Embed Size (px)
Citation preview

UpdateonNovelTherapiesintheMyelomaPipeline
SuzanneTrudel,MD,FRCPCAssociateProfessorofMedicine
Consultant,DivisionofHematology/OncologyPrincessMargaretCancerCentre

Disclosures
• GrantSupport:Janssen,GlaxoSmithKline,Astellas
• Consultant:Celgene,Amgen,Novartis• Honouria:Celgene,Amgen,Takeda
Case
64 yo female diagnosed with MM in 2009. Treated with CYBORD induction and ASCT first line. Received CYBORD + salvage transplant + revlimid maintenance for first relapse and carfilzomib + pom + dex (on clinical trial) for second relapse. What treatment would you consider for this patient:
A) DaratumamabB) SelinexorC) VenetoclaxD) Car-T cell therapy E ) All of the above
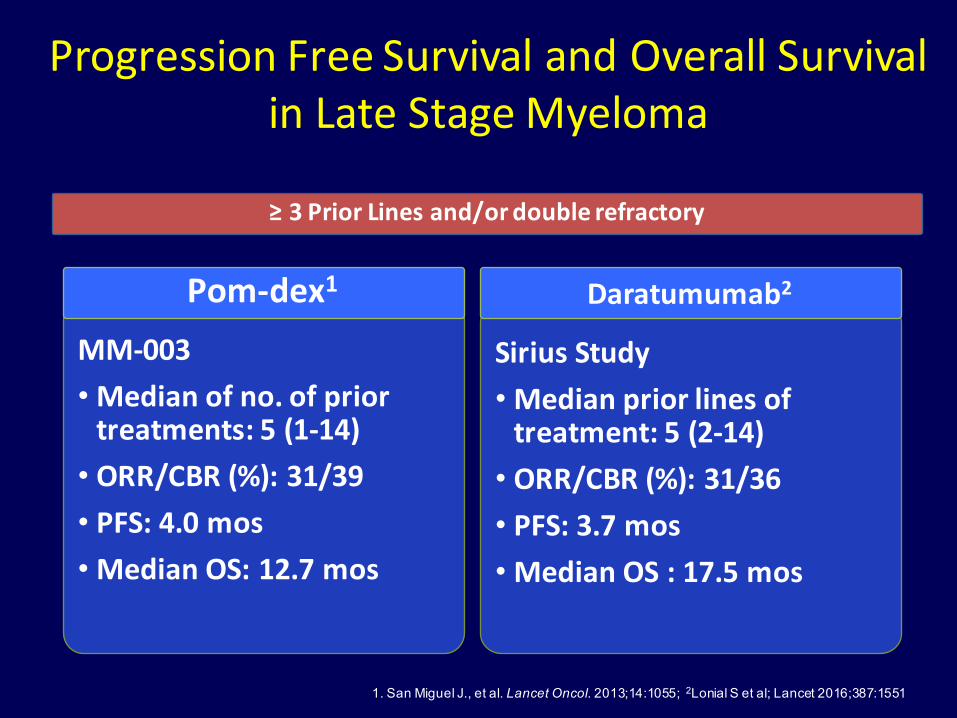
ProgressionFreeSurvivalandOverallSurvivalinLateStageMyeloma
1. San Miguel J., et al. Lancet Oncol. 2013;14:1055; 2Lonial S et al; Lancet 2016;387:1551
MM-003• Medianofno.ofpriortreatments:5(1-14)
• ORR/CBR(%):31/39• PFS:4.0mos• MedianOS:12.7mos
Pom-dex1
SiriusStudy• Medianpriorlinesoftreatment:5(2-14)
• ORR/CBR(%):31/36• PFS:3.7mos• MedianOS:17.5mos
Daratumumab2
≥3PriorLinesand/ordoublerefractory

What’sNewinMMTherapeutics?
• Oprozomib
Oralproteasomeinhibitors
• Afuresertib (AKTinhibitor)
• Dinaciclib(CDKinhibitor)
• LGH447(PIMkinaseinhibitor)
• Trametinib (MEKinhibitor)
• JNJ-4275693(FGFR3)
Kinaseinhibitors
• Ricolinostat(HDAC6inhibitor)
HDACs
• Venetoclax(Bcl2inhibitor)
• Selinexor(XPO-1inhibitor)
Novelmechanisms
• CAR-T
• BispecificTcellengagers(BiTEs)
• Checkpointinhibitors (PDL-1/PD-L1)
• Antibody-drugconjugates(ADC)
Immuno-therapies
HDAC,histonedeacetylase.

ProfileofSingle-AgentOprozomibinPatientsWithMultipleMyeloma:
UpdatedResultsFromaMulticenter,Open-Label,Dose-EscalationPhase
1b/2Study
RaviVij,1 MichaelSavona,2 DavidSiegel,3 JonathanKaufman,4 AshrafBadros,5 IreneGhobrial,6 AgnePaner,7
SundarJagannath,8 AndrzejJakubowiak,9 JosephMikhael,10 PrashantKapoor,11 LindaNeuman,12 JesusBerdeja13
1WashingtonUniversity,St.Louis,MO;2VanderbiltUniversity,Nashville,TN;3JohnTheurerCancerCenteratHackensackUniversityMedicalCenter,Hackensack,NJ;4WinshipCancerInstitute,EmoryUniversity,Atlanta,GA;5UniversityofMaryland,Baltimore,MD;6Dana-FarberCancerInstitute,Boston,MA;7RushUniversity,Chicago,IL;8Mt.SinaiHospital,NewYork,NY;9UniversityofChicagoMedicalCenter,Chicago,IL;10MayoClinic,Scottsdale,AZ;11MayoClinic,Rochester,MN;12OnyxPharmaceuticals,Inc.,anAmgen
subsidiary,SouthSanFrancisco,CA;13SarahCannonResearchInstitute,Nashville,TN
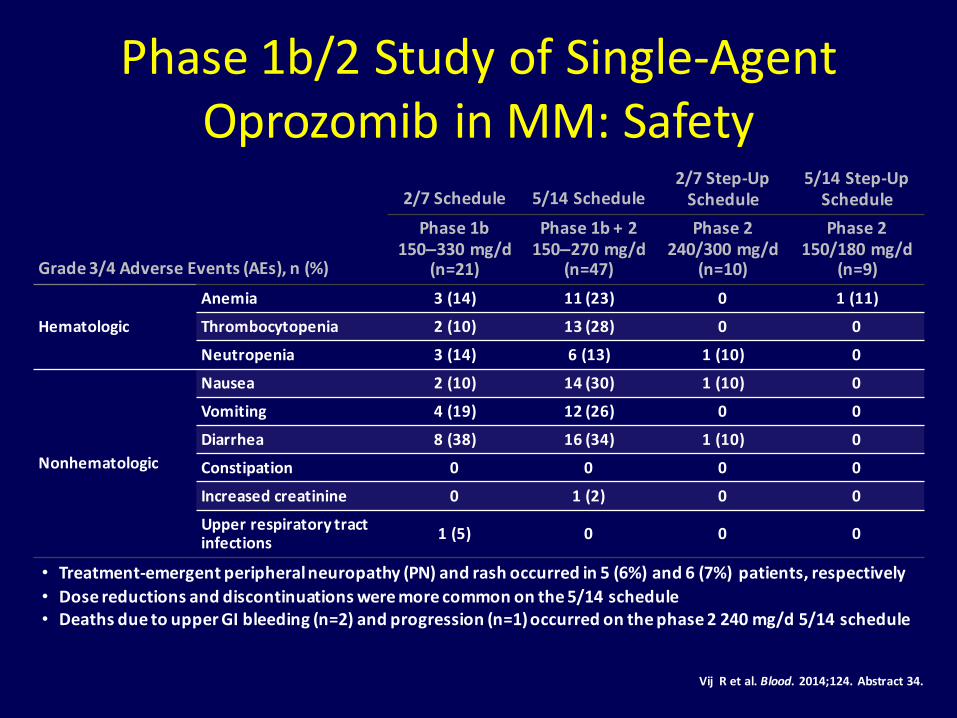
Phase1b/2StudyofSingle-AgentOprozomibinMM:Safety
VijRetal.Blood.2014;124.Abstract34.
Grade3/4AdverseEvents(AEs),n(%)
2/7Schedule 5/14Schedule2/7Step-UpSchedule
5/14Step-UpSchedule
Phase1b150–330mg/d
(n=21)
Phase1b+2150–270mg/d
(n=47)
Phase2240/300mg/d
(n=10)
Phase2150/180mg/d
(n=9)
Hematologic
Anemia 3(14) 11(23) 0 1(11)
Thrombocytopenia 2(10) 13(28) 0 0
Neutropenia 3(14) 6(13) 1(10) 0
Nonhematologic
Nausea 2(10) 14(30) 1(10) 0
Vomiting 4(19) 12(26) 0 0
Diarrhea 8(38) 16(34) 1(10) 0
Constipation 0 0 0 0
Increasedcreatinine 0 1(2) 0 0
Upperrespiratorytractinfections 1(5) 0 0 0
• Treatment-emergentperipheralneuropathy(PN)andrashoccurredin5(6%)and6(7%) patients,respectively• Dosereductionsanddiscontinuationsweremorecommononthe5/14schedule• DeathsduetoupperGIbleeding(n=2)andprogression(n=1)occurredonthephase2240mg/d5/14schedule

Phase1b/2StudyofSingle-AgentOprozomibinMM:Efficacy
5/14Sched
ule2
2/7Sche
dule
1
Patients,%
CBR50%
CBR32.6%
ORR31.3%
ORR23.3%3
12/7schedule:1patient(6%)wasnotevaluable.25/14schedule:5patients(12%)werenotevaluableand2patients(5%)wereoffstudybeforeresponseassessment.
3ORRin11CFZ-refractorypatients(phase2):18.2%.
Response data not shown for step-up cohorts due to limited treatment exposure
VijRetal.Blood.2014;124.Abstract34.
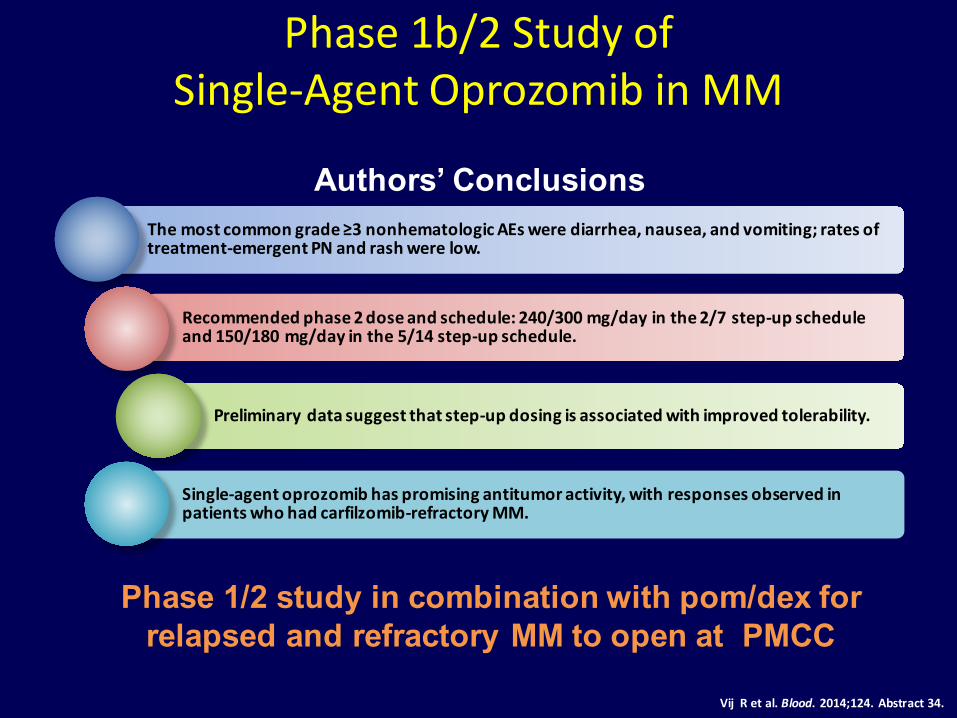
Phase1b/2StudyofSingle-AgentOprozomibinMM
VijRetal.Blood.2014;124.Abstract34.
Authors’ ConclusionsThemostcommongrade≥3nonhematologicAEswerediarrhea,nausea,andvomiting;ratesoftreatment-emergentPNandrashwerelow.
Recommendedphase2doseandschedule:240/300mg/dayinthe2/7step-upscheduleand150/180mg/dayinthe5/14step-upschedule.
Preliminarydatasuggestthatstep-updosingisassociatedwithimprovedtolerability.
Single-agentoprozomibhaspromisingantitumoractivity,withresponsesobservedinpatientswhohadcarfilzomib-refractoryMM.
Phase 1/2 study in combination with pom/dex for relapsed and refractory MM to open at PMCC
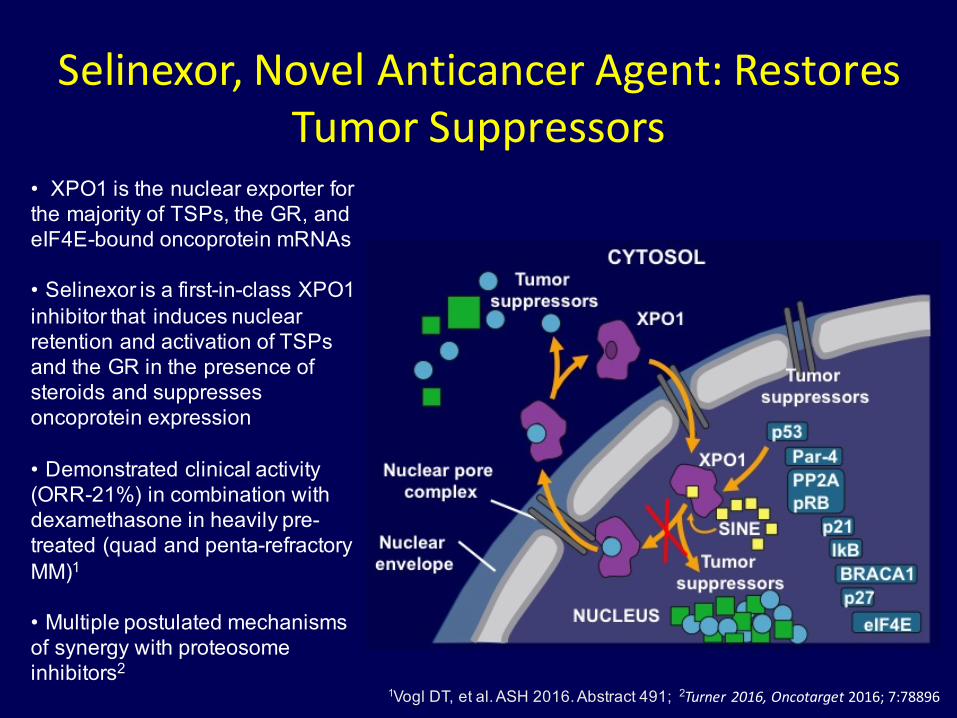
Selinexor,NovelAnticancerAgent:RestoresTumorSuppressors
• XPO1 is the nuclear exporter for the majority of TSPs, the GR, and eIF4E-bound oncoprotein mRNAs
• Selinexor is a first-in-class XPO1 inhibitor that induces nuclear retention and activation of TSPs and the GR in the presence of steroids and suppresses oncoprotein expression
• Demonstrated clinical activity (ORR-21%) in combination with dexamethasone in heavily pre-treated (quad and penta-refractory MM)1
• Multiple postulated mechanisms of synergy with proteosome inhibitors2
1Vogl DT, et al. ASH 2016. Abstract 491; 2Turner2016,Oncotarget 2016;7:78896

SelinexorandbackboneTreatmentsOfmultipleMyelomaPatients:STOMPStudyDesign
§ Primary Objective: Determine the maximum tolerated dose (MTD) and recommended Phase II dose (RP2D)
§ Patient Populations: § Arm SVd: selinexor + bortezomib + dexamethasone
§ MM patients relapsing after ≥ 1 prior therapy may include prior bortezomib, as long as not refractory to bortezomib in their most recent line of therapy
§ Arm SPd: selinexor + pomalidomide + dexamethasone (ASH 2016 - Poster 3330)
§ Arm SLd: selinexor + lenalidomide + dexamethasone § Dosing Scheme SVd: A standard 3 + 3 design will be used for dose escalations:
Bahlis N et al. ASH 2017; 977a
45% 40%
57%
40%50% 50%
18%
13%
29%
30% 8%
33%9%
7%
14%
10%
8%
17%
5%
7%8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
AllPa1ents(N=22) PIRefractory(N=15)
PINon-Refractory(N=7)
PriorTherapies1-3(N=10)
PriorTherapies≥4(N=12)
PINon-Refractory&1-3Priors(N=6)
sCR CR VGPR PR
12
ORR 67%
ORR 77%
ORR 100% ORR 100%
ORR 80%ORR 74%
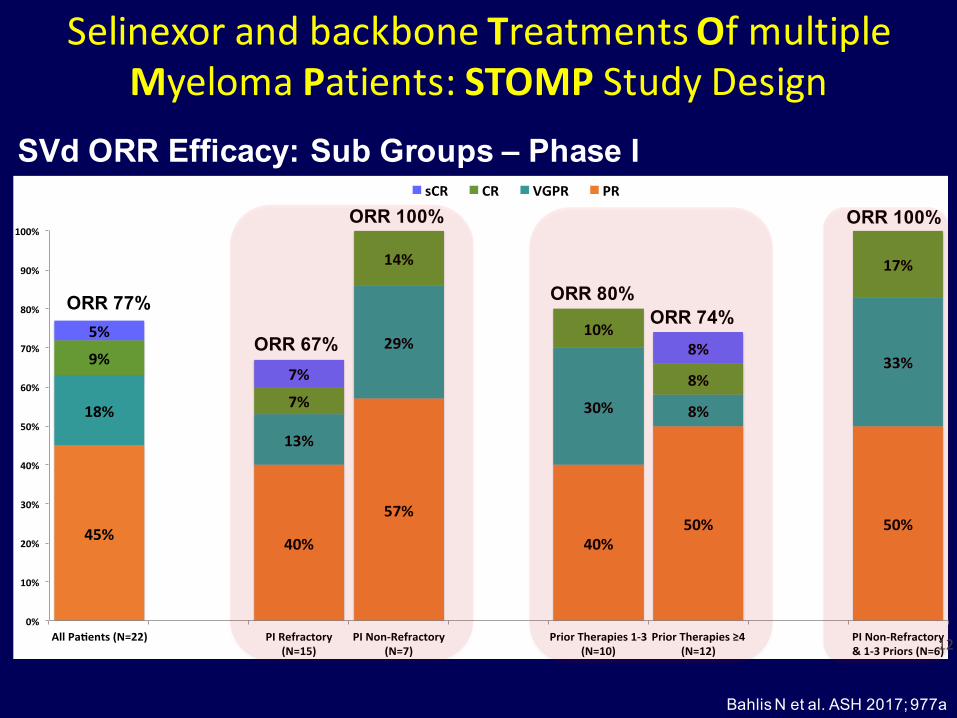
SelinexorandbackboneTreatmentsOfmultipleMyelomaPatients:STOMPStudyDesign
SVd ORR Efficacy: Sub Groups – Phase I
Bahlis N et al. ASH 2017; 977a

SelinexorandbackboneTreatmentsOfmultipleMyelomaPatients:STOMPStudyDesign
100 mg oral selinexor QW + 1.3 mg/m2 bortezomib SC QW x 4 / 5 +
40 mg dexamethasone QW
§ Good tolerability with clear anti-MM activity with once weekly selinexor in combination with once weekly Velcade
§ Considering prolonged tolerability and efficacy across all cohorts, the RP2D is:
TreatmentRelatedAEsatRP2D
Bahlis N et al. ASH 2017; 977a

SelinexorandbackboneTreatmentsOfmultipleMyelomaPatients:STOMPStudyDesign
Authors’ Conclusions§ TherecommendedSVdphaseIIdose:weekly POselinexor100mg,scbortezomib1.3mg/m2
andPOdexamethasone40mg.
Selinexor incombinationwithbortezomib andlowdosedexamethasone (SVd)iswelltoleratedwithlowratesofmajoradverseevents.
§ AEs weremanageable(predominantlyG1/2)andincludednausea,fatigue,anorexia,andthrombocytopenia(mostlyG3/G4).
SVdhaspotentactivityinpatientswithORR77%,67%inPI-refractorydisease,and100%inPI-non-refractory.
Convenient,cost-effectiveandhighlypotentanti-MMregimen.
Phase 3 Randomized BOSTON Study of SVd vs Vd to now open at PMCC
Bahlis N et al. ASH 2017; 977a

Celldeath(apoptosis)
InhibitionofBcl-2CriticalforApoptosis
DeathBH3-only
Bim Bid
Puma
Bak
Bax
MultidomainDeathtriggers Executioners
Caspaseactivation
ActivatedBAX/BAK
Mitochondria
CytC
Bik
Bmf
Bad
NoxaHrk
Bcl-2 Bcl-w
Bcl-xL Mcl-1A-1
Survival
Guardians
Sentinels
Signalsofcellulardamage
TargetsBcl-2
Venetoclax
1. Touzeau C, et al. Leukemia. 2014;28:210-214. 2. Punnouse EA, et al. Mol Cancer Ther.
• Survival of MM cells promoted by proteins BCL-2 and MCL-1[1]
• t(11;14) correlated with higher ratios of BCL2/MCL1 and BCL2/BCL2L1 (BCL-XL) mRNA[1,2]
• In vitro, cells positive for t(11;14) particularly susceptible to venotoclax[1,2]

VenetoclaxMonotherapyforRRMM:ORR
• In subset analysis of pts with t(11;14), similar ORR seen across subgroups with MM refractory to various single agents or multiple agents
Outcome, %Overall
Population(N = 66)
Pts With t(11;14)(n = 30)
Pts Without t(11;14)(n = 36)
Pts With High
BCL2/BCL2L1
(n = 9)
Pts With Low
BCL2/BCL2L1
(n = 15)
ORR 21 40 6 88 20sCR 3 4 3 11 0CR 4 10 0 33 0VGPR 8 13 3 11 13PR 6 13 0 33 7
Kumar S, et al. ASH 2016. Abstract 488
• Patients with RRMM; ECOG PS 0/1 and adequate organ function (N = 66)
• ≥ 70% refractory to bortezomib or lenalidomide; 61% refractory to both
• Dose-limiting toxicity (600 mg): abdominal pain, nausea (n = 2)
• No tumor lysis syndrome documented

VenetoclaxMonotherapyforRRMM:TTP
Kumar S, et al. ASH 2016. Abstract 488
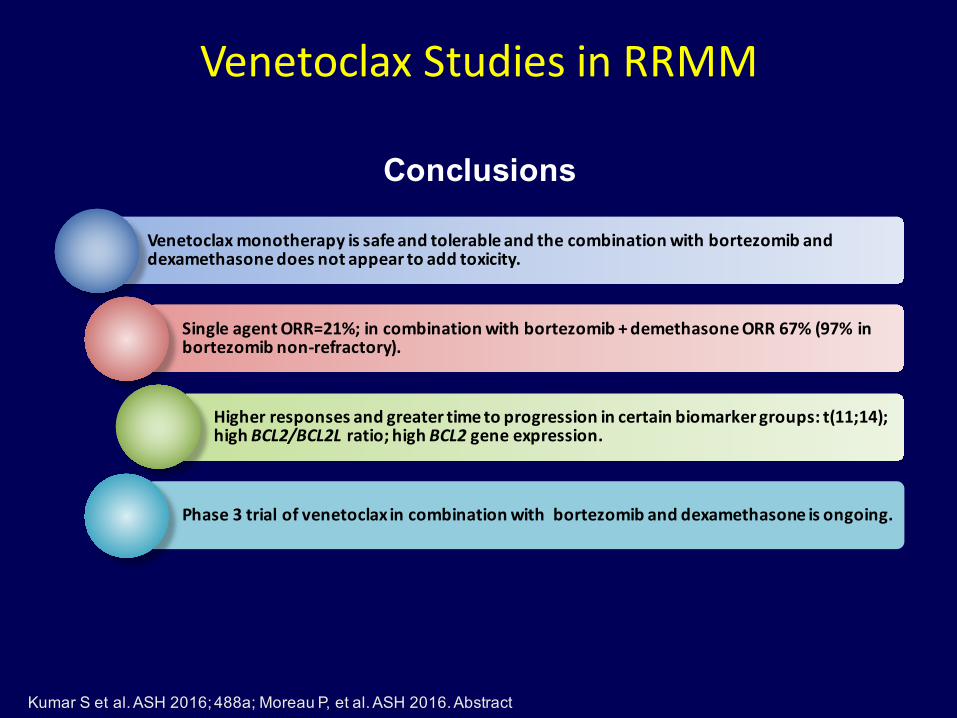
VenetoclaxStudiesinRRMM
Conclusions
Venetoclaxmonotherapyissafeandtolerableandthecombinationwithbortezomibanddexamethasonedoesnotappeartoaddtoxicity.
SingleagentORR=21%;incombinationwithbortezomib+demethasoneORR67%(97%inbortezomibnon-refractory).
Higherresponsesandgreatertimetoprogressionincertainbiomarkergroups:t(11;14);highBCL2/BCL2Lratio;highBCL2 geneexpression.
Phase3trialofvenetoclaxincombinationwithbortezomibanddexamethasoneisongoing.
Kumar S et al. ASH 2016; 488a; Moreau P, et al. ASH 2016. Abstract

FGFR3 is an actionable target for t(4;14) MM
1Chesi M et al. Heamtology AM Soc Hematol Educ Program 2011;2011:344;1Keats JJ et al. Blood 2003;101:1520; 3Santra et al. Blood 2003;101:2374;4Auclair (unpublished data) 4Chang H. et al, Blood 2005;106:353:Trudel et. al, Blood, 2004;103:3521.
• t(4;14) is present in approx 15% of MM patients1
•Activating mutations of FGFR3 were detected in 17 of 57 (30%) FGFR3 expressing newly diagnosed cases, representing an overall incidence of 3% (similar results in MMGI)4 (Data from CoMMpass Study)
• Inhibition of FGFR3 kinase activity inhibits malignant transformation and induced apoptosis of constitutively activated FGFR3 expressing MM cells

JNJ-42756493(FGFRInhibitor)

JNJ42756493+pulsedexx1cycle
\
TrialDesign ScreeningBMRNAseq* and
correlativestudies
FGFR3translocation/FGFR3WT FGFR3mutated
Cycle2/Day1BMforcorrelativestudies
BMforcorrelativestudies
JNJ42756493+pulsedexx1cycle
JNJ42756493+low-dosedexuntilprogression
Documented FGFR3 expression and mutational status must be obtained at screening. Patients in whom FGFR3 expression or mutational status cannot be confirmed will be deemed ineligible 10pts10pts
*MMRF Clinical-grade Sequencing Initiative

Immunotherapeutic Strategies in Development for MM
Neri P et al., Clin Cancer Res 2016; 22:OF1-7
Bispecific T-cell engagers (BiTes)
Antibody Drug Conjugates (ADCs)
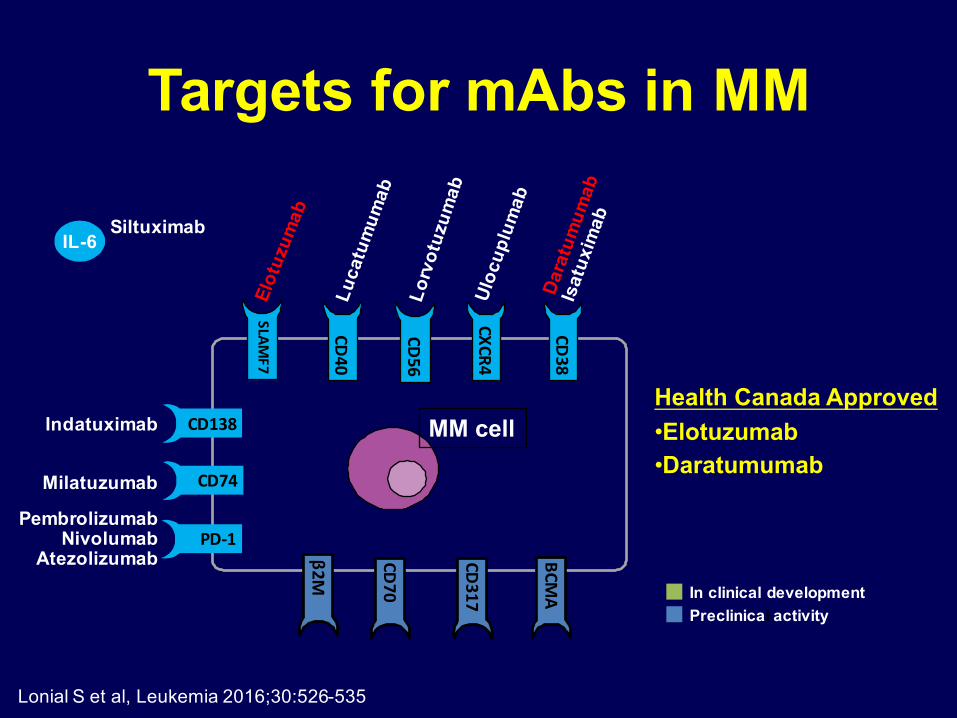
Targets for mAbs in MM
Health Canada Approved•Elotuzumab•Daratumumab
IL-6
CD38
CD40
CD56
CXCR4CD74
PD-1
CD138
β2M
MM cell
SLAMF7
Milatuzumab
PembrolizumabNivolumab
Atezolizumab
Indatuximab
Siltuximab
In clinical developmentPreclinical activity
BCMA
CD70
CD317
Lonial S et al, Leukemia 2016;30:526-535

PhaseIbPAVOStudy:SCDaratumumabinRelapsed/RefractoryMultipleMyeloma
§ Open-label,multicenter,dose-finding,proof-of-conceptphaseIbstudy
§ Primaryendpoints: Ctrough ofdaratumumabatcycle3Day1andsafety;secondaryendpoints:ORR,CR,DoR,timetoresponse
Usmani SZ, et al. ASH 2016. Abstract 1149.
Pts with measurable R/R MM, ≥ 2 lines of therapy, no prior anti-
CD38 therapy(N = 53)
*Pre/postinfusion medication includes acetaminophen, diphenhydramine, montelukast, and methylprednisolone.
Daratumumab 1200 mg SC + rHuPH20 30,000 U SC
(n = 8)*
Daratumumab 1800 mg SC + rHuPH20 45,000 U SC
(n = 45)*
4-wk treatment cycles§Every wk for 8 wks§Every 2 wks for 16 wks§Every 4 wks thereafter
Infusion time§1200 mg: 20 min (60 mL)§1800 mg: 30 min (90 mL)
Characteristic 1200 mg (n = 8) 1800 mg (n = 45)Prior lines of therapy, median (range) 5 (2-10) 4 (2-11)Refractory to PI only/IMiD only, % 0/13 4/20Refractory to both PI and IMiD, % 63 58Refractory to last line of therapy, % 88 71
PAVO:Conclusions§ SCadministrationofdaratumumab+rHuPH20safeandeffective
§ BothdosegroupsshowedresponsestoSCdaratumumab
– 1800-mggrouphaddeeperresponsesvs1200-mggroup
– PreliminaryefficacysimilartoIVdaratumumab:38%ORR,including1sCR
§ Adverseevents(AEs)forSCdaratumumab+rHuPH20similartoIVdaratumumabwithnonewsafetysignals
– Lowincidence(24%at1800mgdose)andintensity(1/53grade3,nograde4)ofinfusionrelatedreactions(IRRs)withSCdaratumumab
§ PKofSCdaratumumab1800mgsimilarto16mg/kgIVadministration
Usmani SZ, et al. ASH 2016. Abstract 1149.
Phase 3 Randomized sc vs IV to open at PMCC

BCMA
EffectorCell
MechanismsofAction:1. ADC
mechanism2. ADCC
mechanism3. Immunogenic
celldeath
xBCMA
BCMA
BCMA
GSK2857916
Lysosome
FcReceptor
ADCC
ADC
Cell death
MalignantPlasmaCell
GSK2857916:BMCAAntibodyDrugConjugated(ADC)
• BCMA is restricted to B cells at later stages of differentiation, broadly expressed on malignant PCs
• GSK2857917 is a human IgG1 anti-BCMA Ab conjugated to Monomethyl auristatine-F
– Targetspecific– EnhancedADCC
FcregionoftheAntibody
– StableincirculationLinker
– MMAF(noncellpermeable, highlypotent auristatin
Drug
ADC, antibody-drug conjugate; ADCC, antibody-dependent cell-mediated cytotoxicity; BCMA, B-cell maturation antigen; Fc, Fragment crystallizable; IgG, immunoglobulin G; MMAF, monomethyl auristatin-F
1Tai YT, et al. Blood 2014;123(20):3128-38; 2Cohen et al, ASH 2016; 1148a

*
Patient ongoing
Patient completed 16 cycles
First-in-HumanStudyofGSK2857916:Part1:ClinicalActivityandDurationonStudy
40 60 100 1400 1601208020 340320300280260240220200180 360
PDSD
PDPDSDPD
MissingMissing
SDMR
MissingMissing
SDSD
PDPD
PRSD
SDMR
VGPRSCR
VGPRPR
SDPR
MRVGPR
PRSD
0.03 mg/kg0.06 mg/kg0.12 mg/kg0.24 mg/kg0.48 mg/kg0.96 mg/kg1.92 mg/kg3.40 mg/kg4.60 mg/kg
Study treatment duration (days)
Patie
nts
6 months
≤1.92 mg/kg, n=21ORR=9.5%
≥3.4 mg/kg, n=9ORR= 66.7%
Cycle 8: increased to 0.48
Cycle 13: to 0.96
*
• First in human, dose escalation• n=30 patients at escalating doses; 70% > 5 prior lines• 100% IMiDs exposed, 100% PI exposed, 90% double refractory
Cohen et al, ASH 2016; 1148a

AEs reported in ≥20% patients, n (%)
N=30Any grade ≥Grade 3*
Any event 29 (97) 22 (73)Ocular Toxicity 16 (53) 2 (7)Nausea 15 (50) 0Thrombocytopenia 15 (50) 13 (43)Fatigue 14 (47) 1 (3)Anemia 10 (33) 6 (20)Pyrexia 10 (33) 0Chills 8 (27) 0AST increased 6 (20) 0Hypercalcemia 6 (20) 3 (10)Neutropenia 6 (20) 4 (13)
First-in-HumanStudyofGSK2857916:Part1:AEsRegardlessofRelationship
AE,adverseevent; IRR,infusion-relatedreactions
– MajorityofAEswereGrade1/2andpredicted
– 8/30(27%)patientsexperienced IRR(reportedacrossdoselevels),all Grade1/2; chills was most frequent symptom– Grade3ocularevents:dryeyein1patientimproved; inanother,limbalstemcelldeficiency resolved
– Thrombocytopeniawastransient
Cohen et al, ASH 2016; 1148a

FirstinHumanStudywithGSK2857916,inPatientswithRelapsed/RefractoryMultipleMyeloma:
ResultsfromStudyBMA117159Part1DoseEscalation
GSK2857916waswelltoleratedwithnodoselimitedtoxicities(DLTs);Maximumtolerateddose(MTD)wasnotreached
Adverseevents(AEs)weremanageablewithcornealtoxicitiesemergingasthemostfrequentreasonfordosemodification
Thrombocytopeniaemergedmorefrequentlyastreatment-relatedathigherdoses;althougheventsweretransientandmanageable
66.7%ORRincludingastringentCRobservedathigherdosesinthisrefractorypatientpopulation
3.4mg/kgwasselectedasthedosetoinvestigateintheexpansionphase
Authors’ Conclusions
Cohen et al, ASH 2016; 1148a
Phase 1/2 study in combination with pom/dex for relapsed and refractory MM underdevelopment and planned to open 2018

Immunotherapeutic Strategies in Development for MM
Neri P et al., Clin Cancer Res 2016; 22:OF1-7
Bispecific T-cell engagers (BiTes)
Antibody Drug Conjugates (ADCs)

AdoptiveCellTherapy– CARTcells
Autologous T cells can be genetically modified to express chimeric antigen receptors (CARs) specific for malignancy-associated antigens

BCMA-Specific CAR in RRMM
Cohen et el ASH 2016; 1147a

Bispecific T cell engagers (BiTEs)
IgG Like• Longer serum half-life • Retain Fc function
Non IgG Like• Better tissue penetrance • Better access to epitopes

BCMA Bispecific Antibodies in Myeloma

Immunotherapeutic Strategies in Development for MM
Neri P et al., Clin Cancer Res 2016; 22:OF1-7
Bispecific T-cell engagers (BiTes)
Antibody Drug Conjugates (ADCs)

Tumor-Mediated Immune Paralysis: PD1 checkpoint pathway
• mAb targeting PD-1/PD-L1 are approved for the treatment of solid tumors• Activities as single agents in myeloma are very modest
• (Single agent Nivolumab 1 CR, N=24; ORR=4%)1
1Lesokhin AM, et al, J Clin Oncol 2016;34:2698-704.

Pembrolizumab inCombinationwithLenalidomide andLow-doseDexamethasone forRRMM(Keynote023)
Mateos M-V, et al. J Clin Oncol 2016;34(suppl):8010a

Phase 1/2 Study: Penbrolizumab + Pom/dex in RRMM
Anti-tumor activity
Badros A, et al. ASH 2016; 490a

Pembrolizumab/Pom/DexaforRRMM
InthissmallstudyofpatientswithRRMM,thecombinationofpembro/pom/dex appearsactive
Adverseevents(AEs)occurredin~50%ofthestudypopulations- Pneumonitis in12%;Discontinuationin10%;mostAEs manageable
HighqualityresponseswereobservedinthosepositiveforPD-L1expressionandwithT-cellinfiltratethatisCD3-/PD-1-
Authors’ Conclusions
Badros A, et al. ASH 2016; 490a
TheresultssuggestthatfuturestudiesarewarrantedtofurtherunderstandtheroleofPD-1/PD-L1inhibitorsinpatientswithMM

Summary• Oralproteasomeinhibitorsareactive;Phase1bstudyofOprozomibincombination
withpom/dextoopensoon
• Selinexorbeingdevelopedincombinations;PhaseIIIofselinexorcombinedwithbortezomibanddex(BOSTONtrial)nowopenatPMCC
• Venetoclaxsingleagentandincombinationforselectpatientpopulationsalsopromising(biomarkerstoidentifytargetpopulationsneedtodevelopinparallel)
• JNJ-42756493(FGFR3inhibitor)willbeevaluatedinpatientswitht(4;14)myelomawithandwithoutFGFR3mutations
• ImmunotherapyforMMhascomeofage– Daratumamabisanewbackbone(future: scadministration-PhaseIIIstudycomparing IV
vssctoopensoon)– BMCAnovelhighly selectivetargetforimmune therapy– GSK2857916highlyactiveassingleagentandwillbeevaluatedincombinations;Phase
1/2incombinationwithpom/dextoopen in2017– BITESandcheckpointinhibitors: toosoon tosay(multiple studiesofanti-PD-1andPD-L1
incombinationsandinvariousmyelomapopulations openandenrolling)– CAR-Tpromising butneedoptimization (BMCACAR-Tplanned toopen2017)

Venetoclax Combined With Bortezomib and Dexamethasone for Patients With RRMM
ORR=PR or better; numbers are based on evaluable patients per subgroups.
Data cutoff of 19Aug2016
• Median prior lines of therapy 3 (1-13)
Moreau P, et al. ASH 2016. Abstract
ORR for all patients was 67% and 90% for bortezomib non-refractory

Venetoclax Combined With Bortezomib and Dexamethasone for Patients With RRMM
ORR: BLC2 high 94%BLC2 love 59%
TTP: bortezomib non-refractory 11.3 monthsbortexomib refractory 1.8 months
Bortezomib refractory
Moreau P, et al. ASH 2016. Abstract





























