Embed Size (px)
Citation preview

1
Unraveling disorders of consciousness: neuroimaging and interpretation
Nicholas D. Schiff, M.D.
Director, Laboratory of Cognitive Neuromodulation
Associate Professor of Neurology and Neuroscience
Department of Neurology and Neuroscience
Weill Medical College of Cornell University
New York, New York
Talk overview• Definitions: global disorders of consciousness
• Evaluation of severely brain-injured patients using neuroimaging methods (positron emission tomography [PET], functional magnetic resonance imaging [fMRI], and diffusion tensor imaging [DTI]):
– Vegetative state (VS) – Minimally conscious state (MCS) – and late emergence from the minimally conscious state
(EMCS)
• Implications for evolving standards of evaluation of DOC:– Need for assessment of risk of misdiagnosis– Frameworks for longitudinal reassessments – Development of guidelines for use of neurodiagnostics

2
Coma:A condition in which the patient remains eyes closed and
cannot be aroused or respond to stimuli.
A result of severe brain injury [or pharmacologic anesthesia].
Comas are invariably transient.
Vegetative state, VS (Jennett and Plum, 1972):
A condition characterize by total unresponsiveness with recoveryof cyclic sleep and wake changes noted as periods of eye opening and eye closure.
A ‘wakeful’ appearing unconscious state associated with severe brain injury.
Definitions

3
Minimally Conscious State, MCS (Giacino et al., 2002):
A condition of severely altered consciousness in which minimal but definite behavioral evidence of self or environmental awareness is demonstrated.
Locked-in State, LIS (Plum and Posner, 1966):
A condition in which the patient may remain eyes closed or open and may not appear to react to stimuli, yet is fully conscious. A result of selective brain injury involving the nerve fibers that control the skeletal muscle system.
Locked-in state is not a disorder of consciousness.
Definitions (continued)
MCS
Cognitive function
Motorfunction
Normal
Total functional loss
VS(PVS)
Coma
Full CognitiveRecovery
Severe to
ModerateCognitive Disability
LIS*
Conceptualizing global disorders of consciousness
Total functional loss
Functional Communication
(Adapted from Schiff, (2004) The neurology of impaired consciousness, In: The Cognitive Neurosciences III, MIT Press)
Braindeath

4
MCS
Cognitive function
Motorfunction
Normal
Total functional loss
VS(PVS)
Coma
Full CognitiveRecovery
Severe to
ModerateCognitive Disability
LIS*
Conceptualizing global disorders of consciousness
Total functional loss
Laureys, Owen, and Schiff (2004) Brain function in brain death, coma, vegetative state, minimally conscious state and the locked-in syndrome. Lancet Neurology, 3(9):537-46.

5
Cerebral metabolism in brain death measured by 18Fluorodeoxyglucose-PET
Laureys, Owen, and Schiff (2004) Brain function in brain death, coma, vegetative state, minimally conscious state and the locked-in syndrome. Lancet Neurology, 3(9):537-46.

6
100
85
75
65
55
Schiff, Ribary, Plum, and Llinas, Words without mind Journal of Cognitive Neuroscience 1999, 11:6; 650-656

7
MCSpatient
Owen AM, Coleman MR, Boly M, Davis MH,
Laureys S, Pickard JD. (2006) Detecting awaren
in the vegetative state. Science. 313:1402.
Clinicalexamination
NeuroimagingResults: Command following,but ??? Level of cognitive function

8
MCS
Cognitive function
Motorfunction
Normal
Total functional loss
VS(PVS)
Coma
Full CognitiveRecovery
Severe to
ModerateCognitive Disability
LIS*
Conceptualizing global disorders of consciousness
Total functional loss
Functional Communication
(Adapted from Schiff, (2004) The neurology of impaired consciousness, In: The Cognitive Neurosciences III, MIT Press)
Braindeath
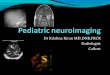
Diffusion Tensor Imaging (DTI)

9
H. U. Voss, A. M. Ulug, R. Watts, L. A. Heier, B. D. McCandliss, S. Niogi, E. J. Kobylarz,J. Giacino,D. Ballon, N. D. Schiff. (2006) Possible axonal regrowth in late recovery from
the minimally conscious state. J Clinical Investigation 16: 2005-2011
Longitudinal measurements of regional fractional anisotropy over an18 month interval following late recovery (20 years after injury)
from MCS
H. U. Voss, A. M. Ulug, R. Watts, L. A. Heier, B. D. McCandliss, S. Niogi, E. J. Kobylarz,J. Giacino,D. Ballon, N. D. Schiff. (2006) Possible axonal regrowth in late recovery from
the minimally conscious state J Clinical Investigation 16:2005-2006

10
Muffled Speech
Reversed Speech
Forward Speech
TW 6 April 2004J. Hirsch et al.
Columbia University fMRI Research CenterColumbia University fMRI Research Center
Isolated residual modular networks
Functional loss of cerebral integration beyond early cortical responses
Preservation of large-scale network responseswith variation in quality of ongoing baseline
brain activation
Conceptual Models of the Spectrum of Vegetative and Minimally Conscious State Patients
? ?
100
85
75
65
55
45
35
Schiff (2005) Progress in Brain Research 150: 477-497

11
0
5
10
15
20
25
30
Mea
n D
RS
Sco
re
1 3 6 12
Months Post Injury
VS NTBI VS TBI MCS NTBI MCS TBI
From “The vegetative and minimally conscious states: A comparison of clinical features and functional outcome, “ J.T. Giacino and K. Kalmar, 1997, Journal of Head Trauma Rehabilitation,12 (4), p. 42.
N=104 (55 VS, 49 MCS)
Conclusions
• Pathological and functional brain imaging studies support a model of widespread cerebral disconnection (functional +/- structural) in VS patients of all causes.
• Atypical behavioral findings in some chronic VS patients may reflect preservation of modular networks. Similarly, recovery of limitedsensorimotor integration in low level MCS may also originate from limited network preservation.
• Some MCS patients, however, retain recruitable large-scale cerebral networks that overlap functionally with normal patterns of activation. These observations require further explanation in terms of mechanism.

12
Conclusions (continued)
• A framework for longitudinal assessments of cerebral function inseverely brain-injured patients should be developed
• Neuroimaging evaluations of patients with severe brain injuries will be impractical until guidelines that are adjusted based on risk of
missing clinical evolution can be developed.
• Guidelines for management of patients with severe brain injuriesshould be developed to identify risk of misdiagnosis or likelihood of significant clinical evolution outside of skilled facilities to reduce potential burden of isolation.
Implications for assessments of severe brain injury:
Conclusions (continued)
• There is a need for rethinking professional standards and ethical obligations to the severely brain injured population
• preserving self-determination, • right-to-die and right-to-care, a• addressing unmet access needs to diagnostic and
therapeutic advances,• defining proportionate palliative goals for patients and
families
• Fins (2003) Constructing a ethical stereotaxy for severe brain injury. Nature Reviews Neuroscience 4:323-327
• Fins JJ. (2005) Clinical Pragmatism and the Care of Brain Injured Patients: Towards a Palliative Neuroethics for Disorders of Consciousness. Progress in Brain Research 150:565-82.

13
Collaborators:Weill Medical College of Cornell University
Jonathan D. Victor, MD, PhDMichael Repucci, PhDJoseph J. Fins, MDFred Plum, MDDaniel G. Herrera, MD, PhDDouglas Ballon, PhDLinda Heier, MDHenning Voss, PhDJohn Dyke, PhDShankar Vallabhajosula, PhDKlaus Hamacher, PhDStanley Goldsmith, MD
Lab. Cognitive NeuromodulationNicholas D. Schiff, MD, DirectorErik Kobylarz, MD, PhDAndrew Goldfine, MDSudhin Thomas, MA
Lab. Visually Guided BehaviorKeith P. Purpura, PhD, DirectorAndrew E. Hudson, BADavid Menzer, BASteven F. Kalik, PhD
Partha Mitra, PhD (CSH Labor.)Hemant Bokil, PhD(CSH Labor.)
Collaborators (continued)
New York University School ofMedicine Center for Neuromagnetism:Urs Ribary, Ph.D.Eugene Kronberg, PhDRodolfo Llinas, MD, PhD
Memorial Sloan Kettering Cancer Center PET Imaging:Ronald Blasberg, MDBradley Beattie, PhD
JFK Johnson Rehabilitation Center:Joseph T. Giacino, PhDCarolyn McCagg, MDKathleen Kalmar, PhD
Functional MRI Laboratory,Columbia University:Joy Hirsch, PhD, DirectorConstance Park, PhDDiana Rodriguez-Moreno, BA
Cleveland Clinic Foundation, Center for Neurological Res.:Ali Rezai, MD, Co-ChairmanCameron McIntyre, PhDChris Butson, PhD

14
AcknowledgementsWe thank
the Charles A. Dana Foundation,
The James S. McDonnell Foundation,
the Cornell-New York Presbyterian Hospital NIH Clinical Research Center,
the National Institutes of Neurological Disease and Stroke(NS02172, NS43451) ,
the National Institute of Mental Health(MH62528-02) ,
the National Institute of Disability and Rehabilitation Research(CFDA 84.133A-5),
for support of these studies.