● Ear, Nose and Throat ● Traumas ● Foreign Bodies ● Infections
Oropharyngeal Lacerations
● Fall with object in mouth ● Injury Central Lateral
Presenter
Presentation Notes
Children may suffer from oropharyngeal lacerations or puncture wounds when they fall with an object such as a stick or pencil in their mouth.
Central Oropharyngeal Lacerations
● Vascular and neural injury unlikely ● Confirm absence of retained foreign body ● Discharge home
Presenter
Presentation Notes
If the injury is restricted to the central portion of the palalte, damaged to vascular or neural structures of the head and neck is unlikely. These children are usually safe to discharge home after confirmation of no retained foreign body.
Lateral Oropharyngeal Lacerations
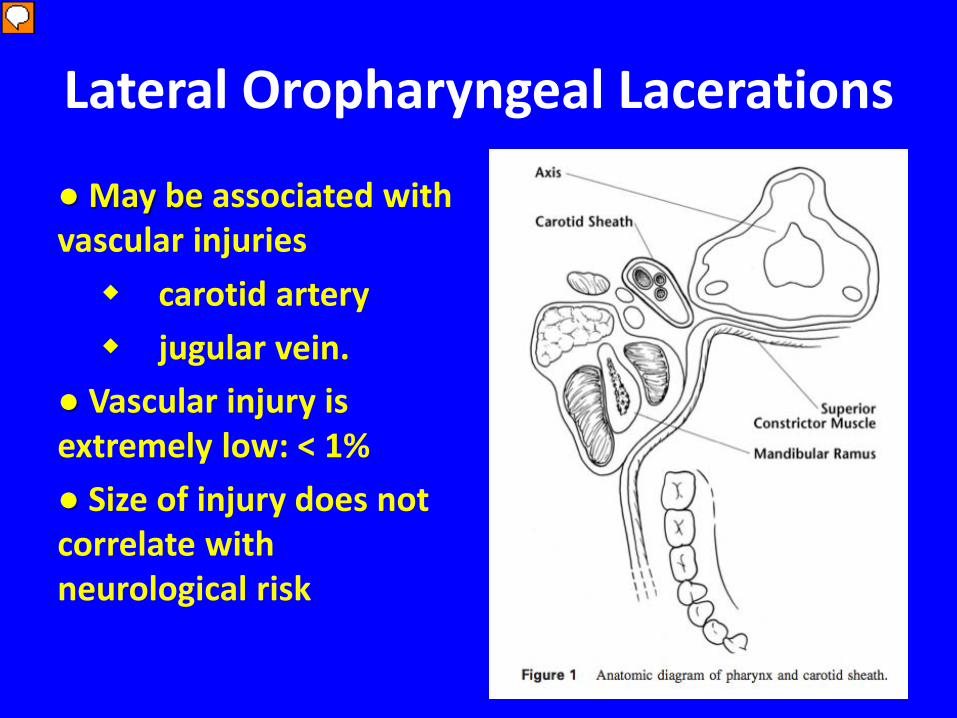
● May be associated with vascular injuries carotid artery jugular vein. ● Vascular injury is extremely low: < 1% ● Size of injury does not correlate with neurological risk
Presenter
Presentation Notes
Lateral oropharyngeal lacerations maybe associated with vascular injury. These injuries in children are quite common however there have been only 32 reported cases of lacerations resulting in thrombosis and and neurological complication. This implies the risk of vascular injury is extremely low < 1%. The size of the injury does not correlate with ineurological risk.
Diagnostic Studies
● Angiography ● MRA ● Carotid duplex
Presenter
Presentation Notes
Laceration Repair
● Most heal well with no repair ● Repair if Excessive bleeding Soft tissue flap Altered oral anatomy Explore for foreign body
Disposition
● Antibiotics if injury large enough to be sutured ● Anticoagulation if thrombosis ● Observation for 48 to 60 hours. ● Minimal risk discharged home with instructions similar to head trauma. ● Follow-up according to laceration care
Presenter
Presentation Notes
They found that a trend existed for benefits with laceration requiring repair felt that antibiotics maybe useful when the wounds are large enough to be sutured. . anticoag-ulation i should be considered in most cases of thrombosis, with or without neurologic change but would discuss with your NS before giving Hospitalization has been suggested by if there is a high concern for vascular injury. There is no agreed upon time frame, most are suggest a period of 48-60hrs. If the families reliable and there is a low risk for vascualr injury provider can discharge the patient home with instructions similar to those with head trauma.
Tongue Lacerations
Tongue Lacerations
● Occur after falls, traumas, or seizures ● Proper Management Preserve tongue function Facilitates swallowing Articulating speech ● Repair or not to repair
Presenter
Presentation Notes
Management of these injuries is complicated by different recs in the OMFS literature and lack of consensus of which lacerations should be repaired.
No Need To Repair
● Most in children ● Simple lacerations ● Linear lacerations ● On dorsum
Which To Repair
In the ED ● Bisecting wounds ● Large flaps ● Bleeding ● Larger than 1cm ● Gaping ● U--shaped
OMFS or ENT ● Partial amputations ● Complete amputations
Assessment in the ED
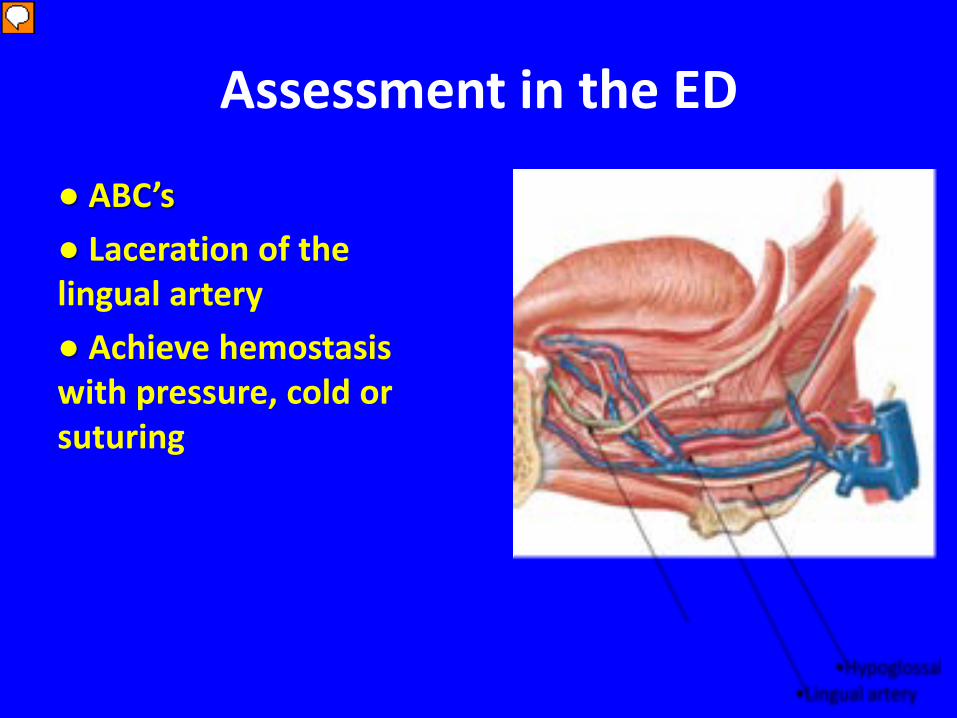
● ABC’s ● Laceration of the lingual artery ● Achieve hemostasis with pressure, cold or suturing
Presenter
Presentation Notes
Can have airway compromise with excessive bleeding due to laceration of the lingual artery. You can achieve hemostasis with pressure, Kohl’s or suturing the lacerated artery.
Anesthesia
● 1% Lidocaine soaked gauze for small lacerations ● Local infiltration of lidocaine with epinephrine ● Inferior alveolar or lingual nerve block ● Conscious sedation
Presenter
Presentation Notes
Can place a 1% lidocaine soaked gauze over the tongue for 5-10mins. For larger or more complicated lacerations, an inferior alveolar nerve block or a lingual nerve block can be more effective.
Keep the tongue in protrusion, by manually held with gauze, grasp with towel clamps, or help with a large suture passed through the tongue
Discharge
● Soft diet for 2-3 days ● Swish and spit with antiseptic mouth wash ● Antibiotics are not necessary
Presenter
Presentation Notes
With adequate irrigation the rate of wound infections is small
NASAL TRAUMA
Nasal Trauma
● Most are minor ● Associated injuries Cervical spine, CNS Eye Chest
Presenter
Presentation Notes
Caused by sports, playing with friends like myself broke mine wrestling and, trauma. Even though most nasal fracture in children are minor they should assessed for associated injury to the
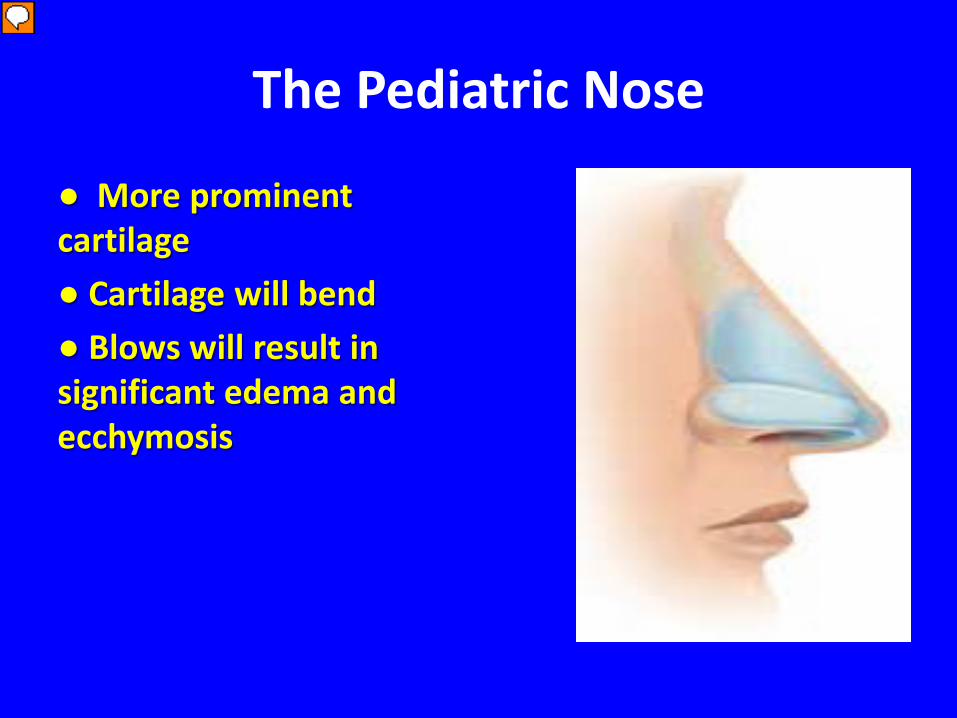
The Pediatric Nose
● More prominent cartilage ● Cartilage will bend ● Blows will result in significant edema and ecchymosis
Presenter
Presentation Notes
And children the nose architecture is different from out of adults it’s more prominent soft cartilaginous position. The cartilage open easily allowing the force of the blows dissipates across midface and may result in significant edema and ecchymosis
Nasal Fracture
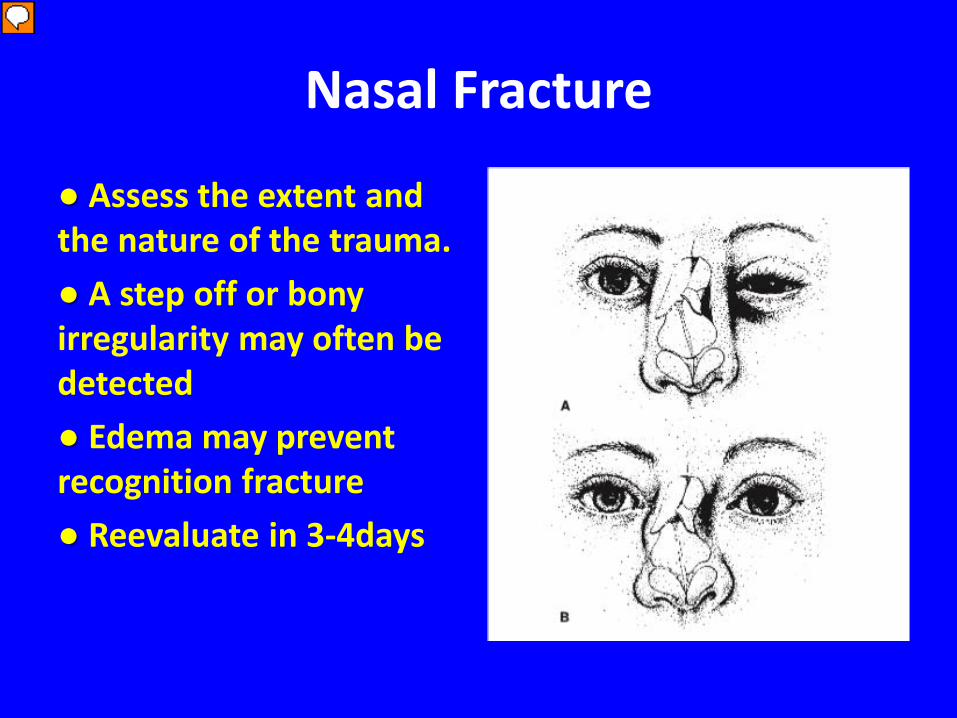
● Assess the extent and the nature of the trauma. ● A step off or bony irregularity may often be detected ● Edema may prevent recognition fracture ● Reevaluate in 3-4days
Presenter
Presentation Notes
The direct blow to the nose can fracturing is a skeleton with result in deviation or depression of the nasal bones in septum. These deformities may be apparent during the initial clinical examination. Be wary post injury edema may prevent it’s recognition for several days until the swelling has subsided. X-rays of the nose have been found to be unreliable and are not recommended for simple nasal fractures. Epistaxis commonly accompanies nasal fractures,
Nasal Trauma
● X-rays are unreliable ● Epistaxis ● Reduced by the ENT ● Must be done with in 7-10 days after injury
Presenter
Presentation Notes
With nasal trauma you must first inspect the externt of the trauma to the skin, skeleton and nasal septum. Reevalaute in 3-4days when the swelling subsides to look for deformity or depression. If reduction is necessary ENT will reduce once is swelling subsides. After 7-10 days post injury nose starts to heal making reduction more difficult.
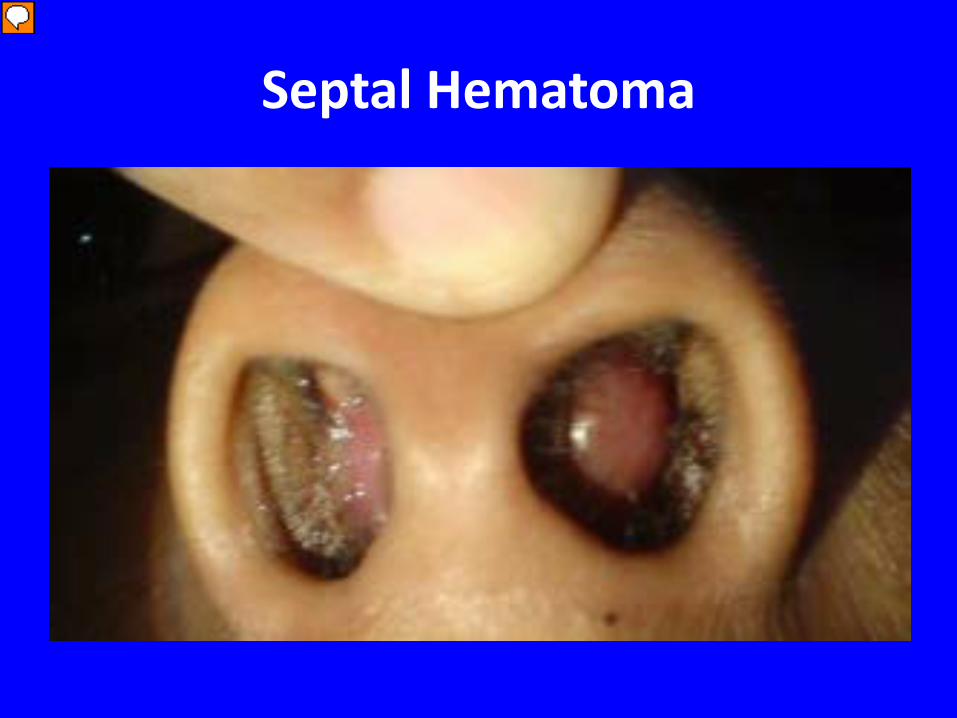
Is a bulging of the nasal septum into one or both sides of the nasal caity. It is caused by disruption of the septal perichondrium from the cartilage when it is deformed by trauma. Blood accumulates between the septal cartilage and its overlying mucoperochondrium resulting in decreased blood supply to the perichondrium.
Septal Hematoma
● Not improved with topical nasal decongestants
● DRAINED RIGHT AWAY ● Septal abscess ● Cartilage destruction Saddle Nose
Presenter
Presentation Notes
The hematoma should be drained as soon as possible mucoperichondrium packed back against the perichondrium to restore blood supply. The septal hematoma will not constrict with topical nasal decongestants. Must be drained right away. If missed can result in a septal abscess which can result in cartilage destruction resulting in a saddle nose deformity
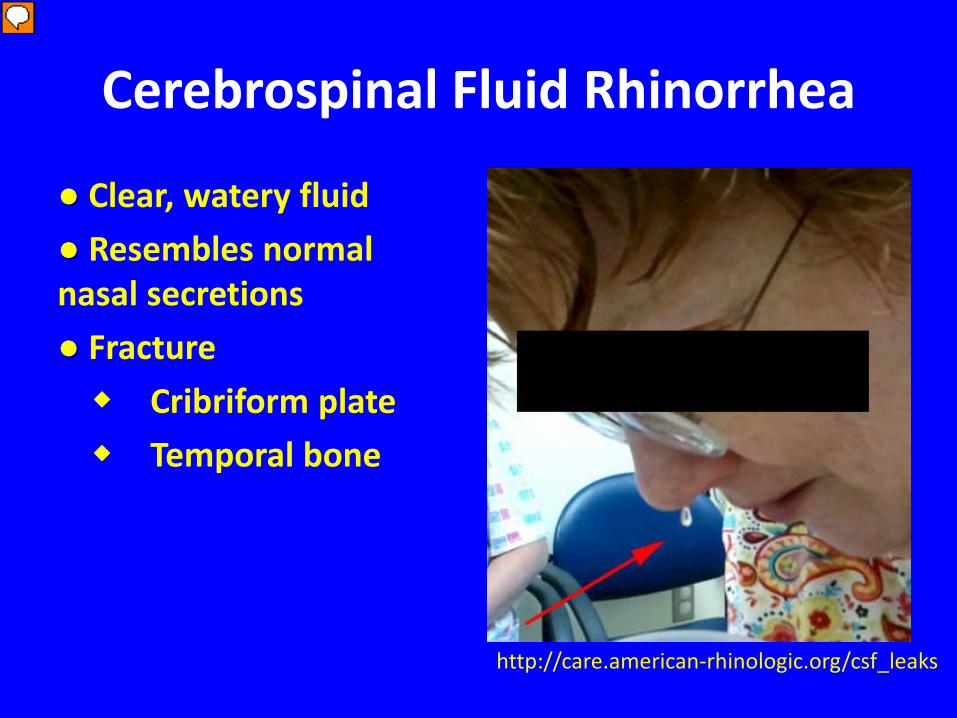
Cerebrospinal Fluid Rhinorrhea
● Clear, watery fluid ● Resembles normal nasal secretions ● Fracture Cribriform plate Temporal bone
http://care.american-rhinologic.org/csf_leaks
Presenter
Presentation Notes
If a temporal fracture it enters the nasopharynx through the eustacian tube.
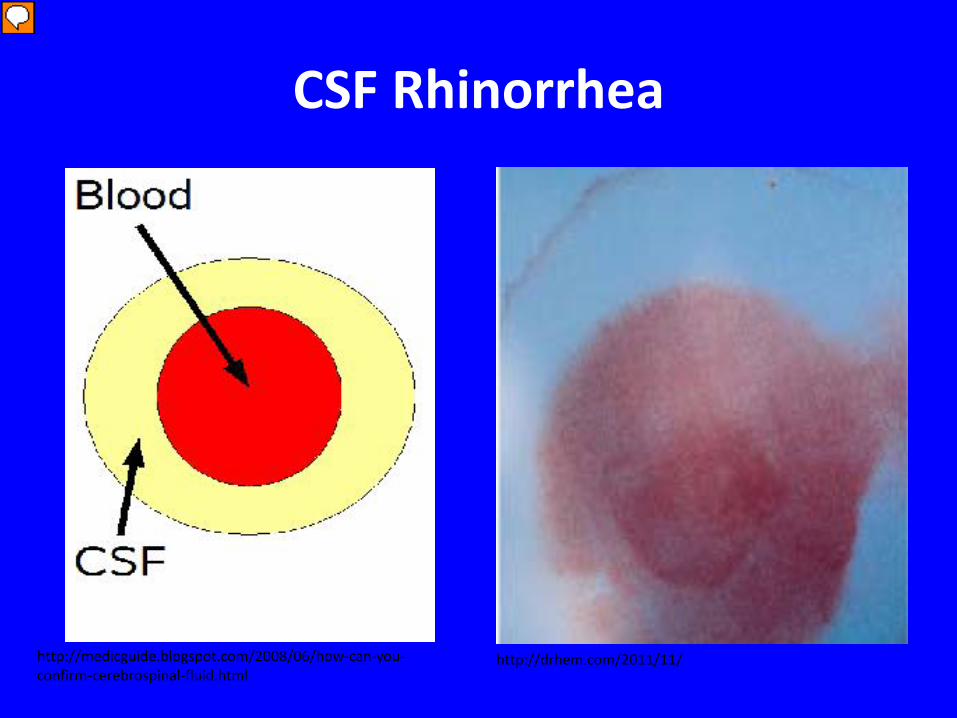
If concern about CSF rhinorrhea. If the person leans forward allowing the nasal drainage dripped onto a piece of paper. CSF will form a characteristic target pattern with the bloodstain in the center the drop and a clear halo of CSF around it.
CSF Rhinorrhea
● Target sign on paper. ● Glucose oxidase test strip ● β-2 transferrin
Presenter
Presentation Notes
CSF is high in glucose which can be detected on a glucose oxidase test strip which is used in urinalysis. Nasal and lacrimal secretions can give a false positive. A definitive test is finding of beta 2 transferrin which is only found in CSF
CSF Rhinorrhea
● CT scan ● ENT and Neurosurgery consult ● Admit, bed rest and head of bed at 30 degrees ● Often heal with rest and conservative management. ● Antibiotics Controversial
Presenter
Presentation Notes
CT scan to look for fracture. Admit, bed rest and head of bed at 30 degrees to attempt to decrease and seal the leak. Often heal within 7-10 days rest and conservative management. Prevent any action that would increase ICP ie cough, sneeze, nose blowing and heavy lifting. Antibiotics are controversial and in studies have shown no stastically significant evidence that antibiotics reduced ascending meningitis in nonsurgical traumatic leaks.
Epistaxis
● Rich vascular supply ● Usually mild and self limited ● Causes nose picking and URI
Presenter
Presentation Notes
The news of the rich vascular supply making vulnerable to episodes of bleeding. Most of the bleeding is mild and self-limited. Most common causes in children is nose picking and upper respiratpry infx less common causes are Facial trauma, foreign bodies, cocaine or heroin sniffing, or sinusitis. Systemic causes such as hepatic disease, leukemia, idiopathic thrombocytopenia, and other coagulopathies.
Epistaxis
Anterior ● 90% of episodes ● Arises from Kiesselsbachs Plexus ● Characterized by a slow, persistent ooze
Posterior ● 10% of episodes. ● Sphenopalatine artery ● Characterized by heavy bleeding ● High-risk of airway compromise, aspirations of blood, and life-threatening hemorrhage.
Presenter
Presentation Notes
Epistaxis is classified according to location of the bleeding in the nasal cavity. Anterior bleeds result in approximately 90% of nose bleed and usually involves Kiesselbach plexus on the anterior nasal septum Posterior bleeds usually originate from the sphenopalatine artery in the posterior nasal cavity and tend to bleed more profusely. This type of bleeding carries a higher risk of airway compromise, aspiration of blood, and life-threatening hemorrhage.
Mild epistaxis without active bleeding
● No work-up is needed ● Minimize recurrence Minimize local trauma Hydration via saline mist Increasing humidity via coolmist humidifier
Presenter
Presentation Notes
No lab work that is needed unless patient lost a lot of blood. Minimize local trauma such as no nose blowing or picking Increase humidity with coolmist vaporizer to reduce because of irritation
Minor Bleeding
● Pinch nostrils for 5-30mins nonstop ● Elevate head but do not hyperextend ● Gauze soaked in Nasal decongestant Epinephrine 1:10,000 Phenylephrine
Presenter
Presentation Notes
Minor bleeding occurs the patient maybe instructed to pinched the nostrils together for 5-30 minutes nonstop (with out peaking). Bleeding is usually controlled and 5 to 10 minutes. Also peace of Gauze soaked in nasal decongestant spray, epinephrine or phenylephrine and placed an effective nostril may help induce localized vasoconstriction. If the bleeding cannot be controlled the patient should be transferred to the nearest emergency department.
In the emergency department ABCs and hemodynamic stability should be assessed. Good nasal exam. If an anterior source of bleeding is identified and the bleeding is active, cautery may be, using either silver nitrate sticks for thermal cautery. The patient is still bleeding besides cautery may need to place nasal packing in the affected nostril. Can use Vaseline or commercial packing that expands when it becomes wet to tamponade the bleeding vessel. f the answer bleeding is unresponsive to cautery may require an answer nasal packing with petroleum jelly got strips or commercial packing it expands when it becomes wet to Tampa not depleting Bethel. Packing should be preceded by the application of localṈ籙
Posterior Bleeding
● Hemoptysis, hematemesis, or blood in the posterior pharynx ● ENT consult ● Nasal packing or epistaxis balloons ● Admission to monitor for hypoxia, or respiratory compromise
http://www.invotec.net/epistaxis_balloons.html
Presenter
Presentation Notes
You could see Hemoptysis, hematemesis, blood in the posterior pharynx. These pt will need an ENT consult. Posterior bleeds often require nasal packing or epistxis. These pt should be admitted and monitored overnight for hypoxia or respiratory compromise.
Nasal Packing
● Antibiotics ● Removed in 3 to 5 days ● Decrease the incidence Toxic shock syndrome Sinusitis
Presenter
Presentation Notes
Antibx with staph and strep coverage. Decrease the incidence of sinusitis are toxic shock syndrome that can be seen with a non-absorbable nasal packing.
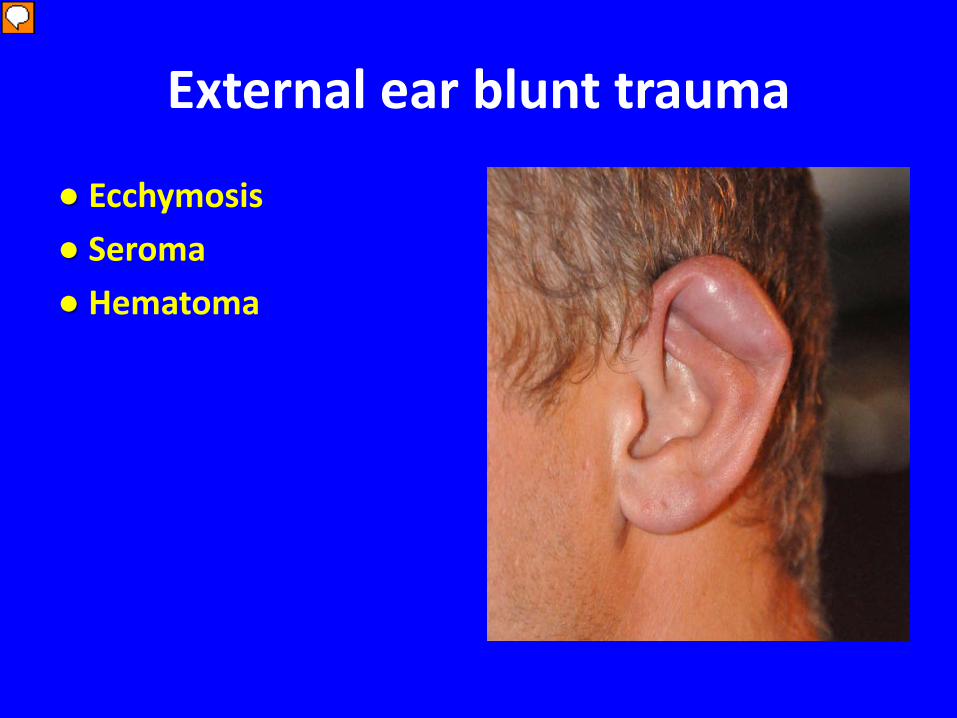
External blunt trauma is often the result of athletic injury, fall or direct blow to the ear. Can result in ecchymosis or disruption in the perichondrial blood supply resulting in a hematoma or seroma.
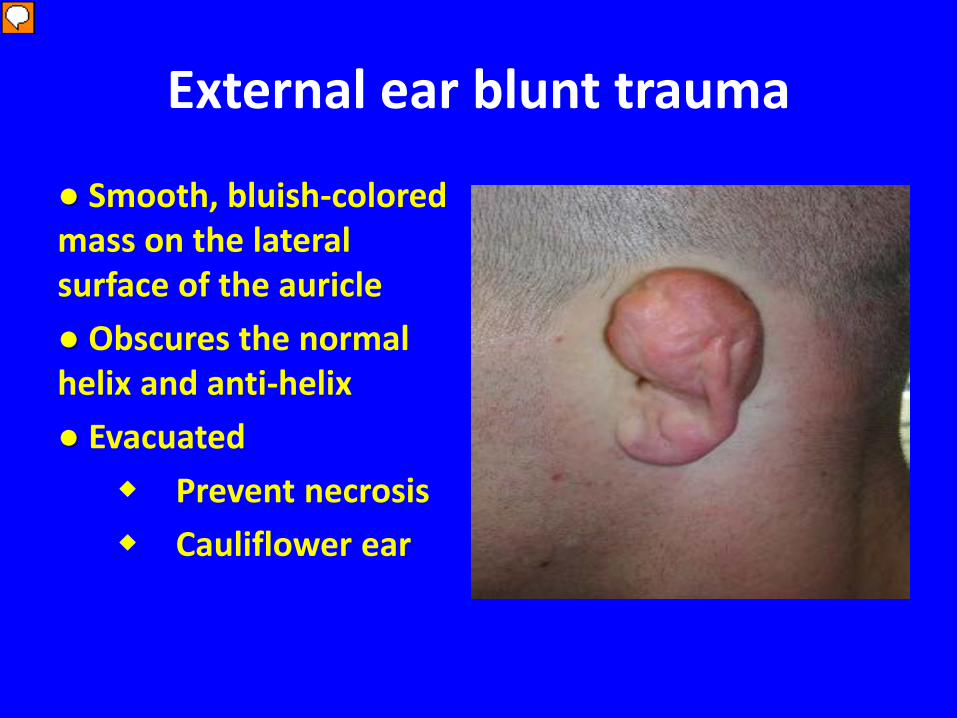
External ear blunt trauma
● Smooth, bluish-colored mass on the lateral surface of the auricle ● Obscures the normal helix and anti-helix ● Evacuated Prevent necrosis Cauliflower ear
Presenter
Presentation Notes
Form a smooth, bluish-colored mass on the lateral surface of the auricle which obscures the normal contour of the helix and antihelix. Must be evacuated expeditiously to prevent necrosis or potentially cauliflower ear.
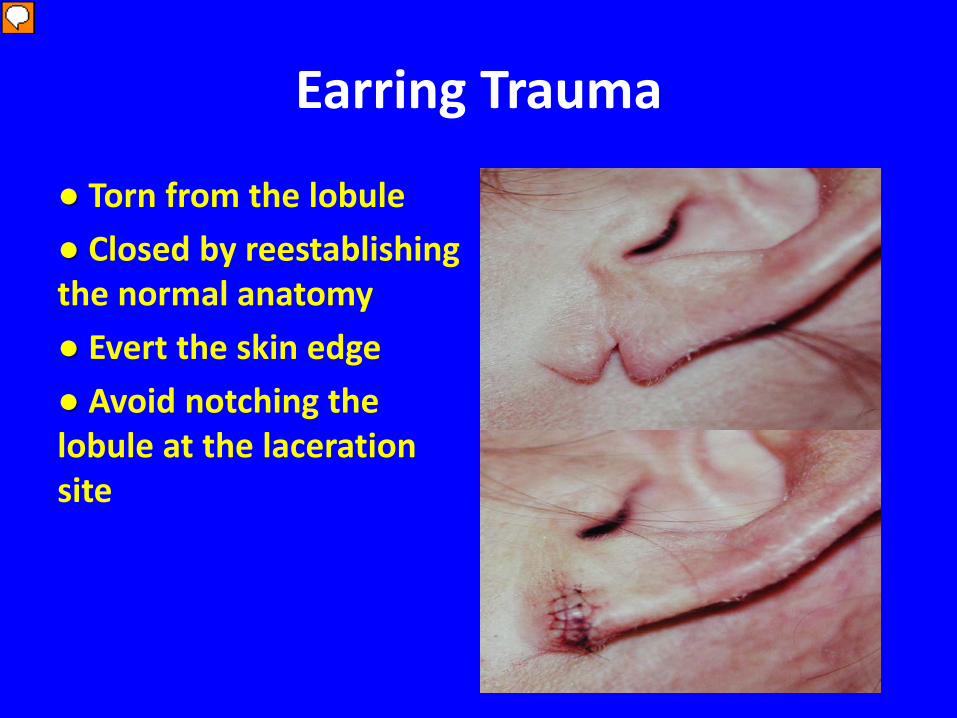
Earring Trauma
● Torn from the lobule ● Closed by reestablishing the normal anatomy ● Evert the skin edge ● Avoid notching the lobule at the laceration site
Presenter
Presentation Notes
Earrings can be torn from the pinna. These lacerations should be closed similar to skin lacerations with the edge everted. Reestablish nl anatomy, Care should be made to avoid notiching of the lobule at the laceration site.
Ear and Nose Foreign Body
Foreign Bodies
● Common in children ● Beads, food, rocks, toys, paper, batteries and insects ● Present Immediately After foul odor Recurrent epistaxis Pain in the ear or nose Accidently
Removal
● Restrained adequately ● Good light source, ● Nasal speculum
Removal
● Manually grasp the object with forceps ● Getting behind the object with curette ● Applying suction to the surface of the foreign body ● Katz extractor ● Mouth-Mouth positive pressure
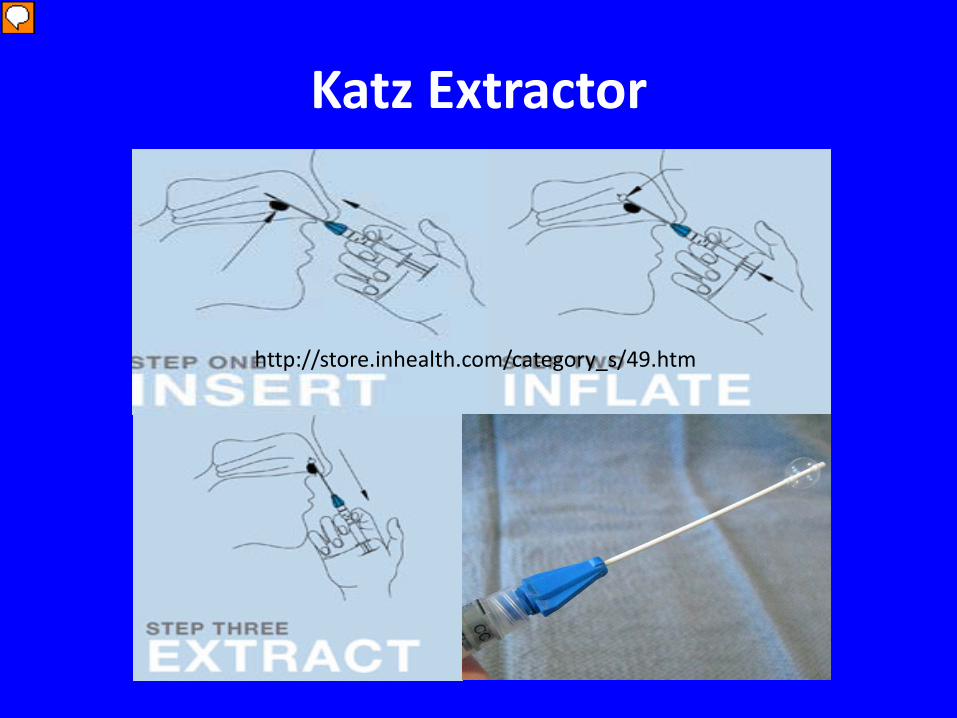
Katz Extractor
http://store.inhealth.com/category_s/49.htm
Presenter
Presentation Notes
Helps you to easily removed foreign body. You insert the Katz extractor passed the foreign body. Inflate the balloon. Retract the catheter and the foreign body comes with it. Can easily be done in the office setting.
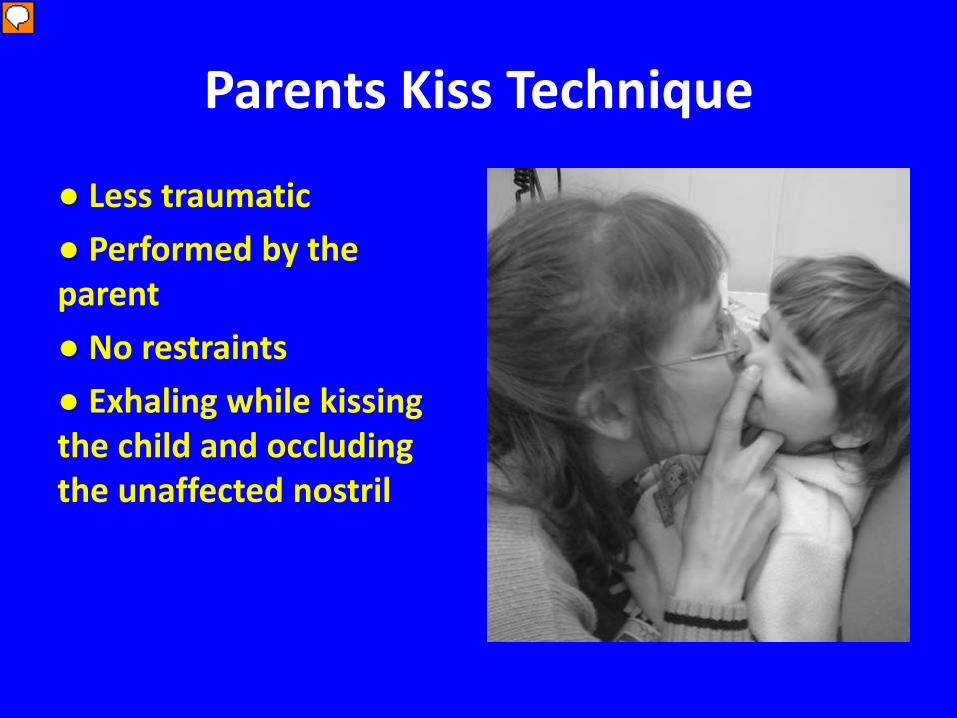
Parents Kiss Technique
● Less traumatic ● Performed by the parent ● No restraints ● Exhaling while kissing the child and occluding the unaffected nostril
Presenter
Presentation Notes
Studies have shiown that this is a quick and effective way to remove foreign bodies. Less dramatic for children. Involves the parents exhaling while kissing their child and occluding the affect nostril. Glottis is closed and little risk of barotrauma.
Unable to Remove
● Consult ENT if unable to remove. ● Consider antibiotics
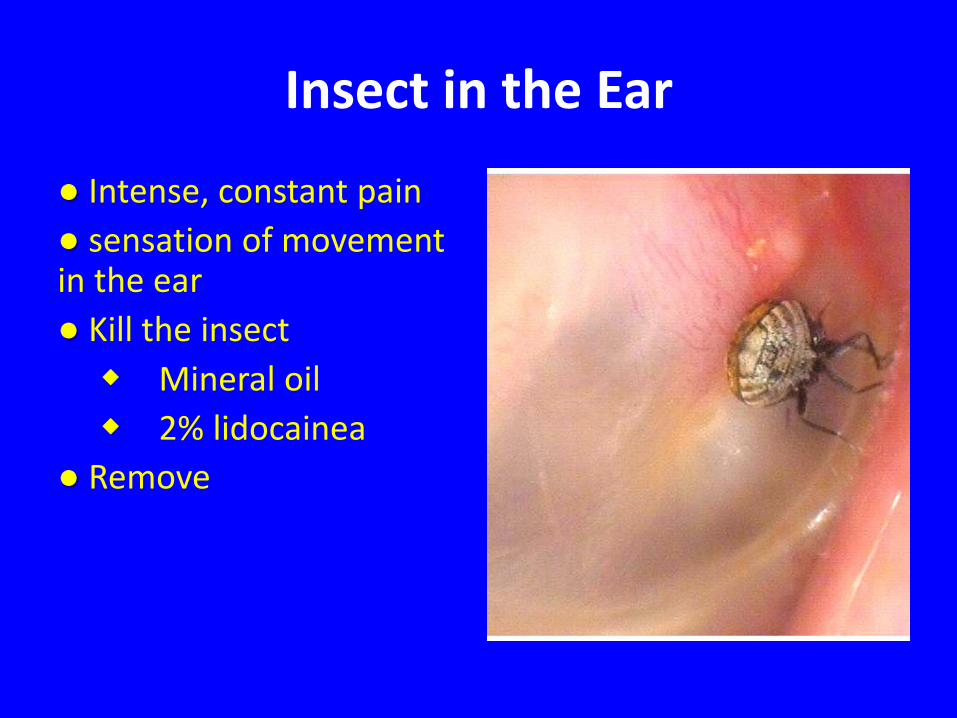
Insect in the Ear
● Intense, constant pain ● sensation of movement in the ear ● Kill the insect Mineral oil 2% lidocainea ● Remove
Button battery in the Ear
● Release small amounts of chemicals and voltage ● Alkaline chemical burns, necrosis, or septal-tympanic perforation ● Removed immediately
Foreign Body Aspiration
• 80% of pediatric FB in airways occur in children < 3yo – Peak incidence between 1 and 2 years old
Presenter
Presentation Notes
most children are able to stand, are apt to explore their world via the oral route, and have the fine motor skills to put a small object into their mouths, but they do not yet have molars to chew food adequately. Additional predisposing factors to FBA in this age group include access to improper foods or small objects, activity while eating, and older siblings (who may place food or objects into the mouths of infants or toddlers). Young children are also particularly vulnerable to FBA because of the smaller diameter of their airway, which is prone to obstruction The absence of the molars makes them unable to chew adequately, however. These factors increase the risk of foreign-body aspiration.
Commonly Aspirated Objects
• Nuts – Peanuts (36%-55%)
• Popcorn • Watermelon seeds • Toys
– Balloons – Coins – Balls – Marbles
• Hardware
Presenter
Presentation Notes
Food items are the most common items aspirated by infants and toddlers, whereas nonfood items (eg, coins, paper clips, pins, pen caps) are more commonly aspirated by older children [18-21]. Toy balloons are the object most commonly involved in fatal childhood FBA; balls, marbles, and other toys also are commonly involved [18,22]. Factors that make foreign bodies more dangerous include roundness (round objects are most likely to cause complete airway obstruction and asphyxiation), failure to break apart easily, compressibility, and smooth, slippery surface [23].
Foreign Body Location
• Majority in the bronchi • Study out of Turkey looked at 1160 children
for suspected FBA – FB removed in 1068 (92%) – 60% right lung – 23% left lung – 13% trachea/carina – 3% larynx
Presenter
Presentation Notes
2003: he majority, 885 (76.3%), presented with a definite history of foreign body aspiration. Bronchoscopy was negative in 85 (7.3%) children. Watermelon seeds, found in 414 (38.7%) children, were the most commonly aspirated foreign bodies. Open surgical procedures were required for 21 (1.8%) children. Bronchial rupture related to bronchoscopy occurred in four children, two of whom died post-operatively. The overall mortality rate was 0.8%.
Presentation
• History of choking • Drooling • Refusal to eat • Vomiting • Focal monophonic wheezing • Decreased air entry • Respiratory distress
Presenter
Presentation Notes
Presentation and diagnosis of 50 to 75% of cases occurs in first 24 hours Witness episode of choking sensitivity of 76 to 92% for dx of FBA
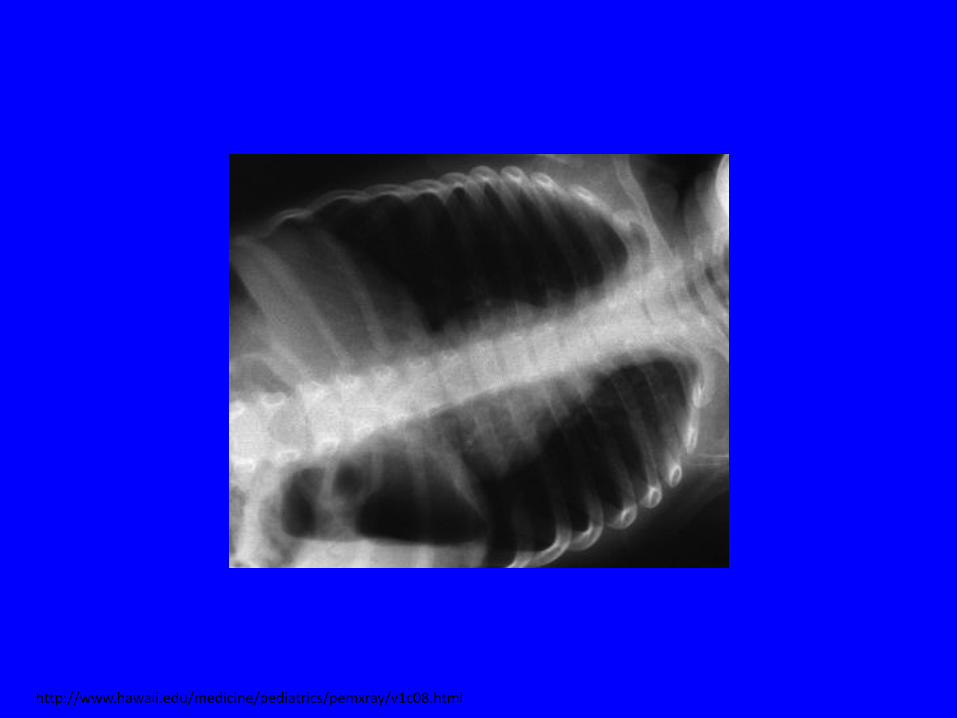
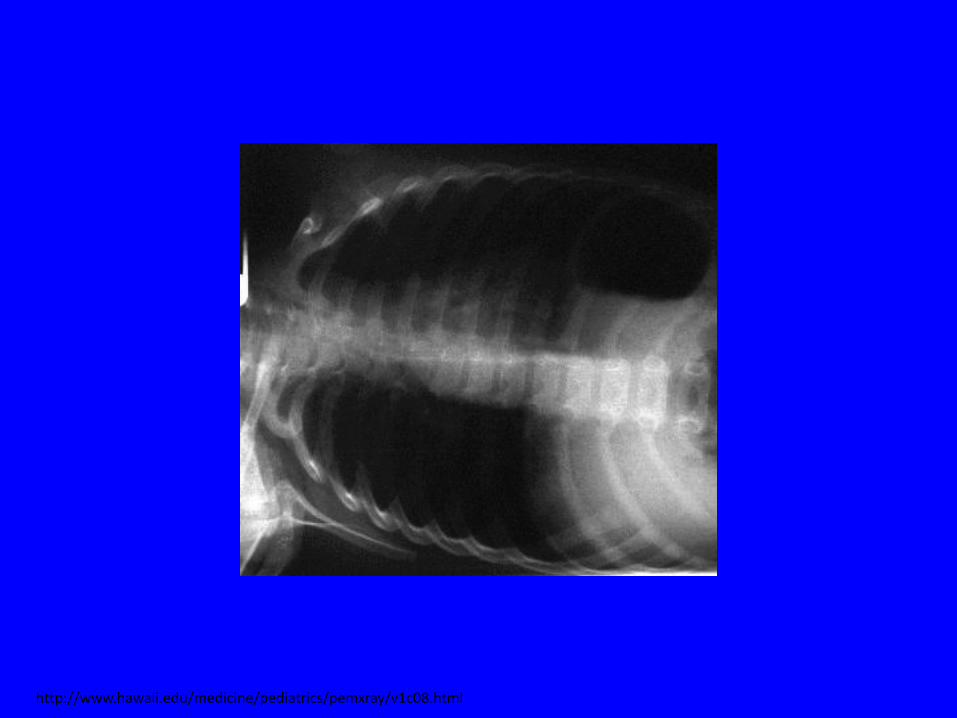
Imaging
• Diagnosis easy when radioopaque (only 10% of FB)
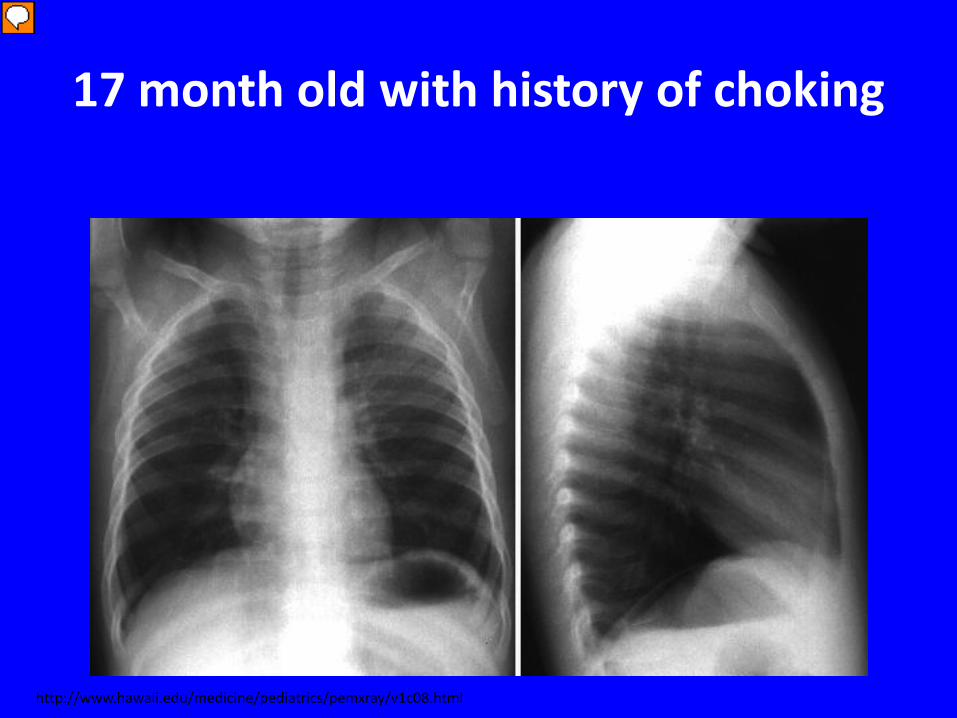
a one-hour history of noisy and abnormal breathing after a choking episode while he was eating a chocolate and almond bar. He was able to speak and drink fluids without difficulty. Vitals WNL He was able to speak, had no cyanosis, no drooling, and no dyspnea. His lung sounds showed mild wheezing with possible mild inspiratory stridor. An albuterol aerosol was administered but no improvement was noted. A chest radiograph was ordered.
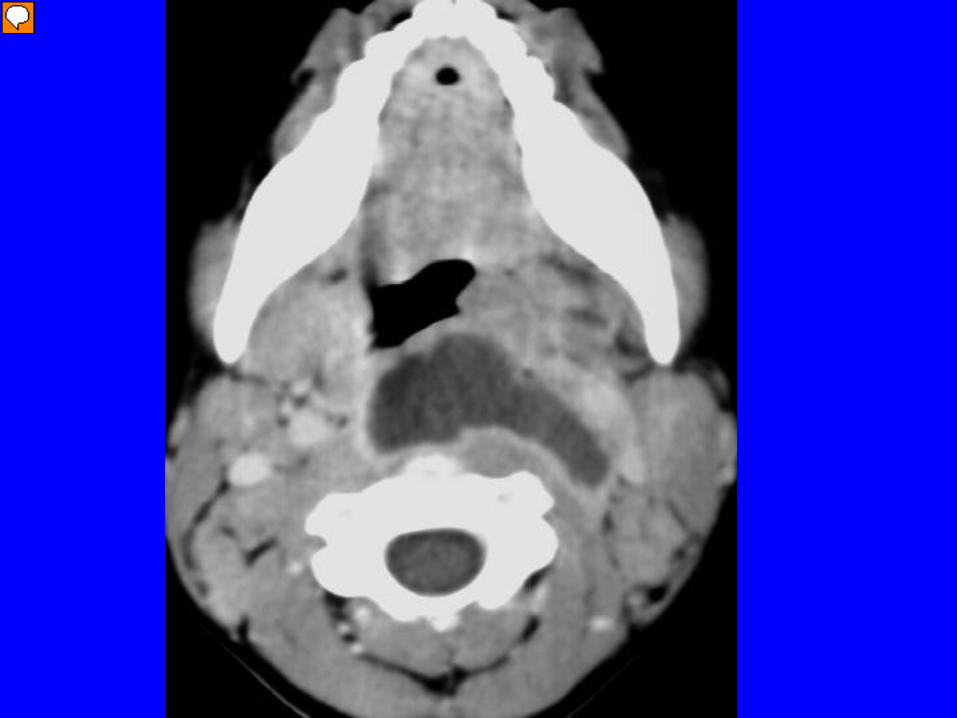
• Infection in potential space between posterior pharyngeal wall and prevertebral fascia
• Cause: – Medical (45%) – Traumatic (27%) – Idiopathic
– INSERT PIC SHOWING RETRO SPACE HERE!!
Presenter
Presentation Notes
Nontraumatic more likely in younger children suppuration of the retrophar- yngeal lymph nodes, which drain from the nasopharynx, oropharynx, nose, paranasal sinuses, adenoids and tonsils. TRAUMATIC: Regional accidental trauma, foreign body ingestion, complication of procedures, or an immunocompromised state account for the majority of adult cases MEDICAL: paranasal sinus infection, nasopharynx, adenoids, or otitis media infections develop in the potential space located between the posterior pharyngeal wall and the prevertebral fascia
Retropharyngeal Abscess
• Occur in children less than 6yo – Peak incidence age 3yo
• Usually preceeded by URI – Pharyngitis – Tonsillitis – Sinusitis – Cervical lymphadenitis
Presenter
Presentation Notes
reduced incidence of retropharyngeal infections in older children has been attributed to the atrophy of these lymphatic structures with age
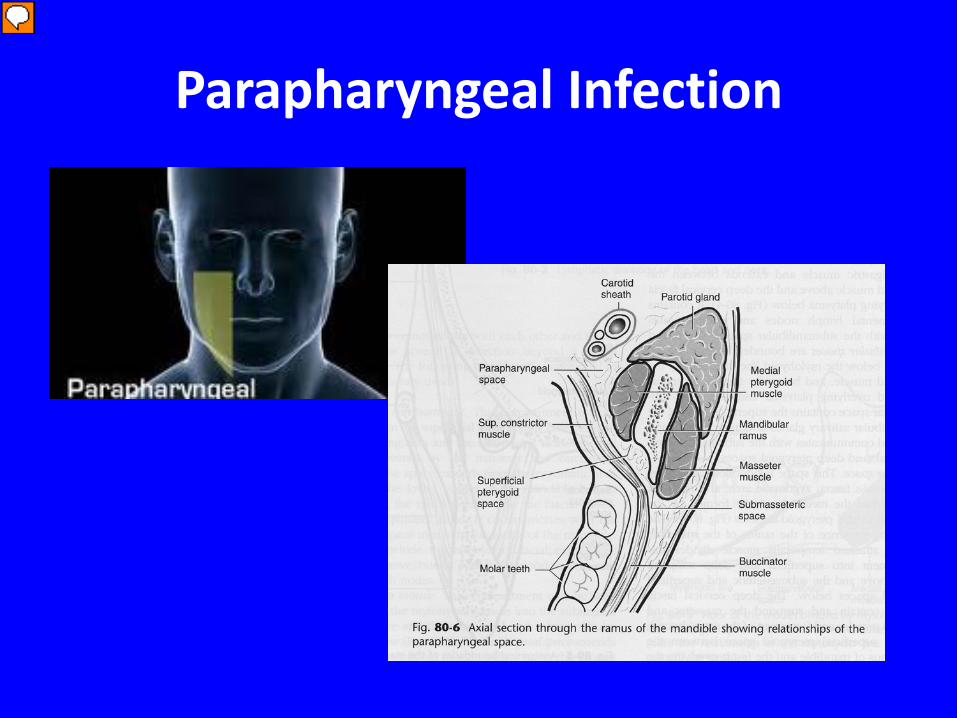
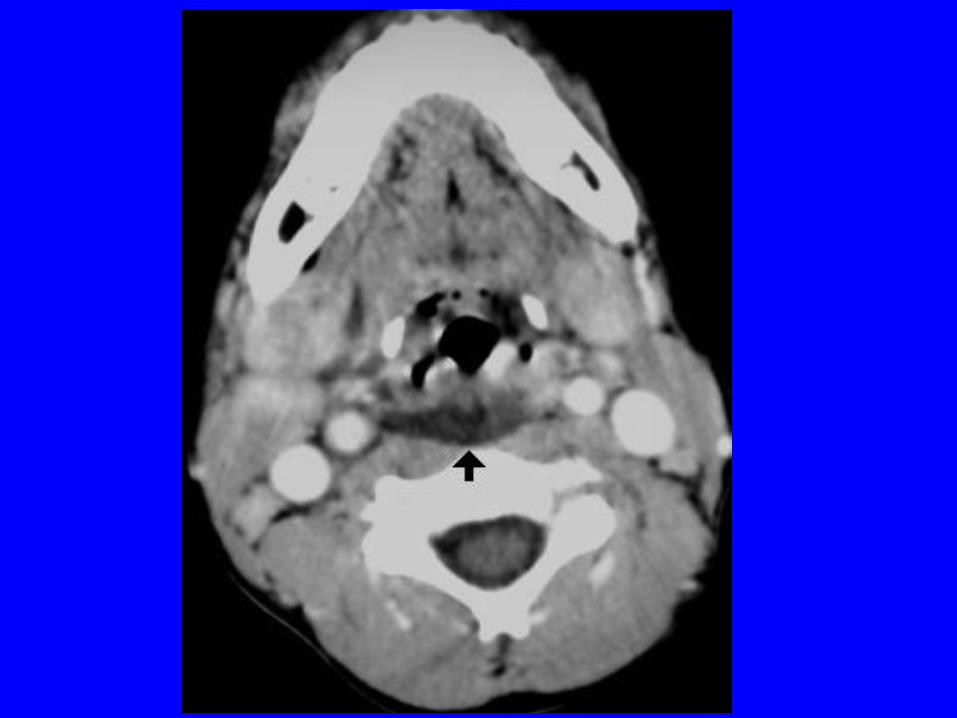
Parapharyngeal Infection
Presenter
Presentation Notes
infections develop in a funnel-shaped space lateral to the pharynx that posteriorly contains the carotid sheath and cranial nerve may be related to complications of pharyngotonsillar, dental, or adjacent deep neck space infections
Parapharyngeal Abscess
• Tend to occur in children 2-12yo • 4th most common deep neck infection • Usually preceeded by URI or history of rapidly
Symptoms similar to epiglottitis but symptoms present more slowly PARAPHARYNGEAL: highly febrile, toxic-appearing child who has neck stiffness. The head may be maintained in a neutral position or rotated away from a unilaterally, diffusely brawny, indurated neck region. The neck may exhibit a true mass.
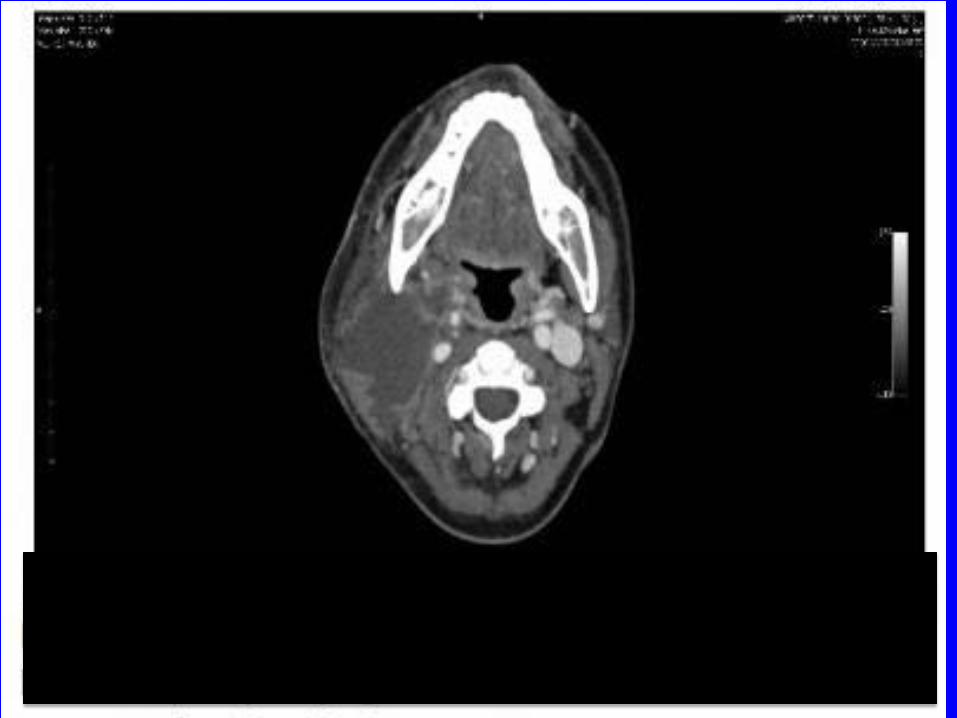
Work-up
• CBC • Blood culture • Imaging
– Lateral neck – CT – Ultrasound
Presenter
Presentation Notes
When looking for parapharyngeal abscess Lateral neck useful to rule out other things Ultrasonography of the neck nonradiating alternative to CT for evaluating deep neck infections as well as monitoring their progression. This modality, especially when combined with color Doppler, can diagnose infections in the early nonsuppurative stage and thereby allow for earlier antibacterial treatment and a reduced number of un- necessary surgeries [56,65,66]. Ultrasonography also has the added benefit of being able to distinguish between adenitis and abscess as well as serve as a tool for guided intraoperative aspiration and drainage
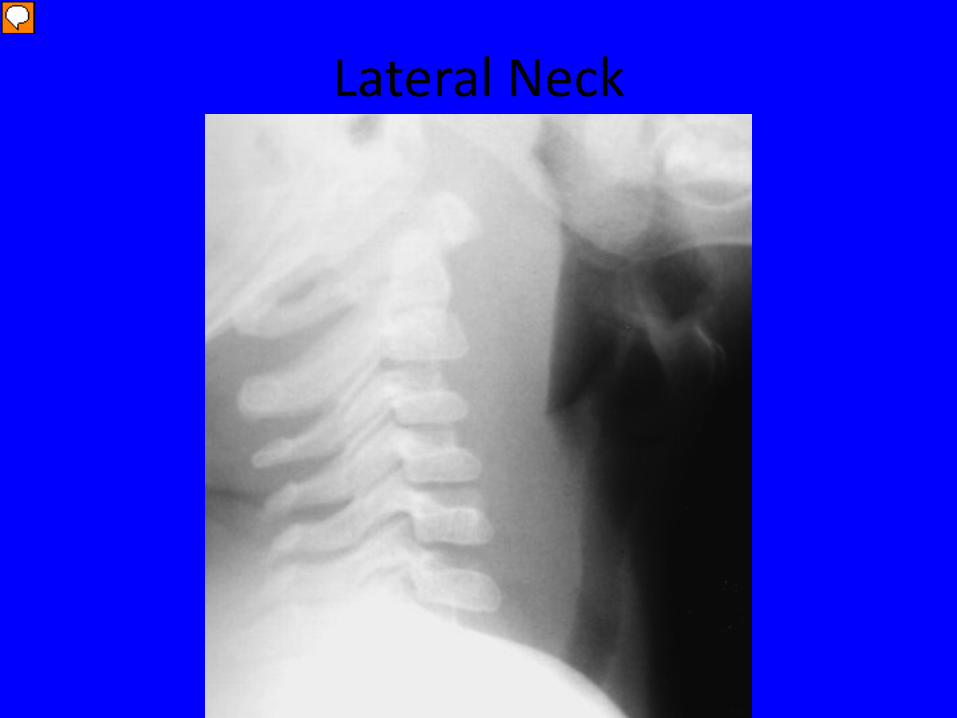
Lateral Neck
Presenter
Presentation Notes
epiglottis is normal in shape. The pre-epiglottic (vallecular) space is preserved. The airway is patent. There is pre-vertebral soft tissue swelling noted. This radiograph is consistent with a retropharygeal abscess, not croup pre-vertebral soft tissue should be no wider than one vertebral body width.
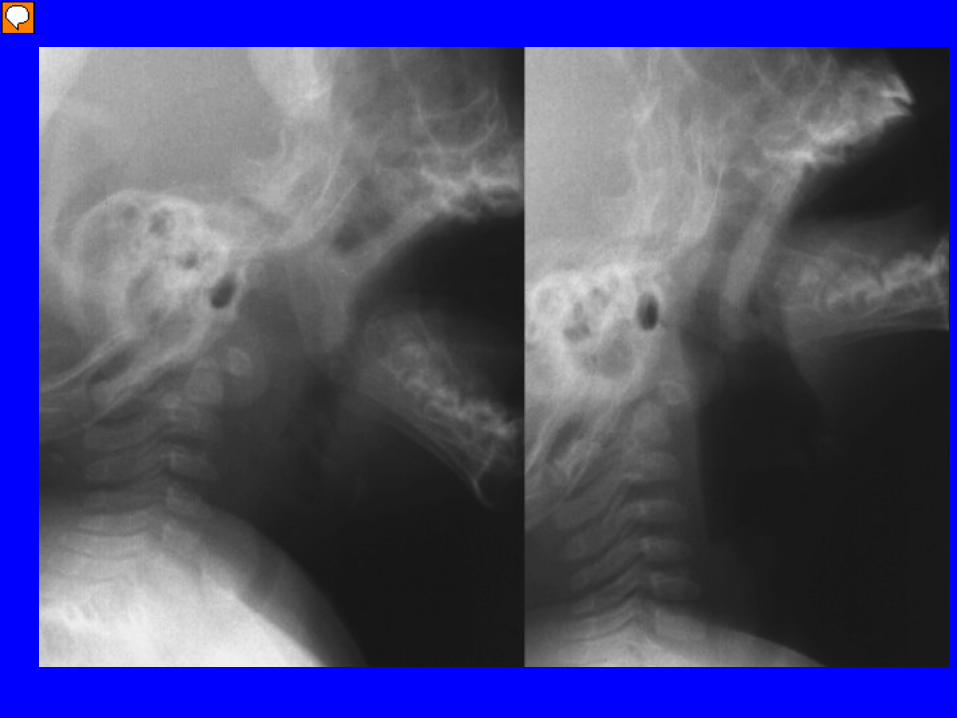
Presenter
Presentation Notes
False positive neck film. On left no hyper extension and looks positive. On right some hyperextension and it goes away
Presenter
Presentation Notes
One study: 95% underwent CT and found: definate abscess in 68%, no abscess in 24%, and possible in 8%. 19 went to OR and of 19, 17 had CT. Of those 17: the surgical and CT findings of these 17 patients were as follows: pus was found in 13 of them during the surgery and their CT scans were interpreted as a showing a definite abscess in 12 and a possible abscess in one. No pus was found during surgery in the other four patients although their CTs showed evidence of an abscess. Sensitivity 92% and specificity 0% Another study sensitivity 43% and specificity 63% when trying to decipher abscess vs cellulitis NO consensus
Retropharyngeal abscesses can result in septicemia, mediastinitis, aspiration pneumonia, empyema, and serious vascular complications, including thrombosis of the internal jugular vein and erosion of the internal carotid artery, pericarditis, and epidural abscess Mediastinits = WATCH out for chest pain, dyspnea, recurrace of fever, CXR evidence
Peritonsillar Abscess
• Most common deep neck infection in children and adolescents
• Commonly preceeded by tonsillitis or pharyngitis
• Can be a clinical diagnosis
Presenter
Presentation Notes
Peritonsillar abscess is a collection of pus located between the capsule of the palatine tonsil and the pharyngeal muscles Peritonsillar infection generally is preceded by tonsillitis or pharyngitis and progresses from cellulitis to phlegmon to abscess [4]. PTA also may occur without preceding infection; such cases are thought to be caused by obstruction of the Weber glands (a group of salivary glands in the soft palate just superior to the tonsil and connected to the surface of the tonsil by a duct) [5-7]. Smoking appears to be a risk factor [
Vanc and linezolid used when mrsa not sensitive to clinda Complications similar to RPA
Deep Neck Infections
• Start IV antibiotics as soon as possible • Get ENT on board early • Monitor for potential complications
Summary
● Trauma ●Remember the Katz extractor and Mother kiss for foreign body removal ● Always keep foreign body in the differential diagnosis for a first time wheeze ● Be mindful for the patient’s potential to deteriorate with deep neck infections
References • Al- Sabah, Basel, et al. Retropharyngeal Abscess in Children: 10-year
Study. The Journal of Otolaryngology. 33:6, 2004. • Amin, Suhail, et al. Acute retropharyngeal abscess with torticollis
and cervical subluxation – Acase report and review of literature. International Journal of Pediatric Otorhinolaryngology Extra. 6 (2011): 252-255.
• Grisaru-Soen, Galia, et al. Retropharyngeal and perapharyngeal abscess in children – Epidemilogy, clinical features and treatment. International Jouranal of Pediatric Otorhinolaryngology.
• Eren, S, et al. Foreign body aspiration in children: experience 1160 cases. Annals of Tropical Paediatrics.
References 1) Current management of penetrating injuries of the
soft palate • How to Repair a Lingual Laceration - Article • 3 by Drs. Brad Stevinson, Jennie Buchanan and Peter
Pryor on June 20, 2012 • 4) Ann R Coll Surg Engl. 2008 July; 90(5): 420–422. • doi: 10.1308/003588408X300966 • PMCID: PMC2645753 • The ‘Parent's Kiss’: An Effective Way to Remove