Embed Size (px)
Citation preview

Update on chronic hepatitis B & C in Hong Kong
Dr Owen Tsang
Princess Margaret Hospital
8 May 2018
HA Convention

Complications of chronic hepatitis
Hepatitis B & C can lead to:• Chronic hepatitis• Cirrhosis• Hepatocellular carcinoma• Acute liver failure in
untreated cases

Global situation of hepatitis B & C
Hepatitis B Hepatitis C
WHO 2017 Global Hepatitis Report

WHO. GLOBAL HEALTH SECTOR STRATEGY ON VIRAL HEPATITIS. 2016–2021

• Goal 3.3: By 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases
2015

WHO response: For the first time, WHO sets goals on hepatitis
WHO. GLOBAL HEALTH SECTOR STRATEGY ON VIRAL HEPATITIS. 2016–2021

The gaps
WHO 2017 Global Hepatitis Report
3 doses
Birth dose

Three-dose hepatitis B vaccine coverage, by WHO region, 2000–2015
WHO 2017 Global Hepatitis Report

Situation of hepatitis in Hong Kong


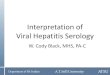
Causes of liver transplant in Hong Kong
Hepatitis B50%
Hepatitis C5%
Fulminant liver failure
14%
Biliary atresia10%
Others21%
Lo CM, et al. Hong Kong Med J 2002;8:240-4
N = 155

Hepatitis B


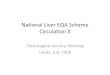
Age distribution of hepatitis B (from 1995 to 2016) (Data source: CHP, DH)
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
<1-14 1 4 2 4 3 2 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0
15-24 44 48 32 44 44 39 41 37 24 31 22 22 7 6 9 0 4 4 3 0 2 3
25-34 34 45 31 46 49 48 42 29 32 46 30 45 21 32 24 23 22 12 9 13 8 12
35-44 13 27 21 32 29 32 30 26 25 34 25 30 23 25 20 25 20 14 14 16 9 9
45-54 7 13 9 14 18 8 17 17 7 17 14 16 16 14 14 17 12 12 10 4 7 9
55-64 3 4 3 4 4 5 2 8 6 4 9 6 5 4 9 3 8 3 1 7 2 3
> 65 0 3 2 1 5 3 1 3 4 2 5 4 2 2 4 5 4 2 3 1 1 1
0
5
10
15
20
25
30
35
40
45
50
No
of
rep
ort
ed
cas
es

In general, the prevalence of hepatitis B is decreasing in all
cohorts

Population survey of hepatitis B in Hong Kong
2.6
7.4
10.9
8 8
7
8.7
0
2
4
6
8
10
12
<26 26-35 36-45 46-55 56-65 66-75 >75
Per
cen
tage
(%
)
Age groups
HBsAg +ve
Liu SH, et al. EASL 2017 Volume 66, Issue 1, Supplement, Page S682
• Blood samples collected from general population in HK from 2015-2017
• Tested for Hepatitis B & C• Total 10256 (M:F 33%:67%)• Mean age: 50.4 (M) vs 52.3 (F)• Overall HBsAg +ve 7.8%• Risk factor for HBsAg +ve:
• Family history of hepatitis • No history of vaccination• Born in Mainland China
If the overall prevalence is 7.8%, the total No of cases
would be 576,000

HB vaccination coverage in HK
SPP, CHP DH 2017. Surveillance of Viral Hepatitis in Hong Kong - 2016 Update Report

Long term protection of HB vaccination
• in 1983, 1112 neonates born to HB +ve Mother• Received 3 doses of HB vaccination• 1006 (92.6%) Developed Anti-HBsAb• 39 (3.5%) failed vaccination and developed chronic hepatitis B infection before age of 2• 30 years follow-up• Anti-HBsAb dropped to 37.4% • 97 (9%) Anti-HBc Seroconversion but none became HBsAg +ve• Anamnestic response possible
Lin AWC, Wong KH. J Hepatol 2013:59:1363-4.

Antiviral treatment for Hepatitis B in Hong Kong
Lamivudine
Adefovir dipivoxil
PegInterferon
Telbivudine
Tenofovir disoproxil fumarate
1998 2002 2005 2006 2008
Entecavir
Tenofovir alafenamide
2018
Essentially a life-long treatment!

Indications for sponsored treatment under the Hospital Authority
• ALT > 2x ULN & HBV DNA > 2000 IU/mL
• Cirrhosis & detectable HBV DNA
• Decompensated liver disease
• Hepatitis B reactivation during chemotherapy
• Transplant patient with hepatitis B infection
• Pre-emptive treatment for patient on anticancer chemotherapy or immunosuppressive therapy with moderate to high risk of hepatitis B reactivation
• Resistance to prior nucleoside analogues treatment (For Tenofovir only)
Hong Kong Hospital Authority Drug Formulary
GuidelineUS1
2018Europe2
2017Asia-pacific3
2016
HBeAg +veALT 1-2x ULNHBV DNA >
20,000 IU/mL
ALT > ULNHBV DNA >
2,000 IU/mL
ALT 1-2xULNHBV DNA >
20,000 IU/mL
HBeAg -veALT 1-2xULNHBV DNA >
2,000 IU/mL
ALT > ULNHBV DNA >
2,000 IU/mL
ALT 1-2xULNHBV DNA >
2,000 IU/mL
1. Terrault N, et al. Hepatology 2018;67:1560-992. EASL. J Hepatol 2017;67:370-963. Sarin S, et al. Hepatol Int 2016;10-1-96

Treatment of hepatitis B under Hospital Authority
Scenario Data
Estimated total number of patients 2007 - 2016 154,905
Percentage of cases under HA (Assume prevalence 7.8%) 154,905 / 576,000 = 27%
Receiving antivirals in HA 35,550
Eligible but not yet given treatment(ALT > 80 & HBV DNA > 2000 IU / ml)
14,342
Percentage of hepatitis B patients on treatment 35,550 / 154,905 = 22.95%
Percentage of eligible patients on treatment35,550 /(35,550 + 14,342)
= 71.25%
HA data: Courtesy of Dr Lao WC of PYNEH

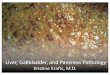
Impact of treatment for hepatitis B in cirrhotic patients
Hepatic events HCC
Liver related mortality All-causes mortality
Wong GL, et al. Hepatology2013; 58: 1537–47.
• Hong Kong study• 1,446 entecavir-treated
patients for at least 12m• 424 treatment-naïve patients

Hepatitis C

Population survey of hepatitis C in HK from 2015-2017• Total 10256 people• 48 out of 10,256 people HCV Ab +ve = 0.47%• Risk factors for HCv Ab +ve:
• History of blood transfusion• Intravenous drug use
Liu SH, et al. EASL 2017 Volume 66, Issue 1, Supplement, Page S682
If the overall prevalence is 0.47%, the total No of cases
in HK would be 34,780

Most are young and healthy adults
Prevalence is low in blood donors

Prevalence is higher in at risk cohorts

Old standard treatment
+
Ribavirin Pegylated interferon (weekly Injections)
Or
Duration of treatment 24 – 48 weeks

New hepatitis C drug: Direct Acting Antivirals (DAA)
No injection
Lower pill burden
Shorter duration
XMinimal side effects
Pan-genotypic

Milestones for treatment of genotype 1
Carter W, et al. J Clin Pharmacol 2017;57(3): 287
Medications available in Hospital Authority:• Pegylated interferon (PEG-IFN) + Ribavirin (RBV)• Sofosbuvir (SOF)• Ledipasvir/Sofosbuvir (LDV/SOF)• Sofosbuvir/Velpatasvir (SOF/VEL)• Viekira Pak (Ombitasvir/Parietaprevir/Dasabuvir)• Daclatasvir/Asunaprevir (DCV/ASP)• Boceprevir
Coming within this year:• Elbasvir/Grazoprevir (ELB/GRZ)• Glecaprevir/Pibrentasvir
Sust
ain
vir
olo
gic
resp
on
se (
SVR
) %
$
$$
$$$

Indications for sponsored DAA under the Hospital Authority
• Advance fibrosis (F3/4) + failure or intolerant to PEG-IFN/RBV
• Treatment naïve Genotype 1b patients with advance fibrosis (F3/4): for Daclatasvir + Asunaprevir
• Post-solid organs or bone marrow transplantation
• Renal dialysis patients on transplant waiting list
Hong Kong Hospital Authority Drug Formulary
1. US & European guidelines have already discouraged PEG-IFN/RBV as treatment options2. Asia-pacific guideline: in areas with limited resources or DAA not available, PEG-IFN/RBV may be considered

Territory-wide study on the clinical characteristics and treatment uptake of patients with chronic hepatitis C in public hospitals in Hong Kong
• Retrospective analysis of 15 participating hospitals in Hong Kong.• From January 2005 to March 2017, patients who were tested positive for anti-HCV were identified.• 30.6% (n=3,456) passed away at the time of review• Annual all-cause mortality rate of 2.5%, and 26.0% of deaths were liver-related• Treatment given in 2201 patients = 19.4%, estimated untreated alive patient = 5224
Patient demographics N = 11,309
Median age, years (IQR) 59 (47-67)
Male 69%
Ethnicity
Chinese 91.4%
Pakistan 1.1%
Vietnamese 0.8%
Nepalese 0.5%
Indian 0.4%
Diabetes mellitus 23.6%
HBV co-infection 7.8%
Severe renal impairment (eGFR<30 mL/min/1.73 m2) 7.1%
HIV co-infection 1.4%
Hemophilia 0.8%
Cooley’s anemia and Hemoglobin H disease 0.8%
Organ transplantation, n (kidney, liver , heart) 118, 103, 1
Courtesy of Dr Hui YT from QEH. Hui YT, et al. Asia Pacific Digestive Week 2017 Abstract No: APDW2017-ONL0113
About 1/3 of all cases in HK

Genotype and treatment uptake
Genotype distribution (n=2,397) Treatment received by patients (n=2,201)
Courtesy of Dr Hui YT from QEH. Hui YT, et al. Asia Pacific Digestive Week 2017 Abstract No: APDW2017-ONL0113

HCV patients given Pegylated Interferon + Ribavirin in HK
231 had completed PR
Courtesy of Dr Hui YT from QEH. Hui YT, et al. 2017 Manuscript submitted to Liver International.
Sub-groups NOverall treatment
uptake (%)
Thalassemia major 11 85.7
Hemophilia 36 50.0
Compensated cirrhosis 271 49.4
HIV co-infection 92 38.0
HCC 124 33.1
PWID 141 27.4
Renal dialysis 29 17.2
Decompensated cirrhosis 120 16.7
Age (years) < 60 965 38.3
60 - 69 360 37.2
70 - 79 149 18.1
≥ 80 59 6.8

HCV patients given Pegylated Interferon + Ribavirin in HK
Courtesy of Dr Hui YT from QEH. Hui YT, et al. 2017 Manuscript submitted to Liver International.

HCV patients given Direct Acting Antiviral (DAA) in HK
Hui YT, et al. Asia Pacific Association for the Study of Liver 2018 Poster Board Allocation Number: 199; Poster ID: HCV-90; Abstract Track ID: CC-01-019
• Sofosbuvir/PR: SVR 100% (N = 4)• Sofosbuvir/Ribavirin: SVR 92.9% (N = 14)
• Overall SVR 97.3%

CUHK & CEVHAP Surveyed of 13 territories in Asia including HK in 2016Goals: • determine the policy climate in these countries
towards implementing plans to prevent and control chronic viral hepatitis
• Identify infrastructural gaps and provide a benchmark for progress in the coming years.
Meyers T, et al. Viral Hepatitis Policy in Asia 2016. The Coalition to Eradicate Viral Hepatitis in Asia Pacific; 2017.



Other Challenges
HCV transmission among HIV Gay men
HCV transmissions within the hospital
2016
2018
2016
Worry on HBV transmission among patients on dialysis
2016
HAV transmission among Gay men
2017

Looking Forward
• The Policy Address of CE of the SAR has determined to focus on prevention, screening and identification for chronic diseases
• Government has been trying to coordinate experts on developing strategies to achieve the goals set out by the WHO
• Some local NGOs have also been trying to look into the issue of hepatitis
• The most easily achievable goal would be on management of chronic hepatitis C.

Summary of hepatitis B/C status in HK
• Prevalence of HBV is still high in HK, though it is gradually decreasing
• HBV is still associated with significant complications
• Uptake rate of universal hepatitis B vaccination is optimal in HK
• Prevalence of HCV is low in HK, but can be significant in high risk groups
• Management of HBV & HCV is still considered suboptimal in HK
• More effort may be needed to bride the gaps on diagnosis, treatment and prevention
• Challenges on eradication of hepatitis in HK still exit but can be overcome.

Thank you

Enablers for eradication
Hepatitis EradicationPreven
tion
Testing
Treatmen
t
Funding