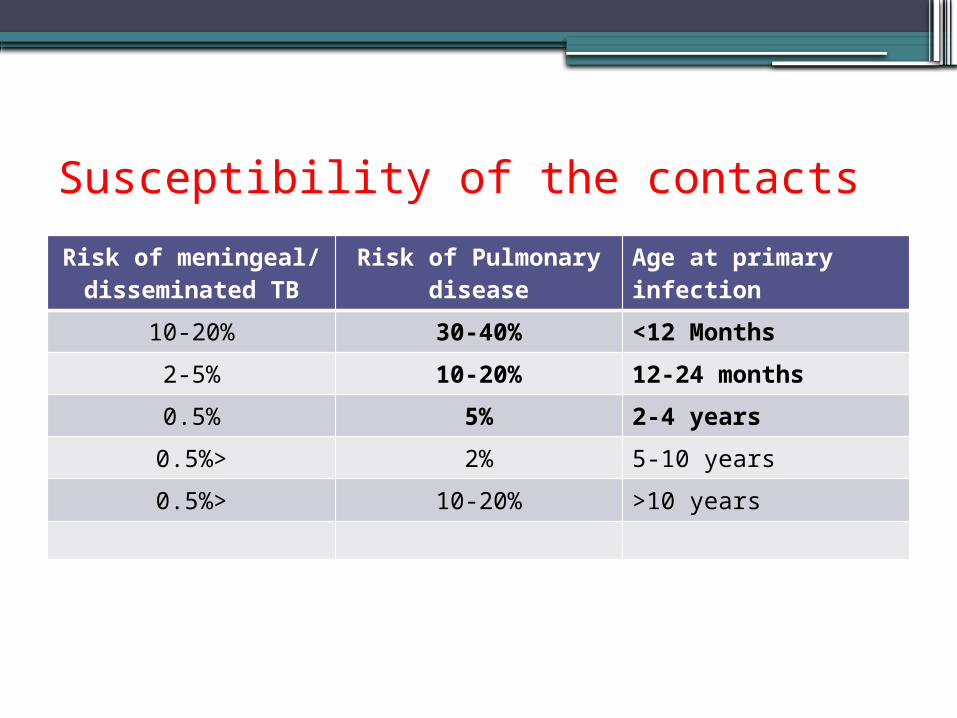
Susceptibility of the contactsRisk of meningeal/ disseminated TB
Risk of Pulmonary disease
Age at primary infection
10-20% 30-40% <12 Months
2-5% 10-20% 12-24 months
0.5% 5% 2-4 years
<0.5% 2% 5-10 years
<0.5% 10-20% >10 years
The tuberculin skin test
•A positive reaction after 6-8 weeks from the infection
•14% anergy in TB children•25% anergy in adults with HIV•Sensitivity
▫95-99% in PPD>5 mm▫91-95% in PPD> 10 mm▫67-80% in PPD> 15 mm
Specificity of PPD
•The longer the time since BCG and the larger PPD reaction size, the higher probability of TB
•Possible causes of FN PPD▫Age (below 6 months, above 65 yrs)▫Cellular immune defects▫Malignancy▫Systemic high dose seteroids▫Sarcoidosis
IGRA
•In immunocompromised persons-more specific and sensitive than PPD
•Less sensitive in immunocompetent pts than PPD
•The specificity is much superior to PPD in immunocompetent with prior BCG
•PPD should not perform in interval of 3 days from IGRA
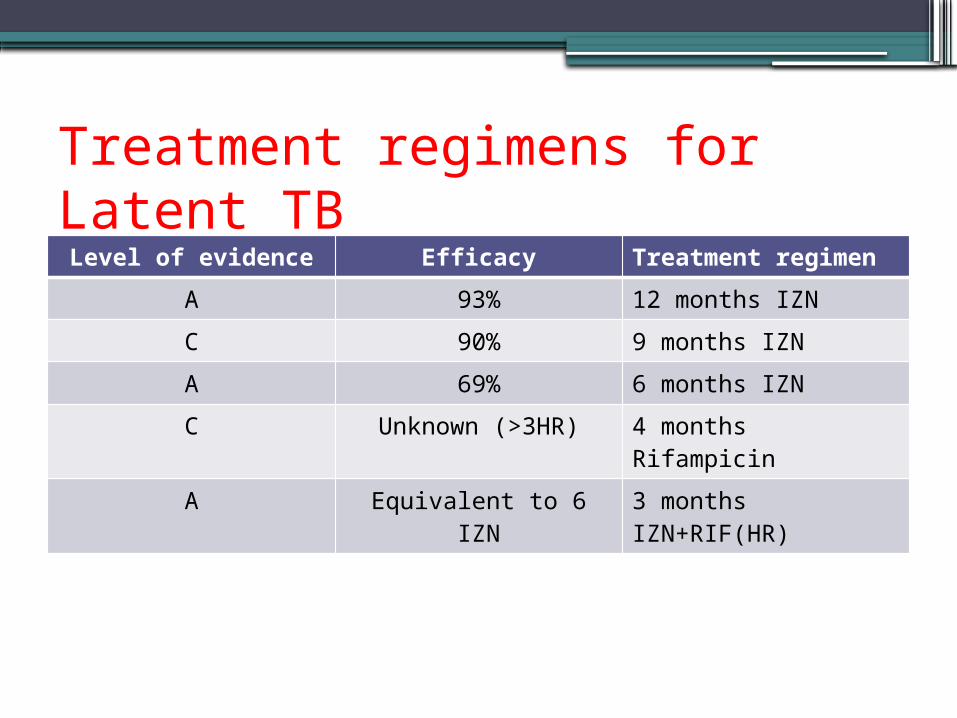
Treatment regimens for Latent TB
Level of evidence Efficacy Treatment regimen
A 93% 12 months IZN
C 90% 9 months IZN
A 69% 6 months IZN
C Unknown (>3HR) 4 months Rifampicin
A Equivalent to 6 IZN 3 months IZN+RIF(HR)
Thank You!