Embed Size (px)
Citation preview

Update in Update in TransplantationTransplantation
Jeffrey J. Kaufhold, MD FACPJeffrey J. Kaufhold, MD FACP
Nephrology AssociatesNephrology Associates
December 2003December 2003

Update in TransplantationUpdate in TransplantationSummarySummary
Trends in Survival after transplantTrends in Survival after transplantExpanded Donor KidneysExpanded Donor KidneysWaiting list Management changesWaiting list Management changesTrends in IS protocolsTrends in IS protocolsKidney Pancreas UpdateKidney Pancreas UpdateEthnic Disparities in TransplantsEthnic Disparities in Transplants Immunology and ToleranceImmunology and ToleranceNew approach to ComplicationsNew approach to Complications

Scope of problemScope of problem
300,000 dialysis patients in US300,000 dialysis patients in US 55,000 patients on waiting List55,000 patients on waiting List 17,000 recovered kidneys per year17,000 recovered kidneys per year
11000 from “deceased donors” 11000 from “deceased donors” 6000 from living related donors6000 from living related donors 1000 kidneys not used after recovery1000 kidneys not used after recovery
Average waiting time 5 years !Average waiting time 5 years !

Survival after TransplantSurvival after Transplant
Patient Survival 1 yr Patient Survival 1 yr LRDLRD 98%98% DDDD 9595
Allograft Survival 1 Allograft Survival 1 yryr LRDLRD 95%95% DDDD 8989
Allograft half-lifeAllograft half-life LRD LRD 21 years21 years
5 yrs5 yrs LRD LRD 91 %91 % DDDD 8181
5 years5 years LRDLRD 76%76% DDDD 6161
DD 13.8 yearsDD 13.8 years

Transplant survivalTransplant survival
Relative risk of deathRelative risk of deathTransplanted in Transplanted in 1993 = 1.01993 = 1.0Transplanted inTransplanted in 1998 = 0.741998 = 0.74Currently on Wait listCurrently on Wait list = 1.7= 1.7
These are the healthy ones!These are the healthy ones!Patients not on wait list = 2.6Patients not on wait list = 2.6

Transplant UpdateTransplant Update
Annual Death RatesAnnual Death RatesPts on listPts on list 6.3 %6.3 %Diabetic pts on list Diabetic pts on list 10.8 %10.8 %Pts not on listPts not on list 21 %21 %
Note that “death censored graft loss” Note that “death censored graft loss” is standard measure used in is standard measure used in transplant outcome reports since this transplant outcome reports since this is desired outcome.is desired outcome.

Risk of Graft LossRisk of Graft Loss
Higher riskHigher risk Deceased donorDeceased donor Recipient over 60Recipient over 60 Donor over 60Donor over 60 Recipient raceRecipient race
Black / HispanicBlack / Hispanic Long Cold Ischemic Long Cold Ischemic
timetime Previous TxpPrevious Txp High PRAHigh PRA
Lower RiskLower Risk Living donorLiving donor Recipient under 60Recipient under 60 Donor under 60Donor under 60 Recipient raceRecipient race
AsianAsian Short cold ischemiaShort cold ischemia Higher HLA matchHigher HLA match Low PRALow PRA

Expanded Donor KidneysExpanded Donor Kidneys
Used when risk of Txp is better than Used when risk of Txp is better than life expectancy on dialysislife expectancy on dialysis
CriteriaCriteriaRecipient/donor over 60Recipient/donor over 60Diabetics over 40Diabetics over 40Failing access for dialysisFailing access for dialysisPatient with poor Quality of LifePatient with poor Quality of Life

Transplant UpdateTransplant Update
HLA MatchingHLA MatchingMain HLA groupsMain HLA groups A B C DA B C DC not important for transplant survivalC not important for transplant survivalHost of minor antigensHost of minor antigens
Most important antigens are B and Most important antigens are B and DDD antigen is inducible and responsible D antigen is inducible and responsible
for more serious (vascular) rejectionsfor more serious (vascular) rejections

Waiting list managementWaiting list management
Point system for UNOS Wait listPoint system for UNOS Wait list1 pt per year on list1 pt per year on list7 pts for 0 mismatch with B, DR antigens7 pts for 0 mismatch with B, DR antigens5 pts for 1 mm with B, DR5 pts for 1 mm with B, DR2 pts for 2 mm with B, DR2 pts for 2 mm with B, DR4 pts for match in pt with PRA > 80 %4 pts for match in pt with PRA > 80 %4 pts for Age < 11, 3 pts for age 11-184 pts for Age < 11, 3 pts for age 11-18
National sharing of 0 mismatch kidneysNational sharing of 0 mismatch kidneys17-20 % of all transplants17-20 % of all transplants

Wait list ManagementWait list Management
Ethnic disparity in rates of transplantEthnic disparity in rates of transplantDue to smaller pool of B antigens in AA Due to smaller pool of B antigens in AA
populationpopulationUNOS is changing point system to UNOS is changing point system to
reflect thisreflect thisEliminating points for B antigen reduces Eliminating points for B antigen reduces
the ethnic disparity in points awarded.the ethnic disparity in points awarded.

Trends in TransplantationTrends in Transplantation
Rejection rates and Creatinine at 6 Rejection rates and Creatinine at 6 months are now surrogates for months are now surrogates for allograft survivalallograft survival
Due to improved survival, a study of Due to improved survival, a study of a new drug would need over 9000 a new drug would need over 9000 enrollees to show a difference.enrollees to show a difference.
Rejection rates are down 50 %Rejection rates are down 50 %Cardiovascular death rate improving.Cardiovascular death rate improving.

Trends in TransplantationTrends in Transplantation
Overall Mortality is unchanged!Overall Mortality is unchanged!Death with functioning graft increasingDeath with functioning graft increasingDonor Age olderDonor Age olderRecipient age is olderRecipient age is olderTime on waiting list is longerTime on waiting list is longer
Older, sicker patients are getting Older, sicker patients are getting transplantstransplants

Induction Induction ImmunosuppressionImmunosuppression
Biological AgentsBiological AgentsSteroid use vs steroid sparingSteroid use vs steroid sparingCellcept used in place of ImuranCellcept used in place of ImuranCalcineurin Inhibitors / SirolimusCalcineurin Inhibitors / Sirolimus

Induction Induction ImmunosuppressionImmunosuppression
Biological AgentsBiological AgentsOKT-3 rarely usedOKT-3 rarely usedThymoglobulin (rabbit) Thymoglobulin (rabbit) ATG (polyclonal)ATG (polyclonal)Basiliximab (Simulect) ChimericBasiliximab (Simulect) Chimeric
Anti CD 25/ anti IL-2 receptor monoclonalAnti CD 25/ anti IL-2 receptor monoclonal
Daclizumab (Zenapax) HumanizedDaclizumab (Zenapax) HumanizedAnti CD 25 MonoclonalAnti CD 25 Monoclonal

Induction Induction ImmunosuppressionImmunosuppression
Biological AgentsBiological AgentsExpensive, complex to useExpensive, complex to useUse in high risk patients:Use in high risk patients:
High PRAHigh PRASecond transplantSecond transplantAfrican American recipientAfrican American recipientDelayed Graft functionDelayed Graft function

Induction Induction ImmunosuppressionImmunosuppression
Biological AgentsBiological Agents Basiliximab and Daclizumab Basiliximab and Daclizumab
Anti CD 25 monoclonalsAnti CD 25 monoclonalsDo not deplete lymphocytesDo not deplete lymphocytesWill not stop ongoing rejectionWill not stop ongoing rejectionOther immunosuppression (CNI, steroid, MMF) should Other immunosuppression (CNI, steroid, MMF) should
continue during usecontinue during use
OKT-3, ATG OKT-3, ATG Deplete lymphocytes, stop rejection,Deplete lymphocytes, stop rejection, reduce or withhold other immunosuppression while reduce or withhold other immunosuppression while
in usein use

Induction Induction ImmunosuppressionImmunosuppression
New Biological Agents coming soon:New Biological Agents coming soon:CTL4 Ig CTL4 Ig
stimulates CTL4 coreceptor on T cell which stimulates CTL4 coreceptor on T cell which leads to leads to
Decreased activation Decreased activation Apoptosis of the activated cell lineApoptosis of the activated cell line
LEA 29 Y LEA 29 Y a second generation CTL4 Iga second generation CTL4 Ig

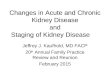
Regulation of T-Cell Regulation of T-Cell ActivationActivation
APC
T-Cell
MHC
TCR
CD 40
CTL4
Negative stimulatory
CD 80/86
CD 25
Positive stimulation
IL -2 Receptor
IL-2
Antigen

T cell CostimulationT cell Costimulation


Induction Induction ImmunosuppressionImmunosuppression
Biological Agents recommendationsBiological Agents recommendationsLow risk patient:Low risk patient:
IL-2 receptor antibody, consider steroid IL-2 receptor antibody, consider steroid sparing regimensparing regimen
High Risk patientHigh Risk patientThymoglobulin plus 3 drug regimenThymoglobulin plus 3 drug regimen
CNI, Steroids, MMFCNI, Steroids, MMF

Maintenance Maintenance ImmunosuppressionImmunosuppression
Categories of Agents:Categories of Agents:SteroidsSteroidsCalcineurin InhibitorsCalcineurin Inhibitors
Intracellular signal modifiersIntracellular signal modifiersCyclosporine, Tacrolimus, PrografCyclosporine, Tacrolimus, Prograf
Adjuvant AgentsAdjuvant AgentsInterfere with cell cyclingInterfere with cell cycling
Sirolimus, RapamicinSirolimus, RapamicinCellcept (MMF)Cellcept (MMF) Imuran (azothioprine)Imuran (azothioprine)

Maintenance Maintenance ImmunosuppressionImmunosuppression
Three Drug Regimen:Three Drug Regimen:Steroid - prednisoneSteroid - prednisoneCalcineurin InhibitorCalcineurin Inhibitor
Cyclosporine, Tacrolimus (Prograf)Cyclosporine, Tacrolimus (Prograf)Adjuvant AgentAdjuvant Agent
Cellcept (MMF)Cellcept (MMF)
Steroid Sparing Regimen:Steroid Sparing Regimen:Prograf + MMF or RapamicinPrograf + MMF or Rapamicin

Drug DosagesDrug Dosages
Steroid Steroid 10 mg daily or every other day10 mg daily or every other day
CyACyA4-6 mg/Kg/day usually 100 - 150 BID4-6 mg/Kg/day usually 100 - 150 BIDLevels 1-6 months: 250 - 400Levels 1-6 months: 250 - 400Level after 6 months: 100 – 250Level after 6 months: 100 – 250
ImuranImuran50 – 100 mg daily at bedtime50 – 100 mg daily at bedtime

Drug DosagesDrug Dosages
PrografPrograf0.1 – 0.2 mg/kg/day0.1 – 0.2 mg/kg/dayUsually about 5 mg BIDUsually about 5 mg BIDLevels 5-15 by ELISALevels 5-15 by ELISA
RapamicinRapamicin6 mg po load then 2 mg po daily6 mg po load then 2 mg po daily
Cellcept (MMF)Cellcept (MMF)1000 mg BID, taper if low WBC or 1000 mg BID, taper if low WBC or
anemia, GI intolerance.anemia, GI intolerance.

Drug Conversion for CauseDrug Conversion for Cause
Refractory Rejection: CyA -> TacRefractory Rejection: CyA -> TacCardiovasc Dz: CyA -> TacCardiovasc Dz: CyA -> Tac
Rapa -> MMFRapa -> MMFDiabetes:Diabetes: decrease steroid dosedecrease steroid dose
Tac -> CyA may be helpfulTac -> CyA may be helpfulHirsuitism: CyA -> TacHirsuitism: CyA -> TacGout: Azo -> MMFGout: Azo -> MMFGingival Hyperplasia: CyA -> TacGingival Hyperplasia: CyA -> Tac
Stop dihydropyridines (procardia XL) Stop dihydropyridines (procardia XL)

Kidney – Pancreas TransplantKidney – Pancreas Transplant

Kidney – Pancreas TransplantKidney – Pancreas TransplantCost:Cost:
Kidney Txp:Kidney Txp: $ 60,000$ 60,000Islet cellsIslet cells 53,000 53,000Panc Txp alonePanc Txp alone 105,000 105,000SPK (K-P)SPK (K-P) 130,000 130,000
Each year on dialysis: Each year on dialysis: $27,000$27,000

Kidney – Pancreas TransplantKidney – Pancreas Transplant
Rejection rates improved Rejection rates improved Options for pancreas placement:Options for pancreas placement:
Attach to bladderAttach to bladderDumps lots of bicarb, CystitisDumps lots of bicarb, CystitisEasy to identify rejection by measuring urine Easy to identify rejection by measuring urine
amylaseamylaseAttach to intestine (enteric anastomosis)Attach to intestine (enteric anastomosis)
Eliminates problems with acidosis and Eliminates problems with acidosis and cystitiscystitis
Rejection harder to identify early.Rejection harder to identify early.

Kidney – Pancreas TransplantKidney – Pancreas Transplant
Rejection Diagnosis:Rejection Diagnosis:HyperglycemiaHyperglycemia
May also occur in face of high steroids, May also occur in face of high steroids, sepsissepsis
Increased serum amylase levelIncreased serum amylase levelDecreased urine amylase level in Decreased urine amylase level in
bladder anastomosis patients.bladder anastomosis patients.Maintenance immunosuppressionMaintenance immunosuppression
Tacrolimus/Cellcept preferred comboTacrolimus/Cellcept preferred comboAvoid steroids if possibleAvoid steroids if possible

Kidney – Pancreas TransplantKidney – Pancreas Transplant
Surgical Complication rate 10% at 1 Surgical Complication rate 10% at 1 yr.yr.
Immunologic Failure Rates:Immunologic Failure Rates:Type of TxpType of Txp % graft loss at 1 yr.% graft loss at 1 yr.
PAKPAK 7 %7 %
PTAPTA 88
SPKSPK 22
Gruessner, Clinical Transplantation 2002, p 52Gruessner, Clinical Transplantation 2002, p 52

Kidney – Pancreas TransplantKidney – Pancreas Transplant
Effect of Pancreas Txp on outcomesEffect of Pancreas Txp on outcomesNo significant QOL improvement compared No significant QOL improvement compared
to kidney aloneto kidney aloneInsulin free for diabetics 50 – 90 %Insulin free for diabetics 50 – 90 %Neuropathy improvesNeuropathy improvesMicrovasculature improvesMicrovasculature improvesRetinopathy – no improvementRetinopathy – no improvementSurvival improved compared to wait list ptsSurvival improved compared to wait list pts
May be slightly better than kidney alone.May be slightly better than kidney alone.

Ethnic Disparities in Ethnic Disparities in TransplantTransplant
Rate of transplantation lower than Rate of transplantation lower than any other ethnic groupany other ethnic group
% of AA patients hearing about the % of AA patients hearing about the option of transplant is only about option of transplant is only about 70% of other groups70% of other groups
Rate of referral once they hear about Rate of referral once they hear about transplant is only about 70% of other transplant is only about 70% of other groups.groups.

Ethnic Disparities in Ethnic Disparities in TransplantTransplant
Socioeconomic Factors:Socioeconomic Factors:70% of AA children born into single parent 70% of AA children born into single parent
homeshomesLess likely to have insuranceLess likely to have insuranceBarriers to travelling to apptsBarriers to travelling to apptsLess likely to be available when calledLess likely to be available when called
No phone or won’t answer due to debtorsNo phone or won’t answer due to debtorsHigher PRA, fewer AA donorsHigher PRA, fewer AA donorsMistrust of systemMistrust of system

Ethnic Disparities in Ethnic Disparities in TransplantTransplant
Insurance Impact on Transplant:Insurance Impact on Transplant:Compared to pts of other ethnic groups Compared to pts of other ethnic groups
with same insurance, 70-80 % of eligible with same insurance, 70-80 % of eligible AA pts get to transplantAA pts get to transplant
HMO rates 70-80 % of eligible pts get to HMO rates 70-80 % of eligible pts get to transplant, evenly across racestransplant, evenly across racesExample of Rationing by InconvenienceExample of Rationing by Inconvenience
Military patients demonstrate NO Military patients demonstrate NO disparity in rates of transplant or Graft disparity in rates of transplant or Graft survival.survival.

Ethnic Disparities in Ethnic Disparities in TransplantTransplant
Immunologic FactorsImmunologic FactorsOnce transplanted, AA pts fare worseOnce transplanted, AA pts fare worse
AA with 0 MM does about as well as Caucasian AA with 0 MM does about as well as Caucasian with 6 MM and 1 rejection episode in first year.with 6 MM and 1 rejection episode in first year.
Require higher doses of ImmunosuppressionRequire higher doses of ImmunosuppressionDon’t tolerate steroid or other drug withdrawal Don’t tolerate steroid or other drug withdrawal
nearly as well as other groupsnearly as well as other groupsHigher levels of IL-6, CD-80, TGF-B, Endothelin, Higher levels of IL-6, CD-80, TGF-B, Endothelin,
Renin.Renin.More Hypertensive, which worsens overall More Hypertensive, which worsens overall
survivalsurvival

RejectionRejection
Clinical Diagnosis:Clinical Diagnosis:HypertensionHypertensionIncreased CreatinineIncreased CreatinineDecreased urine outputDecreased urine output
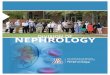
Biopsy findings:Biopsy findings:Tubulitis – usual Vasculitis - badTubulitis – usual Vasculitis - badInterstitial infiltrationInterstitial infiltrationFixing of C 4 dFixing of C 4 d

Rejection Biopsy findingsRejection Biopsy findings

Rejection and ComplementRejection and Complement
Circulating Proteins in blood:Circulating Proteins in blood:#1#1 AlbuminAlbumin#2#2 ImmunoglobulinImmunoglobulin#3#3 Complement, esp C 3.Complement, esp C 3.
Triggers of Complement fixationTriggers of Complement fixationIschemia reperfusion injury (IP - 10)Ischemia reperfusion injury (IP - 10)Brain injury in donorBrain injury in donorDialysis after transplantDialysis after transplantInfectionInfection

Immunology of RejectionImmunology of Rejection
HLA A and B are constitutive HLA A and B are constitutive antigensantigens
HLA D is inducible antigen HLA D is inducible antigen Infection, ischemia induce D antigen Infection, ischemia induce D antigen
expressionexpressionD antigen expression leads to vascular D antigen expression leads to vascular
rejection which is worst typerejection which is worst typeHow does Bactrim SS MWF help? How does Bactrim SS MWF help?

Immunology of RejectionImmunology of Rejection
HLA A and B are constitutive HLA A and B are constitutive antigensantigens
HLA D is inducible antigen HLA D is inducible antigen Infection, ischemia induce D antigen Infection, ischemia induce D antigen
expressionexpressionD antigen expression leads to vascular D antigen expression leads to vascular
rejection which is worst typerejection which is worst typeBactrim SS MWF reduces bacteriuria Bactrim SS MWF reduces bacteriuria

Immunology of RejectionImmunology of Rejection
HLA A and B are constitutive HLA A and B are constitutive antigensantigens
HLA D is inducible antigen HLA D is inducible antigen Infection, ischemia induce D antigen Infection, ischemia induce D antigen
expressionexpressionD antigen expression leads to vascular D antigen expression leads to vascular
rejection which is worst typerejection which is worst typeBactrim SS MWF reduces bacteriuria Bactrim SS MWF reduces bacteriuria What is Acyclovir used for after Txp?What is Acyclovir used for after Txp?

Immunology of RejectionImmunology of Rejection
HLA A and B are constitutive antigensHLA A and B are constitutive antigensHLA D is inducible antigen HLA D is inducible antigen
Infection, ischemia induce D antigen Infection, ischemia induce D antigen expressionexpression
D antigen expression leads to vascular D antigen expression leads to vascular rejection which is worst typerejection which is worst type
Bactrim SS MWF reduces bacteriuria Bactrim SS MWF reduces bacteriuria Acyclovir reduces shedding of Herpes Acyclovir reduces shedding of Herpes
Simplex virus in urineSimplex virus in urine

Immunology of RejectionImmunology of Rejection
Chemoattractant Cytokines Chemoattractant Cytokines (chemokines)(chemokines)Leukocyte recruitmentLeukocyte recruitmentMost important CK is CXCMost important CK is CXCReceptor is CXC-R3Receptor is CXC-R3
Transmembrane proteinTransmembrane proteinActivation of CXC R3 activates rejection pathwayActivation of CXC R3 activates rejection pathwayIP-10 Activates CXC R3IP-10 Activates CXC R3Both CXC R3 and IP-10 are present in urine of pts Both CXC R3 and IP-10 are present in urine of pts
who are rejectingwho are rejecting

Immunology of RejectionImmunology of RejectionThe FutureThe Future
Chemokine receptors:Chemokine receptors:CXC R3 antibody prolongs graft survival CXC R3 antibody prolongs graft survival
in monkey modelsin monkey modelsAlso in clinical trials: CCR-1, CCR-5 Also in clinical trials: CCR-1, CCR-5
which bind CK’s and prevent activation which bind CK’s and prevent activation of receptor.of receptor.
Soluble Complement Receptor CR-1Soluble Complement Receptor CR-1Trypriline decreases synthesis of Trypriline decreases synthesis of
complementcomplementWY14643 ligand for PPAR WY14643 ligand for PPAR

Immunology of RejectionImmunology of RejectionThe FutureThe Future
Protein Tyrosine KinasesProtein Tyrosine Kinases SrcSrc FAKFAK PaxillinPaxillin AktAkt
PPARS peroxisome proliferator activated PPARS peroxisome proliferator activated receptorsreceptors Ligands for PPARs tend to decrease Ligands for PPARs tend to decrease
inflammatory responseinflammatory response Include Piaglitizone, LopidInclude Piaglitizone, Lopid

Immunology of RejectionImmunology of Rejection
Tolerance is the best immunosuppressionTolerance is the best immunosuppressionHas been known for yearsHas been known for yearsFirst seen in pts treated with Steroids/ImuranFirst seen in pts treated with Steroids/ImuranPatients present off all IS with stable renal Patients present off all IS with stable renal
function, normal biopsy.function, normal biopsy.Cyclosporine seems to impair development of Cyclosporine seems to impair development of
tolerancetoleranceHas lead to research about T-Cell coreceptorsHas lead to research about T-Cell coreceptors

Tolerance Inducing Tolerance Inducing MechanismsMechanisms
T- Cell deletion in ThymusT- Cell deletion in ThymusThy – 1 cells lead to rejectionThy – 1 cells lead to rejection
Peripheral T- Cell deletionPeripheral T- Cell deletion IL-2 dependentIL-2 dependentFAS dependentFAS dependentVeto CellsVeto CellsSo immune system activation is required but So immune system activation is required but
apoptosis is favored over rejectionapoptosis is favored over rejection
Peripheral Non-deletional mechanismPeripheral Non-deletional mechanismAnergy – loss of response to antigenAnergy – loss of response to antigenThy 2 cells – regulatory/suppressor cellThy 2 cells – regulatory/suppressor cell

Tolerance in Practice TodayTolerance in Practice Today
For high PRA and Positive Crossmatch For high PRA and Positive Crossmatch pts:pts:IVIG/plasmapheresis before and after TXPIVIG/plasmapheresis before and after TXPLeads to decrease % Anti-donor antibodyLeads to decrease % Anti-donor antibodyAfter Txp, Antidonor Ab returns but does After Txp, Antidonor Ab returns but does
not lead to rejection not lead to rejection AnergyAnergyIncrease in Bcl - 2Increase in Bcl - 2

ToleranceTolerance
““Tolerogenic Immunosuppression”Tolerogenic Immunosuppression”Rapamicin, Tacrilimus seem to be OKRapamicin, Tacrilimus seem to be OKCyclosporine blocks tolerance pathwayCyclosporine blocks tolerance pathway
Starzl Lancet 2003Starzl Lancet 2003Sayegh Annals of Surgery 2003Sayegh Annals of Surgery 2003

Complications of TransplantComplications of Transplant
HypertensionHypertensionCorrelates with AgeCorrelates with AgeDiabetesDiabetesRaceRaceGraft FunctionGraft FunctionCNI useCNI useSteroidsSteroids
Graft Survival reduced if hypertension Graft Survival reduced if hypertension ++

Complications of TransplantComplications of Transplant
HypertensionHypertensionTarget SBP < 130Target SBP < 130Chronic Allograft NephropathyChronic Allograft Nephropathy
ProteinuriaProteinuriaTarget BP 125 / 75Target BP 125 / 75
Recommended Drugs:Recommended Drugs:B blockersB blockersACE inhibitorsACE inhibitorsCCB’s and diuretics as needed.CCB’s and diuretics as needed.

Complications of TransplantComplications of Transplant
New Onset Diabetes after Txp New Onset Diabetes after Txp NODATNODATDecrease steroids if possibleDecrease steroids if possibleConsider Change from TAC to CyA.Consider Change from TAC to CyA.
Cardiovascular Risk of a 25 y.o. Cardiovascular Risk of a 25 y.o. recipientrecipientEqual to the risk for a 55 y.o. without Equal to the risk for a 55 y.o. without
renal disease.renal disease.10 fold higher at any age!10 fold higher at any age!

Complications of TransplantComplications of Transplant
HyperlipidemiaHyperlipidemiaAssume CV risk is presentAssume CV risk is presentLDL target < 100LDL target < 100Consider decreasing SteroidsConsider decreasing SteroidsRecommend changing CyA or Rapa to TAC.Recommend changing CyA or Rapa to TAC.
Thrombin Activatable Fibrinolysis Thrombin Activatable Fibrinolysis InhibitorInhibitorTAFI levels are increased in Txp and DiabetesTAFI levels are increased in Txp and DiabetesIncrease risk of DVT, Unstable Angina.Increase risk of DVT, Unstable Angina.

Complications of TransplantComplications of Transplant
Post Transplant Bone DiseasePost Transplant Bone DiseaseOsteoporosis in 40- 60 % of ptsOsteoporosis in 40- 60 % of ptsBMD decreases 6-10 % per yearBMD decreases 6-10 % per yearFractures occurrence RateFractures occurrence Rate
Diabetics:Diabetics: 40-50 %40-50 %Non diabetics:Non diabetics: 10-15 %10-15 %
Contributing Factors:Contributing Factors:Renal osteodystrophy, ImmunosuppressivesRenal osteodystrophy, ImmunosuppressivesPTH, Age, Gender, Gonadal StatusPTH, Age, Gender, Gonadal Status

Complications of TransplantComplications of Transplant
Post Transplant Bone DiseasePost Transplant Bone DiseaseTreatmentTreatment
Calcium 1200 mg DailyCalcium 1200 mg DailyVit D 400 – 800 mcg dailyVit D 400 – 800 mcg dailyExercise, Tai ChiExercise, Tai ChiQuit smoking!Quit smoking!Fosamax 70 mg week or 5 mg daily for 6-12 Fosamax 70 mg week or 5 mg daily for 6-12
months.months.

Update in TransplantationUpdate in TransplantationSummarySummary
Trends in Survival after transplantTrends in Survival after transplantExpanded Donor KidneysExpanded Donor KidneysWaiting list Management changesWaiting list Management changesTrends in IS protocolsTrends in IS protocolsKidney Pancreas UpdateKidney Pancreas UpdateEthnic Disparities in TransplantsEthnic Disparities in Transplants Immunology and ToleranceImmunology and ToleranceNew approach to ComplicationsNew approach to Complications