Embed Size (px)
Citation preview
Unusual infections in SLE
Jyoti Ranjan Parida
My task today
• Why infection is important in SLE ?
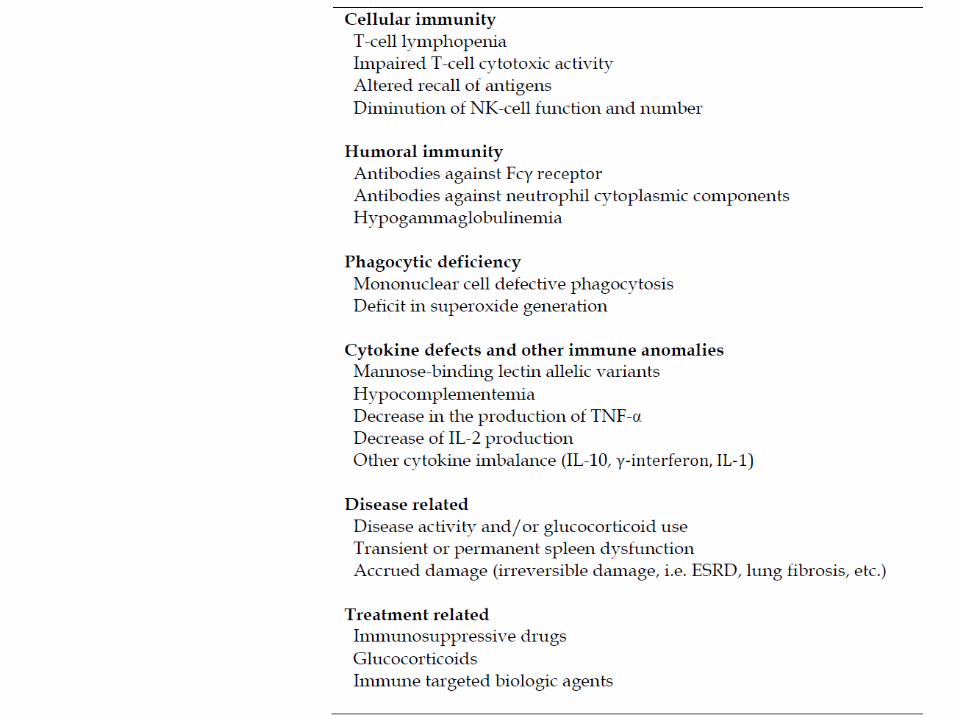
• Why SLE patient develop more infection?
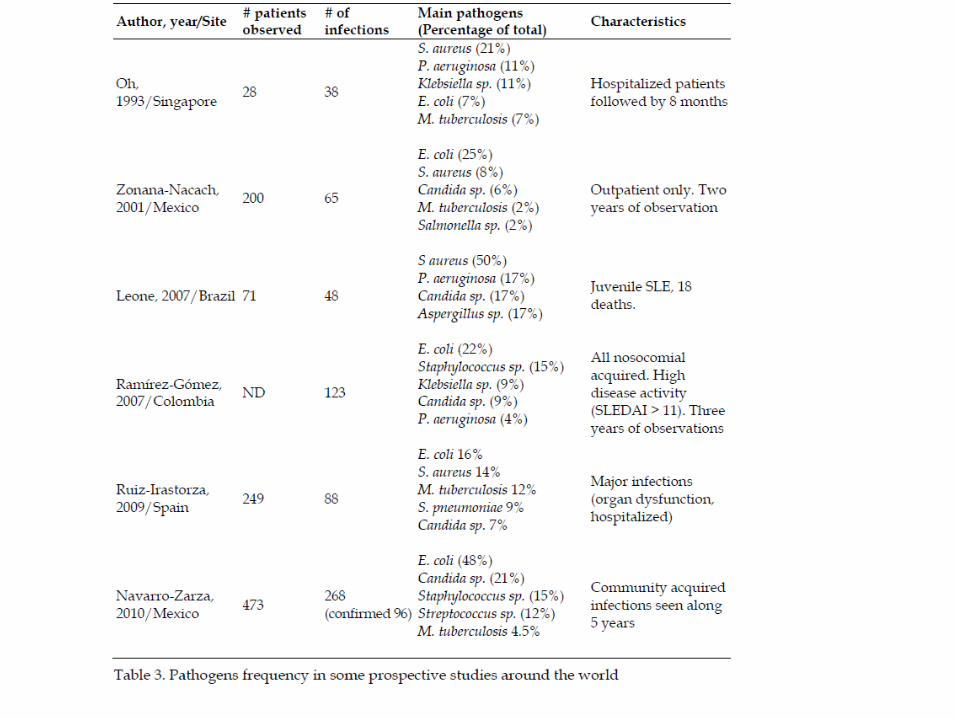
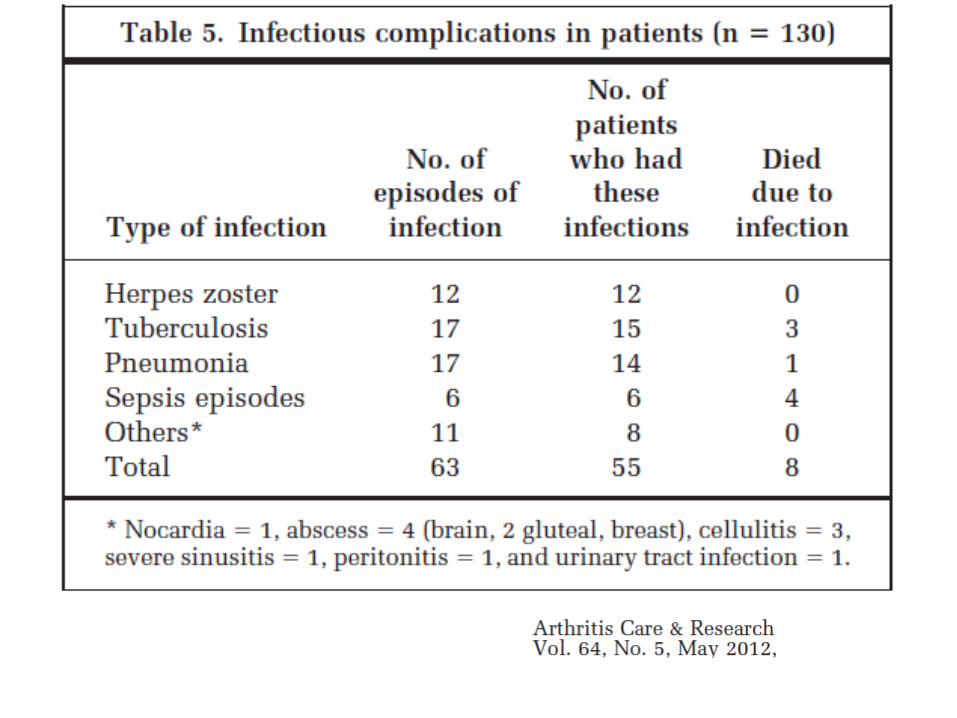
• What are the usual infections ?
• Unusual infections are not so unusual?
• Index cases of different spectrum of infections?
• Can we prevent infection?
My task today
• Why infection is important in SLE ?
• Why SLE patient develop more infection?
• What are the usual infections ?
• Unusual infections are not so unusual?
• Index case of different spectrum of infections?
• Can we prevent infection
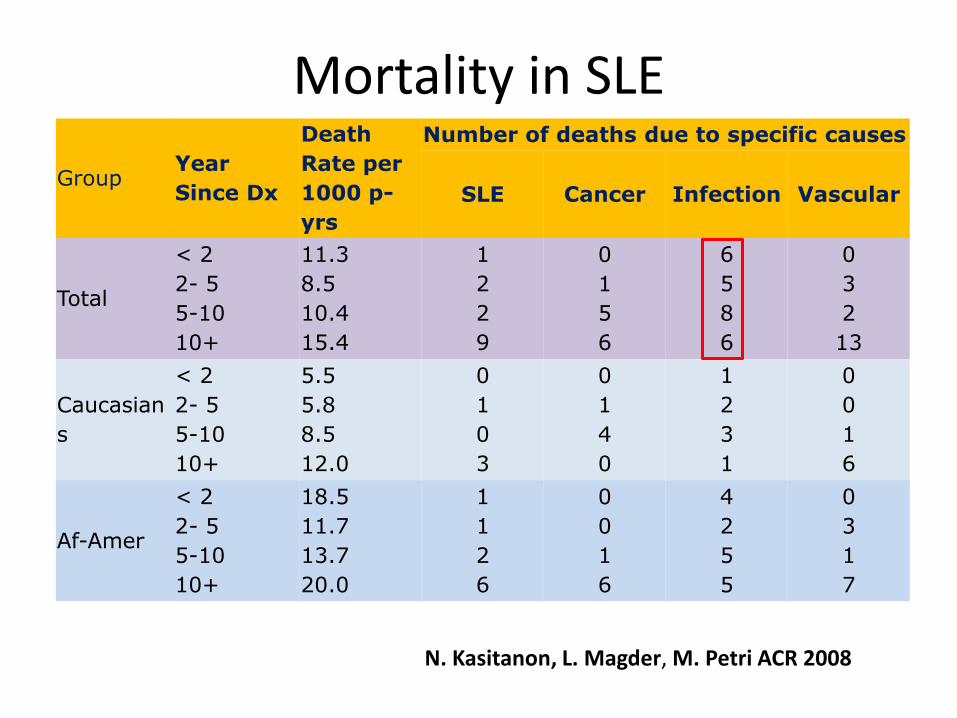
Mortality in SLE
Group Year
Since Dx
Death
Rate per
1000 p-
yrs
Number of deaths due to specific causes
SLE Cancer Infection Vascular
Total
< 2
2- 5
5-10
10+
11.3
8.5
10.4
15.4
1
2
2
9
0
1
5
6
6
5
8
6
0
3
2
13
Caucasian
s
< 2
2- 5
5-10
10+
5.5
5.8
8.5
12.0
0
1
0
3
0
1
4
0
1
2
3
1
0
0
1
6
Af-Amer
< 2
2- 5
5-10
10+
18.5
11.7
13.7
20.0
1
1
2
6
0
0
1
6
4
2
5
5
0
3
1
7
N. Kasitanon, L. Magder, M. Petri ACR 2008
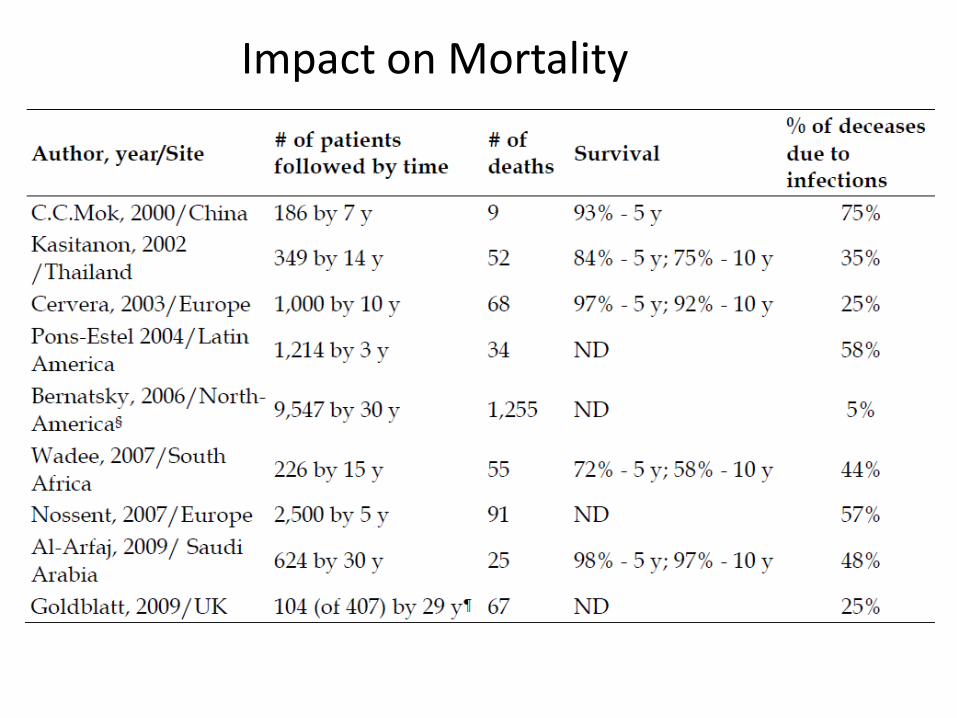
Impact on Mortality
Morbidity related to Infection
• Hospitalization due to infection: 15% of SLE / year
• Infection: 57% of all hospitalisation (Mexico)
• SLE patients admitted for other reasons
– 12.5% develop nosocomial infection
• Risk of major infection in SLE is 60% higher than other chronic diseases
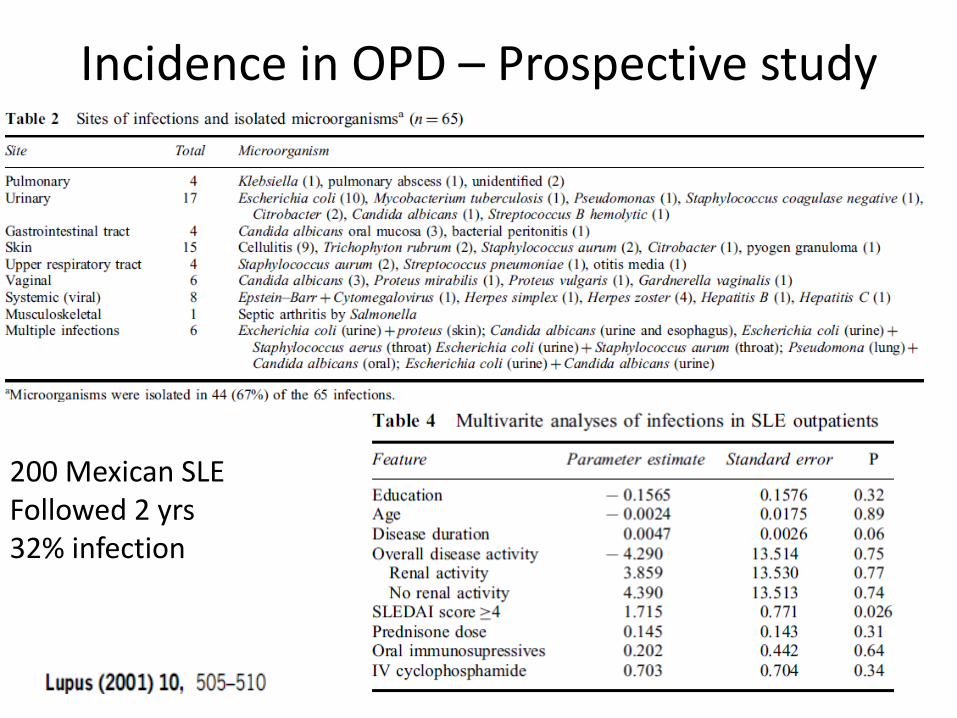
Incidence in OPD – Prospective study
200 Mexican SLE Followed 2 yrs 32% infection
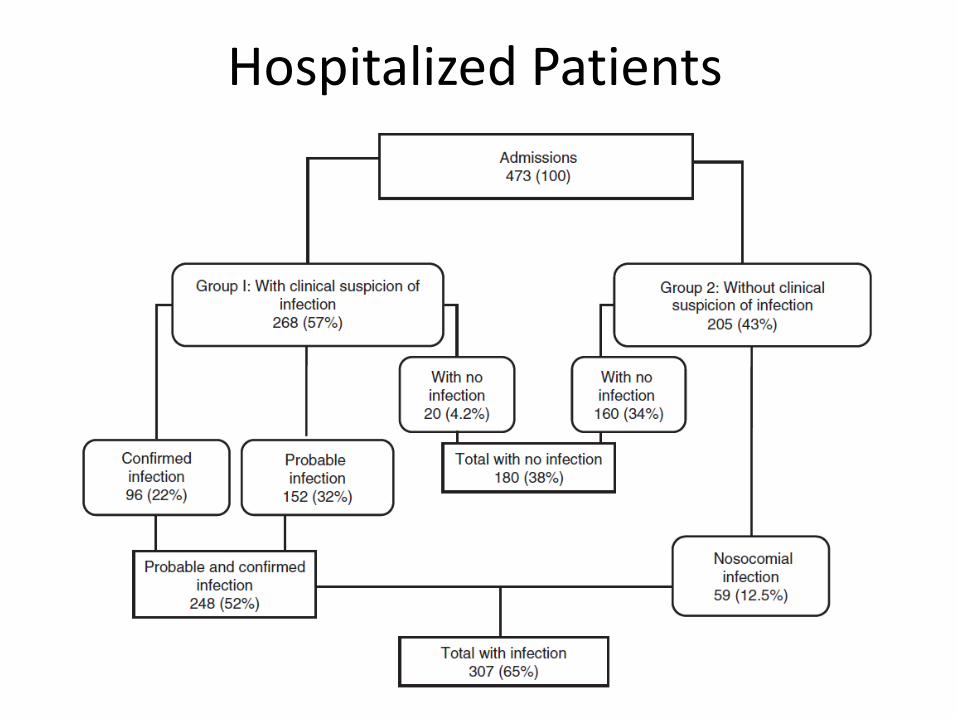
Hospitalized Patients
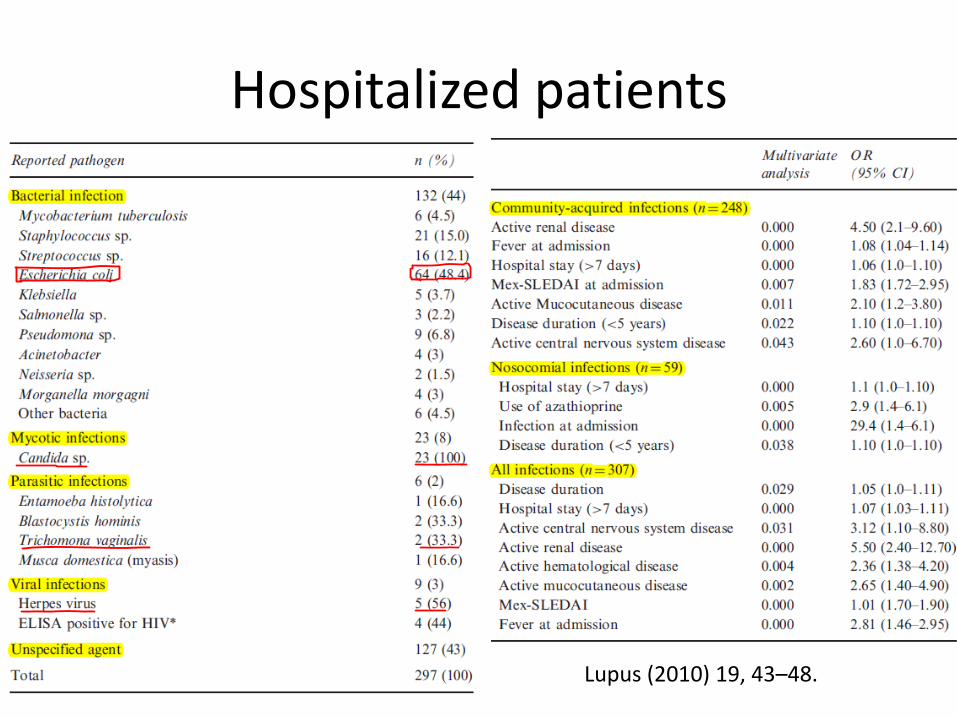
Hospitalized patients
Lupus (2010) 19, 43–48.
My task today
• Why infection is important in SLE ?
• Why SLE patient develop more infection?
• What are the usual infections ?
• Unusual infections are not so unusual?
• Index case of different spectrum of infections?
• Can we prevent infection?
My task today
• Why infection is important in SLE ?
• Why SLE patient develop more infection?
• What are the usual infections ?
• Unusual infections are not so unusual?
• Index case of different spectrum of infections?
• Can we prevent infection?
My task today
• Why infection is important in SLE ?
• Why SLE patient develop more infection?
• What are the usual infections ?
• Unusual infections are not so unusual?
• Index case of different spectrum of infections?
• Can we prevent infection?
Unusual infections?
• No standard definition
• Uncommon
• Mainly case report
• Often delayed diagnosis
• High index of suspicion
My task today
• Why infection is important in SLE ?
• Why SLE patient develop more infection?
• What are the usual infections ?
• Unusual infections are not so unusual?
• Index case of different spectrum of infections?
• Can we prevent infection?
Case 1
50/F
1997: Diagnosed as minor organ SLE
2001 : ILD, Rx 6 IV CP bolus →AZA
Pneumonia : AZA stopped, only on Prednisolone 7.5 mg/d
2008: Transient AF, Moderate MR with TR Rx Acitrom, Carvedilol, Amiodarone
2009 : Skin rash, no evidence of vasculitis , Pred10 mg/d
50/F PG 2010
C/o –
• Partial seizure (3 episodes)
• Forgetfulness 15 days
• Irrelevant talk
• No h/o aura/ incontinence/ Todd’s palsy
• No h/o trauma/TIA/seizure disorder
• No h/o fever/new skin rash/ oral ulcer/alopecia/joint pain
• On Phenytoin and stopped Acitrom
Examination
• PR 92/min, BP 110/70
• Inability to do simple calculation
• Unable to understand meaning of simple paragraph
• B/L papilledema
Possibilities
1. Intracerebral hemorrhage ( Acitrum induced)
2. NPSLE
3. ICSOL ( Malignancy, infective etc)
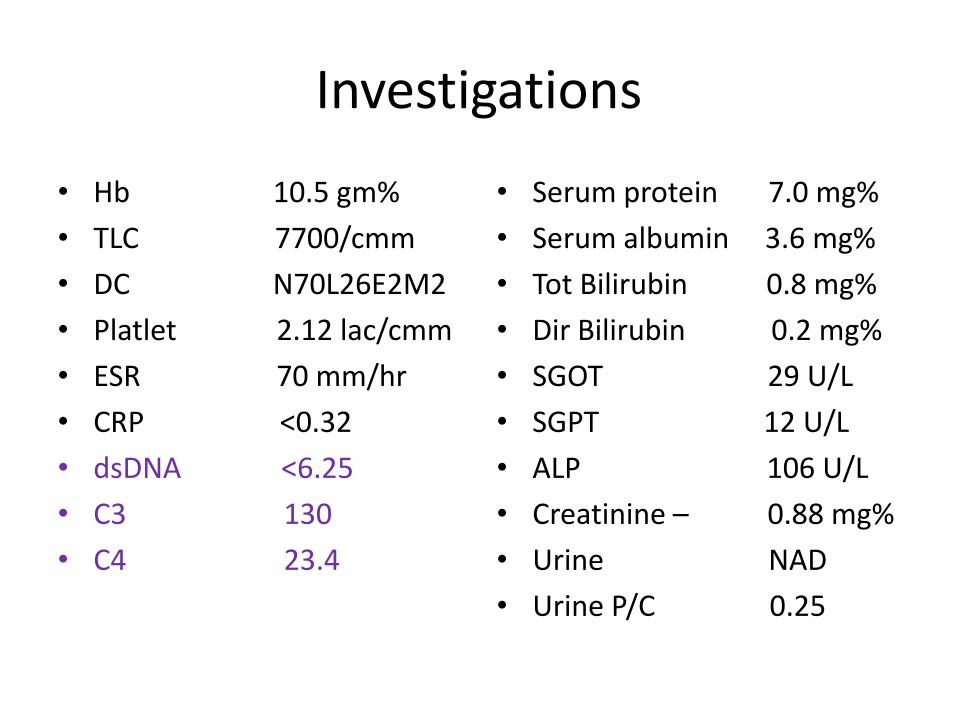
Investigations
• Hb 10.5 gm%
• TLC 7700/cmm
• DC N70L26E2M2
• Platlet 2.12 lac/cmm
• ESR 70 mm/hr
• CRP <0.32
• dsDNA <6.25
• C3 130
• C4 23.4
• Serum protein 7.0 mg%
• Serum albumin 3.6 mg%
• Tot Bilirubin 0.8 mg%
• Dir Bilirubin 0.2 mg%
• SGOT 29 U/L
• SGPT 12 U/L
• ALP 106 U/L
• Creatinine – 0.88 mg%
• Urine NAD
• Urine P/C 0.25
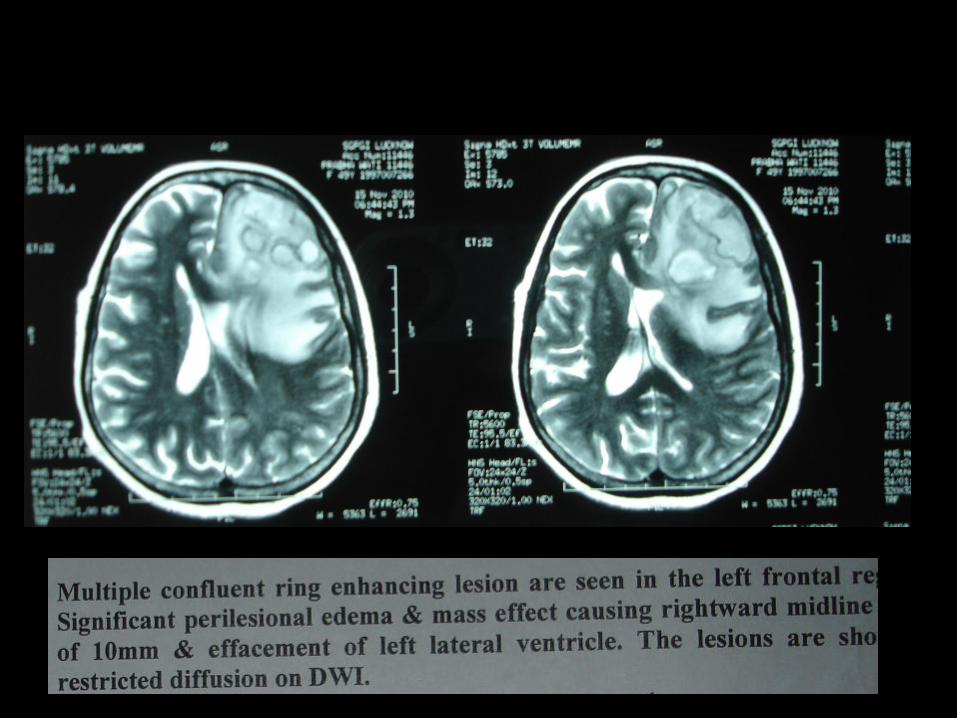
MRI Brain
Hospital course
• Surgical drainage : 15 ml thick pus aspirated and abscess cavity washed with saline -antibiotic
• Rx : Inj Cotrimoxazole + Amikacin
• Symptoms recovered – No seizure
• Discharged after 2 wks – Tab Cotrimaxazole + antiepileptic
• Review MRI after 1 month – significant ↓ in abscess size
Learning from the case
• Infection can mimic disease activity
• When in doubt, do Imaging for CNS symptoms
• Unusual infections are not so unusual in lupus
• CRP may be normal
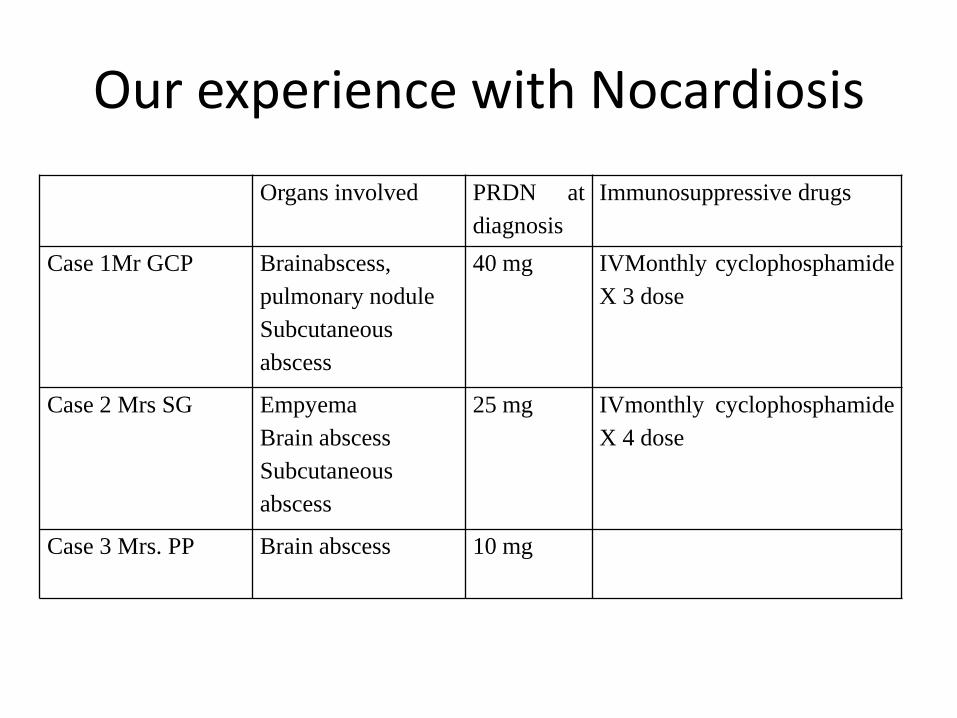
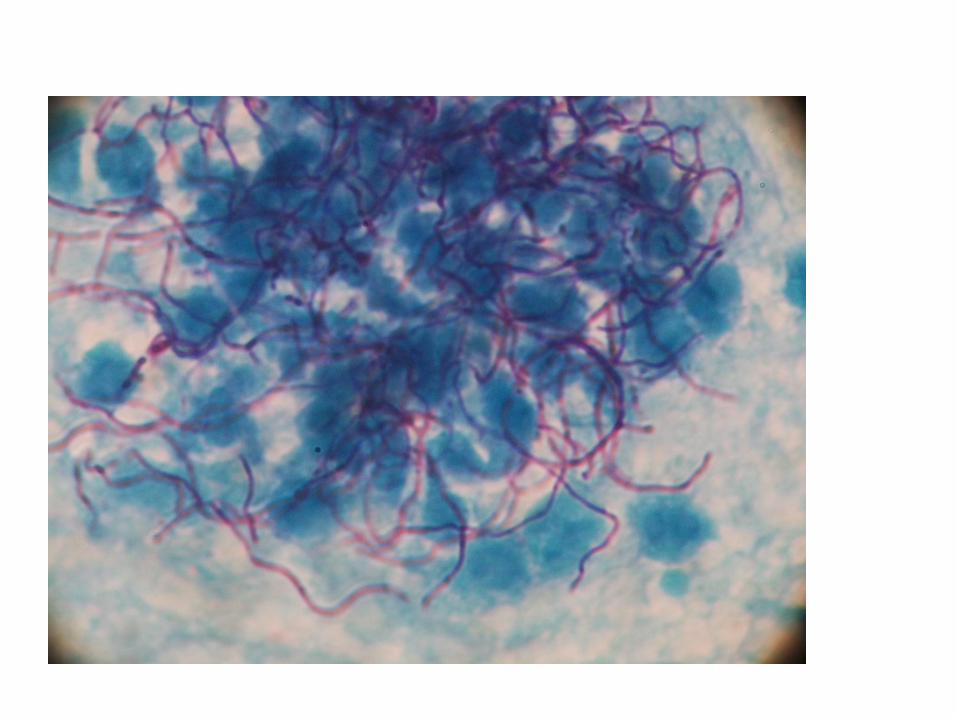
Our experience with Nocardiosis
Organs involved PRDN at
diagnosis
Immunosuppressive drugs
Case 1Mr GCP Brainabscess,
pulmonary nodule
Subcutaneous
abscess
40 mg IVMonthly cyclophosphamide
X 3 dose
Case 2 Mrs SG Empyema
Brain abscess
Subcutaneous
abscess
25 mg IVmonthly cyclophosphamide
X 4 dose
Case 3 Mrs. PP Brain abscess 10 mg
1. Nocardia sepsis in a multigravida with SLE and autoimmune hepatitis.
Anaesth Intensive Care 2007;35(4):601–4. 2. Nocardia brain abscesses in a male patient with SLE: successful outcome despite delay in diagnosis. Clin Rheumatol 2007;26(6):1020–2.
3. Disseminated nocardiosis with initial manifestation mimicking disease flare-up of systemic lupus erythematosus in an SLE patient. Am J Med 2005;118(11):1297–8. 4. Systemic lupus erythematosus associated with pulmonary nocardiosis. Arch Intern Med 1967;119:202–5.
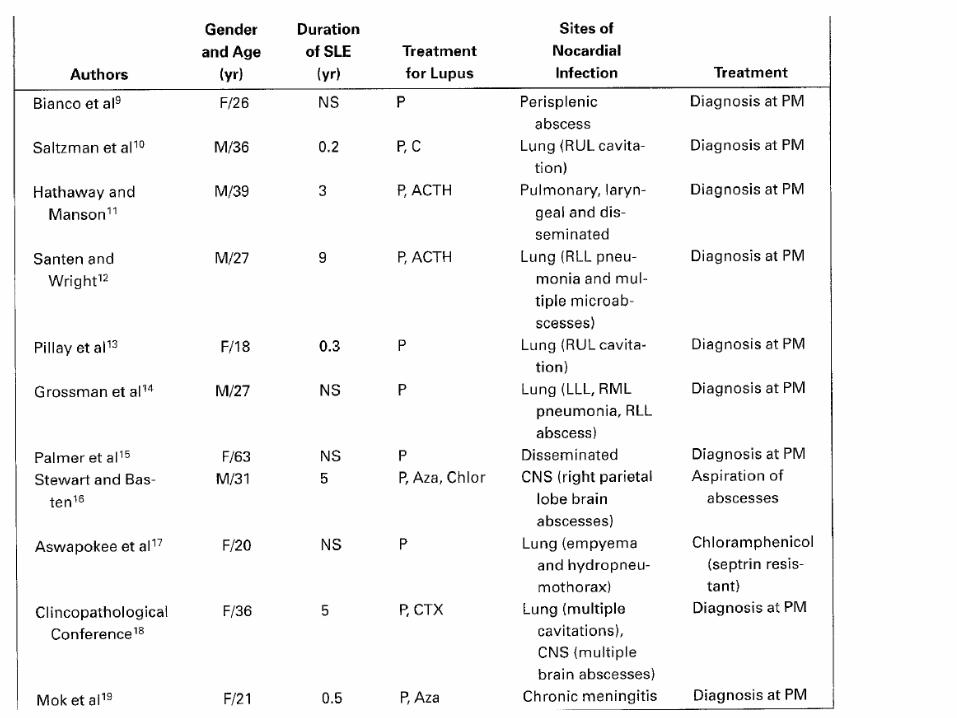
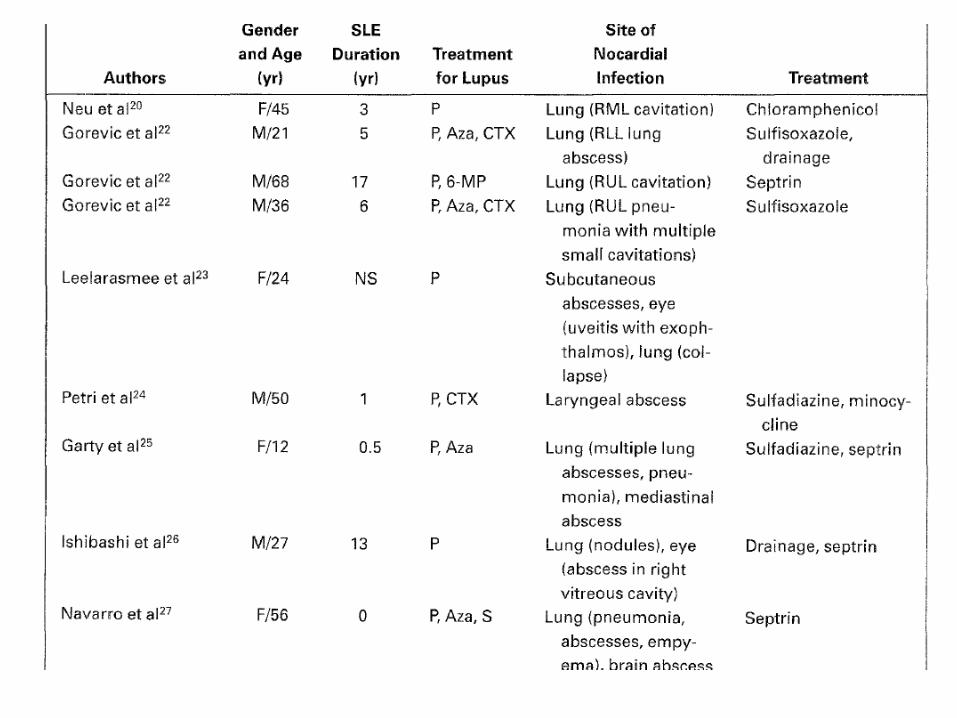
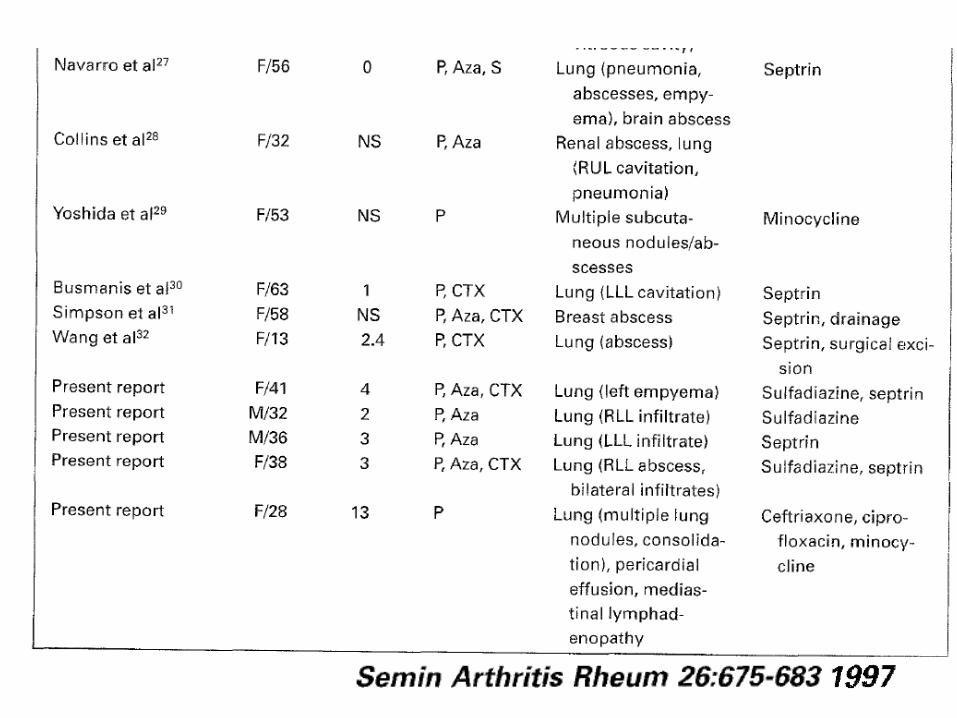
Recent Case Reports
Treatment
Combination (Cotrimoxazole +amikacin +ceftriaxone or imipenem) Clinical improvement - After 1–2 weeks of therapy After definite clinical improvement, 1 oral drug Antimicrobial Susceptibility whenever available Duration of Rx Most systemic infection – 6 -12 months Localized disease – 2-4 months HIV with CD4<200 - Indefinite
Harrison’s Principle Int Med 18th Ed
Case 2
17 year old female
April 2009
Fever
Oral ulcers
Malar rash
Photosensitivity
Painful rash on tips of fingers and toes
Past H/O choroiditis 2 year ago
Recovered with Prednisolone
1 month
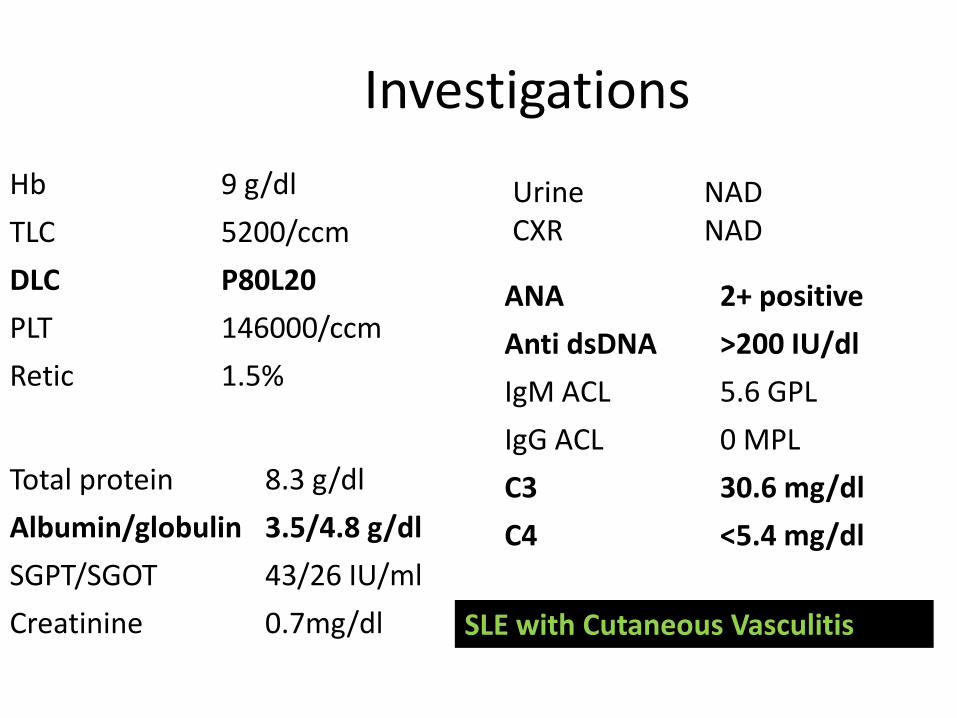
Investigations
Hb 9 g/dl
TLC 5200/ccm
DLC P80L20
PLT 146000/ccm
Retic 1.5%
Total protein 8.3 g/dl
Albumin/globulin 3.5/4.8 g/dl
SGPT/SGOT 43/26 IU/ml
Creatinine 0.7mg/dl
Urine NAD CXR NAD
ANA 2+ positive
Anti dsDNA >200 IU/dl
IgM ACL 5.6 GPL
IgG ACL 0 MPL
C3 30.6 mg/dl
C4 <5.4 mg/dl
SLE with Cutaneous Vasculitis
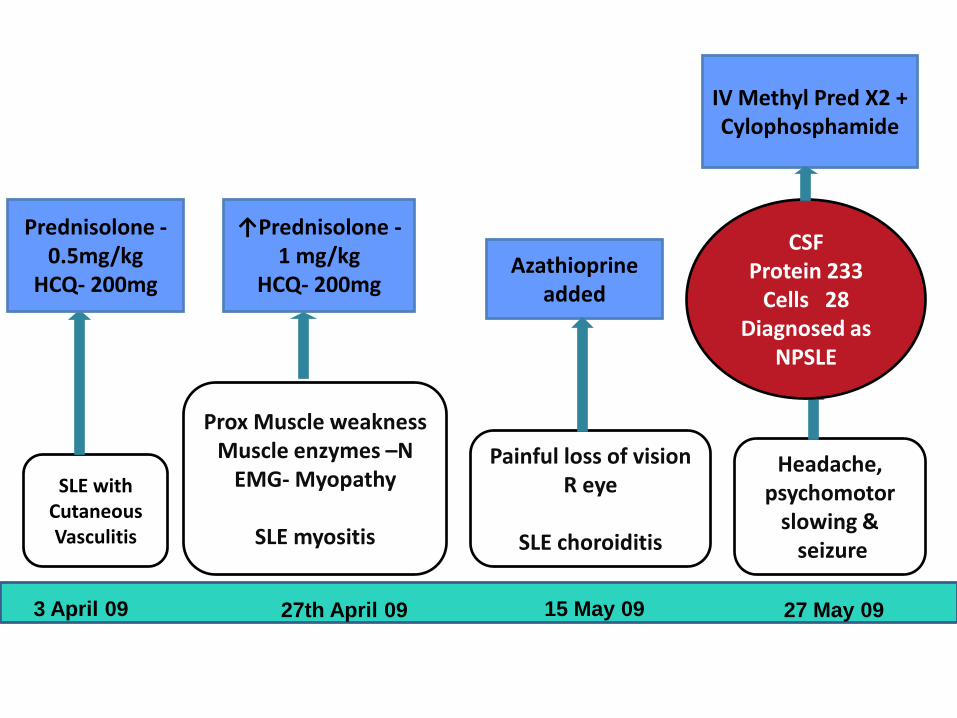
SLE with Cutaneous Vasculitis
Prednisolone -0.5mg/kg
HCQ- 200mg
Prox Muscle weakness Muscle enzymes –N
EMG- Myopathy
SLE myositis
Azathioprine added
↑Prednisolone -1 mg/kg
HCQ- 200mg
Painful loss of vision R eye
SLE choroiditis
Headache, psychomotor
slowing & seizure
CSF Protein 233
Cells 28 Diagnosed as
NPSLE
IV Methyl Pred X2 + Cylophosphamide
3 April 09 27th April 09 15 May 09 27 May 09
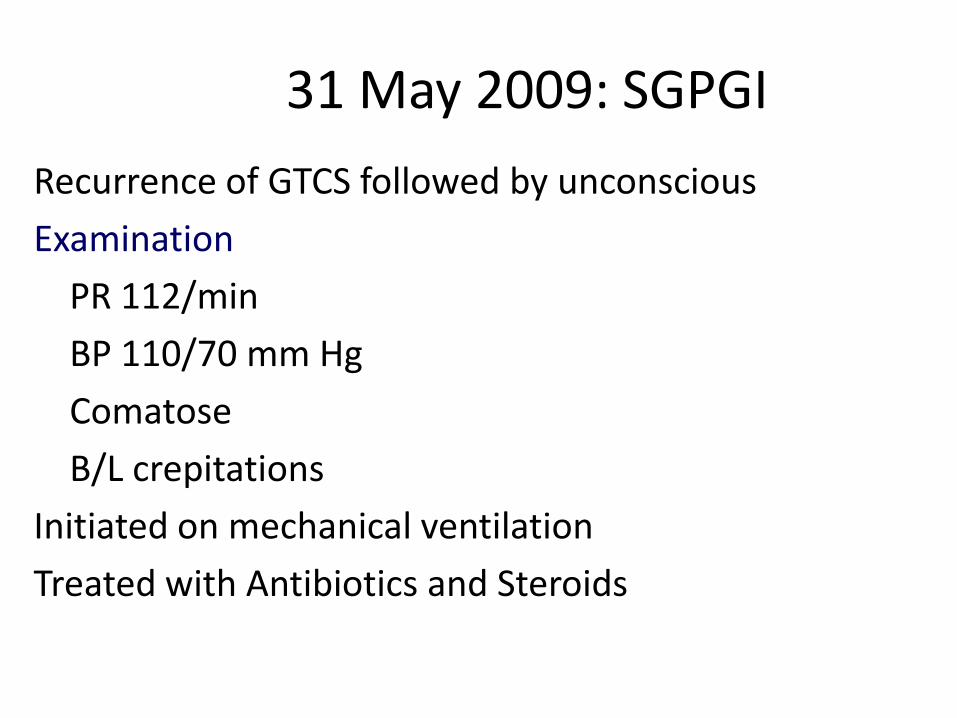
31 May 2009: SGPGI
Recurrence of GTCS followed by unconscious
Examination
PR 112/min
BP 110/70 mm Hg
Comatose
B/L crepitations
Initiated on mechanical ventilation
Treated with Antibiotics and Steroids
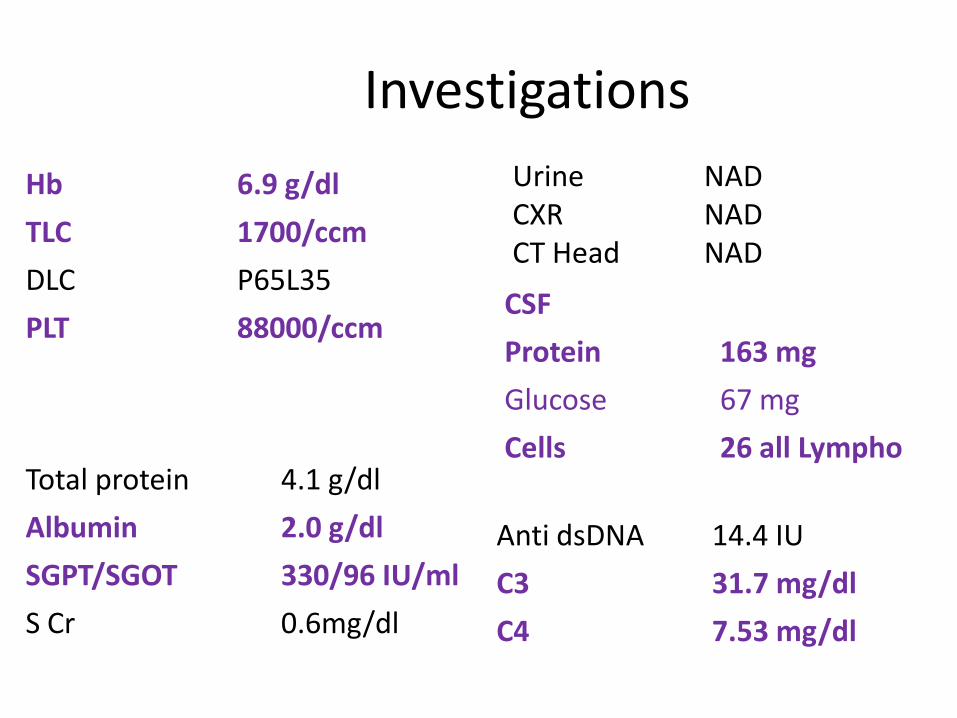
Investigations
Hb 6.9 g/dl
TLC 1700/ccm
DLC P65L35
PLT 88000/ccm
Total protein 4.1 g/dl
Albumin 2.0 g/dl
SGPT/SGOT 330/96 IU/ml
S Cr 0.6mg/dl
Urine NAD CXR NAD CT Head NAD
Anti dsDNA 14.4 IU
C3 31.7 mg/dl
C4 7.53 mg/dl
CSF
Protein 163 mg
Glucose 67 mg
Cells 26 all Lympho
Course
• Day2: Confused, weakness in all 4 limbs LL>UL Rx with IVIG thinking of myositis
• Day 10: Extubated, HZV –V2 and C2, Rx with Acyclovir
• Day15: Persistent diarrhea Rx with antibiotics No improvement in weakness
• Day20: shifted to ward
Course in the ward
• Fever • Abdominal pain, Intermittent diarrhea • Persistent neurological deficit • Disoriented
UL LL Power Grade 3 Grade 0 Pain sensation normal absent DTR normal absent Extensor Plantars Bowel and bladder incontinence
Further evaluation
Stool Examination Normal microscopy, No opportunistic pathogen,
normal flora on culture, Cl difficile antigen negative CT abdomen (to r/o mesentric vasculitis) Normal
Seen by neurologist
?Anoxic encephalopathy with Critical care neuropathy NCV normal MRI Brain few hyper intensities in basal ganglion T2
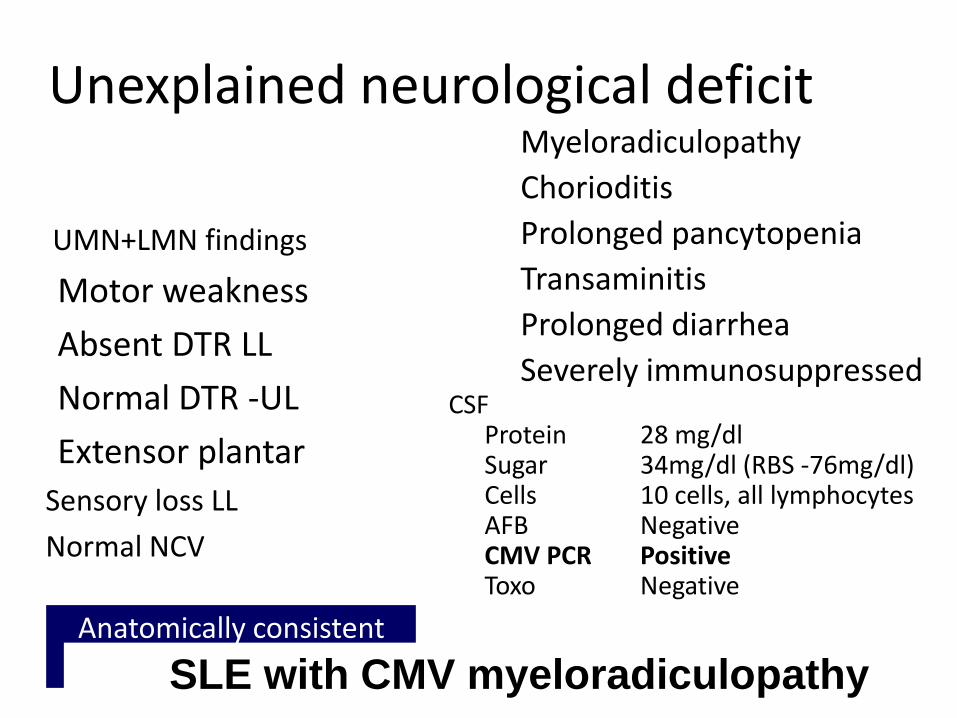
Unexplained neurological deficit
UMN+LMN findings
Motor weakness
Absent DTR LL
Normal DTR -UL
Extensor plantar
Sensory loss LL
Normal NCV
Myeloradiculopathy
Chorioditis
Prolonged pancytopenia
Transaminitis
Prolonged diarrhea
Severely immunosuppressed
CSF Protein 28 mg/dl Sugar 34mg/dl (RBS -76mg/dl) Cells 10 cells, all lymphocytes AFB Negative CMV PCR Positive Toxo Negative
Anatomically consistent with Myeloradiculopathy
SLE with CMV myeloradiculopathy
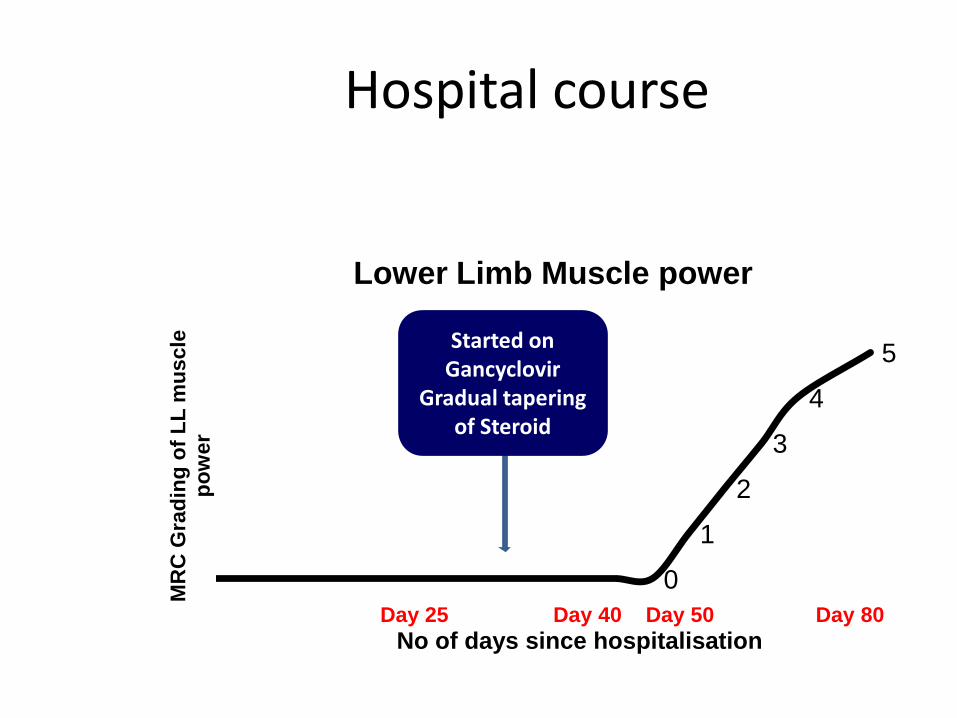
Hospital course
0
1
2
3
4
5
MR
C G
rad
ing
of
LL
mu
scle
p
ow
er
No of days since hospitalisation
Lower Limb Muscle power
Day 25 Day 40 Day 50 Day 80
Started on Gancyclovir
Gradual tapering of Steroid
Follow up
• Completely Recovered
• Completed Graduation
• Regular OPD attendance with a big smile on her face
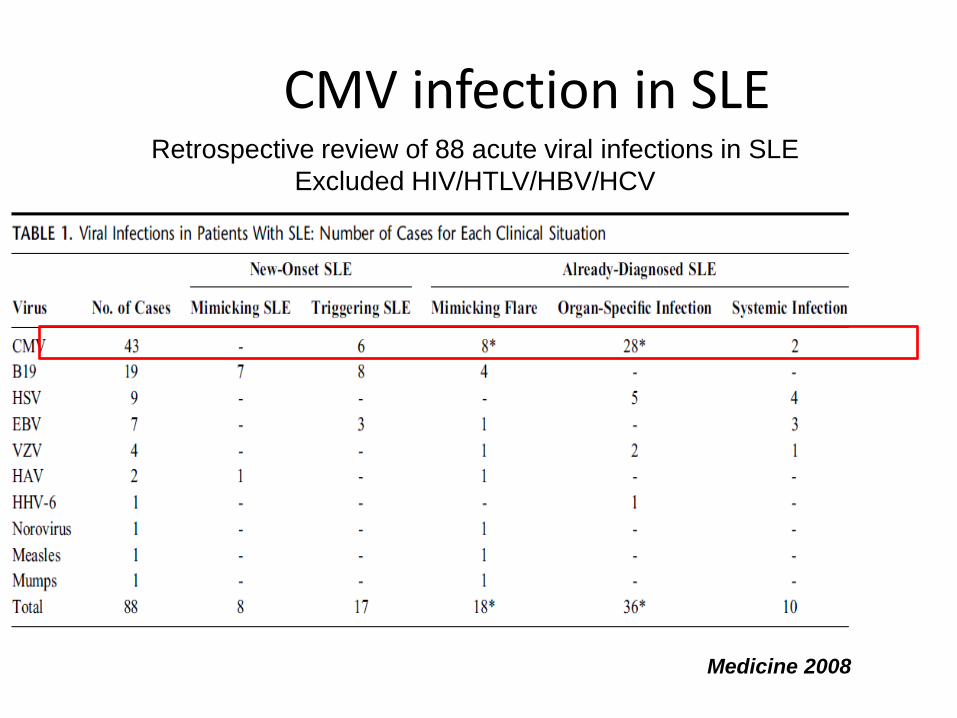
CMV infection in SLE Retrospective review of 88 acute viral infections in SLE
Excluded HIV/HTLV/HBV/HCV
Medicine 2008
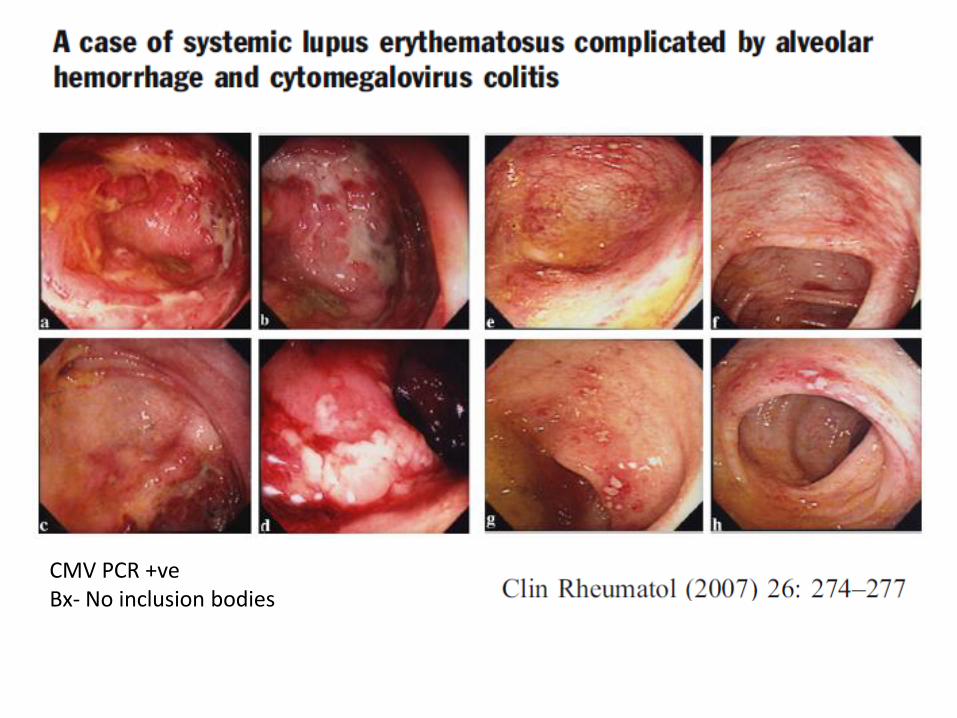
CMV PCR +ve Bx- No inclusion bodies
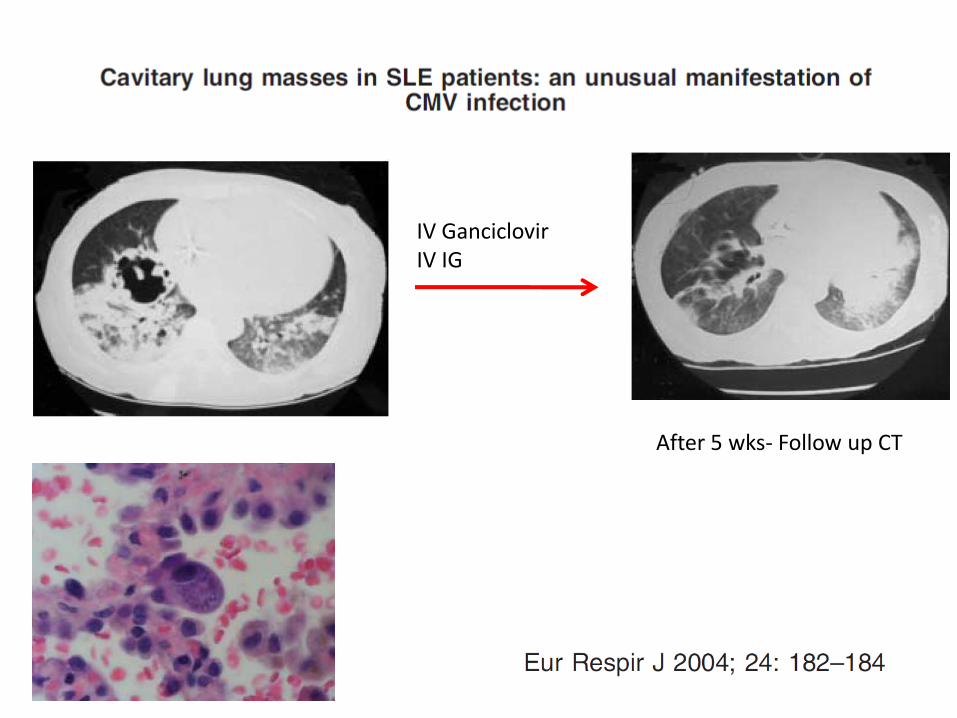
IV Ganciclovir IV IG
After 5 wks- Follow up CT
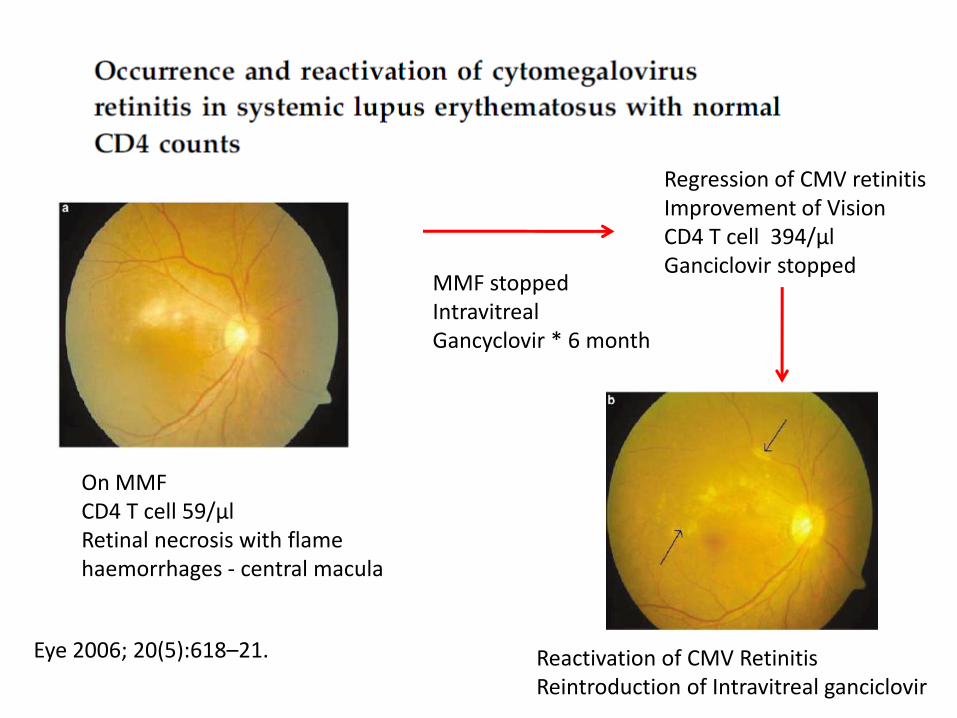
On MMF CD4 T cell 59/µl Retinal necrosis with flame haemorrhages - central macula
MMF stopped Intravitreal Gancyclovir * 6 month
Regression of CMV retinitis Improvement of Vision CD4 T cell 394/µl Ganciclovir stopped
Reactivation of CMV Retinitis Reintroduction of Intravitreal ganciclovir
Eye 2006; 20(5):618–21.
Case 3
27 year old female
August 2009
Fever
Oral ulcers
Malar rash
Photosensitivity
Polyarthritis , alopecia 1 month
7 month
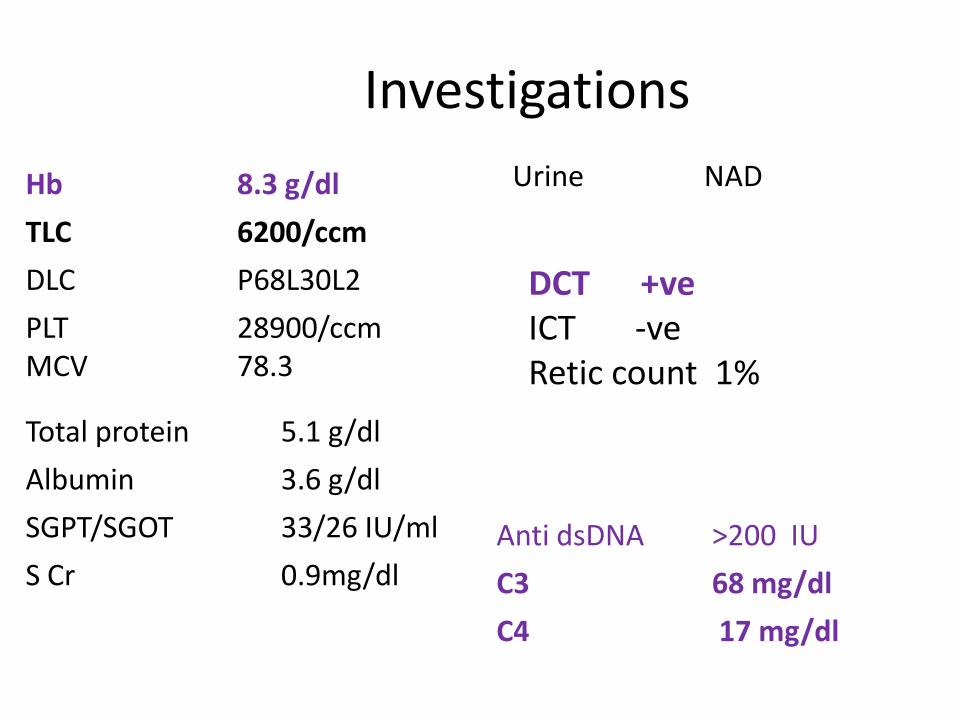
Investigations
Hb 8.3 g/dl
TLC 6200/ccm
DLC P68L30L2
PLT MCV
28900/ccm 78.3 Total protein 5.1 g/dl
Albumin 3.6 g/dl
SGPT/SGOT 33/26 IU/ml
S Cr 0.9mg/dl
Urine NAD
Anti dsDNA >200 IU
C3 68 mg/dl
C4 17 mg/dl
DCT +ve ICT -ve Retic count 1%
SLE with DCT +
anemia
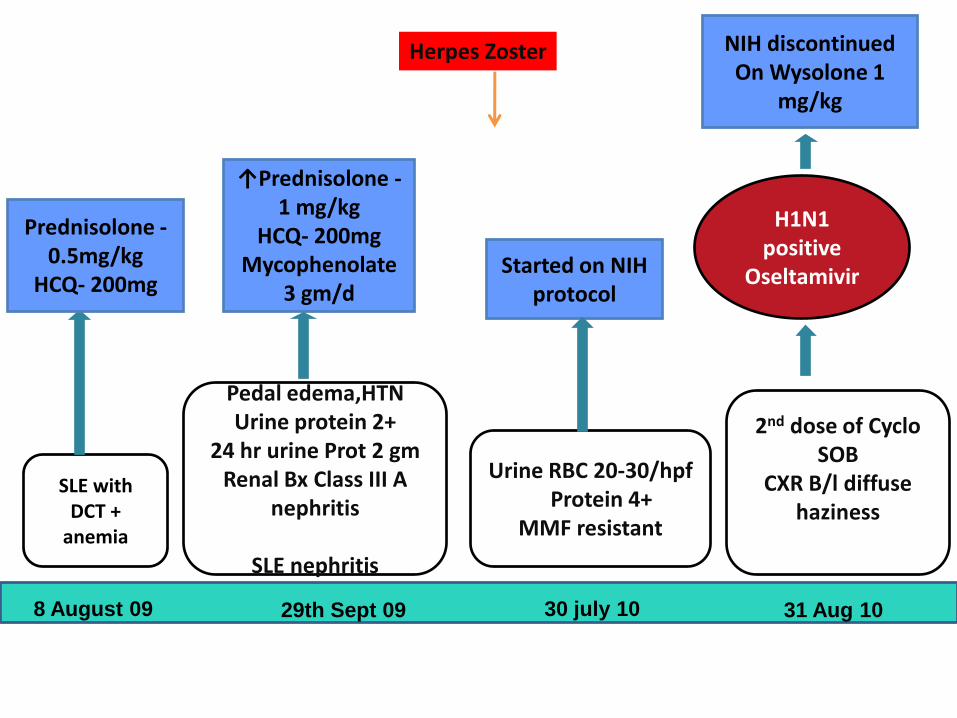
Prednisolone -0.5mg/kg
HCQ- 200mg
Pedal edema,HTN Urine protein 2+
24 hr urine Prot 2 gm Renal Bx Class III A
nephritis
SLE nephritis
Started on NIH protocol
↑Prednisolone -1 mg/kg
HCQ- 200mg Mycophenolate
3 gm/d
Urine RBC 20-30/hpf Protein 4+
MMF resistant
2nd dose of Cyclo
SOB CXR B/l diffuse
haziness
H1N1 positive
Oseltamivir
NIH discontinued On Wysolone 1
mg/kg
8 August 09 29th Sept 09 30 july 10 31 Aug 10
Herpes Zoster
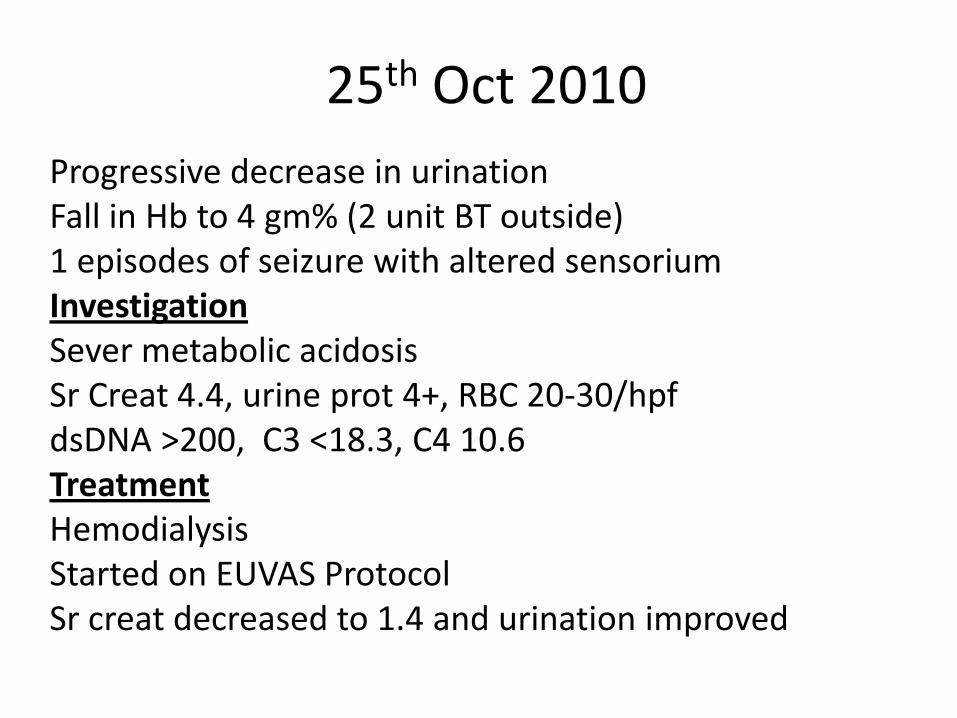
25th Oct 2010
Progressive decrease in urination Fall in Hb to 4 gm% (2 unit BT outside) 1 episodes of seizure with altered sensorium Investigation Sever metabolic acidosis Sr Creat 4.4, urine prot 4+, RBC 20-30/hpf dsDNA >200, C3 <18.3, C4 10.6 Treatment Hemodialysis Started on EUVAS Protocol Sr creat decreased to 1.4 and urination improved
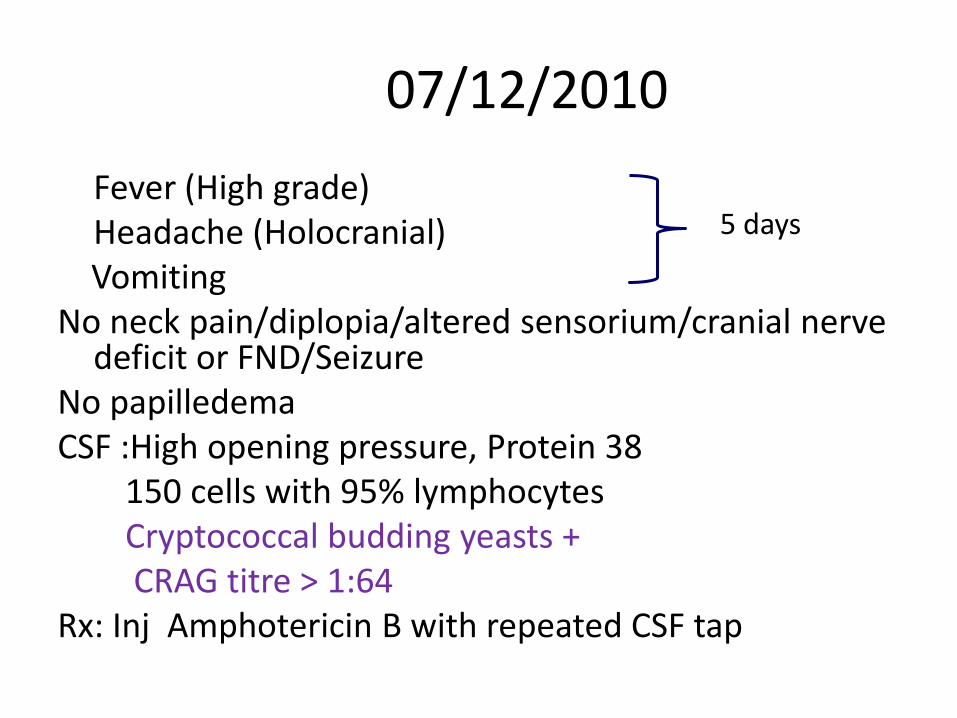
07/12/2010
Fever (High grade) Headache (Holocranial) Vomiting No neck pain/diplopia/altered sensorium/cranial nerve
deficit or FND/Seizure No papilledema CSF :High opening pressure, Protein 38 150 cells with 95% lymphocytes Cryptococcal budding yeasts + CRAG titre > 1:64 Rx: Inj Amphotericin B with repeated CSF tap
5 days
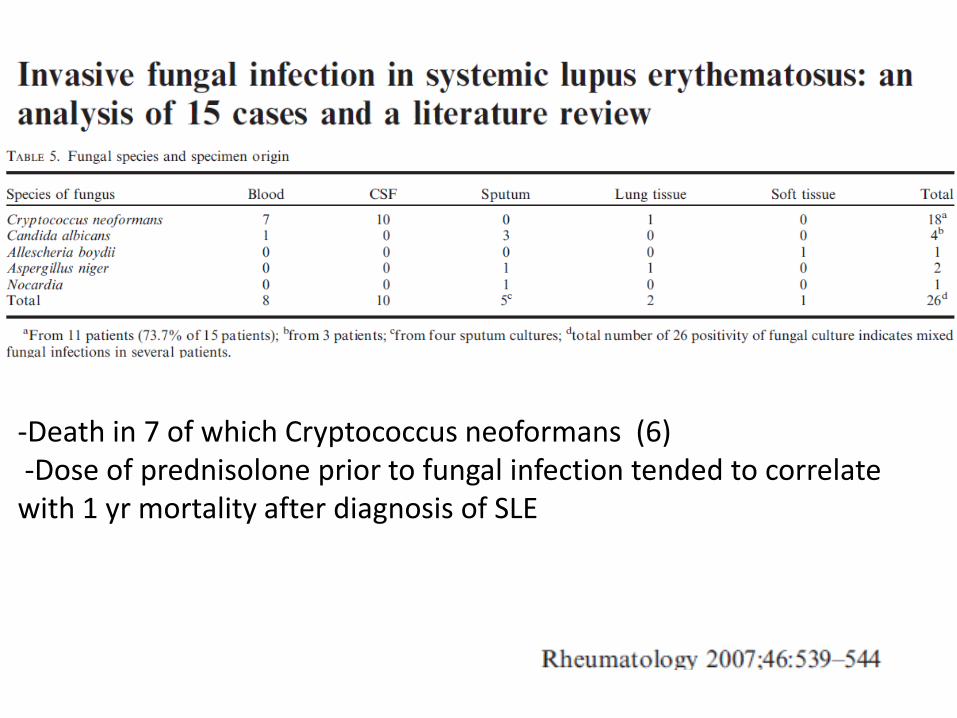
-Death in 7 of which Cryptococcus neoformans (6) -Dose of prednisolone prior to fungal infection tended to correlate with 1 yr mortality after diagnosis of SLE
Meningitis in 5 cases
1 pulmonary cryptococcosis - Died from Resp failure
Induction with amphotericin B
Maintanaince- oral fluconazole indefinitely
None of them has had relapses
Indefinite maintenance therapy with fluconazole is
recommended in SLE patients with cryptococcosis
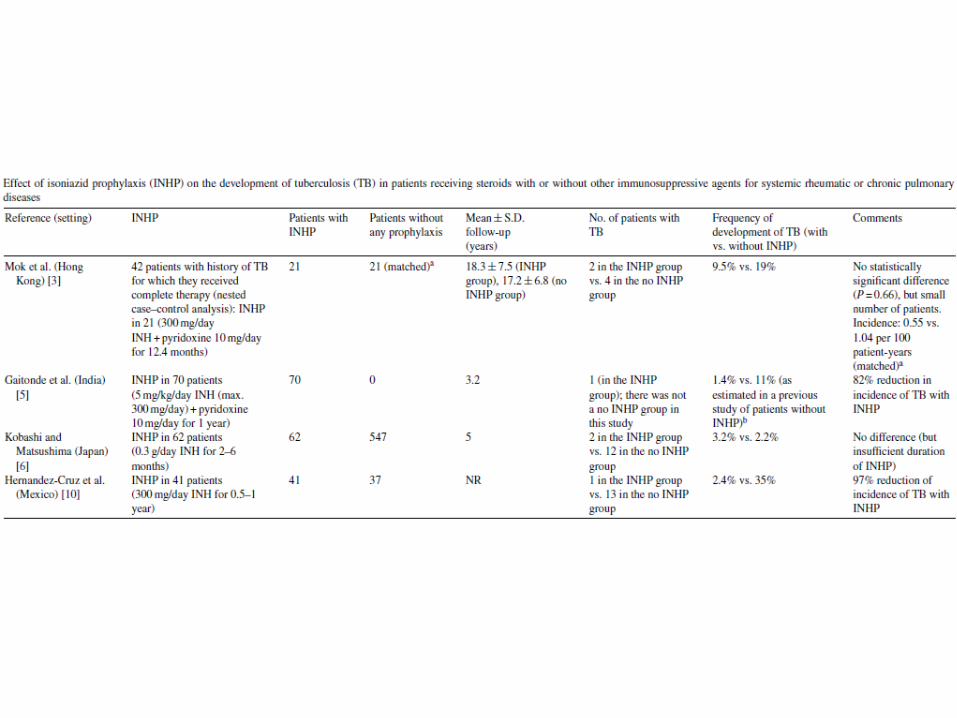
Tuberculosis
• Not unusual in our country
• 11.5% in our center
• Can we prevent it ?
Take home message
• Unusual infections are not so unusual
• Can mimic disease activity
• Early diagnosis and treatment is key
• Need good Microbiology Support
• Most gratifying to treat