Embed Size (px)
Citation preview

Update in COPDUpdate in COPD
Prescott G. Woodruff, MD, MPHPrescott G. Woodruff, MD, MPHAssociate Professor of MedicineAssociate Professor of Medicine
UCSFUCSFDivision of Pulmonary and Critical CareDivision of Pulmonary and Critical Care
Faculty DisclosuresFaculty Disclosures
Personal financial interests in commercial entities thatPersonal financial interests in commercial entities thatare relevant to my presentation(s) or other faculty roles:are relevant to my presentation(s) or other faculty roles:
Prescott Woodruff, MD, MPH
Genentech, Research Grant (completed), Co-inventor on patent applicationRegulus, Unfunded research collaboration (reagents)Pfizer, CTI Strategic AllianceMedImmune, Consultant (completed)
Burden of disease: Understand the need for early recognition, prevention, and treatment of COPD
COPD diagnosis: Importance of spirometry, symptom and exacerbation assessment
Current treatment options: Review current GOLD guidelines Recent Advances: azithromycin for the prevention ofexacerbations
The Future of COPD: Phenotyping in COPD
ObjectivesObjectives

••Chronic BronchitisChronic Bronchitis
••EmphysemaEmphysema
••Chronic Airflow limitationChronic Airflow limitation
COPD: Breadth of the DefinitionCOPD: Breadth of the Definition
GOLD Consensus Report, December 2011
“COPD, a common preventable and treatabledisease is characterized by persistent airflow limitation..”
“Airflow limitation is usually progressive and is associatedassociatedwith an enhanced chronic inflammatorywith an enhanced chronic inflammatoryresponseresponse in the airways and the lung to noxious particlesor gases.”
“Exacerbations and comorbidities Exacerbations and comorbidities contribute tothe overall severity in individual patients.”
COPD: Preventable and TreatableCOPD: Preventable and Treatable
COPD is a Major Public Health ProblemCOPD is a Major Public Health Problem
16.3 million office visits each year due to COPD16.3 million office visits each year due to COPD11
672,000 hospitalizations each year for COPD672,000 hospitalizations each year for COPD22
•• 21% mortality rate at one year after being hospitalized21% mortality rate at one year after being hospitalizedfor a COPD exacerbation in a large VA cohortfor a COPD exacerbation in a large VA cohort33
COPD is currently the 3rd-leading cause of death in theCOPD is currently the 3rd-leading cause of death in theUnited StatesUnited States44
Total costs for COPD estimated at $49.9 billion in 2007Total costs for COPD estimated at $49.9 billion in 2007
1. National Institutes of Health, National Heart, Lung & Blood Institute. Morbidity and Mortality: 2009 chart book on cardiovascular, lung andblood diseases. www.nhlbi.nih.gov/resources/docs/cht-book.htm. Accessed September 13, 2010.
2. American Lung Association. Trends in chronic bronchitis and emphysema: morbidity and mortality. February 2010. www.lungusa.org.Accessed September 13, 2010.
3. McGhan R, et al. Chest. 2007;132:1748-1755.4. WHO. Chronic respiratory diseases. 2011. http://ww.who.int/respiratory/copd/burden/gn. Accessed July 2, 2011.5. American Lung Association. Trends in chronic bronchitis and emphysema: morbidity and mortality. February 2010. www.lungusa.org
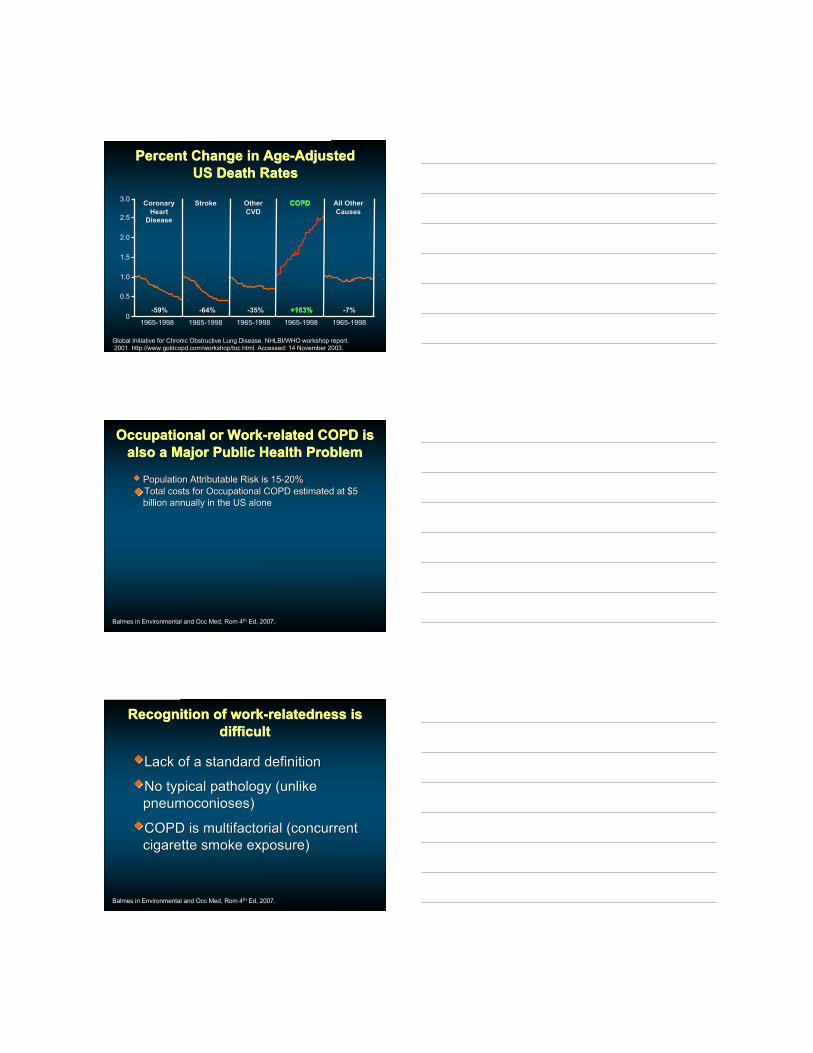
Percent Change in Age-AdjustedPercent Change in Age-AdjustedUS Death RatesUS Death Rates
3.0
2.5
2.0
1.5
1.0
0.5
01965-1998 1965-1998 1965-1998 1965-1998 1965-1998
CoronaryCoronaryHeartHeart
DiseaseDisease
StrokeStroke OtherOtherCVDCVD
All OtherAll OtherCausesCauses
-64%-64%-59%-59% -35%-35% -7%-7%
COPDCOPD
+163%+163%
Global Initiative for Chronic Obstructive Lung Disease. NHLBI/WHO workshop report. 2001. http://www.goldcopd.com/workshop/toc.html. Accessed: 14 November 2003.
Occupational or Work-related COPD isOccupational or Work-related COPD isalso a Major Public Health Problemalso a Major Public Health Problem
Population Attributable Risk is 15-20%Population Attributable Risk is 15-20%
Total costs for Occupational COPD estimated at $5Total costs for Occupational COPD estimated at $5billion annually in the US alonebillion annually in the US alone
Balmes in Environmental and Occ Med, Rom 4Balmes in Environmental and Occ Med, Rom 4thth Ed, 2007. Ed, 2007.
Recognition of work-relatedness isRecognition of work-relatedness isdifficultdifficult
Lack of a standard definitionLack of a standard definition
No typical pathology (unlikeNo typical pathology (unlikepneumoconioses)pneumoconioses)
COPD is multifactorial (concurrentCOPD is multifactorial (concurrentcigarette smoke exposure)cigarette smoke exposure)
Balmes in Environmental and Occ Med, Rom 4Balmes in Environmental and Occ Med, Rom 4thth Ed, 2007. Ed, 2007.

COPD: GeneralCOPD: GeneralRisk FactorsRisk Factors
Tager et al. Tager et al. Am Rev Respir DisAm Rev Respir Dis. 1988;138:837-849; Holt. . 1988;138:837-849; Holt. ThoraxThorax. 1987;42:241-249.. 1987;42:241-249.
EstablishedEstablished ProbableProbable PossiblePossible Cigarette smokingCigarette smoking
OccupationalOccupationalexposureexposure
αα11-Antitrypsin-Antitrypsindeficiency (geneticdeficiency (geneticabnormality)abnormality)
Air pollutionAir pollution
Exposure to primaryExposure to primaryand secondaryand secondarysmokesmoke
Hyperactive airwaysHyperactive airways
AlcoholAlcohol
PovertyPoverty
Low birth weightLow birth weight
ChildhoodChildhoodrespiratory infectionsrespiratory infections
Family historyFamily history
AtopyAtopy
IgA deficiencyIgA deficiency
Blood type ABlood type A
COPD: Occupational Risk FactorsCOPD: Occupational Risk Factorsfor Chronic Bronchitisfor Chronic Bronchitis
Balmes in Environmental and Occ Med, Rom 4Balmes in Environmental and Occ Med, Rom 4thth Ed, 2007. Ed, 2007.
MineralsMinerals MetalsMetals GasesGases CoalCoal
Vitreous fibersVitreous fibers
Oil mistOil mist
Portland cementPortland cement
Silica/silicatesSilica/silicates
OsmiumOsmium
VanadiumVanadium
Welding fumesWelding fumes
Organic DustOrganic Dust•• CottonCotton
•• GrainGrain
•• WoodWood
DiisocyanateDiisocyanate
Sulfur dioxideSulfur dioxide
SmokeSmoke•• Engine exhaustEngine exhaust
•• FiresFires
COPD: Occupational Risk FactorsCOPD: Occupational Risk Factorsfor Emphysemafor Emphysema
Balmes in Environmental and Occ Med, Rom 4Balmes in Environmental and Occ Med, Rom 4thth Ed, 2007. Ed, 2007.
Much harder to measure, data from autopsy studiesMuch harder to measure, data from autopsy studies Gold minersGold miners
Silica exposureSilica exposure
Coal dustCoal dust
COPD: Occupational Risk FactorsCOPD: Occupational Risk Factorsfor Decline in FEV1for Decline in FEV1
Balmes in Environmental and Occ Med, Rom 4Balmes in Environmental and Occ Med, Rom 4thth Ed, 2007. Ed, 2007.
Much harder to specify the cause, Population basedMuch harder to specify the cause, Population basedstudiesstudies MiscellaneousMiscellaneous
exposures to dustexposures to dustand gasesand gases
Burden of disease: Understand the need for early recognition, prevention, and treatment of COPD
COPD diagnosis: Importance of spirometry, symptom and exacerbation assessment
Current treatment options: Review current GOLD guidelines Recent Advances: azithromycin for the prevention ofexacerbations
The Future of COPD: Phenotyping in COPD
ObjectivesObjectives
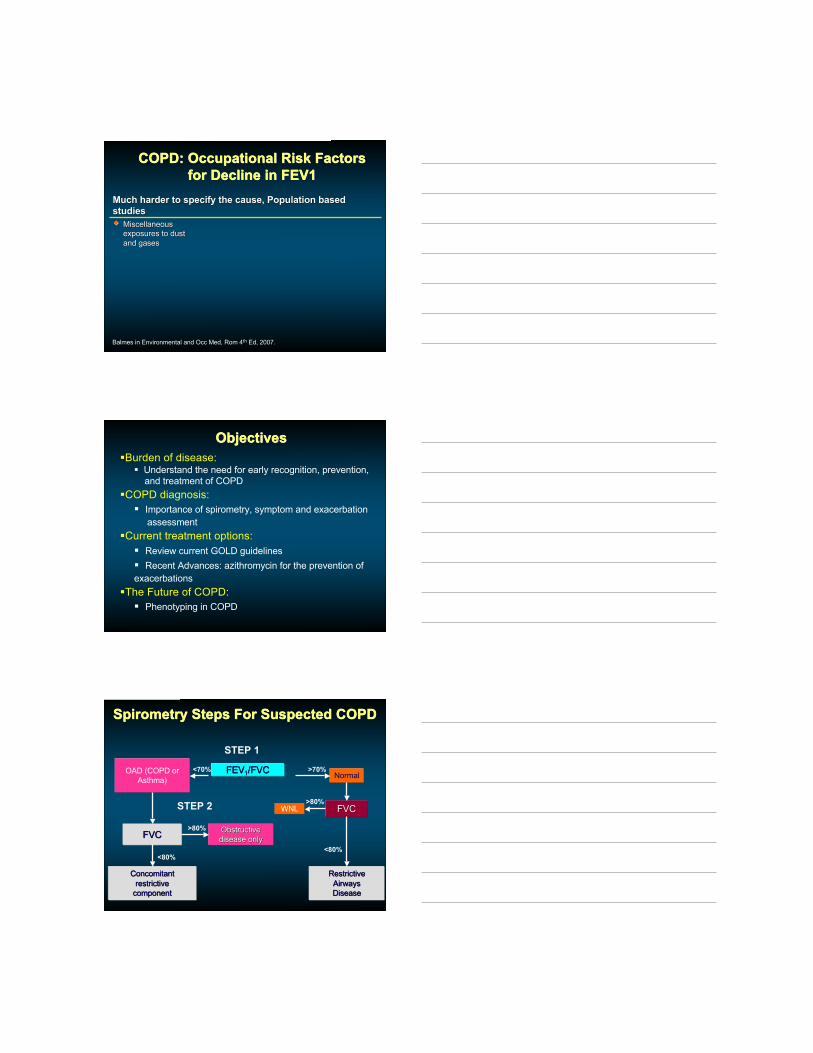
Spirometry Steps For Suspected COPDSpirometry Steps For Suspected COPD
FEVFEV11/FVC/FVCOAD (COPD orAsthma)
<70% >70%Normal
FVCFVC
STEP 1
STEP 2
>80%
ConcomitantConcomitantrestrictiverestrictive
componentcomponent
<80%
ObstructiveObstructivedisease onlydisease only
FVCFVC
RestrictiveRestrictiveAirwaysAirwaysDiseaseDisease
<80%
>80%WNL

Adapted from Fletcher et al. BMJ. 1977;1:1645-1648.
Disease must be detectable in an early stage:Disease must be detectable in an early stage:Lung Function Over TimeLung Function Over Time
FEV
FEV 11
(%) R
elat
ive
to A
ge 2
5 (%
) Rel
ativ
e to
Age
25
Never smoked or notsusceptible to smoke
StoppedSmoking at 45(Mild COPD)
Stoppedsmoking at 65(Severe COPD)Death
Disability
Smoked regularlyand susceptibleto its effects
Age (Years)5050 7575252500
Symptoms
00
2020
5050
6060
100100
8080
4040
Mannino et al. MMWR Morb Mortal Wkly Rep. 2002;51:1-16.
0
50
100
150
200
250
300
350
400
450Diagnosed with chronic bronchitis or emphysema
Airflow limitation (GOLD 1 or higher)
Rat
e pe
r 100
0 of
Pop
ulat
ion
25-44 45-54 55-64 65-74 >/=75Age (years)
Underdiagnosis of COPD in the United States Underdiagnosis of COPD in the United States
7.2%
14%
20.7%
22.9%
The Argument for Selective ScreeningThe Argument for Selective Screening
Martinez, et al., COPD, 2008;5:85. “COPD Screener”

Symptoms in COPDSymptoms in COPD
Exacerbation Frequency Increases WithExacerbation Frequency Increases WithDisease SeverityDisease Severity
1.6
1.9
2.3
0
0.5
1
1.5
2
2.5
>60% 40%-59% <40%
% Predicted FEV 1
Exa
cerb
atio
ns P
er Y
ear
Miravitlles M, et al. Respir Med. 1999;93:173-179.
Exacerbation was defined as an increase in dyspnea, sputum volume, and/or sputum purulence.
Results based on a cross-sectional observational study of ambulatory COPD patients in Spain.General practitioners (N=201) between October 1994 and May 1995 completed a questionnaire onCOPD characteristics of 1001 patients.
-50
-40
-30
-20
-10
0
FEV 1
, mL/
year
<1.5 >1.5Exacerbations Per Year
Frequency of Exacerbations Is AssociatedFrequency of Exacerbations Is AssociatedWith a Decline in Lung FunctionWith a Decline in Lung Function
Results based on a secondary analysis of 32 patients who recorded daily FEV1. The median rate of exacerbationsseen at clinic was 1.5 per patient per year.Donaldson GC, et al. Thorax. 2002;57:847-852.
*P<0.001 -46.1
-25.3*

Patients With Frequent Exacerbations HadPatients With Frequent Exacerbations HadSignificantly Worse Quality of LifeSignificantly Worse Quality of Life
48.953.2
67.7
36.3
64.1
77.080.9
50.4
0
10
20
30
40
50
60
70
80
90
100
Total Symptoms Activities Impacts
SGR
Q S
core
Seemungal T, et al. Am J Respir Crit Care Med. 1998;157:1418-1422. Used with permission from OFFICIAL JOURNALOF THE AMERICAN THORACIC SOCIETY. © AMERICAN THORACIC SOCIETY.
Mean Difference:-15.1*
Mean Difference:-21.9*
Mean Difference:-12.2*
Mean Difference:-14.1*
0-2 Exacerbations
3-8 Exacerbations
*P≤0.002
Burden of disease: Understand the need for early recognition, prevention, and treatment of COPD
COPD diagnosis: Importance of spirometry, symptom and exacerbation assessment
Current treatment options: Review current GOLD guidelines Recent Advances: azithromycin for the prevention ofexacerbations
The Future of COPD: Phenotyping in COPD
ObjectivesObjectives
Treatment of Occupational COPDTreatment of Occupational COPD
PreventionPrevention
•Primary (reduce exposure to irritants)•Elimination•Engineering controls•Administrative controls•Personal protective equipment
•Secondary (screening with questionnaires andspirometry)
•“Tertiary” (the therapeutic options that will beindicated on the subsequent slides)

Treatment of COPD in GeneralTreatment of COPD in GeneralGOLD 2011 Consensus StatementGOLD 2011 Consensus Statement
Goal of the Combined COPD Assessment is toGoal of the Combined COPD Assessment is tostratify subjects based onstratify subjects based on–– Risk for exacerbations, hospitalizations and deathRisk for exacerbations, hospitalizations and death–– SymptomsSymptoms
Metrics used to stratifyMetrics used to stratify–– FEV1% predictedFEV1% predicted–– Exacerbation historyExacerbation history–– Symptoms using either the modified MedicalSymptoms using either the modified Medical
Research Council (mMRC) dyspnea score or theResearch Council (mMRC) dyspnea score or theCOPD Assessment Test (CAT) scoreCOPD Assessment Test (CAT) score
2011 GOLD Consensus Report www.goldcopd.com
Classification of Airflow LimitationClassification of Airflow Limitation
In patients with FEV1/FVC <0.70
GOLD I Mild FEV1 ≥ 80% predicted
GOLD II Moderate 50% ≤ FEV1 < 80% predicted
GOLD III Severe 30% ≤ FEV1 < 50% predicted
GOLD IV Very Severe FEV1 < 30% predicted
Modified Medical Research CouncilModified Medical Research CouncilQuestionnaire for AssessingQuestionnaire for Assessing
BreathlessnessBreathlessnessGrade 0 I only get breathless with strenuous exercise
Grade 1 I get short of breath when hurrying on the level or walkingup a slight hill
Grade 2 I walk slower than people of the same age on the levelbecause of breathlessness, or I have to stop for breathwhen walking on my own pace on the level
Grade 3 I stop for breath after walking about 100 m or after a fewminutes on the level
Grade 4 I am too breathless to leave the house or I am breathlesswhen dressing or undressing
CAT: COPD Assessment TestCAT: COPD Assessment Test
http://www.catestonline.org/images/pdfs/CATest.pdf
GOLD 2011 Consensus StatementGOLD 2011 Consensus Statement !!!!
!!
! ! ! ! ! ! !
!
! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! !
!
!!!
! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !
! ! ! ! ! ! ! ! ! ! !! ! ! ! ! ! ! ! ! ! !!
!"#$!
"#$%&
!'()**+,+-).+/
0!/,! %
"&'()
*+,"-
"./.")01
2!3!
4
!!5
123 143
!"#$!
"67)-89:).+/0!;+*./9<1
+1%3 153
=>?'!5 @4 'AB!C!45!
D
E
3
4
!!
=>?'! 2!3 'AB!2!45!
67-8.)-#
"=>?'!/9!'AB!*-/98 1
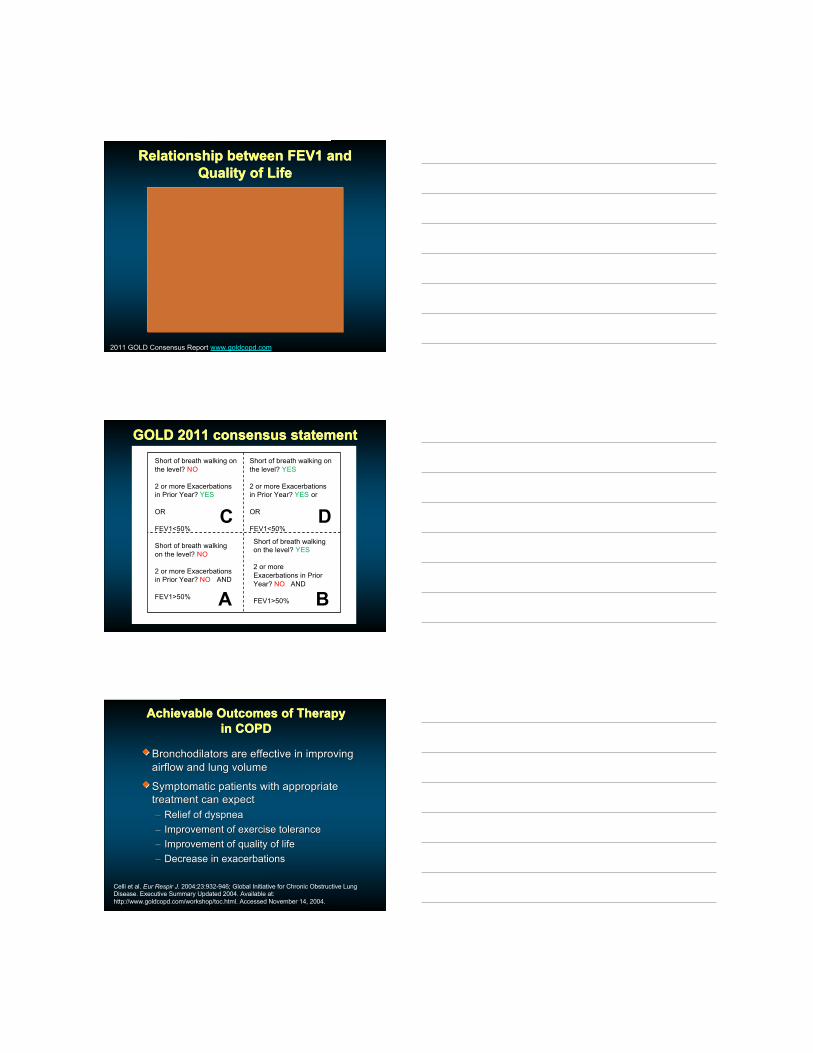
FEVFEV11 and Risk for Exacerbations, and Risk for Exacerbations,Hospitalization and DeathHospitalization and Death
Combined placebo data from TORCH, Uplift andCombined placebo data from TORCH, Uplift andECLIPSEECLIPSE
GOLDspirometric
level
Exacerbations /year
Hospitalizations/ year
3-year mortality
GOLD I - - -
GOLD II 0.7 – 0.9 0.11 – 0.2 11%
GOLD III 1.1 – 1.3 0.25 – 0.3 15%
GOLD IV 1.2 – 2.0 0.4 – 0.54 24%
2011 GOLD Consensus Report www.goldcopd.com
Relationship between FEV1 andRelationship between FEV1 andQuality of LifeQuality of Life
2011 GOLD Consensus Report www.goldcopd.com
GOLD 2011 consensus statementGOLD 2011 consensus statementShort of breath walking onthe level? NO
2 or more Exacerbationsin Prior Year? YES
OR
FEV1<50%
Short of breath walking onthe level? YES
2 or more Exacerbationsin Prior Year? YES or
OR
FEV1<50%
Short of breath walkingon the level? NO
2 or more Exacerbationsin Prior Year? NO AND
FEV1>50%
Short of breath walkingon the level? YES
2 or moreExacerbations in PriorYear? NO AND
FEV1>50%A B
C D
Achievable Outcomes of TherapyAchievable Outcomes of Therapyin COPDin COPD
Bronchodilators are effective in improvingBronchodilators are effective in improvingairflow and lung volumeairflow and lung volume
Symptomatic patients with appropriateSymptomatic patients with appropriatetreatment can expecttreatment can expect–– Relief of dyspneaRelief of dyspnea–– Improvement of exercise toleranceImprovement of exercise tolerance–– Improvement of quality of lifeImprovement of quality of life–– Decrease in exacerbationsDecrease in exacerbations
Celli et al. Eur Respir J. 2004;23:932-946; Global Initiative for Chronic Obstructive LungDisease. Executive Summary Updated 2004. Available at:http://www.goldcopd.com/workshop/toc.html. Accessed November 14, 2004.
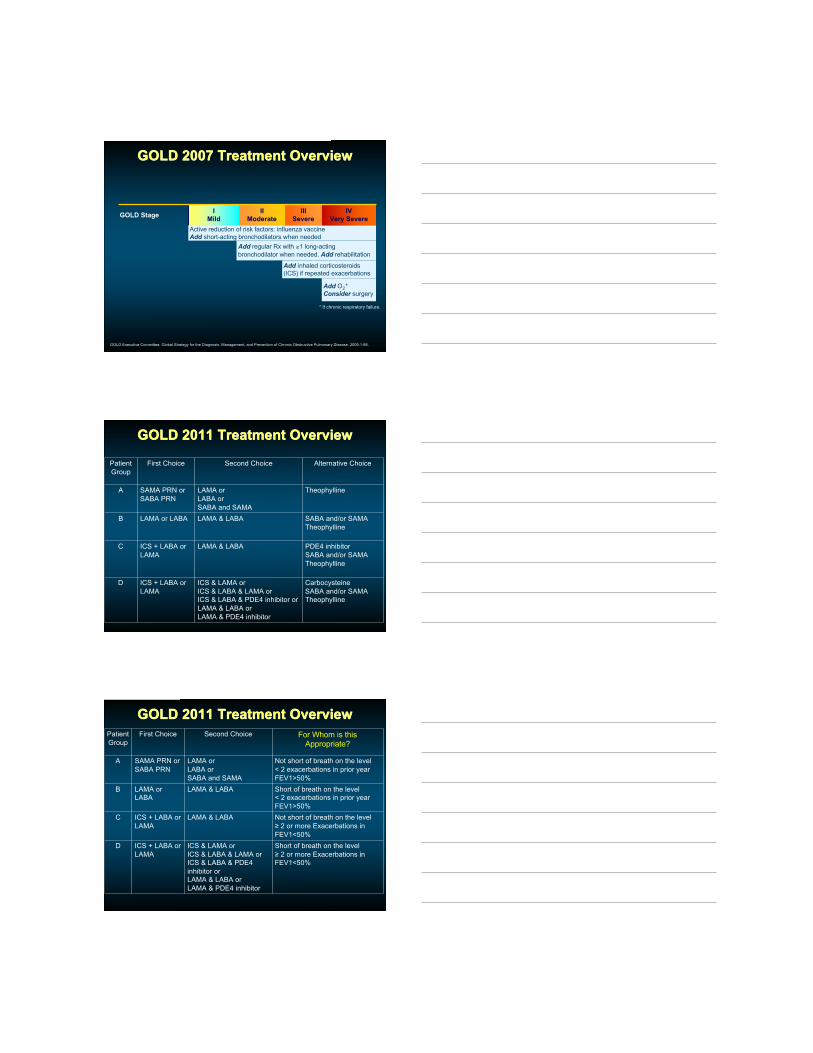
GOLD 2007 Treatment OverviewGOLD 2007 Treatment Overview
GOLD Stage IMild
IIModerate
IIISevere
IVVery Severe
Active reduction of risk factors: influenza vaccineAdd short-acting bronchodilators when needed
Add regular Rx with ≥1 long-actingbronchodilator when needed. Add rehabilitation
Add inhaled corticosteroids(ICS) if repeated exacerbations
Add O2*Consider surgery
GOLD Executive Committee. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2006:1-88.
* If chronic respiratory failure.
GOLD 2011 Treatment OverviewGOLD 2011 Treatment Overview
PatientGroup
First Choice Second Choice Alternative Choice
A SAMA PRN orSABA PRN
LAMA orLABA orSABA and SAMA
Theophylline
B LAMA or LABA LAMA & LABA SABA and/or SAMATheophylline
C ICS + LABA orLAMA
LAMA & LABA PDE4 inhibitorSABA and/or SAMATheophylline
D ICS + LABA orLAMA
ICS & LAMA orICS & LABA & LAMA orICS & LABA & PDE4 inhibitor orLAMA & LABA orLAMA & PDE4 inhibitor
CarbocysteineSABA and/or SAMATheophylline
GOLD 2011 Treatment OverviewGOLD 2011 Treatment OverviewPatientGroup
First Choice Second Choice For Whom is thisAppropriate?
A SAMA PRN orSABA PRN
LAMA orLABA orSABA and SAMA
Not short of breath on the level< 2 exacerbations in prior yearFEV1>50%
B LAMA orLABA
LAMA & LABA Short of breath on the level< 2 exacerbations in prior yearFEV1>50%
C ICS + LABA orLAMA
LAMA & LABA Not short of breath on the level≥ 2 or more Exacerbations inFEV1<50%
D ICS + LABA orLAMA
ICS & LAMA orICS & LABA & LAMA orICS & LABA & PDE4inhibitor orLAMA & LABA orLAMA & PDE4 inhibitor
Short of breath on the level≥ 2 or more Exacerbations inFEV1<50%
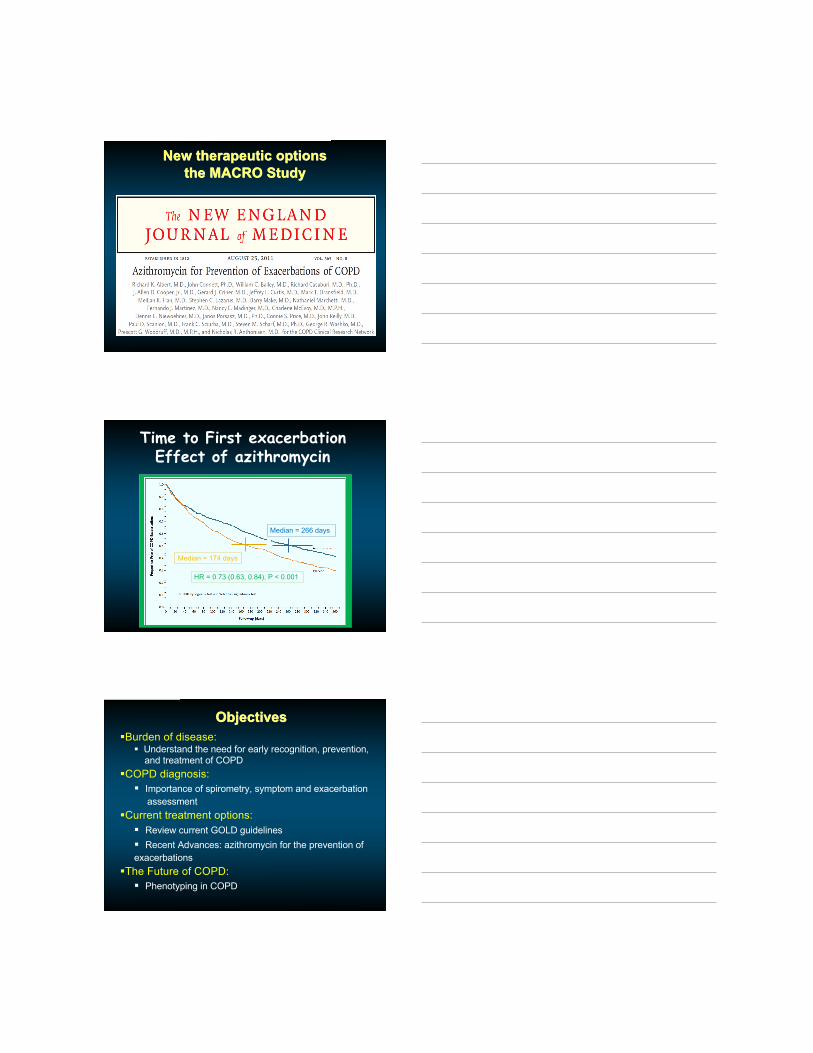
New therapeutic optionsNew therapeutic optionsthe MACRO Studythe MACRO Study
Time to First exacerbationEffect of azithromycin
Median = 174 days
Median = 266 days
HR = 0.73 (0.63, 0.84), P < 0.001
Burden of disease: Understand the need for early recognition, prevention, and treatment of COPD
COPD diagnosis: Importance of spirometry, symptom and exacerbation assessment
Current treatment options: Review current GOLD guidelines Recent Advances: azithromycin for the prevention ofexacerbations
The Future of COPD: Phenotyping in COPD
ObjectivesObjectives

Future DirectionsFuture Directions
Future DirectionsFuture Directions
“Emphysema Predominant” “Airway Disease Predominant”
Future DirectionsFuture Directions
Han, et al. Radiology 2011;261(1):274
SummarySummary
Occupational COPD represents a significantOccupational COPD represents a significantsocietal burden but is difficult to diagnose insocietal burden but is difficult to diagnose inany given patientany given patient
Treatment includes prevention strategies andTreatment includes prevention strategies andthe usual COPD therapiesthe usual COPD therapies
GOLD guidelines for COPD assessment andGOLD guidelines for COPD assessment andtherapy have been significantly revised intherapy have been significantly revised in20112011
Better distinction of the type of COPD anyBetter distinction of the type of COPD anyspecific patient has is comingspecific patient has is coming…… ““phenotypingphenotyping””





























