Embed Size (px)
Citation preview
female�26:13, renal cancer 26 cases, re-nal pelvic cancer 13 cases, total nephrec-tomy 27 cases, partial nephrectomy 12cases, age 40-88), who had normal renalfunction and had not had treatment forhyperuricemia between January 2005 andOctober 2009. We measured serum uricacid and eGFR of these patients preopera-tion and postoperation. And we examinedthe relations of these data and eGFR ofpreoperation, age, sex and BMI value.Results: As for the patients provided to-tal nephrectomy, the mean value of eGFRdecreased in 63.5¡43.5ml/1.47 minute/m2. The hyperuricemia appeared in 4cases of total 27 cases before operation.Although, it appeared additionally in new4 cases. The mean of serum uric acid sig-nificantly increased in from 5.8 to 6.4mg/dl. By sex, uric acid of males significantlyincreased (6.2to7.3mg/dl), although itsvalue in females presented no significantchange (5.4 to 5.6 mg/dl). Only the eGFRof postoperation has shown significantcorrelation with the change rate of serumuric acid at 3 months after the operation.At one side, by cases of partial nephrec-tomy, we showed a little decrease of theeGFR (65.5 to 61.0 ml/minutes/1.47m2),although no new appearance of hyperuri-cemia and no change of serum uric acid(5.1 to 5.1 mg/dl).Conclusions: Hyperuricemia is one ofthe risk factors of chronic renal failure, ispointed out to cardiovascular disease.Even if the serum uric acid of postopera-tion was normal value, the possibility ofits increasing is high. Especially, sufficientconsideration is necessary for hyperurice-mia in males and patients whose kidneyfunctions decrease.
UP-01.166Risk Factor of Hyperuricemia AfterNephrectomySugimoto MDept. of Urology, Okayama RousaiHospital, Okayama, Japan
Introduction and Objectives: Hyperuri-cemia is a common complication afternephrectomy. Although, there were fewreport of its occurrence rate, risk factorand treatment. We assessed the develop-ment and the risk factor of hyperuricemiaafter kidney surgery.Materials and Methods: Serum uric acidconcentration and estimated glomerularfiltration rate (eGFR) were measured in 39cancer patients who received kidney sur-gery (67% male 33% female, 69% total re-section 31% partial resection). Hyperurice-mia was defined as a serum uric acid
concentration of at least 7.0 mg/dl. Weassessed the associations between hyper-uricemia, eGFR, sex, age and BMI value.Results: Serum uric acid concentration ofpatients receiving nephrectomy andnephroureterectomy significantly in-creased. Hyperuricemia was newly ob-served in 4 cases (15%). Only male sexand renal disfunction were associatedwith hyperuricemia after kidney surgery.No significant change of uric acid concen-tration was shown in patients receivingpartial nephrectomy.Conclusions: Hyperuricemia is a com-mon complication after total nephrec-tomy, and may be associated with malesex and renal dysfunction.
UP-01.167Successful Improvement ofAmbulatory Function by DirectDecompressive Surgery in Non-Ambulatory Patients with ExtraduralSpinal Cord Compression Due toSpinal Metastasis of Renal CellCarcinomaTakagi T1, Kondo T1, Izuka J1,Kobayashi H1, Hashimoto Y1, Tomita E1,Suzuki H1, Tanabe K1, Kubota M2,
Wada K2
1Dept. of Urology; 2Dept. of Orthopedics,Tokyo Women’s Medical University,Tokyo, Japan
Introduction and Objective: Direct de-compressive surgery has been reported tosignificantly improve ambulatory functioncompared to radiotherapy alone in non-ambulant patients with metastatic extra-dural spinal cord compression (ESCC), butthere have been only a few reports focus-ing on those with renal cell carcinoma(RCC). In the present study, we analyzedthe results of our surgery-based therapy.Materials and Methods: Six non-ambula-tory patients, corresponding to Frankelgrade C, with ESCC due to spinal metasta-ses of RCC who underwent direct decom-pressive surgery were the subjects of thisstudy.The surgery consisted of laminac-tomy, debulking of tumors and posteriorstabilization.Tumor embolization was per-formed prior to surgery to reduce intraop-erative blood loss.Radiotherapy and sys-temic therapy including the cytokine ortargeted therapy and zoledronic acid wereadded to the surgery.Results: The mean age at time of surgerywas 58.0 years. Three patients had spinal
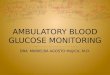
day 0
Cystain C0.0 0.5 1.0 1.5
0
50
100
150krea GFRcysC GFR
UP-01.164, Figure 3.
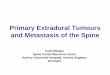
day 1
Cystatin C0.0 0.5 1.0 1.5 2.0
0
50
100
150krea GFRcysC GFR
UP-01.164, Figure 4.
UNMODERATED POSTER SESSIONS
S242 UROLOGY 78 (Supplement 3A), September 2011

metastases alone.All patients had progres-sive neurological deficit and were non-ambulant at the time of surgery. Spinalsurgery was successfully performed with amean operation time of 265 minutes andmean intraoperative bleeding of 1726ml.No surgery-related complication wasobserved. After surgery, all patients re-gained ambulatory function within 2months after surgery. Cytoreductive ne-phrectomy was performed within 1month after spinal surgery for 3 patientswho showed the symptoms of ESCC asthe first presentation. All patients receivedsystemic therapy after surgery, includingcytokine or targeted therapies. Zoledronicacid was used in 4 patients. They wereambulatory with the use of the assistingapparatus, corresponding to Frankel gradeD, just before the terminal stage of thedisease for 4 � 29 months (median 10.5months). Four patients died of disease,but one patient survived for 3 years. Me-dian overall survival time after surgerywas 13 months (4 - 30 months).Conclusions: The direct decompressivesurgery effectively improved ambulatoryfunction in the non-ambulant patientswith ESCC due to metastatic RCC. Al-though it remains undetermined whetherthis surgical intervention will improve theoverall survival, patients with a single siteof cord compression, who are fit for sur-gery may be considered for decompres-sive surgery before radiotherapy.
UP-01.168Incidence of Lymph NodeInvolvement According toPathological T Stage or Tumor Gradein the Urothelial Carcinoma of theUpper Urinary TractTakagi T, Kondo T, Izuka J, Kobayashi H,Hashimoto Y, Tomita E, Yoshida K,Tanabe KDept. of Urology, Tokyo Women’sMedical University, Tokyo, Japan
Introduction and Objectives: Our retro-spective study showed survival benefits oflymphadenectomy in the advanced stageof patients with urothelial carcinoma ofthe upper urinary tract (UCUUT). To iden-tify the incidence of lymph node metasta-sis by malignant potential of the tumorswill help to determine the patients in
whom lymphadenectomy is indicated.Inthe present study, we analyzed the inci-dence of lymph node metastases accord-ing to the pathological T stage or tumorgrade in the patients with UCUUT.Materials and Methods: Until August2010, 279 patients with UCUUT under-went surgical therapy in our departmen-t.All patients were histologically con-firmed to have urothelial carcinoma.Results: Mean age of patients was 68.2 �10.5 years (36 – 90).Follow up period was50.4 � 51.2 months (1 – 231). During thefollow up period, 68 patients were foundto have lymph node metastases at the re-gional sites. Fifty-one patients were diag-nosed to have lymph node metastasis atthe time of surgery. An additional 17 pa-tients newly developed lymph node me-tastases after curative surgery.Accordingto the pathological stage, the incidence oflymphatic metastases was 20% (2/10) inpTis, 0% (0/12) in pT1, 2% (1/51) in pT1,11% (5/46) in pT2, 9% (4/48) in pT3 withinvasion to renal parenchyma in tumors ofrenal pelvis, 39% (15/36) in pT3 with in-vasion to peripelvic fat in tumors of renalpelvis, 41% (18/44) in pT3 with invasionto periureteral fat in tumors of the ureter,and 75% (24/32) in pT4.According to thetumor grade, the incidence was 0% (0/11)in grade 1, 13% (16/120) in grade 2, and35% (52/148) in grade 3.Postoperativesurvival was positively correlated with theincidence of survival.Conclusions: The risk of lymphatic me-tastases in UCUUT amplified as T stage ortumor grade increased. The invasion toadipose tissue around the renal pelvis orthe ureter dramatically increased thechance of lymphatic metastases. The con-trol of lymphatic metastasis in muscle in-vasive disease, especially in the diseaseextending into to the surrounding adiposetissue seems to be strongly associatedwith the improvement of patients’ sur-vival.
UP-01.169Impact of the Tumor EnhancementPattern in Computed Tomography inDetecting Renal Cell Carcinoma fromSmall Renal Masses: Who ReallyRequires Biopsy?Takagi T, Kondo T, Izuka J, Kobayashi H,
Hashimoto Y, Tomita E, Tanabe KDept. of Urology, Tokyo Women’sMedical University, Tokyo, Japan
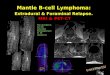
Introduction and Objective: We exam-ined the accuracy of multiphasic com-puted tomography (CT) findings in detect-ing renal cell carcinoma (RCC) from smallrenal masses to identify the patients whoare candidates for biopsy.Materials and Methods: From August2007 to December 2010, 150 patientswith renal tumors who underwent partialnephrectomy for presumed T1a RCC inour department were the subject of thisstudy. All patients received preoperativecontrast-enhanced multiphasic CT for thetumor evaluation. The CT density(Hounsfield unit) of the tumor was calcu-lated at pre-contrast (P), early arterialphase (A) and the venous phase (V).Results: Of the 150 renal masses, patho-logical examination showed benign find-ings in 11 (7%) including angiomyolipomain 4, metanephretic adenoma in 2 andothers in each 1. One hundred and thirty-nine (93%) were found to be malignant.When compared to the benign tumors,RCC tumors showed stronger early en-hancement indicated by an A/P ratio(4.47�2.30 versus 2.15�0.96, p�0.0011)and a more prominent washout pattern(0.86�0.38 versus 1.32�0.73, p�0.0005).The area under the curve of the receiveroperating characteristic analysis showedthe A/P ratio at 2.480 and the V/A ratio at0.995 as a cut-off value improved the abil-ity to distinguish the RCC tumors frombenign tumors. We categorized the pa-tients as shown in the table according toenhancement and washout patterns. Al-though 73% (22/30) of patients with weakenhancement in the early phase (A/P�2.48) and less washout (V/A�0.995)showed malignant findings, 97% (117/120) of the other patients showed malig-nant findings.Conclusions: The enhancement patternof multiphasic contrast enhanced CT ap-pears to be effective in distinguishingRCC tumors with early enhancement andlate washout. The tumors with weak earlyenhancement and without washout have a27% possibility of being benign tumorsand thus may be best advised to undergopreoperative biopsy.
UP-01.171Age and Gender, IndependentPrognostic Factors of Renal CellCarcinomas: A Multicenter StudyCho I1, Yoo C2, Oh C2, Kim S3, Km Y4,Kim H5, Seong D6, Chung H7, Hong S8,
UP-01.169, Table 1.
Early enhancement
Strong(A/P>2.48) Weak(A/P<2.48)Washout Prominent(V/A�0.995) 97/99(98%) 8/9(89%)
Weak(V/A�0.995) 12/12(100%) 22/30(73%)
UNMODERATED POSTER SESSIONS
UROLOGY 78 (Supplement 3A), September 2011 S243