Embed Size (px)
Citation preview

UPDATE IN PSYCHIATRY
Robert K. Schneider, MD
James L. Levenson, MD
Departments of Psychiatry and Medicine
The Medical College of Virginia at
the Virginia Commonwealth University
Richmond, Virginia

Annals: October 1999
Annals: March 2001
Annals: February 2002
Previous Updates

TOPICS COVERED –
• Mood Disorders
• Anxiety Disorders
• Medical-Psychiatric Interface
• Cognitive Disorders

MOOD DISORDERS

sertraline
Prozac
paroxetine
Celexa
fluoxetinePaxil
Zoloftcitalopram
Which SSRI is works best?

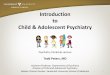
SSRIs Compared in Primary CareKroenke, JAMA 2001;286:2947
• Many claims of differences in efficacy
• ARTIST: – A Randomized Trial Investigating SSRI Treatment
• Aim: – Compare the effectiveness of 3 SSRIs in
depressed primary care patients.

SSRIs in Primary Care
• Methods– RCT of paroxetine, fluoxetine and sertraline
– 573 patients, in 2 primary care consortiums
• Main Findings– No statistical differences between the 3 SSRIs
in any of the outcomes.

0%
20%
40%
60%
80%
100%
Recovery Rate 84% 81% 77%
Completers 43% 41% 50%
Sertraline Paroxetine Fluoxetine

SSRIs in Primary Care
• Limitations– Therapy based on MD perception
– 74% met diagnostic criteria for major depression at baseline
– Low power for small differences
– No placebo control
– Mostly female (80%) and white (80%)
– No citalopram

Impact on clinical practice
• Efficacy not a basis for choosing SSRI
• Consider instead:– Comorbidities
– Half-life
– Side effects

Which came first, the depression or the erectile dysfuction?

Erectile Dysfunction and DepressionSeidman, Am J Psych 2001;158:1623
• Depression and erectile dysfunction occur often together in men, but the causal relationship is unclear.
• Aim: – Evaluate sildenafil in men with erectile
dysfunction and mild depression

Erectile Dysfunction and Depression
• Methods– RCT, double bind, placebo controlled
– Mild depression only
• Main Findings– All measures of sexual function improved
significantly more in the sildenafil group (p<.001).
– Treatment-responders (48/66 given sildenafil, 10/70 given placebo) had significant improvements in depression symptoms and quality of life compared to nonresponders

Erectile Dysfunction and Depression
• Limitations– ? generalizable to patients with major
depression or taking psychotropic medications
– 12 week trial

Impact on clinical practice
• Treating physical symptoms in patients with minor depression relieves depressive symptoms.– Erectile dysfunction
– Insomnia
– Pain

Is St. John’s wort an effective antidepresant?

St. John’s WortShelton, JAMA 2001; 285:1978
• Background:– Many controlled trials of St. John’s wort claim
efficacy for the treatment of depression, but they are methodologically flawed.
• Aim:– To compare the efficacy and safety of St.
John’s wort vs. placebo in major depression

St. John’s Wort
• Methods– RCT, double-blind, placebo-controlled
– 200 patients received either St. John’s wort or placebo for 8 weeks.
• Main Findings– No significant differences in any outcome
measures between the two groups
– St. John’s wort: 1% discontinued due to adverse effects

St. John’s Wort
• Limitations– Subjects had chronic depression (average
over 2 years)
– Subjects from tertiary care clinics

Impact on clinical practice
• St. Johns wort probably safe in minor depression
• Caution with interactions with other drugs – warfarin, cyclosporine, theophylline, digoxin,
protease inhibitors, anticonvulsants, oral contraceptives, triptans, SSRIs
• Not a good choice for severe depression

Is estrogen an antidepressant in menopausal women?

Estradiol for depression Novaes Soares, Arch Gen Psych 2001;58:529
• Depressive and somatic symptoms are common in women entering menopause.
• Studies of ERT for mood symptoms are complex and have shown mixed results. – Estrogen preparation: oral vs. transdermal
– Longitudinal measurements of estradial
– Endocrine confirmation of perimenopause: FSH
– Measurement of mood symptoms
– Placebo control difficult

Estradiol for depression
• Aim– Assess efficacy of transdermal ERT for treating
depression in perimenopausal women.
• Methods– RCT, double-blind, placebo-controlled
– FSH > 25 IU/L
– Depressive disorder (i.e. major depression, dysthymia or minor depression)
– 17β-estradiol (100μg) transdermal patches or placebo for 12 weeks and 4 week washout.

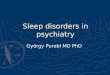
Estradiol for depression
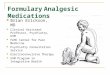
Main Findings– Remission of depressive symptoms in 68% vs. 20%
(P=0.001)
– no significant differences in response per type of depressive disorder
– 50% reduction in menopausal symptoms was seen in 68% vs. 28% (P=0.005).
Limitations– Small, short study in specialty clinic
– No progesterone

MADRSDepression
BKMIPerimenopausal
Symptoms
0
5
10
15
20
25
30
Baseline Week 4 Week 8 Week 12 Week 16
Estradiol
Placebo
0
5
10
15
20
25
Baseline Week 4 Week 8 Week 12 Week 16
Estradiol
Placebo

Impact on clinical practice
• Treatment with transdermal estrogen patches is effective for depressive symptoms in some perimenopausal women.
• This represents a good first step in treatment of the depressed perimenopausal women
• If symptoms persist or worsen, then consider the addition of an antidepressant

How often do depressed patients turn out to be bipolar?

Conversion from unipolar to bipolar depression Goldberg, Am J Psychiatry 2001;158:1265
• Background– Underdiagnosis of bipolar disorder
– 20% of Major Depression may be bipolar
– Prescription of antidepressants without mood stabilizers may precipitate a switch to mania

Unipolar to bipolar depression
• Aim– In patients presenting with depression,
what are the odds they will turn out to really be bipolar?
• Methods– Young (mean 23 years), hospitalized
patients with depression
– Followed prospectively for 15 years

Unipolar to bipolar depression • Main Findings
– 41% developed either hypomania or mania (26% hypomania, 15% mania).
– 80% of the 10 patients who were initially psychotic developed hypomania (4/10) or mania (4/10).
– 34% of the non-psychotically depressed eventually became either manic or hypomanic

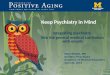
What’s the differnece between mania and hypomania? • Mania (Bipolar I):
– At least 7 days of racing thoughts, sleeplessness, grandiosity and sometimes psychosis
• Hypomania (Bipolar II)– At least 4 days of racing thoughts,
irritability, and sleeplessness

5-5 Stahl S M, Essential Psychopharmacology (2000)
DEPRESSION
NORMAL MOOD
MANIA
HYPOMANIA
MIXED EPISODE

Unipolar to bipolar depression
• Limitations– Started in the early 1980s
• psychiatric hospitalization differs
• treatments differ
– Psychiatric inpatients
– Naturalistic study and not a treatment intervention

Impact on clinical practice
• Younger patients with depression especially with psychotic features may be at a particularly high risk for conversion to bipolar depression.
• Remember that antidepressants may precipitate switch to mania.
• “Side Effects” to antidepressants may represent hypomania or mania
• Screen for mania/hypomania BEFORE starting an antidepressant

How good is the care given for depression and anxiety disorders?

Quality of Care for Depression and Anxiety Disorders Young, Arch Gen Psych 2001;58:55
• Depressive and anxiety disorders are common, and cause substantial disability.
• Medications and psychotherapies have empirically demonstrated efficacy
• BUT many patients do not receive adequate treatment

Quality of Care
• Aim– To estimate the rate of appropriate treatment
of anxiety and depressive disorders
– Measure effects of insurance, provider type, and demographics
• Methods– One year of data, from the National
Comorbidity Survey (1997-98)

Quality of Care One year, adults, major anxiety or depression
• Main Findings:– 83% saw a health care provider
– 30% received some appropriate treatment
– Most only saw PCP’s; 19% received appropriate care.
– 90% visiting MH professionals received appropriate care.
– Insurance status affected whether the individual saw a provider, but had no effect on whether appropriate care was received.

Quality of CareOne year, adults, major anxiety or depression
• Main Findings:– Appropriate treatment was less likely for
• men
• blacks
• the less educated
• those <30 or >59 years old
– When a psychiatric medication was used, it was at an appropriate dose and duration in about 75% of the individuals.

Quality of Care
• Main Findings:– For patients seeing PCPs, those who received
poor quality care were less likely to report that…
• their mental health problems were evaluated
• psychiatric drugs were recommended
• referral to a mental health specialist was made
– Patients who received poor quality care were less likely to view themselves as needing mental health care (31.4% vs. 70%)

Impact on clinical practice• Limitations
– Self report data, response rates
• Conclusions– Most adults with depression or anxiety disorders did
not receive appropriate treatment, though they saw health care providers
– When given, psychiatric medications were usually given at appropriate dosage and duration.
– The current barriers to appropriate treatment lie in recognition, diagnosis, referral, and acceptance by patients.

ANXIETY DISORDERS

What are the psychiatric consequences of a terrorist disaster?
“The most severe incident of terrorism ever experienced on American
soil.”

Psychiatric Disorders Among Survivors of the Oklahoma City Bombing North, JAMA 1999; 282:755
• Sometimes difficult to distinguish normal from pathological reactions
• Aim– Assess the psychiatric impact on adult survivors
directly exposed to the bomb blast.

Oklahoma City Bombing• Methods
– Single diagnostic interview
• Main Findings– 87% reported injuries
– Predisaster (lifetime) prevalence vs postdisaster prevalence:
• PTSD [15% vs. 34%]
• Major Depression [12.6% vs. 22.5%]

Oklahoma City Bombing
• Main Findings:– Postdisaster, 74% of PTSD and 56% of
major depression was new.
– Conversely, 71% of those with no predisaster psychiatric diagnosis remained without a postdisaster diagnosis

Oklahoma City Bombing
• Main Findings:– Over 80% of the survivors had intrusive
reexperiences or hyperarousal symptoms.
– Only 34% of survivors had all three criteria (including avoidance) for PTSD.
– Avoidance/numbing criterion was 100% sensitive for detecting PTSD.

Oklahoma City Bombing
• Limitations– Retrospective; direct exposure only
• Conclusions– PTSD and Major Depression were the major
psychiatric disorders
– Hyperarousal and reexperiences common
– Avoidance/numbing screens for full PTSD

Impact on clinical practice• Health predicts health
• Terror trauma uncommon,
sudden death of a loved one is not
• PTSD is very treatable– Medications
– Psychotherapy


What’s the best initial drug treatment for panic disorder?

Early Coadministration of Benzodiazepines and SSRIs Goddard, Arch Gen Psych 2001;58:681
• SSRIs are indicated for all anxiety disorders
• But response to SSRIs is delayed
• Psychiatrists often start benzodiazepines with SSRIs, but few controlled trials

Short vs. Longer Acting Benzodiazepines• Short acting benzodiazepine (alprazolam) seems
like a good choice (rapid onset of action) – BUT is bad (rebound anxiety, euphoria, difficult to taper)
• Clonazepam is a intermediate half-life benzodiazepine with a slower onset of action– Early symptom reduction without euphoria
– Easily tapered
– Also, few active metabolites

Early Benzodiazepinesand SSRIs • Aim
– Test the efficacy of early coadministration of clonazepam and sertraline in panic disorder
• Methods– 12 week, RCT
– Open-label sertraline
– Blinded to clonazepam 0.5mg TID or placebo
– Three week clonazepam taper at week 4

Early Benzodiazepinesand SSRIs• Main Findings:
– Response rates:• Week one (41% vs. 4%)
• Week three (63% vs. 32%)
– At end of trial, both groups’ response rates were over 70%.
– No differences in secondary measures between groups (i.e. drop out rates, adverse reactions).

Early Benzodiazepinesand SSRIs• Limitations
– Small group size
– 100 mg of sertraline may be more than needed
– May titrate slower
• Conclusions– Rapid stabilization of panic disorder can be
achieved with early coadministration of sertraline and clonazepam

Impact on clinical practice
• Panic disorder is common in the primary care setting.
• A common practice used by psychiatrists that could easily be used by non-psychiatrists in the early treatment of panic disorder.
• Intermediate-acting benzos have advantages over short-acting ones

MEDICAL-PSYCHIATRIC
INTERFACE

Can medication-induced depression be prevented?

Interferon and Treatment of Depression Musselman, N Engl J Med 2001; 344:961
• Background– Depression is the most frequent adverse effect
leading to discontinuation of interferon
– Interferons are important in the treatment of: hepatitis C, multiple sclerosis, and malignancies
– Antidepressants effective in treating interferon-induced depression

Interferon and Depression
• Aim– Will pretreatment with antidepressants reduce
depressive symptoms following interferon?
• Methods– RCT, placebo controlled
– 2 week pretreatment with paroxetine before interferon alpha for malignant melanoma

Interferon and Depression
• Major findings: – Major depression (paroxetine vs. placebo):
11% vs. 45%
– Severe depression led to discontinuation of interferon (paroxetine vs. placebo):
5% vs. 35%
– In the placebo group, if major depression,
then 78% discontinued interferon

Interferon and Depression
• Conclusions– Pretreatment with paroxetine appears
effective in preventing depression induced by interferon alfa in malignant melanoma
• Limitations– Generalizable to other interferons and
diseases?

Impact on clinical practice• Vital drugs may cause depression
e.g.interferons, steroids, betablockers, isotretinoin
• When it is not possible to substitute an alternative medication, then:– try treating the drug-induced depression with
antidepressants
– consider prevention before administering the drug

What’s the risk of sudden cardiac death with antipsychotics?

Antipsychotics and QTc Prolongation Ray, Arch Gen Psych 2001;58:1161
• Background– Case reports have linked antipsychotic drugs with:
QTc prolongation, torsades de pointes, and sudden deaths
– “Black box” warnings regarding these risks added to PDR for the older antipsychotics thioridazine and mesoridazine
– Sertindole (new antipsychotic), was not registered in the U.S. because it caused QTc prolongation and sudden
death

Antipsychotics and QTc
• Aim:
To determine the risk of sudden cardiac death in antipsychotic users.
• Methods:
Retrospective cohort study of Tennessee Medicaid enrollees

Antipsychotics and QTc
• Main Findings:Corrected Risk Ratios:
– Moderate-dose antipsychotic use vs. nonuse: 2.39
– Low-dose antipsychotic use vs. nonuse: 1.30
– Moderate-dose antipsychotic use vs. nonuse in patients with severe cardiovascular disease : 3.53

Antipsychotics and QTc • Limitations
– Cannot determine causality
– Era before atypical antipsychotics
– Smoking and obesity not controlled for
– Sudden Death may be first symptom of CAD
• Conclusions– Relative and absolute increases in the risk of
sudden death in patients taking moderate doses of antipsychotics

Impact on clinical practice
• If prescribing an antipsychotic, take a careful history for syncope or family history of sudden death
• Patients at high risk should have pretreatment EKG and receive antipsychotics not shown to increase QTc
(olanzapine, risperidone, quetiapine)

Does group therapy prolong life in metastatic breast cancer?

Group Therapy and Breast CancerGoodwin, N Engl J Med. 2001;345:1719
• Background
Group therapy has been reported to provide benefits for metastatic breast cancer, including improvement in mood, pain control, and in some but not all studies, survival.

Group Rx and Breast Cancer
• Aim– To assess whether group therapy influences
survival, mood, and pain in women with metastatic breast cancer
• Methods– Multi-center randomized trial of supportive-
expressive group therapy
– Group therapy consisted of weekly 90-minute sessions for at least one year
– All received routine care

Group Rx and Breast Cancer
• Main Findings:– Greater improvements in psychological symptoms and
pain control (p=0.04) in the intervention group
– These benefits occurred in those women who were more distressed at baseline.
– Did not prolong survival compared to routine care alone (17.9 vs. 17.6 months)
• Limitations– Only 9% of eligible women were randomly assigned

Impact on clinical practice• Conclusions
– Many support groups are available
– Some women do not want to participate
– But increased survival is “proven” so they may feel obligated to join
– Patient can be reassured that groups improve pain control and mood but do not prolong survival

COGNITIVE DISORDERS

Does cognitive function decline after CABG?

Cognition after CABG Newman, N Eng J Med 2001;344:395
• Background– Perioperative cognitive decline after CABG
appears to be greatest at discharge.
– Cognition gradually improves for most patients over next 6 months.
– But a significant number (10-30%) continue to
decline
• Aim– To prospectively assess cognitive functioning
before and after CABG for five years

Cognition after CABG• Methods
– Neurocognitive testing was performed before surgery, at discharge, 6 weeks, 6 months and 5 years after CABG
• Main Findings– Incidence of cognitive decline:
• 53% at discharge
• 36% at six weeks
• 24% at six months
• 42% at five years

Cognition after CABG
• Main Findings (cont)– Most returned to baseline functioning
within 6 months.
– However, at 5 years, the patients with cognitive decline at discharge had a marked decline from their baseline functioning (P<0.001); the patients without cognitive decline at discharge did not.

Cognition after CABG• Limitations
– Selective attrition may underestimate cognitive decline
• One third of sample not available for long term followup were more likely to have had complex disease
– Some cognitive decline due to illness not CABG
• Conclusions– Patients with cognitive decline immediately after
elective CABG are at increased risk for long-term cognitive decline

Impact on clinical practice• Prior to elective CABG, the potential for
cognitive decline should be discussed :– Cognitive decline is common
– Most improve over the first six months
– But a significant number will have impairment at five years post-operatively
– This is one quality of life factor among others• Especially important in the elderly

Is there a quick way to screen for dementia?

Mini Cog: New, Easy-to-use Screening Test for Dementia Scanlan, Int J Geriatr Psych 2001;16:216 Borson, Int J Geriatr Psych 2000;15:1021
Background
• Screening for cognitive disorders has usually been with the Mini Mental Status Exam (MMSE). – Hard to remember and time consuming.
– Research tool NOT a screening tool

Mini Cog Screen for Dementia
• Background (cont)The Mini-Cog has just:
the 3-item recall from the MMSE
the Clock Drawing Test (CDT)Requests the subject to fill in the numbers on a predrawn circle and then add the hands for a designated time.
• Aim– To evaluate the Mini-Cog at case-finding for
cognitively impaired adults.

Mini Cog Screen for Dementia
• Methods– Community dwelling subjects, seen at a
university memory clinic
– Completed the MMSE, CASI (Cognitive Abilities Screening Instrument), and the Mini-Cog.
– Expert raters performed the MMSE and CASI and “naïve” raters performed the Mini-Cog.

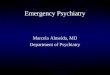
Mini Cog Screen for Dementia
SENSITIVITY SPECIFICITY
MMSE 91% 92%
CASI 92% 96%
MINI-COG 99% 93%

Mini Cog Screen for Dementia
• Main Findings– Concordance between naïve and trained raters
was >98% for normal, moderately and severely impaired clock drawings.
– Concordance dropped to 60% in mildly impaired clock drawings
• But assuming naive raters would score mildly impaired clocks as normal
• Then the Mini-Cog sensitivity and specificity changed little (97% and 95%).

Mini Cog Screen for Dementia
• Conclusions– The Mini-Cog is a time-efficient, sensitive and specific
tool that effectively identifies patients with probable dementia, even by naïve raters.
• Limitations– Conducted in a university memory clinic
– The population screened by an internist would have a lower incidence of dementia, increasing false positives and lowering specificity.

Impact on clinical practice• The Mini-Cog provides an effective first-stage
screening tool for detecting dementia.
• Trained staff (naïve raters) could easily perform this in an office setting.
• Combining this first-stage screening with a second stage caregiver brief interview probably represents an efficient and effective system for screening for cognitive impairment in the elderly.