Embed Size (px)
Citation preview

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Update diagnostiek en behandeling van hartfalen
Rudolf de Boer, MD PhD FESC Cardioloog, Universitair Medisch Centrum Groningen WCN Congres “Hart voor de Zaak”, 27-28 November, 2014 Mövenpick Hotel, Amsterdam
Thanks to: A.A. Voors, A. Mosterd & A.S. Maisel for sharing slides

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Update diagnose – ESC 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
ESC: (nog?) géén “stage A & B”

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
The Short of Breath Pie

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Heart Failure
Pneumonia Pneumothorax
Anemia
Pulmonary Embolus
Musculoskeletal Pain
MetHgb Mondor’s Syndrome Tietze’s
disease
COPD exacerbation
Pneumomediastinum
Breast Cancer
Cyanide poisoning
FB Aspiration
Metabolic acidosis
Anaphylaxis
Chemical Exposure
Mediastinitis
Lung Cancer
Anxiety Panic Attack
DKA
Subdiaphrag Abcess
Empyema
Amniotic Fluid Embolus
IVDA Pulm Infarction
Asthma

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
• Shortness of breath • Edema • Neck vein Distension • S-‐3
Francis GS. Am J Med. 2001; 110 (suppl):375-‐465

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
How Good Is the History and Physical in AHF?
Variable Sensitivity (%) Specificity (%) Accuracy (%)
Hx of HF 62 94 80
Dyspnea 56 53 54
Orthopnea 47 88 72
Rales 56 80 70
S3 20 99 66
JVD 39 94 72
Edema 67 68 68
Dao Q, et al. J Am Coll Cardiol. 2001; 37:379-‐385.

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
BNP Levels in Patients Presenting With Either Systolic or Diastolic Dysfunction
J Am Coll Cardiol 2003; 410:2010-‐17.
1000
500
300 200
100
50
30 20
10
5
BN
P (p
g/m
L)
Non CHF Diastolic Systolic n=844 n=165 n=287
Median= 34 pg/mL
Median= 821 pg/mL
Median= 413 pg/mL

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Perceived NYHA Class in Patients Ultimately Admitted
374 93 168 103 10 ≥200 pg/mL
44 111 18 14 1 <200 pg/mL
Total IV III II I BNP
Singer AJ. Circ Heart Fail. 2009; 2:287-‐93

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1 P
roba
bilit
y (R
RT
)
Biomarker X
BM <xx
High NPV
BM >XX
High PPV R
ule
out
Rul
e in
Grey area

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
SegmenKng a Sub-‐type of Heart Failure Based on Underlying Disease
HF GENERAL POPULATION
de Boer RA, et al. Cardiovasc Drugs Ther. 2014; 28:237-‐46.

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
SegmenKng a Sub-‐type of Heart Failure Based on Underlying Disease
HF GENERAL POPULATION
de Boer RA, et al. Cardiovasc Drugs Ther. 2014; 28:237-‐46.

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
SegmenKng a Sub-‐type of Heart Failure Based on Underlying Disease
BIOMARKER X MEDIATED HF HF GENERAL POPULATION
NON-‐BIOMARKER X MEDIATED HF
de Boer RA, et al. Cardiovasc Drugs Ther. 2014; 28:237-‐46.

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
SegmenKng a Sub-‐type of Heart Failure Based on Underlying Disease
BIOMARKER X MEDIATED HF HF GENERAL POPULATION
• AcVve disease process mediated by X (e.g. fibrosis), with adverse remodeling
• Progressive
• ~30-‐50% are at greatest risk of adverse outcome
• Heterogeneous eVology
• Not inherently progressive
• ~50-‐70% are at lower risk of adverse outcome
NON-‐BIOMARKER X MEDIATED HF
de Boer RA, et al. Cardiovasc Drugs Ther. 2014; 28:237-‐46.

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen Cappadocia
BNP
GDF-15 PCT
Gal-3
ST-2
HD profiles proteomics
phenomics

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Current and Future treatment of HF
• ACE-inhibitor and beta-blocker as standard therapy: what next?
• Role of ivabradine • Future therapy for HFrEF • Current and Future Treatment of HFpEF • Current and Future Treatment of Acute Heart
Failure

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen McMurray JJ, et al. Eur J Heart Fail. 2012; 14:803-‐69. ESC HF Guidelines 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen McMurray JJ, et al. Eur J Heart Fail. 2012; 14:803-‐69. ESC HF Guidelines 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen McMurray JJ, et al. Eur J Heart Fail. 2012; 14:803-‐69. ESC HF Guidelines 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen McMurray JJ, et al. Eur J Heart Fail. 2012; 14:803-‐69. ESC HF Guidelines 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
MRAs in Severe HFrEF and post-MI
RALES: CHF NYHA III-IV 30% mortality reduction
EPHESUS: LV-dysfunction After AMI; 15 % mortality reduction

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen Zannad F, et al. N Engl J Med 2011; 364: 11-‐21

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
EMPHASIS: primary outcome
Zannad F, et al. N Engl J Med 2011; 364: 11-‐21

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Recommendation MRA and ARB
McMurray JJ, et al. Eur J Heart Fail. 2012; 14:803-‐69. ESC HF Guidelines 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
• 6558 HF patients; LVEF ≤ 35%, in sinus rhythm, with HR ≥ 70 BPM despite optimal beta blockade, HF hosp <1 year on stable background medication
• randomized to (maximum) 7·5 mg twice daily or matching placebo
• Primary endpoint was the composite of cardiovascular death or hospital admission for worsening heart failure
Swedberg K, et al. Lancet 2010; 376:875-‐85

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
SHIFT – main results
Swedberg K, et al. Lancet 2010; 376:875-‐85

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Recommendations Ivabradine
Teerlink JR. Lancet 2010; 376:847-‐9

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
• ICD, class I indicaVon in eligible paVents
• CRT-‐D, class I indicaVon in eligible paVents
• Vagal Nerve sVmulaVon: mixed results!
• Renal denervaVon: starVng all over again
• Telemonitoring……………………………
Devices

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Guidelines are just Guidelines
• Example:
• ICD implantation

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Guidelines ICD in primary prevention of SCD
• ICD implantation is reasonable (Class I Level A)
• LV ejection fraction < 30-35%
• Optimal medical therapy
• Not within 40 days of infarction
• 90 year old woman, class II/IV, LVEF 28% should be
considered for ICD (in absence of contraindications)
McMurray JJ, et al. Eur J Heart Fail. 2012; 14:803-‐69. ESC HF Guidelines 2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Here is the truth ICDs for primary prevention
• Your patient thinks: • ICD: life saving for at least 50 of 100 patients receiving them
• But you know: • ICD: life saving for 7 of 100 patients receiving them
• No such thing as immortality
• Benefits only after 1 year

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Current and Future treatment of HF
• ACE-inhibitor and beta-blocker as standard therapy: what next?
• Role of ivabradine • Future therapy for HFrEF • Current and Future Treatment of HFpEF • Current and Future Treatment of Acute Heart
Failure

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
X
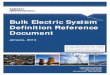
Future therapy for HFrEF: LCZ696?
Beneficial physiological response Pathophysiological response
Vasodilation ! blood pressure ! sympathetic tone ! aldosterone levels ! fibrosis ! hypertrophy Natriuresis/Diuresis
HF symptoms/ progression
NPs Ang II
NEP
Damage
Inactive fragments
AT1 receptor X
RAAS NP system
Vasoconstriction " blood pressure " sympathetic tone " aldosterone " fibrosis " hypertrophy
Dual NEP/RAAS
inhibition (LCZ696)
Neurohormonal balance
X

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
LCZ696 (Valsartan and NEP inhibitor, AHU 377)
STUDY TERMINATED EARLY BY DSMB

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
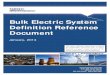
Primary endpoint: Death from CV causes or first hospitalization for HF
McMurray, et al. N Engl J Med 2014; ePub ahead of print: DOI: 10.1056/NEJMoa1409077.
Hazard ratio = 0.80 (95% CI: 0.73–0.87) p<0.001
Days since randomization No at risk LCZ696 4187 3922 3663 3018 2257 1544 896 249 Enalapril 4212 3883 3579 2922 2123 1488 853 236
Cum
ulat
ive
prob
abili
ty
1.0
0.6
0.4
0.2
0 0 180 360 540 720 900 1080 1260
Enalapril LCZ696

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Treatment of Diastolic Heart Failure
“No treatment has yet been shown, convincingly, to reduce morbidity and mortality in paVents with HF-‐PEF. DiureVcs are used to control sodium and water retenVon and relieve breathlessness and oedema as in HF-‐REF. Adequate treatment of hypertension and myocardial ischaemia is also considered to be important, as is control of the ventricular rate in paVents with AF.”
ESC HF Guidelines 2008/2012

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
RAAS-‐blockers in HFpEF: unsuccessfull
Charm-Preserved
PEP-CHF I-PRESERVE
Drug Candesartan 32 mg vs. Placebo
Perindopril 4 mg vs. Placebo
Irbesartan 300 mg vs. Placebo
Number 3023 850 4128
Age 67 years 75 years 72 years
% Female 40 55 60
LVEF >40% (54) >40% (64) >45% (60)
Primary Outcome
CV-death or HF-hosp
Death or HF-hosp
Death or CV-hosp
Follow-up 37 months 25 months 50 months

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
• Objective: to determine effects of spironolactone on composite endpoint of CV-mortality, aborted cardiac arrest or HF-hospitalization in HFpEF patients
• Inclusions: Symptomatic HF, Age ≥50, LVEF ≥45%, stratified according to: • HF-hospitalization in past year
• Elevated NPs (BNP ≥100 pg/mL or NT-proBNP ≥360 pg/mL)
• Major exclusions: eGFR <30 ml/min/1.73m2, K+ ≥5 mmol/L, AF >90/min, recent ACS.
Pil B, et al. N Engl J Med 2014; 370: 1383-‐1392

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Primary outcome
Outcome Spironolactone Placebo HR (95%CI) and p-value
Primary Outcome 320 (18.6%) 5.9/100pt-yr
351 (20.4%) 6.6/100pt-yr
0.89 (0.77-1.04) P=0.138
Primary Components
CV Mortality 160 (9.3%) 2.8/100pt-yr
176 (10.2%) 3.1/100pt-yr
0.90 (0.73-1.12) P=0.354
Aborted Cardiac Arrest
3 (<1%) 0.05/100pt-yr
5 (<1%) 0.09/100pt-yr
0.60 (0.14-2.50) P=0.483
HF Hospitalization 206 (12.0%) 3.8/100pt-yr
245 (14.2%) 4.6/100pt-yr
0.83 (0.69-0.99) P=0.042
Mean follow-up 3.3 years
Pil B, et al. N Engl J Med 2014; 370: 1383-‐1392

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Safety
Spironolactone Placebo P-value Hyperkalemia (≥ 5.5 mmol/L)
322 (18.7%)
157 (9.1%)
<0.001
Hypokalemia (< 3.5 mmol/L)
279 (16.2%)
394 (22.9%)
<0.001
Total number of SAE’s: spironolactone 835 (48.5%) placebo 855 (49.6%)
However… Doubling Creatinine above ULN HR=1.49 (1.18-1.87); P<0.001
Pil B, et al. N Engl J Med 2014; 370: 1383-‐1392

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen Pfeffer MA, et al. Circula>on. 2014; 131: 00-‐00 (ePub)

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
• Target patient population: ∼4,300 patients with symptomatic HF (NYHA Class II–IV) and LVEF ≥45%
PARAGON-HFPEF: study design
*Valsartan 40 mg BID (up to 2 weeks) followed by valsartan 80 mg BID as an optional starting run-in dose for those patients being treated with less than the minimum dose of ACEI or ARB at Visit 1
up to 2 weeks ~240 weeks
Valsartan 160 mg BID
LCZ696 200 mg BID
LCZ696 100 mg BID
On top of optimal background medications for co-morbidities (excluding ACEIs and ARBs)
Primary outcome: CV death and total (first and recurrent) HF hospitalizations (anticipated ~1,721 primary events)
Valsartan 80 mg BID* Screening
3–8 weeks
Active run-in period
Double-blind treatment period
Randomization 1:1
• Solomon SD, et al. Poster presentation at ESC-HF Congress, 25 May 2013; Clinicaltrials.gov NCT01920711;accessed March 2014

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Effect of ivabradine versus placebo on cardiac function, exercise capacity, and neuroendocrine activation in patients with Chronic Heart Failure with Preserved left ventricular
Ejection Fraction An 8-month, randomised double-blind, placebo controlled, international,
multicentre study
• Primary objective± to assess the effect of ivabradine compared to placebo on the diastolic function, exercise capacity, and the neuroendocrine activation over an 8-month treatment period in patients with chronic HF-PEF

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Current and Future treatment of HF
• ACE-inhibitor and beta-blocker as standard therapy: what next?
• Role of ivabradine • Future therapy for HFrEF • Current and Future Treatment of HFpEF • Current and Future Treatment of Acute Heart
Failure

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Drugs in AHF: current 1. Diuretics
2. Vasodilators (nitrates) ?
3. Oxygen
4. Morphine
5. Ventilation
6. Treat underlying condition(s)
Lille change in last ~30 years

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Drug Trials in AHF: unsuccessful 1. PDE-inhibitors: Milrinone: OPTIME-CHF
2. Endothelin antagonists: Tezosentan: VERITAS
3. Ca-sensitizers: Levosimendan; SURVIVE/REVIVE
4. AVP Antagonists: Tolvaptan; EVEREST
5. Adenosine A1-Receptor Antagonist: Rolofylline; PROTECT
6. Natriuretic Peptides: Nesiritide: ASCEND-HF
7. Low dose Dopamine/Nesiritide: ROSE

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Relaxin
Hsu et al. Science 2002;295:671–674; Jeyabalan et al. Adv Exp Med Biol 2007;612:65–87; Dschietzig et al. Circ Res 2003;92:32–40
Relaxin
• Naturally occurring hormone, discovered in 1929
• Elevated in circulation in first trimester of pregnancy and throughout 9 months
• Relaxin receptors, identified in 2002, localized in blood vessels
• Mechanism of action involves activation of the endothelial endothelin type B receptor
• Contributes to maternal hemodynamic adjustments to pregnancy

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
RELAX-AHF: Patients
• 1161 patients hospitalized for AHF, with elevated BNP/NT-proBNP levels and pulmonary congestion by chest X-ray
• Systolic blood pressure >125 mmHg at the beginning and at the end of screening
• Able to be randomized within 16 hours from presentation to the hospital
• Impaired renal function defined as a eGFR on admission between 30–75 mL/min, calculated using the simplified Modification of Diet in Renal Disease (sMDRD) equation
Teerlink JR, et al. Lancet 2013; 381:29–39

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
1st Primary Endpoint: Change in dyspnea with VAS
2nd Primary Endpoint: Change in dyspnea with Likert
35
30
25
20
15
10
5
0
Cha
nge
from
bas
elin
e (m
m)
0 6h Day 1 Day 2 Day 3 Day 4 Day 5 Follow-up
12h
Serelaxin (n=581)
Placebo (n=580)
Placebo: mean AUC (SD)=2,308 (3,082) mm*h Serelaxin: mean AUC (SD)=2,756 (2,588) mm*h
p=0.007
100
80
60
40
20
0
–20
–40
–60
–80
–100
Pat
ient
s (%
)
p=0.113 p=0.051 p=0.086
31.4 35.8 44.6 50.3 63.1 67.9
8.7 9.8 16.6 16.4 26.7 25.8
42.1
21.1 7.3
36.4
22.8 7.8
33.9
32.9
14.5
28.0
35.0
16.4
26.0
37.4
24.7
22.7
37.5
26.4
Dyspnea Likert Scale
Moderately improved Markedly improved
Minimally improved No change Minimally worsened Markedly worsened
Placebo Serelaxin Placebo Serelaxin Placebo Serelaxin 6 h 12 h 24 h
SD=standard deviation
Teerlink JR, et al. Lancet 2013; 381:29–39

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
• (Cardiovascular) mortality was not the primary endpoint of the study
• In order to get EMA/FDA approval/registration for reduction of mortality, a follow-up study needs to be done
However….

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
RELAX-‐AHF-‐2: study design Please note that the study design informa3on for RELAX-‐AHF-‐2 is subject to change
Discharge#
Placebo i.v.
Serelaxin 30 µg/kg/d i.v.*
0 6 12 24 48 72 96 120 h 14 60 120 180 d
48 h study drug infusion (i.v.) period
*Same weight range-‐adjusted dosing as in RELAX-‐AHF; ‡Standard HF therapy permiied at physician’s discreKon; #If discharge visit coincides with a scheduled visit, only the discharge visit will be performed. AHF=acute heart failure; CV=cardiovascular; d=day; h=hour; i.v.=intravenous; SBP=systolic blood pressure Clinicaltrials.gov: NCT01870778; NovarVs, data on file 2013
In addiKon to standard HF therapy‡
Screening
Double-‐blind randomized treatment period
Screening occurred aner ≥40 mg i.v. furosemide
PresentaKon <16 h
RandomizaKon 1:1
Target patient population: 6,375 patients hospitalized with AHF, presenting with dyspnea, normal to elevated SBP (≥125 mmHg) and mild-to-moderate renal impairment
Primary outcome: Kme to CV death

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Conclusions
HFrEF: ACEi (or ARB) and beta-blocker
Still NYHA II or more: aldosterone blocker
In selected patients: ivabradine
Big bang: LCZ696
Still no evidence based therapy for HFpEF • Maybe MRAs? • Maybe ARNI?
Still no evidence based therapy for AHF • Maybe Serelaxin?

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
SegmenKng a Sub-‐type of Heart Failure Based on Underlying Disease
BIOMARKER X MEDIATED HF HF GENERAL POPULATION
• AcVve scarring (fibrosis) and adverse remodeling
• Inherently progressive
• ~30-‐50% are at greatest risk of adverse outcome
• Heterogeneous eVology
• Not inherently progressive
• ~50-‐70% are at lower risk of adverse outcome
NON-‐BIOMARKER X MEDIATED HF

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Hypertension Blood Pressure
Diabetes Glucose, HbA1c
Lipids Cholesterol,LDL

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
So everyone is supposed to be on the same dose of heart failure medications.
That cannot be “personalized medicine”

Har
tfale
n: U
pdat
e di
agno
stie
k en
beh
ande
ling
University Medical Center Groningen
Comparison of Trials BNP-‐Guided Therapy
Adapted from Felker M, et al. Am Heart J. 2009; 158: 422
Troughton
STARS-BNP
TIME-CHF
BATTLE-SCARRE
D
PRIMA SIGNAL-HF
Berger et al.
PROTECT
n 69 220 499 364 345 252 278 151
Blinding No No Single Double Single Single ? No
Marker NT-BNP BNP NT-BNP NT-BNP NT-BNP NT-BNP NT-BNP NT-BNP
Aim (ng/l) 1692 100 400/800 1270 discharge 50% red. 2200 1000
Control HF score Usual care
≤class II 2 groups Usual care
HF spec. 2 groups Usual care
1° EP Death, CV
hosp., HF
HF death,
HF hosp.
Death, all-cause
hosp.
All-cause mortality
d alive out hosp.
d alive out CV hosp.
HF hosp., death
CV events
Age 70 66 77 76 72 77 71 63
NT-BNP 1981 350 4328 2008 2940* ~2500 ~2350 2118
1˚ EP Pos Pos Neg Neg Neg Neg Pos Pos Mortality p=0.06 7/11, ns p=0.06 Identical p=0.21 Identical Identical p=0.52