-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Update on Thrombolysis and
Thrombectomy
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
I received financial compensation from Boehringer -Ingelheim for
my time and efforts as Chairman of the SC of ECASS 1-3 and from
Paion for DIAS and DIAS II
I have received honoraria for lectures and advisory boards from
BI and Paion
I have received an unrestricted scientific grant by BI to
organize the ECASS 4, an IIT sponsored by the University of
Heidelberg
I am a member of the SC of SWIFT-PRIME and TASTE
Relevant Disclosures
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Introduction:
• The preconditions for recanalization therapies Part I:
Thrombolysis
• Penumbra and vessel occlusion • The Dark Ages- Intra-arterial
thrombolysis case series • I.V.-Thrombolysis- past and present
The groundbreaking studies
New lytics and Penumbral selection
rtPA in clinical routine
Part II: Mechanical recanalization
• The early cohorts and early RCTs • The new Thrombectomy
trials
Summary
Content
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Successful recanalization therapies need a perfectly
orchestrated stroke management system
Recanalization must be offered to all people qualifying, not
only to a handful of those, who live near private hospital
The management system includes
• Recognition (FAST) • EMS and ER • A network of stroke ready
hospitals with Stroke Units
connected by teleneurology
• Imaging and interventions • Rehabilitation and prevention
Preconditions for Recanalization Treatment
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Stroke ready hospitals offer Imaging (CT, CTA), Stroke Units and
co-operation with stroke centers
• They can perform thrombolysis Stroke centers offer MRI,
interventions, neuro-ICU facilities
and neurosurgery
• They will receive transferrals from the smaller hospitals for
elective therapies
Regional organization of stroke services is key
Preconditions for Recanalization Treatment
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
The incidence of acute ischemic stroke in Germany is
250-300/100,000/year, a total of 200,000 new strokes every year
In Germany (Population 82 Mio), we have a network of 280 Stroke
units, among them 50-60 comprehensive stroke centers
For Argentina (Population 41 Mio), we can expect about 70,000 to
80,000 new strokes per year according to the few epidemiological
data available
I believe that both incidence and prevalence numbers are much
higher
How Many Patients Qualify for Recanalization?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Under optimal circumstances, about 30% of all stroke patients
can qualify for i.v. Thrombolysis
Of them, about 20-30% may also qualify for thrombectomy
Transferral to stroke centers leads to relatively higher numbers
of thrombectomy, because the patients come from a larger catchment
area
In Heidelberg, a city with a catchment area (Lysis) of 800.000
Inhabitants, we do 300 i.v.rtPA cases per year
The thrombectomy number for the first half of 2016 are already
over 800, most of them with rtPA co-treatment
The Buenos Aires metro area (13 Mio) is comparable BW (10.5 Mio)
with 15% rtPA (4,500 rtPA cases per year)
How Many Patients Qualify for Recanalization
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Part I:
Thrombolysis
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• Ischemic stroke is caused by vessel occlusion
• Successful thrombolysis requires both, salvageable tissue
and remaining vessel occlusion
• This is reflected in the „penumbra + mismatch concepts“
already irreversibly damaged infarct core
hypoperfused but still viable tissue at risk to undergo
definite infarction
• Recanalization is time-critical because tissue damage may
progress unless reperfusion occurs
The Rationale of Recanalization
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
It all started with pilot cases of intra-arterial thrombolytic
therapy in cases with acute basilar artery occlusion, and otherwise
deadly condition
• Published in German, because leading journals would not accept
it for „ethical concerns“
Zeumer, Hacke, Kolmann and Poeck DMW 107 (1981) 728-731
Zeumer, Hacke and Ringelstein AJNR 4(1983) 401-404
The authors received really encouraging reviews:
„Everybody knows that thrombolysis is dangerous
and should be avoided in stroke...
The technique described in this paper is unethical
and should not be studied further...“
The original 1979 film
The Early Thrombolysis Cohorts
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
ECASS (JAMA 1995)
The NINDS Study leading to 3 h approval (NEJM 1995)
ECASS II (Lancet 1998)
The Pooled Analysis of ATLANTIS, ECASS and NINDS
indicating benefit up to 4.5 h (Lancet 2004)
ECASS 3 confirming the 4.5h time window (NEJM 2008)
The second Pooled Analysis (Lancet 2009)
IST 3 showing that treatment works outside the labelling
and does not cause harm (Lancet 2012)
The STTC*-Analysis (Lancet 2012)
*Stroke Thrombolysis Trialists’ Collaborative Group, Lancet
2012
The Groundbreaking Trials
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
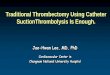
The Groundbreaking Studies: NINDS 1996
The NINDS Study consisted of Part 1 and 2
Plain CT selection with emphasis on early treatment
A 3 h time window, but one half of the patients had to be
treated within 90 mins
Part 1 (300) was negative, Part 2 (300) with a different
(global) endpoint was positiv and so was the combined
analysis
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
26%
26%
21%
25%
23%
27%
17%
21%
+13%
NINDS Investigators. N Engl J Med 1995; 333 (24): 1581–1587.
13% more rt-PA treated patients in favourable outcome (mRS
0-1)
Death mRS
Placebo
(n = 312)
Actilyse
(n = 312)
0 - 1 2 - 3 4 - 5
NINDS-study 1996:
Thrombolysis within 3h increases excellent functional
outcome
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
The Groundbreaking Studies: NINDS 1996
Based on the NINDS study rtPA was approved in the US
for treatment of AIS in the 3 h time window
Because of the relatively small trial and the fact that only
a
300 patient substudy was positive, there was a lot of
resistance (ER-physicians) in the US to use rtPA
The lysis rates were in the order of 2-3% for many years
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
The Groundbreaking Studies: ECASS 3
• Trial designed upon request of EMA • 3-4.5h time window, 821
patients randomized to rtPA
or placebo
• We didn´t believe that it would have a chance to be positive,
although we increased the number of patients
from 600 to 800
• It took some time to finalize the trial, recruitment was
difficult, but we succeeded
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• We were deeply surprised • This time the choice of endpoint
didn´t matter • Positive in primary endpoint mRS 0,1, positive in
global
outcome and in shift
• An undisputed positive and guideline changing trial
p=0.024*
Intent-to-treat population
Alteplase
(n=418)
mRS score
Placebo
(n=403)
1 2 3 0 4 5 6
27.5
23.3 21.8 16.4
9.3 14.1 24.9
13.7
9.3
8.2
6.7 8.1
11.4 5.2
ECASS 3
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
The 2008 medical paper of the year
Editors choice - The Lancet
The Groundbreaking Studies: ECASS 3
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Stroke Thrombolysis Trialists Cooperation*
„Single patient date prospective pooled analysis“
>6.700 Patienten
Confirms time dependent treatment effect
Indicates increased risk of mortality, mostly over 4.5h
and in severe old patients
Benefit/risk Ratio remains positive despite increased
sICH risk
Stable effect for age, severity in the under 4.5h group
Emberson, Lees, Lyden….Sandercock, Hacke Lancet 2014
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Emberson, Lees, Lyden….Sandercock, Hacke: STTC ISC 2014, Lancet
2014
Stroke Thrombolysis Trialists Cooperation*
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Emberson, Lees, Lyden….Sandercock, Hacke: 2014
Stroke Thrombolysis Trialists Cooperation*
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Latest News: ENCHANTED-Trial
Rationale
• Testing the hypothesis that low dose (0.6mg/kg) rtPA is
equally effective as regular dose (0.9mg/kg) in a
(mostly Asian) population
Design
• 2x2 factorial design of 3,310 patients eligible for rtPA
within 4h
• (additionally, patients with elevated BP randomly assigned to
early intense or standard BP lowering)
935 patients eligible for that trial included
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
ENCHANTED-Trial: Low vs High Dose rtPA
Mdn age 67, asians 70%
Results
• Primary outcome mRS 2-6 Low dose 53.2%, regular dose 51.1%
OR 1.09 (95%CI 0.95-1.25)
The upper boundary exceeded the non-inferiority margin
(p for non-inferiority .51)
• Ordinal mRS Common odds 1.0 (95%CI .89-1.13), p
non-inferiority .04
• sICH Low dose 1% standard dose 2,,1% p=.01
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
rtPA in the Field
Results of RCTs and pooled analyses can be repeated
in the field
SITS-MOST
Data from >10.000 thrombolysis patients from a
German state (thromectomy excluded)
15% Lysis rate (25% plus in stroke centers)
Results comparable with pooled data
Gumbinger et al, BMJ 2014
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
rtPA in the Field
Gumbinger et al, BMJ 2014
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Part II:
Intra-arterial Thrombectomy (IAT)
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Intraarterial Lysis And Mechanical
Revascularisation
Selection of patients and preparation of the mechanical
intervention may be associated with a longer door to
needle time than IV-rtPA
• Lack of collaterals in proximal occlusion may even shorten the
window of opportunity
• On the other hand, once the device is in situ, recanalization
may occur faster than with IV rtPA
Nevertheless- „time is brain“ is important here too
Recanalization 8 or 10h after onset may not be beneficial
and in patients with high stroke severity even harmfull
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• 2012: Three RCTs are presented (Honululu ISC 2012) and
published
IMS III (Broderick et al NEJM 2012)
MR-RESCUE (Kidwell et al NEJM 2012)
SYNTHESIS (Ciccione et al NEJM 2012)
• All studies missed efficacy endpoints
History of Transvascular Stroke Trials
Broderick et al NEJM 2013
Kidwell eta l NEJM 2013
Ciccone eta NEJM 2013
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• Reasons include: long time window
use of old devices
underestimation of rtPA response in distal occlusion,
slow recruitment due to treatment outside the trial
treatment with no proof of vessel occlusion
(Furlan and Hacke IJS 2012)
• A subgroup analysis of SWIFT PRIME showed signal of efficacy
in early reperfusion and severe stroke
(Khatri et al Lancet Neurology 2012)
History of Transvascular Stroke Trials
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
New Devices
Early treatment
Severe stroke with proven Carotid T or M1 occlusions
On top of rtPA
Consequences For The New Thrombectomy Trials
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Time and Outcome
Grotta and Hacke Stroke 2015
Hacke IJS 2015
Hacke and Diener Nervenarzt 2015
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
The Thrombectomy Trials
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
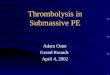
MR CLEAN
ESCAPE
EXTEND IA
SWIFT PRIME REVASCAT
mRS 0-2%
80 -
60 -
40 -
20 -
0 - ctl act ctl act ctl act ctl act ctl act
+ 24%
+ 14% + 16%
+ 31%
+ 21%
Berkhemer et al NEJM 2015, Goyank et al NEJM 2015, Campbell et
al NEJM 2015, Saver et al NEJM 2015, Jovin et al NEJM 2015,
Range of Differences: 14-31%
3
3
5
3
7
1 6
0 4
4
1
9
2
9
4
0 3
6 2
8
Good Outcome (mRS 0-2) Compared
Treatment Effects
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
How Can the Differences in Magnitude of Effects be
explained?
All studies show the same pattern
• Thrombectomy always significantly superior to standard
treatment
But: Major differences in the rates of good outcome in
both tx and control arms between trials
*Berkhemer et al NEJM 2015, Goyank et al NEJM 2015, Campbell et
al NEJM 2015, Saver et al NEJM 2015, Jovin et al NEJM 2015,
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
What does this mean for stroke management
structures?
How many patients are candidates?
• A center with 1000 Strokes per year possibly 250 rtPA
(25%)
There of 100 endovascular (20%), probably more with
referrals
Are there enough endovascular specialists?
• How do we train more? • Also Neurologists?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• Severe AIS with average NIH-SS 17 • CT-selection (the better,
the better the outcome) • No age limit • CTA proven Carotid-T or M1
occlusions • Co-Treatment with rtPA • Early treatment with
reperfusion or first thrombuspass
below 6h
• Use of Stentriever (Solitaire) Devices • Treatment in large
volume endovascular centers and
drip and ship strategies
For which patients do the results apply?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• Mild stroke • M2 Occlusions • Basilar artery occlusion • rtPA
uneligable patients • Recanalization not possible within 6 hours •
CT: Major infarct, ASPECTS 5 or below, no collaterals
For which patients do the results not apply?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• All trials were CT and CTA based • There were different
qualities of CT-assessment
required, but superiority of IAT was also achieved with
plain CT, even without major infarct assessment
ASPECTS 6 or more
RAPID assessment in 141 patients
• The more detailed the assessment was, the better the outcome
in both the IAT group and the control
What kind of imaging is necessary?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• In all trials the far majority of patients received rtPA in a
4.5h time window
• The lowest rtPA rate was in ESCAPE (76%) which also allowed
rtPA ineligable and wake-up patients
• ECTEND IA and SWIFT PRIME had almost 100% rtPA use
• The number of non-rtPA patients in the individual trials was
to small to draw conclusions
• Joint analyses of the trials may give more insight into that
question
Is rtPA necessary for the success?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• In one trial, which had the most restrictive inclusion
criteria, 1000 patients were treated with rtPA and only
70 patients were randomized
• In general, it appears that about 10% of all ischemic stroke
patients present with a severe stroke (NIHSS
over 12), not all in a time window suitable for IAT
• About 20-30% of patients who are treated with rtPA may be
candidates for IAT
• This may be more at large referral centers
How many patients are candidates for IAT?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
What does this mean for stroke management
structures? Question?
How many endovascular centers do we need?
• The Netherlands (16 Mio inhabitants, 18 centers) 1
center/Million inhabitants
• Berlin (4 Mio): 3 comprehensive stroke Units • BW 10.5 Mio): 7
comprehensive SUs
How can we offer the treatment economically and with
sufficient quality?
• Large centers, minimum treatment numbers, high personal
expertise
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• If in clinical practice CT criteria are handled not strictly,
the time window is not strictly observed and the IAT is
performed with devices other than stentrievers, the
results may be worse
• In clinical routine, it appears unlikely that the results of
SWIFT PRIME or EXTEND IA can be repeated
• Results achieved in daily practice may be closer to those of
MR CLEAN
What kind of results can we expect in everyday routine?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
• A city with 500.000 inhabitants and 5 interventional centers,
each doing 20 or less IAT per year, mostly on
workdays, is not well served
• This scenario is not economically sound, lacks quality and
experise, and bound to widen the indication for IAT
for financial reasons beyond the evidence
• It also allows not for good training conditions if there is a
patient only once in 2 weeks
How many interventional centers do we need?
-
Seniorprofessur Neurologie UniversitätsKlinikum und Universität
Heidelberg
Excellent News, and a lot of work
in front of us
Overall