Embed Size (px)
Citation preview

Update on novel combinations for relapsed/refractory disease: “Coming soon”
1
Tomer M. MarkDepartment of Medicine, Division of Hematology /
OncologyWeill-Cornell Medical College /
New York Presbyterian Hospital, New York, NY, USA
Lymphoma & Myeloma 2012

Disclosures
2
Research Funding: Celgene Inc.; Onyx Inc.
Speakers Bureau: Celgene Corp; Millenium Inc.; Sanofi-Aventins Inc.; Onyx Inc.
Membership on an entity's advisory committees: Celgene Corp. There is no FDA indication for pomalidomide or elotuzumab at this time.
Off-label uses of bortezomib and lenalidomide are discussed.

“Novel Agents”
• New drugs not yet available on the market– Elotuzumab
• Single-agent• In combination with bortezomib• In combination with lenalidomide
– Pomalidomide• Single-agent• In combinations
3
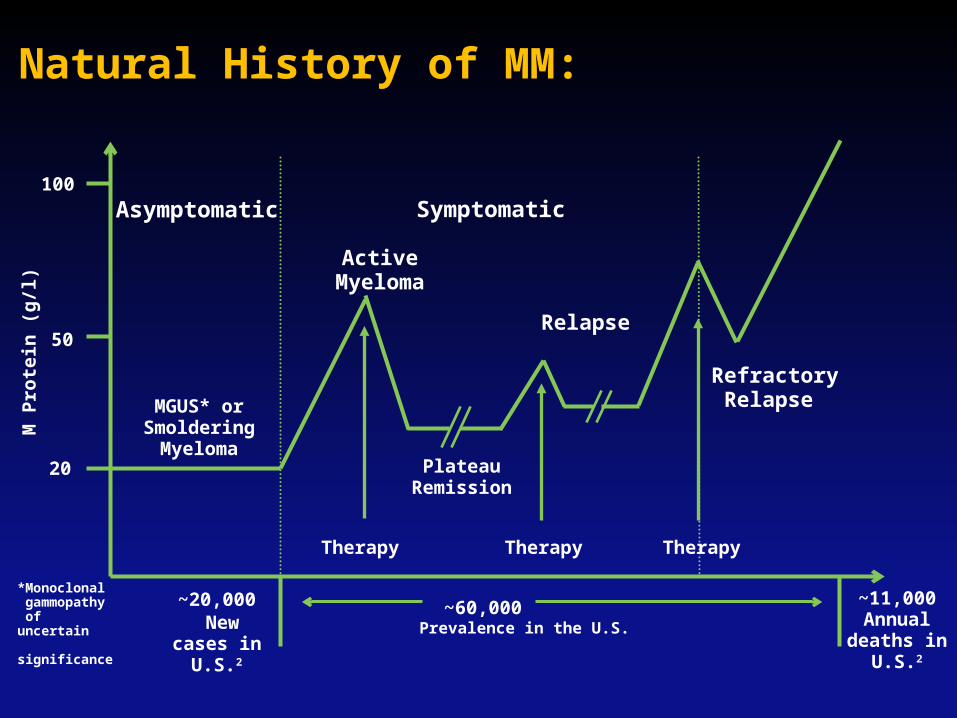
Natural History of MM:
Asymptomatic
20
50
100
Refractory Relapse MGUS* or
SmolderingMyeloma
Active Myeloma
Plateau Remission
Symptomatic
Relapse
Therapy
~60,000~20,000 New cases
in U.S.2
~11,000 Annual
deaths in U.S.2
Prevalence in the U.S.
M P
rote
in (
g/l
)
*Monoclonal gammopathy of uncertain significance
Therapy Therapy

Myeloma after bortezomib and lenalidomide
5
• What is the outlook for MM refractory to both bortezomib and an IMiD?– Retrospective study of 286 pts treated at nine sites
T0 = time eligibility met
Kumar et al., 2012, Leukemia, 26, 149-157
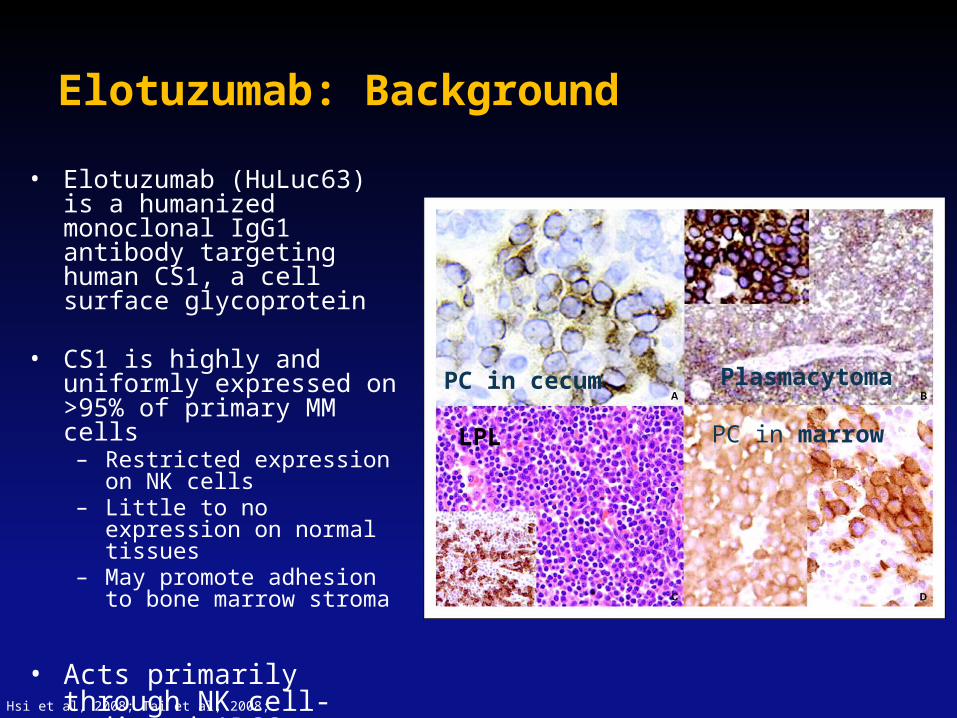
Elotuzumab: Background
• Elotuzumab (HuLuc63) is a humanized monoclonal IgG1 antibody targeting human CS1, a cell surface glycoprotein
• CS1 is highly and uniformly expressed on >95% of primary MM cells– Restricted expression on
NK cells– Little to no expression on
normal tissues– May promote adhesion to
bone marrow stroma
• Acts primarily through NK cell-mediated ADCC
Hsi et al, 2008; Tai et al, 2008;
PC in cecum Plasmacytoma
LPL PC in marrow

Elotuzumab: single agent experience
• Phase 1 study: doses 0.5-20mg/kg every two weeks, n = 54
• Median # prior tx: 4.5; len (82%), thal (80%), bort (82%)
• No objective responses seen; 9 pts (26.5%) with SD.
• MTD not seen
Zonder et al., 2012, Blood, 120, 552-9.
7

Elotuzumab: MM xenograft model
• The combination of elotuzumab and bortezomib worked better than either agent alone…
8van Rhee F et al. Mol Cancer Ther 2009;8:2616-2624

Elotuzumab + Bortezomib:
9
Jakubowiak A J et al. JCO 2012;30:1960-1965
©2012 by American Society of Clinical Oncology
Phase 1 study• N = 28, median 2 prior tx (64% prior bort, 39% prior len, 43% refractory
to last tx)• Elo: (5,10,20 mg/kg); bortezomib 1.3mg/m2 IV; (no dexamethasone).• DLT assessed in cycle 1; no MTD was found

Elo + Bort + Dex: efficacy
10
Response All pts Prior Bort Bort Refr (n=3)
Prior Len Refractory to last tx
ORR 48% 45% 0 42% 45%
CR 7% 0 0 8% 9%
PR 41% 45% 67% 33% 36%
MR 15% 0 0 8% 18%
SD 30% 45% 0 33% 27%
PD 7% 9% 33% 17% 9%
• 2/3 patients refractory to bort with PR• Favorable results compared to Phase III APEX study.
APEX(n=333)
38%
6%
32%
---
---
---
Richardson P. et al. Blood. 2008. 110(10): 3557-60.

• Median TTP = 9.36m• APEX median TTP = 6.2m
11
Kaplan-Meier analysis of time to disease progression.
Jakubowiak A J et al. JCO 2012;30:1960-1965©2012 by American Society of Clinical Oncology

Elo + Bort: Most Common Adverse Events
• 71% (20/28) pts had at least 1 infusion reaction, incl nausea, dyspnea, chills, dizzyness, headache, vomiting, rash – all Grade 1 or 2; One grade 3 hypersensitivity rxn
12
Adverse Event All Grades (%) Grade 3 / 4 (%)
Fatigue 82 14
Anemia 71 14
Diarrhea 71 0
Thrombocytopenia 68 11
Hyperglycemia 61 11
Nausea 61 0
Neutropenia 50 11

Elotuzumab: xenograft model
13
• The combination of elotuzumab and lenalidomide worked better than either agent alone…
Lonial S et al. Blood. 2009;114:432

Lonial S et al. JCO 2012;30:1953-1959
©2012 by American Society of Clinical Oncology
Elotuzumab + Lenalidomide / Dex in RRMM
Phase 1 study• N = 29, median 3 prior tx (69% prior bort, 21% prior len)• Elo: (5,10,20 mg/kg); len 25mg 21/28d, dex 40mg weekly• DLT assessed in cycle 1; no MTD was found

Elo + Len + Dex: efficacy
15
Response All pts Len-naïve Prior thal Prior bort Refractory to last tx
ORR 82% 95% 94% 75% 83%
CR 4% 5% 0 5% 0
VGPR 29% 32% 44% 20% 33%
PR 50% 59% 50% 50% 50%
SD 11% 5% 6% 15% 17%
PD 7% 0 0 10%
MM-009 MM-010
61% 60%
14% 16%
10% 9%
37% 36%
31% 30%
3% 2%
• 6 with prior len: 1 CR, 1 VGPR

Kaplan-Meier estimate of time to disease progression for the 20-mg/kg cohort (n = 22).
Lonial S et al. JCO 2012;30:1953-1959
©2012 by American Society of Clinical Oncology

Elo + Len + Dex: Most Common Adverse Events
• 89% (25/28) pts had at least 1 infusion reaction, incl nausea, dyspnea, chills, dizzyness, sweating, cough, rash
• 2 pts withdrew for tox: 1 pt with stridor, 1 with anaphylaxis
17
Adverse Event All Grades (%) Grade 3 / 4 (%)
Fatigue 61 11
Anemia 46 7
Diarrhea 50 11
Nausea 43
Constipation 39 4
Neutropenia 39 36
Muscle Spasms 32

Future of elotuzumab
• Appears to enhance antitumor activity of both bortezomib and lenalidomide.
• Combination with Lenalidomide + low-dose dexamethasone: two phase III trials:– ELOQUENT-1: upfront treatment (CA204-006;
NCT01335399)– ELOQUENT-2 in RRMM (CA204-004;
NCT0123979)
• Combination with Bortezomib + low-dose dexamethasone Phase 1 / 2 trials.
18

Pomalidomide (CC-4047)
Thalidomide
Analog of thalidomide – 2nd generation IMiD– Equivalent anti-angiogenic activity– 8x greater stimulation of apoptosis– 15,000x greater inhibition of TNF-alpha production– Stimulates ADCC
Lenalidomide

Pomalidomide Mechanisms of Action:
– Anti-proliferative• Demonstrated upregulation of p23WAF1, inhibiting CDK
pathway, leading to G1/G0 arrest
– Pro-apoptotic• Enhanced sensitivity to Fas and TRAIL-induced
apoptosis
– Antiangiogenic• Decreased VEGF secretion
– Modulates bone resorption• Inhibition of differentiation of osteoclasts by down-
regulating PU.1
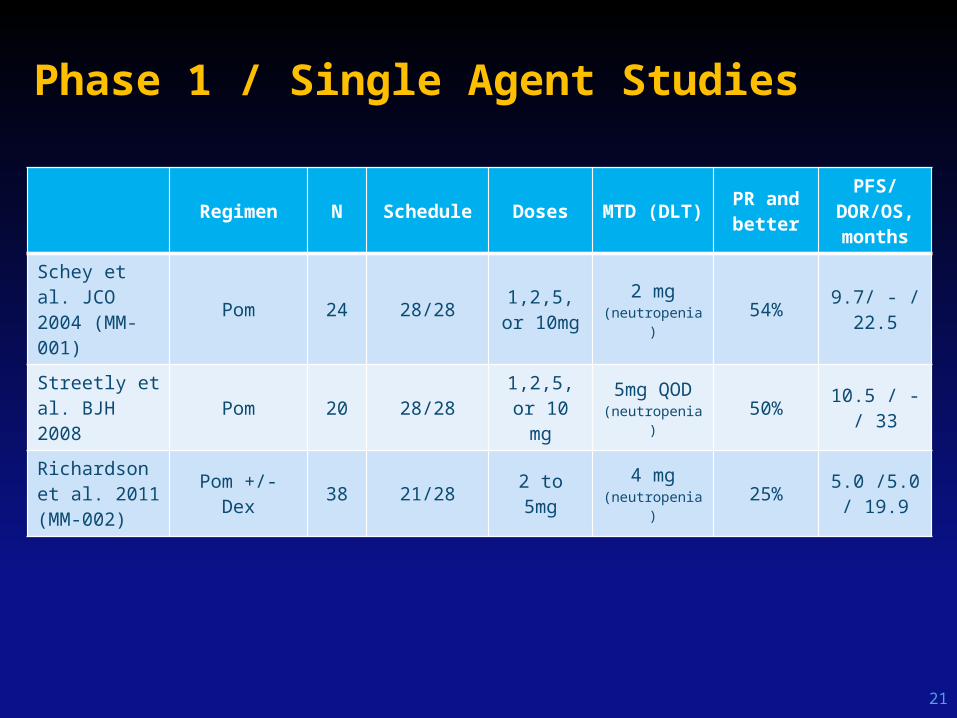
Phase 1 / Single Agent Studies
21
Regimen N Schedule Doses MTD (DLT)PR and better
PFS/DOR/OS, months
Schey et al. JCO 2004 (MM-001)
Pom 24 28/281,2,5, or
10mg2 mg
(neutropenia)54%
9.7/ - / 22.5
Streetly et al. BJH 2008 Pom 20 28/28
1,2,5, or 10 mg
5mg QOD(neutropenia)
50%10.5 / - /
33
Richardson et al. 2011(MM-002)
Pom +/- Dex 38 21/28 2 to 5mg 4 mg(neutropenia)
25%5.0 /5.0 /
19.9

Response to Pomalidomide / Dexamethasone In Previously Treated MM (Phase 2 studies)
§ Responses assessed by the investigator.Dex, dexamethasone; PR, partial response; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; Pom, pomalidomide; VGPR, very good PR.
Study # of prior Regimens
N Pom schedule (dose)
ORR, %
Lacy MQ, et al.1 2 60 28/28 (2 mg) 63
Lacy MQ, et al.2
(Len-refractory)4 34 28/28 (2 mg) 32
Leleu X, et al. 3
IFM 2009-02(Double refractory)
4 43 21/28 (4 mg) 42
4 41 28/28 (4 mg) 39
Richardson P, et al.4 MM-002
5 113 21/28 (4 mg) 34§
5 10821/28 (4 mg)
(no dex)13§
Lacy MQ, et. al.5
(Double refractory)6 35 28/28 (2 mg) 25
6 35 28/28 (4 mg) 29
1. Lacy MQ, et al. J Clin Oncol. 2009;27:5008-14. 2. Lacy MQ, et al. Leukemia. 2010;24:1934-9.
3. Leleu X, et al. IMW 2011;P-148..4. Richardson P, et al. Blood. 2011;118:[abstract 634].
5. Lacy MQ, et al. Blood. 2011;118:2970-5.

IFM 2009-02
23
Until Progression (relapse or refractory)
- Simon two stage design
- 22 IFM centres
- 92 pts included
- N=84 evaluable
STOP #1/DMC – TOLERANCERule: acceptable
STOP #2 DMC - EFFICACYRule: 4 PR and better/arm
Simon stage 1 17 pts per arm
Simon stage 2 40 pts per arm
6 pts per arm
Arm B – Cycle 28 days• Pomalidomide 4mg oral/d, d 1–28 Dexamethasone 40mg oral/w, 1, 8, 15, 22
• Aspirin/LMWH
Arm A – Cycle 21 days•Pomalidomide 4mg oral/d, 1–21 Dexamethasone 40mg oral/w, 1, 8, 15, 22• Aspirin/LMWH

Patient Characteristics at entry into IFM2009-02
24
Arm 21/28 (N = 43) 28/28 (N = 41)
Median age, years (range) 54 (39-78) 53 (36-69)
Gender ratio (M/F) 2 2
Neuropathy (all grades), N (%) 34 (79) 25 (61)
DVT/PE prophylaxis, N(%) LWMH 10 (23) 8 (19.5)
VKA 7 (16) 4 (10)
T(4;14), N(%) 0 3 (7)
Del17p, N(%) 5 (12) 4 (10)
Prior line of therapy, N (range) 4 (1-8) 4 (1-8)
Thalidomide, N (%) 20 (46.5) 24 (58.5)
Lenalidomide, N (%) (100) (100)
Bortezomib, N (%) (100) (100)
DVT: Deep Veinous Thromboembolism/PE: Pulmonary Embolism; LWMH: Low Weight Molecular Heparin; VKA: Vitamin K antagonist

Response (ITT - Central lab)
25
Arm 21/28N=43
28/28N=41
Number of cycle, median 5 5
ORR (PR and better), N(%) 18 (42) 16 (39)
sCR 0 0
CR 1 (2) 0
VGPR 3 (7) 2 (5)
PR 14 (32.5) 14 (34)
Stable disease, N(%) 20 (46.5) 21 (51)
Progression, N(%) 5 (12) 1.7 (10)
Time to best response, months (range) 2 (1-9) 1.7 (1-9)

Time To Progression (TTP)
Median follow-up is 6.5 months (arm A 21/28) and 7 months (arm B 28/28)
26
Perc
ent w
ithou
t pro
gres
sion
0.00
0.25
0.50
0.75
1.00
Days0 50 100 150 200 250 300 350 400
Arm O/N Median, months Range
21/28 19/43 7 (4 - )
28/28 16/41 9.7 (4 - )
O/N: observed number / total number

Lessons from Phase 2 Studies
• Activity present in lenalidomide-refractory patients– ORR 32% in len-refractory– ORR 25% in both len and bortez-refractory
• 4 mg daily is NOT better than 2mg• 4 mg daily is NOT better than 4mg 21/28
days• ORR correlates with # of prior lines of
therapy

Toxicities in Phase 2 studies
Toxicity Lacy 2009 (n=60)
Lacy 2010 (len refractory)
(n=34)Lacy 2011 (double - refractory
RRMM), n=70Leleu 2010 (IFM 2009-02)
n=84
2 mg 4 mg4 mg 21/28
days4 mg 28/28
days
Hematological (%) 23.5* 26.5*
Neutropenia 32 29 51 65
Thrombocytopenia 3 9 32 31
Anemia 5 12 26 26
Non-hematological (%) 23* 13* 12* 9*
Fatigue 17 9 9 9
Pneumonia 8 3 31 3
Hyperglycemia 5 3 9 3
Peripheral neuropathy
2 0 0 3
Thomboembolic complications
2 0
* No breakdown of grade 3 or 4 adverse events reported
ClaPD (Clarithromycin, Pomalidomide, Dexamethasone) Therapy in Relapsed or
Refractory Multiple Myeloma
Tomer M. Mark1, Melissa Rodriguez1, Manan Shah1, Ryann Quinn1, Jessica Campbell1, Ramsey Abdullah1, Roger Pearse1, Faiza
Zafar1, Karen Pekle1, Patrice Mignott1, David Jayabalan1, Scott A. Ely2, Morton Coleman1, Selina Chen-Kiang2, Ruben Niesvizky1
1Department of Medicine, Division of Hematology and Oncology; and 2Department of Pathology and Laboratory Medicine, Weill Cornell Medical College, New York, NY, USA
ASH 2011

Rationale for Clarithromycin
• Treatment in newly diagnosed, symptomatic MM with BiRD (clarithromycin, lenalidomide, dexamethasone) in a phase 2 trial yielded:
– N = 72, 90.3% ≥ partial response (PR), 38.9% complete response1
• Clarithromycin:
– slows hepatic clearance of dexamethasone leading to greater corticosteroid exposure2–4
– acts as a weak immunomodulatory agent5,6
• A case-control study showed superior clinical outcomes for BiRD versus lenalidomide plus low-dose dexamethasone.7
5. Takizawa H, et al. Biochem Biophys Res Commun. 1995;210:781-6.6. Matsuoka N, et al. Clin Exp Immunol. 1996;104:501-8.
7. Gay F, et al. Am J Hematol. 2010;85:664-9.
1. Niesvizky R, et al. Blood. 2008;111:1101-9. 2. Garey KW et al. Chest. 2000;118:1826-7. 3. Fost DA, et al. J Allergy Immunol. 1999;103:1031-5.4. Spahn JD, et al. Ann Allergy Asthma Immunol. 2001;87:501-5.

Study Design
A single-center, phase 2 study of clarithromycin combined with Pomalidomide+Dexamethasone in RRMM
p.o., orally; b.i.d., twice a day; RRMM, relapsed, refractory MM.
1 2 8 9 15 16 21 22 28Day
Dex 40mg PO
Dex 40mg PO
Dex 40mg PO
Dex 40mg PO
Pomalidomide 4 mg PO
Clarithromycin 500mg PO BID

Key Patient Eligibility Criteria
Inclusion criteria Exclusion criteriaAge > 18 years Nonsecretory MM
Relapsed or progressive MM after at least 3 prior therapeutic treatments/regimens for MM
History of thromboembolic event within the past 6 months prior to enrollment
Must have been previously treated with lenalidomide
Unable to take prophylactic anticoagulation or antiplatelet therapy
Adequate bone marrow, liver, and renal function
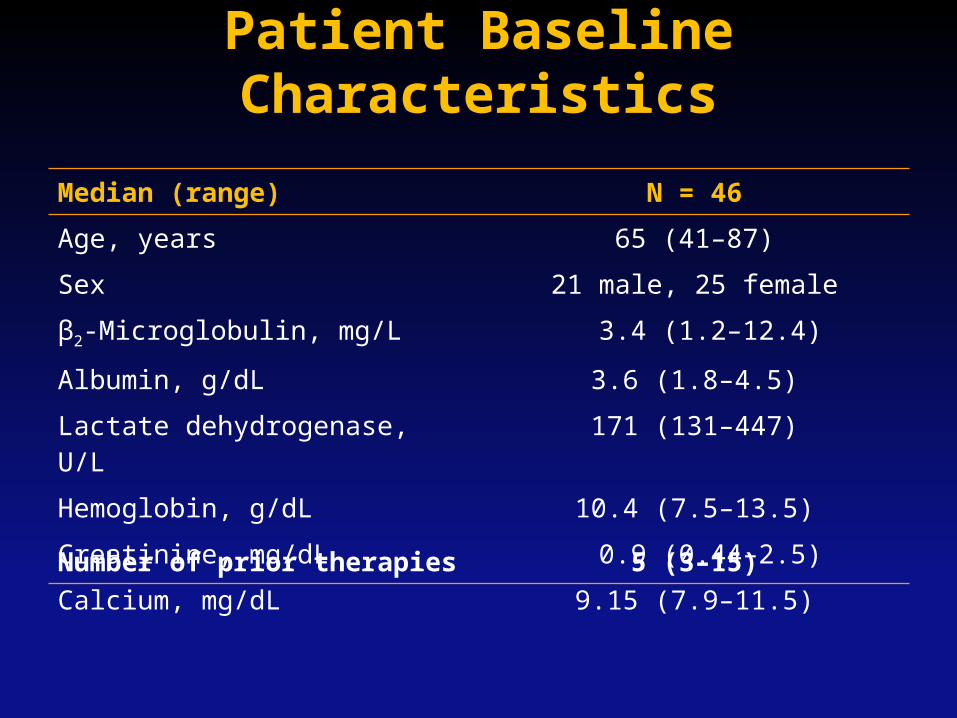
Patient Baseline Characteristics
Median (range) N = 46
Age, years 65 (41–87)
Sex 21 male, 25 female
β2-Microglobulin, mg/L 3.4 (1.2–12.4)
Albumin, g/dL 3.6 (1.8–4.5)
Lactate dehydrogenase, U/L 171 (131–447)
Hemoglobin, g/dL 10.4 (7.5–13.5)
Creatinine, mg/dL 0.9 (0.44–2.5)
Calcium, mg/dL 9.15 (7.9–11.5)
Number of prior therapies 5 (3–15)

Baseline MM Stage and Cytogenetic Abnormalities
n (%)
Durie-Salmon stage, N = 46
Ia 25 (54)
IIa 16 (35)
IIb 3 (7)
IIIa 2 (4)
International Staging System stage, N = 33
I 14 (42)
II 11 (33)
III 8 (24)
Cytogenetics*, N = 44
Standard risk 20 (45)
High risk 24 (55)
*Standard risk, n (%), defined by the presence of one or more of the following: t(11;14): 4(16); hyperdiploidy, 12(46); FISH del 13q14, 12(46); no abnormality: 5(19).High risk, n (%), defined by the presence of one or more of the following: del 17p: 5(19); karyotype del 13q: 3(12); amp 1q/ del 1p: 5(19);
t(14;20): 1 (6); t(14;16): 1(6); t(4;14): 1(6); or other complex cytogenetic abnormalities.

Prior Therapy History (N = 46)
Refractory: disease that is nonresponsive while on therapy, or progresses within 60 days of last therapy. Relapsed: previously treated myeloma that progresses and requires initiation of salvage therapy but does not meet the definition of refractory MM.ASCT, autologous stem cell transplantation.
33 patients (71%) were refractory to both lenalidomide and bortezomib.
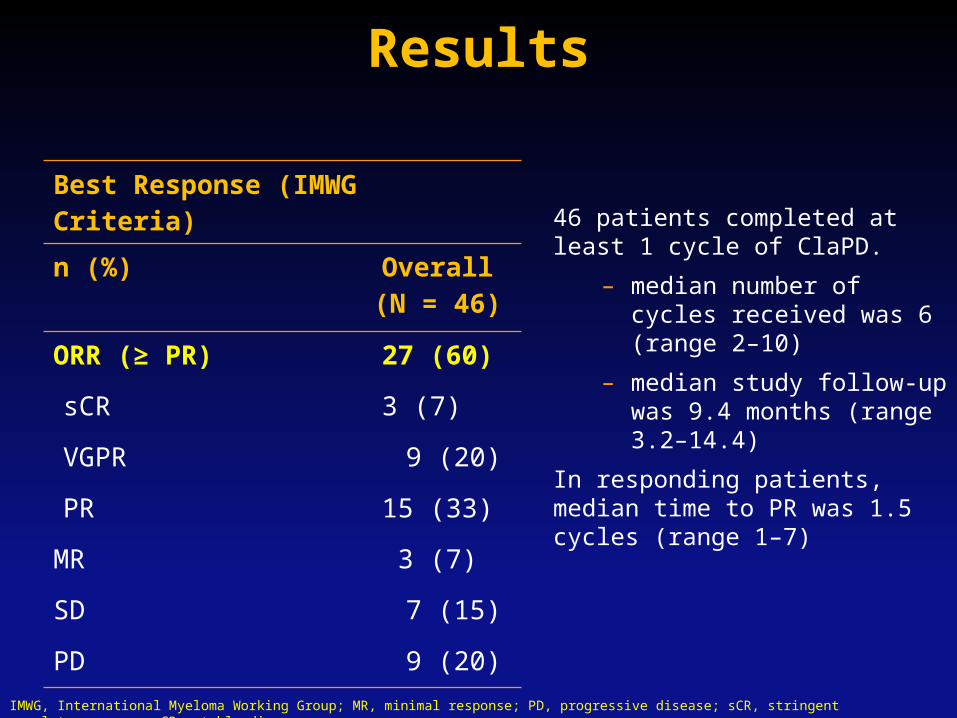
Results
46 patients completed at least 1 cycle of ClaPD.
– median number of cycles received was 6 (range 2–10)
– median study follow-up was 9.4 months (range 3.2–14.4)
In responding patients, median time to PR was 1.5 cycles (range 1–7)
Best Response (IMWG Criteria)
n (%) Overall(N = 46)
ORR (≥ PR) 27 (60)
sCR 3 (7)
VGPR 9 (20)
PR 15 (33)
MR 3 (7)
SD 7 (15)
PD 9 (20)
IMWG, International Myeloma Working Group; MR, minimal response; PD, progressive disease; sCR, stringent complete response; SD, stable disease.

Treatment History With Len/Bort Did Not Influence Response to ClaPD
37
Best Response (IMWG Criteria)
n (%) Overall(N = 46)
Lenalidomide refractory(N = 38)
Lenalidomide and bortezomib refractory
(N = 33)
ORR (≥ PR) 27 (60) 24 (63) 20 (61)
sCR 3 (7) 3 (8) 3 (9)
VGPR 9 (20) 7 (18) 5 (15)
PR 15 (33) 14 (37) 12 (36)
MR 3 (7) 2 (5) 2 (6)
SD 7 (15) 4 (11) 3 (9)
PD 9 (20) 8 (21) 8 (24)
IMWG, International Myeloma Working Group; MR, minimal response; PD, progressive disease; sCR, stringent complete response; SD, stable disease.
25
50
75
100
100 200 300
No
pro
gres
sion
(%
)Time (days)
00
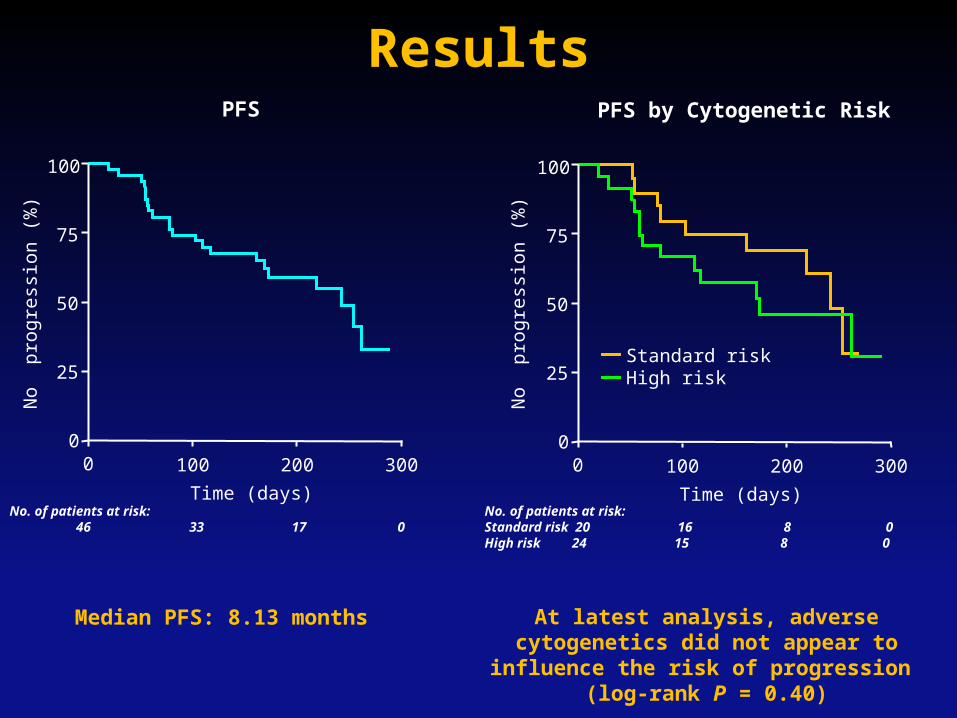
PFS by Cytogenetic Risk
Standard riskHigh risk
Results
Median PFS: 8.13 months At latest analysis, adverse cytogenetics did not appear to influence the risk of progression
(log-rank P = 0.40)
25
50
75
100
100 200 300
No
pro
gres
sion
(%
)
Time (days)
00
PFS
No. of patients at risk: 46 33 17 0
No. of patients at risk:Standard risk 20 16 8 0High risk 24 15 8 0
25
50
75
100
100 200 300
No
pro
gres
sion
(%
)
Time (days)
00
25
50
75
100
100 200 300
No
pro
gres
sion
(%
)Time (days)
00
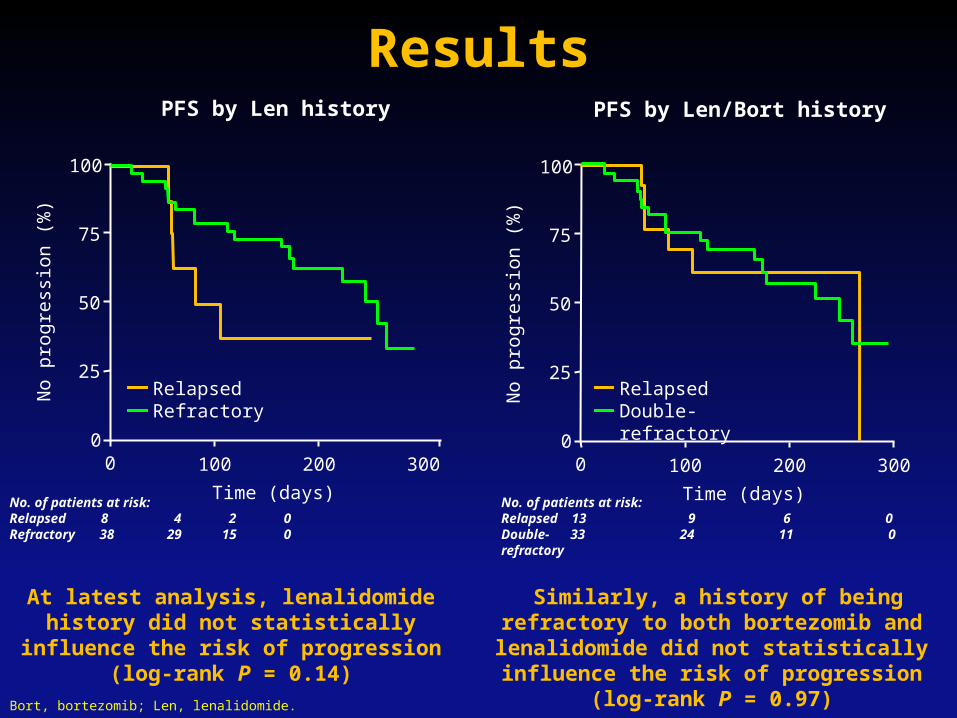
RelapsedDouble-refractory
PFS by Len history PFS by Len/Bort history
RelapsedRefractory
Results
At latest analysis, lenalidomide history did not statistically influence the risk of
progression (log-rank P = 0.14)
Similarly, a history of being refractory to both bortezomib and lenalidomide did not
statistically influence the risk of progression (log-rank P = 0.97)
Bort, bortezomib; Len, lenalidomide.
No. of patients at risk:Relapsed 8 4 2 0Refractory 38 29 15 0
No. of patients at risk:Relapsed 13 9 6 0Double- 33 24 11 0refractory
25
50
75
100
100 200 300
Sur
viva
l (%
)
Time (days)
00
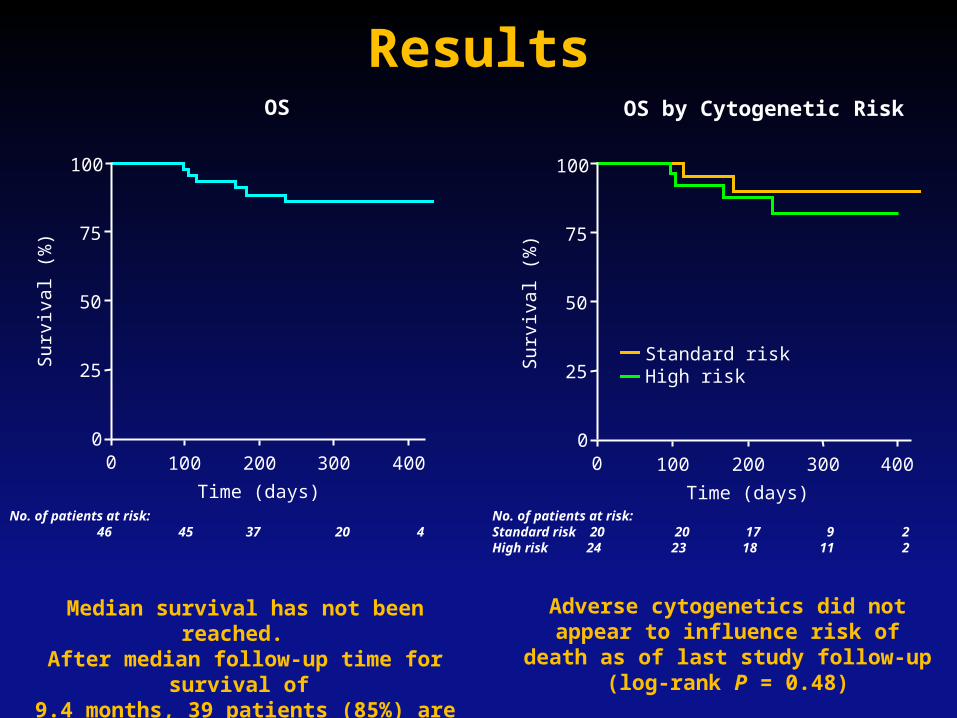
OS
25
50
75
100
100 200 300
Sur
viva
l (%
)
Time (days)
00
OS by Cytogenetic Risk
Standard riskHigh risk
Median survival has not been reached. After median follow-up time for survival of
9.4 months, 39 patients (85%) are alive
Adverse cytogenetics did not appear to influence risk of death as of last study
follow-up (log-rank P = 0.48)
Results
No. of patients at risk: 46 45 37 20 4
No. of patients at risk:Standard risk 20 20 17 9 2High risk 24 23 18 11 2
400400

Grade 3/4 Adverse EventsAdverse event, n (%) Grade 3* Grade 4
Anemia 6 (13) 2 (4)
Thrombocytopenia 6 (13) 8 (17)
Neutropenia 15 (32) 6 (13)
Febrile neutropenia 5 (11) 1 (2)
Lymphopenia 11 (24) 5 (11)
Hypoglycemia 5 (11) 4 (9)
*Occurring in ≥ 10% of patients.
Two patients withdrew from study, both due adverse events: – 1 due to grade 3 fatigue – 1 due to grade 4 muscular weakness
There was no treatment-related mortality

Conclusions
• ClaPD is a highly effective regimen for heavily treated relapsed or refractory MM patients.
• ClaPD demonstrates clinical activity in patients with advanced MM who have received multiple prior therapies, including many who are refractory to both lenalidomide and bortezomib.
• PFS in patients treated with ClaPD is sustained for > 6 months in the majority of patients.

Conclusions
• High-risk cytogenetics did not impact PFS or OS in patients treated with ClaPD.
• A history of being refractory to prior lenalidomide or double-refractory to lenalidomide and bortezomib did not influence PFS in patients treated with ClaPD.
• Discontinuation due to adverse events was low (2 patients).

Pomalidomide Summary
• Pomalidomide is:– 2nd generation IMiD– Has anti-proliferative, anti-angiogenic, and IMiD
properties– Primary toxicities are similar to lenaliomide:
• Myelosuppression• Venous thromboses
– Active as a single agent– Synergizes with dexamethasone– Active in MM that is lenalidomide-refractory– Active in MM that is double-refractory– Less active as number of prior lines of therapy increases
44
Thank you
45