Embed Size (px)
Citation preview
“Unprofessional and Distressed Resident Physician Behaviors”
Charlene M. Dewey, M.D., M.Ed., FACPAssociate Professor of Medical Education and Administration
Associate Professor of MedicineVanderbilt University School of Medicine
Marshall University Joan C. Edwards School of MedicineAugust 28, 2012
Introduction
• Distressed physicians can have disruptive behavior
• Est. prevalence of disruptive behavior in U.S. MDs is 5% (International similar)
• Focus of attention: disruptive behavior can have destructive impact on:– institutions, staff, and pt care
Samenow, Swiggart, and Spickard. “A CME Course Aimed at Addressing Disruptive Physician Behavior” Physician Executive Jan/Feb, 2008:pg 32-40
Introduction
• Five different state medical societies data demonstrate disruptive behaviors comprise up to 30% of complaints received. *(independent of substance abuse and other forms of impairment)
Samenow, Swiggart, and Spickard. “A CME Course Aimed at Addressing Disruptive Physician Behavior” Physician Executive Jan/Feb, 2008:pg 32-40
Introduction
Disruptive behavior leads to problems with communication which leads to adverse events1
– Communication breakdown factored in OR errors 50% of the time2
– Communication mishaps were associated with 30% of adverse events in OB/GYN3
– Communication failures contributed to 91% of adverse events involving residents4
1) Dayton et al, J Qual & Patient Saf 2007; 33:34-44; 2) Gewande et al, Surgery 2003; 133: 614-621. 3) White et al, Obstet Gynecol 2005; 105(5 Pt1):1031-1038; 4) Lingard et al, Qual Saf Health Care 2004; 13: 330-334
Introduction Case
Your team standing at the nurses’ station blowing off steam after a rough morning. The upper level resident used a particularly graphic and insulting metaphor to describe one morbidly obese and challenging patient. Everyone laughed at the description. The nurse gives a look of disdain and the residents flips her the bird after she turns her head. You are uncomfortable with the resident’s level of professional conduct.
1. Is this blowing off stress or distressed behavior? Why?
2. What do YOU do?
3. What systems exist to help with complaints and interventions?
4. What does the resident need?
5. How does any system promote or dissuade such behavior?
Goals
The purpose of this session is to discuss unprofessional and distressed behaviors of resident physicians and discuss and share resources and tools for identifying and assisting residents in need.
Objectives
Participants of the session will:1. Discuss the behaviors and consequences of
unprofessional and distressed resident physicians.
2. Discuss and share methods for identifying and addressing unprofessional and distressed behaviors during residency.
3. Practice 1 method of communication when approaching residents with unprofessional conduct.
4. Determine if changes are needed to their policy for identifying, addressing and managing unprofessional conduct by resident physicians.
Agenda
1. Introduction
2. Unprofessional and distressed behaviors
3. Methods and tools for identification and intervention
4. Review & practice DRAN and Cup of Coffee Conversations
5. Program/policy assessments
6. Summary
Ground Rules
• Lecture discussion workshop
• Interactive
• Flexible
• Share experiences
• Time limited
Stressed or Disruptive
Is this blowing off s
tress or d
isruptive behavior?
Stress Reactions
Permission to be human!!!
Flooding
1. Neurological and biochemical event2. Triggers3. Sudden onset: “Like an oncoming
truck”4. Inability to self-soothe or self-regulate5. Tend to keep away or isolate
Flooding
• “This means you feel so stressed that you become emotionally and physically overwhelmed…”
• “Pounding heart, sweaty hands, and shallow breathing.”
• “When you’re in this state of mind…you are not capable of hearing new information or accepting influence.”
John M. Gottman, Ph.D. The Relationship Cure, Crown Publishers, New York, 2001, 74-78.
Flooding
• Things to do when you flood:– Step away from the situation: if possible go into
the restroom– Self-sooth: Breathe, relax– Practice mindfulness techniques
• Things to do after you flooded:– Reflection – triggers, symptoms, event– Seek coaching & mentoring
Disruptive Behavior
• “Behavior or behaviors that undermine a culture of safety.”1
• Disruptive behavior is a sentinel event2
1) The Joint Commission's Comprehensive Accreditation Manual for Hospitals, LD.03.01.01, elements of performance (EP) 4 and 5, Spring 2012; 2) Joint Commission, Issue 40 July 9, 2008

Aggressive Passive Passive
Aggressive
Figure 1
Inappropriate anger, threats
Yelling, publicly degrading team members
Intimidating staff, patients, colleagues, etc.
Pushing, throwing objects
Swearing
Outburst of anger &physical abuse
Hostile notes, emails
Derogatory comments about institution, hospital, group,
etc.
Inappropriate joking
SexualHarassment
Complaining,Blaming
Chronically late
Failure to return calls
Inappropriate/inadequate charts
Avoiding meetings & individuals
Non-participation
Ill-prepared, not prepared
Swiggart, Dewey, Hickson, Finlayson. “A Plan for Identification, Treatment, and remediation of Disruptive Behaviors in Physicians.” Frontier's of Health Services management, 2009; 25(4):3-11.
Spectrum of Disruptive Behaviors
Etiology of Distressed Behaviors
Individual Factors:• Psychological Factors1:
– Substance use/abuse, FHx, trauma history, religious fundamentalism, familial high achievement
• MH issues2: – Personality disorders,
narcissism, depression, bipolar, OCD, etc.
• Genetic/developmental issues: – Asperger’s, non-verbal
learning differences, etc.
• Family systems• Stress/physiologic
reactions• Burnout3
• Reduced wellness
1) Valliant, 1972; 2) Gabbard, 1985; 3) Spickard and Gabbe, 2002
Etiologies of Distressed Behaviors
Institutional Factors:– Scapegoats– System reinforces Behavior– Individual pathology may over-shadow
institutional pathology
Williams and Williams, 2004 Sutton, R. “The No Asshole Rule: Building a Civilized Workplace and Surviving on the Isn’t.” Business Plus, New York, 2007
Risk Factors
• Personality types• Lack of self-awareness• Lack of emotional intelligence• Training/experience• Lack of training in coping skills and stress
management• Lack of training dealing with conflict• Your family system• Poor self-care
Introduction Case
What do YOU do?
Warning
Do Nothing Immediate Intervention Report
Lack of authorityLack of protectionUnclear process
Risk of retribution/retaliationLetters of recommendation in future
Concerns of own deficiencies
Barriers to Action
• Fear
• Loyalty
• Culture
• Lack of training
Hickson et al. “The why and how of dealing with special colleagues: discouraging disruptive behaviors.” Center for Patient and Professional Advocacy, Vanderbilt University School of Medicine, October 28-9, 2010.
Reluctance to “betray’Potential loss of recog/reputationImplications for patients loyaltiesLack of incentive to do right
Misuse of informationNeeds a scapegoatLack of…
Conflict management skillsAssertiveness training
Communication training
Assertive Communication
• When asking for something, use the acronym – DRAN
Describe
Reinforce
Assert
Negotiate
Swiggart et al. “Program for Distressed Physicians”, Center for Professional Health, Vanderbilt University School of Medicine.
Describe
• Describe the other person’s behavior objectively – use reflective “I”
• Use concrete terms
• Describe a specified time, place & frequency of action
• Describe the action/behavior, not the “motive”
• Be respectful but avoid minimizing
Swiggart et al. “Program for Distressed Physicians”, Center for Professional Health, Vanderbilt University School of Medicine.
Reinforce
• Recognize the other person’s past efforts• Remember: It takes eight positive comments to
compensate for one negative comment.
Swiggart et al. “Program for Distressed Physicians”, Center for Professional Health, Vanderbilt University School of Medicine. & John Gottman, Ph.D. The Relationship Cure. Crown Publishers, New York, 2001, 74-78
Assert Directly and Specifically
• Express your feelings
• Express them calmly
• State feelings in a positive manner
• Direct yourself to the offending behavior, not the entire person’s character
• Ask explicitly for change in the other person’s behavior
Swiggart et al. “Program for Distressed Physicians”, Center for Professional Health, Vanderbilt University School of Medicine.
Negotiate
• Work toward a compromise that is reasonable
• Request a small change at first• Take into account whether the person can
meet you needs or goals• Specify behaviors you are willing to change• Make consequences explicit• Reward positive changes
Swiggart et al. “Program for Distressed Physicians”, Center for Professional Health, Vanderbilt University School of Medicine.
Tips
• If flooding – make an escape!• Listen• Avoid judgment• Be empathetic but don’t join the pity party• Beware the 7 traps:
• Pulling rank • Expectation of thanks• Adopting their role • Fail to deliver the message• Control contest • Fail to recognize self-issues• Giving to much advice
• End positively
Specific Phrases
• I am coming to you as a colleague.• You are a valued member of the team.• I hear and saw the event…• You may be right.• I know this may be frustrating.• I want to address some concerns I have.• Give me a minute, I’ll get right back to you.
Swiggart et al. “Program for Distressed Physicians”, Center for Professional Health, Vanderbilt University School of Medicine.
Practice DRAN
• Role plays• Use the introduction case• Each person takes turn practicing
DRAN; then switch• You are practicing – mistakes are
ok.• Person listening assess other’s
performance & provides feedback
Dewey et al. “Teaching Professionalism” EDP Workshop, Vanderbilt University School of Medicine, April 2010.
Introduction Case
What systems exist to help with complaints and interventions?
What do we do well?
Introduction Case
What does the resident need?
ACGME
ACGME Competency-Professionalism: Residents must demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles, and sensitivity to a diverse patient population. Residents are expected to:
• demonstrate respect, compassion, and integrity; a responsiveness to the needs of patients and society that supersedes self-interest; accountability to patients, society, and the profession; and a commitment to excellence and on-going professional development
• demonstrate a commitment to ethical principles pertaining to provision or withholding of clinical care, confidentiality of patient information, informed consent, and business practices
• demonstrate sensitivity and responsiveness to patients’ culture, age, gender, and disabilities
Interventions
• Education– Clear policy
– Rules/regulations
– Ethics/professionalism
– Self-care
• Training & coaching• Assessments (burnout, MH, SU, FFD, BVI, FOO, etc.)
• Monitoring (B29-BMT, pt surveys, intent to change)
• Experiences – witness doing right (role models)
• Emotional intelligence• Referrals
Interventions
• Internal vs. external referrals– EAP– Fitness for duty assessments (MH, SU)
– State physician health program– Out of state programs (education, training, treatment)
Emotional Intelligence
• Self-awareness
• Self-regulation
• Motivation
• Empathy
• Social skills
Goleman, D. “What makes a leader?” HBR 1998:82-91
Self-Awareness
• “First, people need self-awareness to reflect on their behaviors, including their emotional displays, so as to judge them against group norms.”
• “…encourages people to reflect on their actions and understand the extent to which those actions match both personal values and beliefs as well as group standards.”
• How do you teach self-awareness?
Heatherton, TF. “Neuroscience of Self and Self-Regulation.” Annu Rev Psychol 2011:62:363-90.
Self-Regulation
• “The process by which people change thoughts, feelings, or actions in order to satisfy personal and society goals and standards.”
• “Self-regulation involves both the initiation and maintenance of behavioral change in addition to inhibiting undesired behaviors or responding to situational demands.”
• How do you teach self-regulation?
Heatherton, TF. “Neuroscience of Self and Self-Regulation.” Annu Rev Psychol 2011:62:363-90.
Introduction Case
How does any system promote or dissuade such behavior?
Disruptive Behaviors
CycleHorizontal Hostility
PoorCommunication
Reduced PtSafety
Lost of Finances& Reputation
Staff Turnovers
Increase Liability and Risk
Poor Work Environment
Samenow, Swiggart, and Spickard. “A CME Course Aimed at Addressing Disruptive Physician Behavior” Physician Executive Jan/Feb, 2008:pg 32-40; Felps, W et al. How, when, and why bad apples spoil the barrel: negative group members and dysfunctional groups. Research and Organizational Behavior, 2006; 27:175-222.
Failure to Address
• Disruptive behavior leads to problems with communication which leads to adverse events1
– Communication breakdown factored in OR errors 50% of the time2
– Communication mishaps were associated with 30% of adverse events in OBGYN3
– Communication failures contributed to 91% of adverse events involving residents4
1. Dayton et al, J Qual & Patient Saf 2007; 33:34-44. 3. White et al, Obstet Gynecol 2005; 105(5 Pt1):1031-1038.2. Gewande et al, Surgery 2003; 133: 614-621. 4. Lingard et al, Qual Saf Health Care 2004; 13: 330-334
Failure to Address
• Team members may adopt disruptive person’s negative mood/anger (Dimberg & Ohman, 1996)
• Lessened trust leads to lessened task performance & effects quality and pt safety (Lewicki & Bunker,
1995; Wageman, 2000)
• High turnover• Pearson et al, 2000 found that 50% of people who were targets
of disruptive behavior thought about leaving their jobs• Found that 12% of people actually quit
• These results indicate a negative effect on return on investment
Felps, W et al. 2006. How, when, and why bad apples spoil the barrel: negative group members and dysfunctional groups. Research and Organizational Behavior, Volume 27, 175-222.
Joint Commission
Goals:1. Reform health care settings to address the
problem (history of tolerance and indifference)
2. Promote a culture of safety
3. Improve the quality of patient care by improving the communication and collaboration of health care teams
Gundersen, DC. “The Disruptive Physician” Federation of State Physician Health Programs (FSPHP) Annual Meeting Chicago, IL 2010.

The Joint Commission
Requirements:1. EP 4: The hospital/organization has a code of
conduct that defines acceptable and disruptive and inappropriate behaviors.1
2. EP 5: Leadership create and implement a process for managing disruptive and inappropriate behaviors1
• Multiple levels of leadership• Professional/leader training• E.g., CPPA – PARS® at Vanderbilt2
1) The Joint Commission. “Behaviors that undermine a culture of safety.” Issue 40, July 9, 2008 and 2) Center for Patient and Professional Advocacy – Patient Advocacy Reporting System. http://www.mc.vanderbilt.edu/centers/cppa/
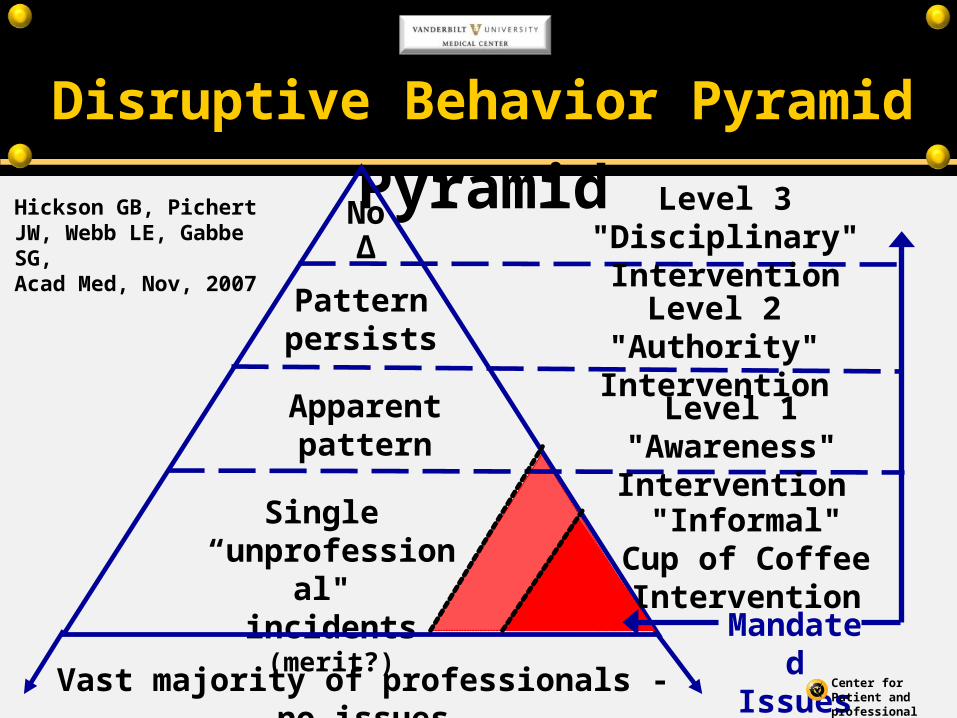
Apparent pattern
Single “unprofessional" incidents (merit?)
Disruptive Behavior Pyramid
Mandated Issues
"Informal" Cup of Coffee Intervention
Level 1 "Awareness" Intervention
Level 2 "Authority" Intervention
Level 3 "Disciplinary" Intervention
Pattern persists
No ∆
Vast majority of professionals - no issues
Hickson GB, Pichert JW, Webb LE, Gabbe SG,Acad Med, Nov, 2007
Center for Patient and professional Advocacy at Vanderbilt
Disruptive Behavior Pyramid
The Joint commission
11 Suggestions:1. Educate all team members
2. Hold all team members accountable
3. Develop and implement policies and procedures/processes
4. Develop an organizational process for addressing intimidating and disruptive behaviors
5. Provide skills-based training and coaching for all leaders/managers
6. Develop and implement a system for assessing staff perceptions
The Joint Commission. “Behaviors that undermine a culture of safety.” Issue 40, July 9, 2008
The Joint Commission
7. Develop and implement a reporting/ surveillance system (possibly anonymous) for detecting unprofessional behavior.
8. Support surveillance with tiered, non-confrontational interventional strategies
9. Conduct all interventions within the commitment to the health and well-being of all staff,
10. Encourage inter-professional dialogues
11. Document all attempts to address behaviors
The Joint Commission. “Behaviors that undermine a culture of safety.” Issue 40, July 9, 2008
Recap Intro Case
1. Is this blowing off stress or distressed behavior? Why?
2. What do YOU do?
3. What systems exist to help with complaints and interventions?
4. What does the resident need?
5. How does any system promote or dissuade such behavior?
Take Home Points
1. Disruptive and unprofessional behaviors have significant consequences for many individuals and the institution and thus should not be ignored.
2. Physicians demonstrate unprofessional and disruptive behaviors for many reasons.
3. Provide means for remediation through assessments, education, training, monitoring, self-improvement, role modeling, and referrals.
4. Policies and codes of conduct should be implemented and made clear for all those working within the institution.
Summary
1. Discussed behaviors and consequences of unprofessional and distressed resident physicians.
2. Discussed and shared methods for identifying and addressing unprofessional and distressed behaviors during residency.
3. Practiced 1 method of communication (DRAN) when approaching residents with unprofessional conduct.
4. Determined if changes are needed to the policy for identifying, addressing and managing unprofessional conduct by resident physicians.





























