Embed Size (px)
Citation preview

Update on Antibiotic Treatment of Emergency Department InfectionsUpdate on Antibiotic Treatment of Emergency Department Infections
David A. Talan, MD, FACEP, FIDSADavid A. Talan, MD, FACEP, FIDSA
Professor and ChairProfessor and Chair
UCLA School of MedicineUCLA School of Medicine
Olive View-UCLA Dept. of Emergency Medicine Olive View-UCLA Dept. of Emergency Medicine
and Division of Infectious Diseasesand Division of Infectious Diseases
David A. Talan, MD, FACEP, FIDSADavid A. Talan, MD, FACEP, FIDSA
Professor and ChairProfessor and Chair
UCLA School of MedicineUCLA School of Medicine
Olive View-UCLA Dept. of Emergency Medicine Olive View-UCLA Dept. of Emergency Medicine
and Division of Infectious Diseasesand Division of Infectious Diseases


Adjusted Mortality Odds Ratio P
Initial abx < 8 hrs 0.85 (0.75-0.96) <0.001 (75.5%)
Meehan TP. JAMA 1997;278:2080.
Adjusted Mortality Odds Ratio P
Initial abx < 8 hrs 0.85 (0.75-0.96) <0.001 (75.5%)
Meehan TP. JAMA 1997;278:2080.
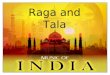
Time to Antibiotics for CAP: Mortality and Length of Stay
Time to Antibiotics for CAP: Mortality and Length of Stay
ED Abx (n=473)ED Abx (n=473)
LOS <9 days 71% 51% (OR 0.31*)
(ED 3.5 + 1.4 vs. after 9.5 + 3.0 hrs) Battleman DS. Arch Intern Med 2002:162:682.
LOS <9 days 71% 51% (OR 0.31*)
(ED 3.5 + 1.4 vs. after 9.5 + 3.0 hrs) Battleman DS. Arch Intern Med 2002:162:682.
LOS >9 days(n=136)
LOS >9 days(n=136)

What's New in 2003?What's New in 2003?
Emerging bacterial resistance New antibiotics Short-course regimens Outpatient management Practice guidelines Restricting diagnoses/antibiotic use
Emerging bacterial resistance New antibiotics Short-course regimens Outpatient management Practice guidelines Restricting diagnoses/antibiotic use

Levofloxacin (Levaquin) Moxifloxacin (Avelox) Gatifloxacin (Tequin) Ertapenam (Invanz) Augmentin XR (1000 mg amoxicillin,
dose: 2 tabs Q 12 hours) Cipro XR (500-1000 mg QD)
Levofloxacin (Levaquin) Moxifloxacin (Avelox) Gatifloxacin (Tequin) Ertapenam (Invanz) Augmentin XR (1000 mg amoxicillin,
dose: 2 tabs Q 12 hours) Cipro XR (500-1000 mg QD)
Newer AntibioticsNewer Antibiotics
QuinolonesQuinolones withwith
enhancedenhanced pneumococcalpneumococcal
activityactivity
QuinolonesQuinolones withwith
enhancedenhanced pneumococcalpneumococcal
activityactivity

Azithromycin (Zithromax) Cefadroxil (Duricef) AminoglycosidesCefixime (Suprax) Ceftriaxone (Rocephin)Ceftibuten (Cedax) Ertapenam (Invanz)Cefdinir (Omnicef)Levofloxacin (Levaquin) Moxifloxacin (Avelox)Gatifloxacin (Tequin)Clarithromycin ER (Biaxin XL)
Azithromycin (Zithromax) Cefadroxil (Duricef) AminoglycosidesCefixime (Suprax) Ceftriaxone (Rocephin)Ceftibuten (Cedax) Ertapenam (Invanz)Cefdinir (Omnicef)Levofloxacin (Levaquin) Moxifloxacin (Avelox)Gatifloxacin (Tequin)Clarithromycin ER (Biaxin XL)
Once-Per-Day AntibioticsOnce-Per-Day Antibiotics
Oral Parenteral

DRSP (including QR-DRSP)
Macrolide-res. S. pneumoniae/pyogenes
TMP/SMX/FG ceph./Quinolone-res. E. coli
Quinolone-res. N. gonorrheae (QRNG)
Community-acquired (CA-MRSA)
DRSP (including QR-DRSP)
Macrolide-res. S. pneumoniae/pyogenes
TMP/SMX/FG ceph./Quinolone-res. E. coli
Quinolone-res. N. gonorrheae (QRNG)
Community-acquired (CA-MRSA)
Emerging Bacterial ResistanceEmerging Bacterial Resistance

Dx: inflamed and immobile TM
New higher dose, shorter duration
No treatment OK - 2 day follow-up
Dx: inflamed and immobile TM
New higher dose, shorter duration
No treatment OK - 2 day follow-up
Acute Otitis Media: New ConceptsAcute Otitis Media: New Concepts

Wait and See Approach for Acute Otitis Media in British Children
Wait and See Approach for Acute Otitis Media in British Children
Days of earache 2.6 3.6
Nights disturbed 1.6 2.5
Days school missed 2.0 2.1
Diarrhea (%) 19 9
Very satisfied (%) 91 77
Would need MD in future (%) 83 63
Days of earache 2.6 3.6
Nights disturbed 1.6 2.5
Days school missed 2.0 2.1
Diarrhea (%) 19 9
Very satisfied (%) 91 77
Would need MD in future (%) 83 63
Immediate Rx(98% used, n=135)
Immediate Rx(98% used, n=135)
Pick up Rx in 3 day(24% used, n=150)
Pick up Rx in 3 day(24% used, n=150)
Non-blind, randomized 6 months to 10 years Pain & erythema, bulging or perforation
Non-blind, randomized 6 months to 10 years Pain & erythema, bulging or perforation
Little P. BMJ 2001:322:336.Little P. BMJ 2001:322:336.

Acute Otitis Media: 1999 US CDC Working Group
Acute Otitis Media: 1999 US CDC Working Group
1st line - HD amoxicillin - 80-90 mg/kg/day (BID, - HD amoxicillin - 80-90 mg/kg/day (BID, to 2 grams, up to 1 grams TID)to 2 grams, up to 1 grams TID)
2nd line - HD amoxicillin/clavulanate, cefuroxime, - HD amoxicillin/clavulanate, cefuroxime, IM ceftriaxone (50 mg/kg)IM ceftriaxone (50 mg/kg) Risk groups - day care, prior abx, < 2 years Refractory cases - IM ceftriaxone QD X3,
clindamycin, tympanocentesis
1st line - HD amoxicillin - 80-90 mg/kg/day (BID, - HD amoxicillin - 80-90 mg/kg/day (BID, to 2 grams, up to 1 grams TID)to 2 grams, up to 1 grams TID)
2nd line - HD amoxicillin/clavulanate, cefuroxime, - HD amoxicillin/clavulanate, cefuroxime, IM ceftriaxone (50 mg/kg)IM ceftriaxone (50 mg/kg) Risk groups - day care, prior abx, < 2 years Refractory cases - IM ceftriaxone QD X3,
clindamycin, tympanocentesis
Dowell SF. Pediatr Infect Dis J 1999;18:1.Dowell SF. Pediatr Infect Dis J 1999;18:1. Avoid: cefaclor, cefprozil, Avoid: cefaclor, cefprozil, cefixime, ceftibuten b/o DRSP activitycefixime, ceftibuten b/o DRSP activity
Avoid: cefaclor, cefprozil, Avoid: cefaclor, cefprozil, cefixime, ceftibuten b/o DRSP activitycefixime, ceftibuten b/o DRSP activity
A/C >AZ bac and clin. curePed Infect Dis J 2000:19:95.
3 days > 1 day (DRSP)Ped Infect Dis J 2000:19:1040.

Community-Acquired PneumoniaCommunity-Acquired Pneumonia

US Study to Predict Low-Risk Pneumonia Patients
US Study to Predict Low-Risk Pneumonia Patients
Less than 50 years of age
No history of cancer, CHF, cerebrovascular, HIV, renal or liver disease
Normal mental status
P < 125, RR < 30, BP > 90, T 35-40oC
Less than 50 years of age
No history of cancer, CHF, cerebrovascular, HIV, renal or liver disease
Normal mental status
P < 125, RR < 30, BP > 90, T 35-40oC
Fine MJ. NEJM 1997;336:243.Fine MJ. NEJM 1997;336:243.

CAP Mortality Prediction RuleCAP Mortality Prediction Rule
Demographic: Exam:Age (-10 women) MS, RR >30, BP< 90 20 Nursing home 10 HR >125 15
T < 35o or > 40oC 10Co-morbidity: Lab:Cancer 30 pH < 7.35 30CHF 20 BUN > 30, Na < 130 20CVA, renal, liver 10 Glu>250, Hct <30, 10
pO2 <60, pleural effusion
Fine MJ. NEJM 1997;336:243.
Demographic: Exam:Age (-10 women) MS, RR >30, BP< 90 20 Nursing home 10 HR >125 15
T < 35o or > 40oC 10Co-morbidity: Lab:Cancer 30 pH < 7.35 30CHF 20 BUN > 30, Na < 130 20CVA, renal, liver 10 Glu>250, Hct <30, 10
pO2 <60, pleural effusion
Fine MJ. NEJM 1997;336:243.

CAP Risk Classes, Mortality, and Management
CAP Risk Classes, Mortality, and Management
Risk Class - score 30 Day Mortality (%) Rec. Care
I <0.5 Outpatient II <70 0.5-1 Outpatient III 71-90 1-4 Inpatient (brief) IV 91-130 4-10 Inpatient V >130 >10 Inpatient
Fine MJ. NEJM 1997;336:243.
Risk Class - score 30 Day Mortality (%) Rec. Care
I <0.5 Outpatient II <70 0.5-1 Outpatient III 71-90 1-4 Inpatient (brief) IV 91-130 4-10 Inpatient V >130 >10 Inpatient
Fine MJ. NEJM 1997;336:243.

Canadian CAP Clinical Pathway TrialCanadian CAP Clinical Pathway Trial
ED Dx Pneumonia22 hospitals, 1,743 patients
ED Dx Pneumonia22 hospitals, 1,743 patients
Pneumonia score (+Pox) given to MD by nurse
<90 recommended d/c home
Pneumonia score (+Pox) given to MD by nurse
<90 recommended d/c homeStandard careStandard care
Inpatient care - 31%Inpatient care - 31% Inpatient care - 49%Inpatient care - 49%
2 &6 week QOL scores37 & 43
2 &6 week QOL scores37 & 43
2 &6 week QOL scores38 & 41
2 &6 week QOL scores38 & 41
Marrie TJ. JAMA 2000;283:749.Marrie TJ. JAMA 2000;283:749.

US CAP Antimicrobial StrategiesUS CAP Antimicrobial Strategies
Pneumococcal Etiology (Degree of Illness)
Pneumococcal Etiology (Degree of Illness)
DRSP(Prevalence, prior Abx/ hosp.)
DRSP(Prevalence, prior Abx/ hosp.)
Atypical Etiology (Young age)
Atypical Etiology (Young age)
MacrolideDoxycycline
MacrolideDoxycycline
New fluoroquinolones2nd-3rd GC/Macrolide
New fluoroquinolones2nd-3rd GC/Macrolide

Azithromycin 500/250 mg QD (5 d)
Clarithromycin 500 mg BIDDoxycycline 100 mg BID
-lactam (HD amox, amox/clav, ceftriaxone -cefpodoxime /cefuroxime) with aboveLevofloxacin 500 mg QD
Moxifloxacin 400 mg QD Gatifloxacin 400 mg QD
Azithromycin 500/250 mg QD (5 d)
Clarithromycin 500 mg BIDDoxycycline 100 mg BID
-lactam (HD amox, amox/clav, ceftriaxone -cefpodoxime /cefuroxime) with aboveLevofloxacin 500 mg QD
Moxifloxacin 400 mg QD Gatifloxacin 400 mg QD
CAP: Outpatient Treatment in USCAP: Outpatient Treatment in US
Oral regimens10-14 days
Oral regimens10-14 days
American Thoracic Society. Am J Respir Crit Care Med 2001;163:1730.Bartlett JG. Clin Infect Dis 2000;31:347. CDC. Arch Intern Med 2000;160:1399.
American Thoracic Society. Am J Respir Crit Care Med 2001;163:1730.Bartlett JG. Clin Infect Dis 2000;31:347. CDC. Arch Intern Med 2000;160:1399.
treatment failureshigh-riskdocumented DRSP
treatment failureshigh-riskdocumented DRSP

Worldwide OutpatientCAP Guidelines
Worldwide OutpatientCAP Guidelines
Country/Org/YearCountry/Org/Year RecommendationRecommendation
ACEP 2001 See US IDSAUS IDSA 2000 Macrolide or doxycycline or FQCanadian ID/TS 2000 Macrolide or doxycycline
mod. factor – FQUS ATS 2001 “ or BLI+ macrolideFrance 1991 AmoxicillinItaly 1995 BLI + macrolideSpain 1992 Penicillin or erythromycinUK BTS 2001 Amoxicillin HD or macrolide
ACEP 2001 See US IDSAUS IDSA 2000 Macrolide or doxycycline or FQCanadian ID/TS 2000 Macrolide or doxycycline
mod. factor – FQUS ATS 2001 “ or BLI+ macrolideFrance 1991 AmoxicillinItaly 1995 BLI + macrolideSpain 1992 Penicillin or erythromycinUK BTS 2001 Amoxicillin HD or macrolide

CAP: Inpatient Treatment in USCAP: Inpatient Treatment in US
2nd/3rd gen. cephalosporin plus azithro or doxy Levofloxacin 500 mg Q24o
Gatifloxacin 400 mg Q24o
Moxifloxacin 400 mg Q24o
2nd/3rd gen. cephalosporin plus azithro or doxy Levofloxacin 500 mg Q24o
Gatifloxacin 400 mg Q24o
Moxifloxacin 400 mg Q24o
ATS. Am J Respir Crit Care Med 2001;163:1730.Bartlett JG. Clin Infect Dis 2000;31:347. CDC. Arch Intern Med 2000;160:1399.Finch R. Antimicrob Agents Chemother 2002;1746.
ATS. Am J Respir Crit Care Med 2001;163:1730.Bartlett JG. Clin Infect Dis 2000;31:347. CDC. Arch Intern Med 2000;160:1399.Finch R. Antimicrob Agents Chemother 2002;1746.
Ceftriaxone plus either
New Quinolone
or
Macrolide and aminoglycoside
Ceftriaxone plus either
New Quinolone
or
Macrolide and aminoglycoside
FloorFloor ICUICU
Consider vancomycin ifquinolone exposure
Consider vancomycin ifquinolone exposure

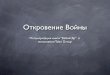
3rd gen. ceph plus macrolide 0.66 (0.51-0.86)
Fluoroquinolone only 0.64 (0.36-1.14)
-lactamase inh. plus macrolide 1.61 (1.08-2.39)
3rd gen. cephalosporin only reference
3rd gen. ceph plus macrolide 0.66 (0.51-0.86)
Fluoroquinolone only 0.64 (0.36-1.14)
-lactamase inh. plus macrolide 1.61 (1.08-2.39)
3rd gen. cephalosporin only reference
US Study of Relative 30-Day Mortality by Initial Antibiotic Regimen for CAP
US Study of Relative 30-Day Mortality by Initial Antibiotic Regimen for CAP
Gleason PP. Arch Intern Med 1999;159:2562.Gleason PP. Arch Intern Med 1999;159:2562.
Adjusted hazard ratio (95% CI)Adjusted hazard ratio (95% CI)9,751 patients > 65 yrs, regimen9,751 patients > 65 yrs, regimenwithin 48 hrs of admissionwithin 48 hrs of admission9,751 patients > 65 yrs, regimen9,751 patients > 65 yrs, regimenwithin 48 hrs of admissionwithin 48 hrs of admission

Cystitis Pathogen Antimicrobial Resistance - Seattle 1992-6
Cystitis Pathogen Antimicrobial Resistance - Seattle 1992-6
92 93 94 95 96
AMP
CEPH
NITRO
T/S
CIPRO
%%%%
Gupta K. Gupta K. JAMAJAMA 1999;281:736. 1999;281:736.Gupta K. Gupta K. JAMAJAMA 1999;281:736. 1999;281:736.
10101010
20202020
30303030
40404040
Shift to quinolones/nitrofurantoin/3rd gen. cephs.

Cystitis: Effect of T/S Resistance on Clinical Success in T/S-Treated Patients In Israel
Cystitis: Effect of T/S Resistance on Clinical Success in T/S-Treated Patients In Israel
0
10
20
30
40
50
60
70
80
90
100
Susceptible Resistant
%%
Raz R. Clin Infect Dis 2002;34:1165. (follow-up 4-6 weeks)Raz R. Clin Infect Dis 2002;34:1165. (follow-up 4-6 weeks)
Resistance mattersLow morbidity disease
Resistance mattersLow morbidity disease
54%(81/151)
88%(293/333)

TMP/SMX BS BID (n=39) 82*
Nitrofurantoin 100 mg QID (n=36) 61
Cefadroxil 500 mg BID (n=32) 66
Amoxicillin 500 mg QID (n=42) 67
TMP/SMX BS BID (n=39) 82*
Nitrofurantoin 100 mg QID (n=36) 61
Cefadroxil 500 mg BID (n=32) 66
Amoxicillin 500 mg QID (n=42) 67
Three-Day Cystitis RegimensThree-Day Cystitis Regimens
Hooton TM. JAMA 1995;273:41.Hooton TM. JAMA 1995;273:41.
% Cure 2 weeks% Cure 2 weeks
At least 7 days
At least 7 days

Routine culture not recommended 3 days -more effective than 1 dose
less side effects than 7 days TMP/SMX DS BID (if < 20% resistance) Levofloxacin 250 mg QD Ciprofloxacin XR 500 mg QD Ofloxacin 200 mg BID Gatifloxacin 400 mg QD 7 days – Nitrofuratoin (low-cost/resistance)
Cephalexin (resistance), 3rd GC Culture if no symptom resolution in 2 days
Routine culture not recommended 3 days -more effective than 1 dose
less side effects than 7 days TMP/SMX DS BID (if < 20% resistance) Levofloxacin 250 mg QD Ciprofloxacin XR 500 mg QD Ofloxacin 200 mg BID Gatifloxacin 400 mg QD 7 days – Nitrofuratoin (low-cost/resistance)
Cephalexin (resistance), 3rd GC Culture if no symptom resolution in 2 days
Therapy for Uncomplicated CystitisTherapy for Uncomplicated Cystitis
Cost-effectiveness modelsupports at 22% T/S resistance rate
Clin Infect Dis 2002:33:615.

Acute Uncomplicated Pyelonephritis in US: Cipro 7 Days vs. TMP/SMX 14
Days
Acute Uncomplicated Pyelonephritis in US: Cipro 7 Days vs. TMP/SMX 14
Days
0102030405060708090
100
PO +/- IVCipro
PO T/S +/-IV Ceftri-axone
%%
p =.004 99%(113) 89%
(101) 85% (111) 74%
(108)
p =.08
Talan DA. Talan DA. JAMA JAMA 2000;283:1583.Talan DA. Talan DA. JAMA JAMA 2000;283:1583.
91%(106)
77%(106)
96%(113)
83%(111)
p =.002p =.015
4-11 days 22-48 days 4-11 days 22-48 days4-11 days 22-48 days 4-11 days 22-48 days
Bacteriologic cureBacteriologic cure Clinical cureClinical cure

Effect of TMP/SMX Resistance in TMP/SMX-Treated AUP Patients
Effect of TMP/SMX Resistance in TMP/SMX-Treated AUP Patients
0
10
20
30
40
50
60
70
80
90
100
Susceptible Resistant
Bacterio-logiccure
Clinicalcure
%%
92%(76/83)
p < 0.0001 (both) p < 0.0001 (both)
96%(73/76)
50%(7/14)
35%(6/17)
Talan DA. Talan DA. JAMA JAMA 2000;283:1583.Talan DA. Talan DA. JAMA JAMA 2000;283:1583.
Resistance mattersHigh morbidity disease
Resistance mattersHigh morbidity disease
Cost/patient Cipro $510 TMP/SMX $725 Cost/patient Cipro $510 TMP/SMX $725

Ciprofloxacin 400 mg Levofloxacin 250 mg Gentamicin 5-7 mg/kg Ceftriaxone 1 gram
Cipro XR 1000 mg QD(7days) Levofloxacin 250 mg QD
Ciprofloxacin 400 mg Levofloxacin 250 mg Gentamicin 5-7 mg/kg Ceftriaxone 1 gram
Cipro XR 1000 mg QD(7days) Levofloxacin 250 mg QD
Outpatient ED Treatment of Acute Uncomplicated Pyelonephritis
Outpatient ED Treatment of Acute Uncomplicated Pyelonephritis
Initial PO/IV Dose
Oral regimens
QREC Spain 17% ’96Garau J. AAC 1999;43:2736.
QREC Spain 17% ’96Garau J. AAC 1999;43:2736.

Cefixime 400 mg Ceftriax. 125/cefotax. 500 mg IM Ciprofloxacin 500 mg* Ofloxacin 400 mg* Levofloxacin 250 mg*
Azithro 1 gram Doxy 100 mg BID X 7 d
Cefixime 400 mg Ceftriax. 125/cefotax. 500 mg IM Ciprofloxacin 500 mg* Ofloxacin 400 mg* Levofloxacin 250 mg*
Azithro 1 gram Doxy 100 mg BID X 7 d
Treatment of Urethritis and Cervicitis Treatment of Urethritis and Cervicitis
GonorrheaGonorrhea
ChlamydiaChlamydia
Female sex workersBangladesh-GCcervicitis
micro. successCipro susc. (62%) 97.5% Cipro resist. (38%) 8.3 %
Rahman M. Clin Infect Dis 2001;32:884)
Female sex workersBangladesh-GCcervicitis
micro. successCipro susc. (62%) 97.5% Cipro resist. (38%) 8.3 %
Rahman M. Clin Infect Dis 2001;32:884)
Not where QRNGNot where QRNG
Widespread QRNG – SE Asia, India, Israel,othersWidespread QRNG – SE Asia, India, Israel,others


Acute Cellulitis / LymphangitisAcute Cellulitis / Lymphangitis
Kontiainen S. Eur J Clin Microbiol 1987;6 :420.Kontiainen S. Eur J Clin Microbiol 1987;6 :420.
Staphylococcus aureus Streptococcus pyogenes
First-generation cephalosporinsLong acting - ceftriaxoneprobenecid/cefazolinazithromycin/linezolid
Staphylococcus aureus Streptococcus pyogenes
First-generation cephalosporinsLong acting - ceftriaxoneprobenecid/cefazolinazithromycin/linezolid

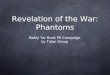
Canadian Study of Effect of Probenecid on Cefazolin Concentrations
Canadian Study of Effect of Probenecid on Cefazolin Concentrations
0 4 8 12 16 20 24
Cefazolin +Probenecid(1 gr each)
Cefazolin1gr alone10101010
100100100100
1000100010001000
Cef
azo
lin
(u
g/m
l)C
efaz
oli
n (
ug
/ml)
Cef
azo
lin
(u
g/m
l)C
efaz
oli
n (
ug
/ml)
HoursHoursHoursHours
Brown G. J Antimicrob Chemother 1993;31:1009. Grayson ML. Clin Infect Dis 2002;34:1440.
1111
Now clinically confirmed!

Community-Associated MRSACommunity-Associated MRSA
Methicillin-resistant Staphylococcus aureus
Also resistant to all penicillins/cephalosporins
Increasing proportion of staph isolates
30% of skin infections at Olive View-UCLA
Susceptible to clindamycin, quinolones,
TMP/SMX,rifampin, tetracylcne, vancomycin
Methicillin-resistant Staphylococcus aureus
Also resistant to all penicillins/cephalosporins
Increasing proportion of staph isolates
30% of skin infections at Olive View-UCLA
Susceptible to clindamycin, quinolones,
TMP/SMX,rifampin, tetracylcne, vancomycin
Naimi TS. Naimi TS. Clin Infect DisClin Infect Dis 2001;33:990. 2001;33:990.Naimi TS. Naimi TS. Clin Infect DisClin Infect Dis 2001;33:990. 2001;33:990.

Otitis- high-dose amoxicillin/Augmentin,
consider wait and see approach CAP - scoring helps, guidelines work, quinolones very
effective, even as ICU monotherapy UTI - short-course and TMP/SMX resistance STDs - quinolone resistance in West, no cefixime,
consider flagyl for PID regimens Infectious diarrhea - antibiotics work CA-MRSA - biggest new problem
Otitis- high-dose amoxicillin/Augmentin,
consider wait and see approach CAP - scoring helps, guidelines work, quinolones very
effective, even as ICU monotherapy UTI - short-course and TMP/SMX resistance STDs - quinolone resistance in West, no cefixime,
consider flagyl for PID regimens Infectious diarrhea - antibiotics work CA-MRSA - biggest new problem
Take Home PointsTake Home Points