Embed Size (px)
Citation preview

Unlock the Secret to E/M Coding: Medical Necessity Skills for Coders
2014AAPC2480 South 3850 West, Suite BSalt Lake City, Utah 84120800-626-CODE (2633), Fax 801-236-2258www.aapc.com
AAPC Workshops


Unlock the Secret to E/M Coding: Medical Necessity Skills for Coders
By Stephanie Cecchini, CPC, CEMC, CHISP, Approved ICD-10 Trainer

ii AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Introduction
AAPC Disclaimer This course was current at the time it was published. This course was prepared as a tool to assist the participant in under-standing the concepts of Medical Necessity in Evaluation and Management (E/M) coding and is not intended to grant rights or impose obligations. Although every reasonable effort has been made to assure the accuracy of the information within these pages, the ultimate responsibility for the correct submission of claims and response to any remittance advice lies with the provider of services.
AAPC agents, writers, contributors, contractors, employees and staff make no representation, warranty, or guarantee that this compilation of information is error-free and will bear no responsibility or liability for the results or consequences of the use of this course. This guide is a general summary that explains commonly accepted aspects of selecting E/M codes, but it is not a legal document.
Viewpoints are discussed from the standpoint of the 1995 and 1997 Centers for Medicare and Medicaid Services (CMS) Evaluation and Management Documentation Guidelines with Medical Necessity and the nature of the presenting problem as the primary criterion of code selection (Medicare Claims Processing Manual Chapter 12 - Physicians/Nonphysician Practitioners, 30.6.1 - Selection of Level of Evaluation and Management Service, A. Use of CPT® Codes.)
For the purpose of objective consistency, specific logics are primarily based on the same used by the E/M Documenta-tion Auditors’ Worksheet, Marshfield Clinic, available through the Medical Group Management Association (MGMA). Specific payers, including Medicare Carriers, may use different and sometimes varied audit tools logics to gain objective consistency around the 1995 and 1997 Documentation Guidelines. Official provisions are contained in the relevant laws, regulations, rulings and contractual agreements of providers.
US Government RightsThis product includes CPT®, which is commercial technical data and/or computer data bases and/or commercial com-puter software and/or commercial computer software documentation, as applicable, which was developed exclusively at private expense by the American Medical Association, 515 North State Street, Chicago, Illinois, 60610. U.S. Government rights to use, modify, reproduce, release, perform, display, or disclose these technical data and/or computer data bases and/or computer software and/or computer software documentation are subject to the limited rights restrictions of DFARS 252.227-7015(b)(2) (November 1995), as applicable, for U.S. Department of Defense procurements and the limited rights restrictions of FAR 52.227-14 (June 1987) and/or subject to the restricted rights provision of FAR 52.227-14 (June 1987) and FAR 52.227-19 (June 1987), as applicable, and any applicable agency FAR Supplements, for non-Department of Defense Federal procurements.
AMA DisclaimerCPT® copyright 2013 American Medical Association. All rights reserved.
Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT®, and the AMA is not recommending their use. The AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for data contained or not contained herein.
CPT® is a registered trademark of the American Medical Association.
The responsibility for the content of any “National Correct Coding Policy” included in this product is with the Centers for Medicare and Medicaid Services and no endorsement by the AMA is intended or should be implied. The AMA disclaims responsibility for any consequences or liability attributable to or related to any use, nonuse or interpretation of information contained in this product.
It is recommended that the participant of this course will familiar with:
z CMS 1995 Documentation Guidelines for Evaluation and Management Services z CMS 1997 Documentation Guidelines for Evaluation and Management Services

Unlock the Secret to E/M Coding www.aapc.com iii
Introduction
About the Author:Stephanie Cecchini, CPC, CEMC, CHISP, Approved ICD-10 Trainer, VP Coding Operations joined Aviacode in 2012 where she continues her commitment to best serve the revenue cycle management needs of physicians and the healthcare community. She is an executive Level consultant with significant healthcare business experience. Stephanie is an expert in clinical documentation requirements for coding and billing to Medicare, Medicaid and all lines of commercial payer busi-ness. She brings to her position more than 18 years’ involvement in healthcare regulations including: coding and billing compliance, HIPAA privacy, security, and transactions, and HITECH “meaningful use” compliance. Previously, Stephanie served as SVP at the American Society of Health Informatics Managers, working to fill the needs of physicians adopt-ing Health IT and at its sister organization, AAPC as VP, Product Management. In prior roles she served as Chief Audit Officer for Parses, Inc., designing audit programs for payers and managing overpayment recovery. As a public speaker and published writer, she is a nationally respected advocate of fair and proper payment for medical services. Stephanie lives in Salt Lake City, Utah with her husband Jim and their three children. Stephanie is LION (Linked In Open Network). Please feel free to connect with her at: http://www.linkedin.com/in/stephaniececchini
Notice Regarding Clinical Examples Used in this BookAAPC believes it is important in training and testing to reflect as accurate a coding setting as possible to students and examinees. All examples and case studies used in our study guides and exams are actual, redacted office visit and proce-dure notes donated by AAPC members.
To preserve the real world quality of these notes for educational purposes, we have not rewritten or edited the notes to the stringent grammatical or stylistic standards found in the text of our products. Some minor changes have been made for clarity or to correct spelling errors originally in the notes, but essentially they are as one would find them in a coding setting.
© 2014 AAPC2480 South 3850 West, Suite B, Salt Lake City, Utah 84120800-626-CODE (2633), Fax 801-236-2258, www.aapc.com
All rights reserved.CPC®, CPC-H®, CPC-P®, CIRCC®, CPCOTM, and CPMATM are trademarks of AAPC.


Unlock the Secret to E/M Coding www.aapc.com v
Contents
Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Chapter 1: Refresher—Code Selection by Documentation Markers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3History of Present Illness: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Review of Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Past, Family & Social History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Physical Exam . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5The CMS 1995 Documentation Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
The CMS 1997 Documentation Guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Medical Decision Making (MDM) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5The Number of Diagnoses and Management Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Amount and/or Complexity of Data to be Reviewed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Risk Significant Complications, Morbidity, and/or Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Chapter 2: Medical Necessity—What is it? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Chapter 3: How Sick is Sick? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Nature of the Presenting Problem and Medical Necessity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
MDM and Medical Necessity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7Example: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Chapter 4: Who Says How Sick Is Sick? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Relating Medical Necessity to Coding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Medical Necessity “Faces” E/M Coding Scale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Sick: Level Three Outpatient (Level One Inpatient) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
Sicker: Level Four Outpatient (Level Two Inpatient) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
Sickest: Level Five Outpatient (Level Three Inpatient) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
Communicating Effectively with Documenting Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Chapter 5: Combining ICD-10 CDI Training Sessions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
Chapter 6: Mastering a Good Coder-Physician Relationship . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
Let’s Help! . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
References Cited . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Appendix A: E/M Code Selection (Reference Sheet) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19

vi AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Contents
Appendix B: Medical Necessity Flow Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Appendix C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Slide Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 1
SummaryEvaluation and management (E/M) codes are the most commonly billed codes. Although there are guidelines to proper E/M code selection, Medical Necessity is the pri-mary driver of correct coding. We are told that a physician may take a full history and provide a full physical, but without medical need to back it up…we should select a lesser code. For example, a resolved contact dermatitis with no other problem or complaint, is not a Level Five service because there is no need for a full Level Five service. It is a coder’s responsibility to verify that the diagnosis in the chart supports the procedure being billed. The question becomes: How does a coder, who is not medical peer, chal-lenge the questions of Medical Necessity when the reason for the services are NOT so black and white? And, the largest shade of grey, what supports a Level Three versus a Four? This workshop will provide you with the insights necessary to unlock the secret of accurate E/M coding by introducing the skills needed to accurately identify and effectively address Medical Necessity concerns.
IntroductionE/M codes, the codes that bill for patient visits, are subjec-tive in nature. One of the biggest conundrums faced by coders is Medical Necessity in E/M coding. Legally, the CMS 1995 and 1997 Documentation Guidelines are not statutes, and they are interpretive and arguable. Medical need for services rendered is the authoritative and winning factor.
From the aspect of Medical Necessity, the correct level of service is determined simply by how sick a patient is. Conditions that pose an immediate threat to life or bodily function qualify for the highest code Level, whereas patients with minor or well controlled problems are at the lowest.
A coder may review a document and establish that a com-prehensive service was rendered; however, a medical review may find the same service lacking in necessity. A compre-hensive service may be a physician’s personal art and style of practice but may not be considered necessary and bill-able by a majority of his or her peers. For example, a com-prehensive history and physical may not be necessary to repeat on a two week follow-up visit to check the patient’s normal blood pressure.
This is a problem that only asserts itself in the healthcare industry, but it is rather like pulling in for an oil change…
and then also being charged for new wiper blades, fans, and a transmission flush – all before manufacturer recom-mendation - and without being asked first. Although the services were rendered, and might even be superior to the services by the mechanic down the street…but they were unnecessary per industry standards. The customer might complain and feel cheated. In the world of healthcare, payers are required to guard against medically unnecessary services.
In its annual financial report, the Department of Health and Human Services disclosed Medicare fee-for-service improper payments increased by 18 percent to total some $36 billion during the 2013 fiscal year, which ended in September . The report finds that the primary cause of improper Medicare Fee for Service (FFS) payments is Administrative and Documentation errors (63 percent), in large part due to insufficient documentation. The other cause of improper payments is classified as Medical Neces-sity errors (37 percent), caused by medically unnecessary services.
Accurate E/M coding requires interpretation of docu-mented medical records---followed by code look up and knowledge of coding rules. Certified coders are well equipped to define clinical documentation insufficiency errors and to educate our physicians to improve. However, Medical Necessity issues are a different story. A coder might code correctly per the rules of documentation requirements …however, still miscode the service if they incorrectly interpret the severity of the patient’s problem as compared to proper payment.
The problem many coders have is that they are not medi-cal peers to physicians. Challenging the medical need for services is not appropriate, even though they are often required to make decisions that involve it. Coding auditors without access to a Medical Director or other peer are even more disadvantaged.
Although many coders are good at identifying a Medical Necessity concern, they are often uncertain about how to respond to it. Because the vast majority of medical coders are not physicians or qualified to act as a medical peer in making Medical Necessity determinations -and may be worried about the implications of querying the physician. A wrong step can lead to significant barriers in the coder-physician relationship.
Yet coder silence can be damaging. Concerns left unvoiced may lead to over-payments and risk of negative payer audits, which are projected to rise in 2014. In fiscal year

Unlock the Secret to E/M Coding
2 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
(FY) 2013, CMS reported an error rate of 10.1 percent for Medicare Fee-for-Service. This exceeds the 10 percent threshold set by the Improper Payments Elimination and Recovery Act of 2010 (IPERA) and is an increase from FY 2012. Exacerbating the problem, EHR templates are in growing use. These templates are known to increase the likelihood of artificially inflated codes due to expanded documentation that is not supported by Medical Necessity. This type of “false positive” code can be costly on payer audit. The bottom line is: no one can afford to make a mistake.
This workshop is designed to make the topic of Medical Necessity less intimidating for coders. It also teaches you how to connect with documenting physicians to make E/M coding easier, audit ready, and accurate for fair pay-ment. Maybe even...fun!
In this workshop, you will learn:
z Three little known secrets to accurate E/M coding z The definitions of Medical Necessity for purposes of accurate coding
z How to clinically differentiate E/M service Levels z Effective techniques for communication with physi-cians regarding Medical Necessity

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 3
Chapter 1: Refresher— Code Selection by Documentation MarkersThis workshop will first review the documentation require-ments to ensure that this foundation is addressed. If you are an E/M documentation requirements expert, skip to Chapter 2: Medical Necessity – What is it?
The CMS 1995 and 1997 Documentation Guidelines are defined methods to determine the correct code for a patient visit. If all work that is documented is Medically Necessary, these guidelines serve to select a correct Level of service. In most cases, the E/M code is calculated by fol-lowing relational rules from three parent tables (together called the “Key Components”). Each of these three tables has child variables that are considered by themselves and then together before selecting the final E/M code.
The Key Components
1. History
History of Present Illness (HPI)
Review of Systems (ROS)
Past, Family and Social History (PFS)
2. Exam
3. Medical Decision Making
Number of Diagnoses and Treatment Options
Amount and Complexity of Data
Overall Risk
History There are sub components, which could be thought of as “child variables” to measuring the amount of physician’s work in taking a patient’s medical history. These are: His-tory of Present Illness (HPI), Review of Systems (ROS), and Past, Family Social History (PFS).
History of Present Illness: The patient’s EXPLANATION of what brought them to the PHYSICIAN
z LOCATION: For example “chest” pain, sore “knee”, etc. z SEVERITY: A statement of degree or measurement regarding how “bad” it is… that it is improved, it is extreme pain, “Blood Sugar is 200,” feeling “better,” pain is bad enough “that the patient can’t sleep” etc.
z TIMING: A measurement of when or at what fre-quency; i.e. “intermittent,” “constant,” in the “morn-ing,” lasted “5 minutes,” “occasional,” “on and off,” etc.
z ASSOCIATED SIGNS AND SYMPTOMS: Any associated or secondary complaints.
z MODIFYING FACTORS: Anything that makes the problem better or worse, a factor that changes, improves, or alters the problem. For example, improved “with Tylenol,” worse “when standing,” better “when resting,” “calms down when mother feeds her”
z CONTEXT: What the patient was doing, the envi-ronmental factors/circumstances surrounding the com-plaint, for example, “while sleeping,” “MVA,” “slipped and fell,” after “eating peanuts,” “while dusting,” “when arguing with his wife,” etc.
z DURATION: A measurement of time regarding when the complaint first occurred. For example, began “in childhood,” “since 1995,” first noticed “2 weeks” ago, “symptoms x 3d,” etc.
z QUALITY: Any characteristic about the problem and/or expresses an attribute. For example: how it looks or feels; for example. “green” phlegm, “popping” knee, “dull” ache, “sharp” pain, “metallic” taste, etc.
Review of SystemsThe review of system (ROS) is an account of body systems obtained through a series of questions seeking to spot signs and/or symptoms that the patient may be experiencing or has experienced. This query is made by the physician and/or the staff (verbally or via patient intake forms) in order to best define the patient’s total problem. It includes defin-ing the need for expanded examination, testing, possible affected management options, etc. The review may be about the system(s) directly related to the problem(s) iden-tified in the HPI and/or additional body systems.
z CONSTITUTIONAL: Patient answers about general constitutional signs or symptoms: Examples - fatigue, general appearance, exercise tolerance, fever, weakness, impaired ability to carry out functions of daily living, etc.
z RESPIRATORY: Patient answers about signs or symp-toms of the respiratory system: Examples - cough, phlegm, wheeze, SOB, rapid or difficult breathing, chest pain on deep inhalation, etc.
z INTEGUMENTARY: Patient answers about signs or symptoms of the skin or breast: Examples - skin reac-tions to hot or cold, itching, rash, changes in scars,

Unlock the Secret to E/M Coding
4 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
moles, sores, lesions, nail color or texture, changes in the color of the skin, bruising, breast pain, tenderness, swelling, lumps, nipple discharge or changes, etc.
z PSYCHIATRIC: Patient answers about signs or symp-toms of the psychiatric condition: Examples - depres-sion, stress, excessive worrying, suicidal thoughts, persistent sadness, anxiety, lost pleasure from usual activities, energy loss, physical problems not respond-ing to treatment, restlessness, irritability, excessive mood swings, etc.
z EYES: Patient answers about signs or symptoms of the eye: Examples - use of glasses, discharge, itching, tear-ing or pain, spots or floaters, blurred or double vision, twitching, light sensitivity, visual disturbances, swell-ing around eyes or lids, etc.
z GASTROINTESTINAL: Patient answers about signs or symptoms of the GI system: Examples – heart burn, indigestion or pain with eating, burning sensa-tion in the esophagus, frequent nausea and/or vomit-ing, changes in bowel habits or stool characteristics, abdominal swelling, diarrhea or constipation, use of digestive aids or laxatives, etc.
z NEUROLOGICAL: Patient answers about signs or symptoms of the neurologic system: Examples - numb-ness, tingling, dizziness, syncope or unconsciousness, seizures, convulsions, attention difficulties, memory gaps, hallucinations, disorientation, speech or lan-guage dysfunction, tremor or paralysis, inability to concentrate, sensory disturbances, motor disturbances including gait, balance, coordination, etc.
z ALLERGIC/IMMUNOLOGIC: Patient answers about signs or symptoms of the allergic/immunologic system: Examples - allergies to medicine, foods, envi-ronmental or other substances, frequent sneezing, hives and/or itching, chronic clear PND, conjunctivi-tis, chronic infections, etc.
z ENT: Patient answers about signs or symptoms of the ears, nose of throat: Examples - Ears: sensitivity to noise, ear pain, vertigo, ringing in the ears, “full-ness” in the ears, ear wax abnormalities, etc. Nose: nosebleeds, post nasal drip, nasal drainage, impaired ability to smell, sinus pain, snoring, difficulty breath-ing, sinus infections, etc. Throat/Mouth: sore throats, mouth lesions, teeth sensitivity, bleeding gums, hoarseness, change in voice, difficulties swallowing, changed ability to taste, etc.
z GENITOURINARY: Patient answers about signs or symptoms of the GU system: Examples - painful urination, urine color, urinary patterns, hesitance, flank pain, decreased or increased output, dribbling, incontinence, frequency at night, genital sores, erectile dysfunction, irregular menses, toilet training or bed-wetting, etc.
z ENDOCRINE: Patient answers about signs or symp-toms of the endocrine system: Examples – Blood Sugar readings at home, changes in height and/or weight, increased appetite or thirst, intolerance to heat or cold, etc.
z CARDIOVASCULAR: Patient answers about signs or symptoms of the cardiovascular system: Examples – heart rate, chest pain, tightness, numbness, palpita-tions, heart murmurs, irregular pulse, color changes in fingers or toes, edema, leg pain when walking, etc.
z MUSCULOSKELETAL: Patient answers about signs or symptoms of the MS system: Examples - cramps, twitching or pain, difficulty walking, running or par-ticipation in sports, joint swelling, redness or pain, joint deformities, stiffness, noise with joint movement, etc.
z HEMATOLOGIC/LYMPHATIC: Patient answers about signs or symptoms of the hematologic/lymphatic systems: Examples - easy bruising, fevers which can come and go, swollen glands, night sweats, itching without rash, excessive bleeding, unusual bleeding, etc.
Past, Family & Social HistoryWhen it is medical necessity to perform the ROS and PFSH again at a second encounter, it does not have to be completely re-documented. It may be updated by including the original history date and describing any new ROS and/or PFSH information or noting there has been no change.
z PAST HISTORY: The patient’s past experiences with illnesses, operations, injuries and treatments, and medications; If a patient presents for follow up on a chronic condition both HPI and Past History would be considered. Positive findings of past diagnoses and current medication discovered on ROS would be con-sidered.
z FAMILY HISTORY: A review of medical events in the patient’s family, including age at death, diseases which may be hereditary or place the patient at risk.
z SOCIAL HISTORY: An age-appropriate review of past and current activities, for example occupation, smoking, alcohol use (EtOH), sexual activity, marital status, etc.

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 5
Physical ExamThere are sub components, which could be thought of as “child variables” to measuring the amount of physician’s work in performing a patient exam. These are defined by two different rule tables: The 1995 Documentation Guide-lines and the 1997 Documentation Guidelines. Physicians are allowed to choose which set of rule tables to use.
The CMS 1995 Documentation GuidelinesBody Areas:
z Head/Face z Neck z Back z Abdomen z Genitalia z Chest/axillae/breast
Systems: z Constitutional z Eyes z Ears, nose, mouth and throat z Cardiovascular z Respiratory z Gastrointestinal z Genitourinary z Musculoskeletal z Skin z Neurologic z Psychiatric z Hematologic, lymphatic immunologic
The CMS 1997 Documentation GuidelinesThe guidelines use the same body areas and systems but expand them for specialty specific use. Please review the official guidelines for details.
Medical Decision Making (MDM)The Number of Diagnoses and Management OptionsThe Number of Diagnoses and Management Options is based on the relative level of difficulty in making a diag-nosis and by the status of the problem (controlled versus worsening.) Usual indicators include the following:
z Problems that are new to the patient or that the physi-cian is seeing in this patient for the first time
z Seeking additional work-up such as a consultant’s opinion
z Ordering additional work-up such as diagnostic tests to confirm or to rule out the suspected diagnoses and/or differential diagnoses for the patient
Amount and/or Complexity of Data to be ReviewedThe Amount and Complexity of Data to Be Reviewed is measured by the need to order and review tests and the need to gather information and data. Planning, schedul-ing, and performing clinical labs and tests from the CPT® Medicine and Radiology sections are indicators. The need to request old records or to obtain additional history from someone other than the patient (for example. family member, care giver, teacher, etc.) is credited in this section. Also documented are discussions with the performing phy-sician about unusual or unexpected patient results.
If a physician needs to make an independent visualization and interpretation (for example, MRI film, gram stain, etc.) and he or she is not billing separately for this service, it too is credited to this component of code selection.
Risk Significant Complications, Morbidity, and/or MortalityRisk is measured based on the physician’s determination of the patient’s probability of becoming ill or diseased, having complications, or dying between this encounter and the next planned encounter. The nature of the presenting problem and the urgency of the visit, comorbid conditions, as well as the need for diagnostic tests or surgery, are indi-cators of risk.
Putting It TogetherView the form in Appendix A to visualize typical code selection for Outpatient visits (based on combining each of the key components).

Unlock the Secret to E/M Coding
6 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Chapter 2: Medical Necessity—What is it?Medical Necessity determines the correct code Level. Ful-filling documentation requirements is secondarily required to support correct code use. Although each payer might have its own definition of “Medical Necessity,” most follow Medicare’s example of using Medical Necessity as the “overarching criterion for payment in addition to the individual requirements of a CPT® code”. However, before we can address the problem of Medical Necessity, we must first fully define what Medical Necessity means.
Medicare (and many other insurance plans) may deny pay-ment for a service that the physician believes is clinically appropriate, but which is not reasonable and necessary. To distinguish between “clinically appropriate” and “medically necessary” is a fine line. There are many definitions:
Per the Social Security Act 42 U.S.C. § 1395y(a)(1)(A), Medicare only pays for medical items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a mal-formed body member,” unless there is another statutory authorization for payment.
Medicare has a number of policies, including National Coverage Determinations (NCDs) and Local Cover-age Determinations (LCDs). Section 522 of the Benefits Improvement and Protection Act (BIPA) defines an LCD as a decision by a Medicare carrier whether to cover a par-ticular service in accordance with the Social Security Act.
The AMA definition of “Medical Necessity” is: “Health-care services or products that a prudent physician would provide to a patient for the purpose of preventing, diag-nosing, or treating an illness, injury, disease or its symp-toms in a manner that is: (a) in accordance with generally accepted standards of medical practice; (b) clinically appro-priate in terms of type, frequency, extent, site and duration; and (c) not primarily for the convenience of the patient, physician, or other healthcare provider.”
What is common acknowledged as “generally accepted”?
z Standards that are based on credible scientific evidence published in peer-reviewed, medical literature gener-ally recognized by the relevant medical community;
z Physician specialty society recommendations; z The views of physicians practicing in the relevant clinical area.
When dealing with E/M codes, there are few diagnoses that concretely fall into any of the five levels of care (Out-patient) or three levels of care (Inpatient). There are no NCDs or LCDs to direct a coder to an ICD-9-CM code that is unarguably correct.
This leaves a coder with two distinct questions:
1. How sick does a patient have to be to fall into one of the five levels of care (Outpatient) or three levels of care (Inpatient);
How sick is sick?
2. Who can authoritatively say how sick a patient is;
Who can say how sick is sick?
Chapter 3: How Sick is Sick?Let’s begin with the question of: How sick does a patient have to be in order to fall into one of the five levels of care (Outpatient) or three levels of care (Inpatient)? We know it is imperative to answer this correctly. Medicare contractors and carriers may identify fraud or abuse in situations where they determine Medical Necessity is not met…yet the defi-nitions are broad, subjective, and ambiguous.
There are two references that are commonly employed as a “best practice” in an effort to provide reproducible coding and auditing results. They include the Nature of the Pre-senting Problem as defined by the CPT®, and the Medi-cal Decision Making (MDM) component of the CMS 1995 and 1997 Documentation Guidelines. Both of these approaches have benefits and challenges.
Nature of the Presenting Problem and Medical NecessityThe CPT® describes the nature of the presenting problem to assist the physician in determining the appropriate Level of E/M service. It prompts the reader that the extent of the examination is dependent on clinical judgment per on the nature of the presenting problem(s). It describes five types of presenting problems:
1. Minimal: A
2. Self-limited or minor: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status OR has a good prognosis with management/compliance.

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 7
3. Low severity: A problem where the risk of morbidity without treatment is low; there is little to no risk of mortality without treatment; full recovery without functional impairment is expected.
4. Moderate severity: A problem where the risk of mor-bidity without treatment is moderate; there is mod-erate risk of mortality without treatment; uncertain prognosis OR increased probability of prolonged functional impairment.
5. High severity: A problem where the risk of morbid-ity without treatment is high to extreme; there is a moderate to high risk of mortality without treatment OR high probability of severe, prolonged functional impairment.
CPT® provides clinical examples in its Appendix C to describe presenting problems that are frequently seen with a level of service with a given specialty. The language is broad, interpretive, and warns: “Of utmost importance is that these clinical examples are just that: examples. A particular patient encounter, depending on the specific circumstances, must be judged by the services provided by the physician…”
This approach is not wholly objective or unfailingly repro-ducible. Therefore, even after typically 12 years of school, four years of college, four years of medical school, resi-dency, fellowship, licensing, and certification—many phy-sicians are not able to use these definitionscomparatively with the patient’s condition to confidently determine the correct level of service.
MDM and Medical NecessityTo solve this problem, some physician practices have adopted the MDM component to classify Medical Neces-sity. Does this work better?
Let’s take a closer look to determine this by reviewing the form referenced in this workbook under Appendix A. This form is an audit tool based on the “Marshfield Clinic model”. It is an industry accepted standard that was developed jointly between the Marshfield Clinic and CMS in the 1990s as a method for Medicare carriers to create reproducible audit results across many reviewers by better defining the key components. The form has three compo-nents displayed as tables. The component on the bottom of the page is referenced as MDM -Medical Decision Making. The MDM table requires two of three columns to line up with the row that classifies the MDM. If all three
columns don’t line up, the column in the middle of the three rows is selected.
1. In the header of the first column, called “Number of Diagnoses and Management Options”, we see that not all diagnoses are “equal” - some require more work than others based on the type of diagnosis, not just the number of diagnoses. All diagnosis values are summed together to select a row in that column on the table.
2. The second column captures the work associated with compiling and analyzing outside information, from various sources, to obtain relevant facts about the patient and his or her condition. These values are summed to select a row in that column on the table.
3. The last column works to qualify the medical risk that the patient faces of complications, morbidity, and/or mortality. It is an abbreviated version of the CMS Table of Risk.
Because the determination of risk is complex and not readily quantifiable, the table includes common clinical examples rather than absolute measures of risk. The assess-ment of risk of the presenting problem(s) is based on the risk related to the disease process anticipated between the present encounter and the next one. The row containing the highest value, by example, is selected in that column on the table.
Example: 1. Number of Diagnoses and Management Options:
A patient with a new problem is diagnosed during the same encounter with a problem that is more severe than a minor problem. This is worth “3” on the MDM scale of Number of Diagnoses and Management Options.
2. Amount/Complexity of Data:
The physician ordered and reviewed a medical test in his office. This is worth “1” on the Amount and Complexity of Data
3. Overall Risk:
The problem requires a prescription medication, which the physician orders.

Unlock the Secret to E/M Coding
8 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
MDM - Medical Decision Making ( 2 of 3)Number of Diagnoses and Management Options
Amount/Complexity of Data:
Overall Risk: Type Level (X)
1 SF 1 & 2
L 3
3 Rx drug management M 4
H 5
Stated as a clinically illustrated example:
The patient has sudden central vision loss and is sent to a retina specialist for diagnosis and treatment. A history is obtained and both eyes are thoroughly examined. Several optic tests are used, including an Amsler grid and optical coher-ence tomography. A new diagnosis is made by the physician of sub choroidal neovascularization for which he recommends a monthly injection of Avastin. He explains the risk of the injec-tions, and shares with the patient the risk of continued vision loss with or without the injection. The patient elects to have the injection the same day. Follow up in 3 weeks for evalua-tion and repeat injection.
In this clinically illustrated example, the patient was given the classification of a Moderate Level of MDM. If you are using the MDM as a driver In terms of code selection, this is a Level Four new or established Outpatient patient visit.
So the answer is a Level Four, right? Perhaps, but let’s take a deeper look…
1. What if the patient was sent by the physician to be worked up at an outside facility, and the patient returned with the test results for final diagnosis with the results on the same day? The patient’s medical need is not different, but this would now be a “4”, not a “3”, on the MDM scale of Number of Diagno-ses and Management Options.
2. What if the provider decides that the risk of the problem is not classifiable as that associated with prescription drug management, but rather with the risk associated with an acute illness or injury that poses a threat to bodily function (in this case vision)? This would bump the office visit classifica-tion to a High Level of MDM.
In terms of code selection, this would now support a Level Five new or established Outpatient patient.
The clinical example below further demonstrates the sub-jectivity (and possible lack of reproducibility among coders) associated with the MDM method of code selection:
45-year-old, otherwise healthy male returns for a non-resolved problem first seen 5 days ago ….a cough x 7 days which is now productive. This patient is also under the physician’s care for well controlled hypertension and hypercholesterolemia. The diagnosis today is URI. She reviews all the patient’s cur-rent medications and adds to it by ordering an antibiotic. No follow up requested.
Under this case, the MDM still objectively measures by documentation to a Moderate Level, which is what is needed for a visit Level Four. Some medical peers would argue that a patient seen in follow up for an antibiotic is medically indicated as Low or Straightforward, and that a Detailed History and Examination would not be needed. Therefore the coding would more accurately support a visit Level Two or Three. The code values require a combina-tion of the coding component tables, therefore reviewing the MDM alone may not be fully conclusive. Like the Nature of the Presenting Problem, the MDM component, used to classify Medical Necessity, is not wholly objective or unfailingly reproducible. While both of these are help-ful, they are not the silver bullet of proper code selection.
Chapter 4: Who Says How Sick Is Sick?The best way to stay within the boundaries of Medical Necessity is to think of each element of the history and physical exam as a separate procedure that should be per-formed only if there is a clear medical reason to do so. A coder, while better educated than most non-clinicians, is not able to make that judgment with the certainty of a medical peer. Only a medical peer has the authority to

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 9
define the medical need of the patient. Due to the repeti-tive nature of documentation review in coding, a coder is well practiced in the analysis of the Levels of service com-pared to the documented diagnoses. They are often able to identify possible outliers and cases when Medical Neces-sity might be questioned. Responding to that concern by reviewing it with the treating physician, or a medical peer of the treating physician, is an important part of correct coding.
We know it is the necessity of the work versus the actual volume of work and documentation that should be coded and billed. But, in today’s world of EHR, more documen-tation is produced than ever. Many EHRs have the ability to carry forward old clinical information into the latest note, which is could be seen as “cloning.” Cloning is the billing for services not provided on the actual date of ser-vice billed, but rather provides on a previous already billed date. The problem lies in copying forward old information, such as patient complaints from an earlier visit that have resolved themselves. It can create confusion about what the patient is presenting for on the actual date of service.
Effective documentation is clinically relevant, easy to navi-gate, and provides a solid record of the patient problem and care. The best defense for correct coding is to provide the physician with insight on the clinical relationships in proper code selection. The silver bullet to proper code selection is to empower the physician with the knowledge of that medical need is supported by each Level of service. And, to document what is relevant only to support the patient care and the subsequent coding. No more. No less.
Relating Medical Necessity to Coding One of the most important jobs of a coder is to teach the provider what is medically relevant to each of the levels of service in E/M coding. Provide the documenting pro-vider with a clear understanding of code selection related to Medical Necessity and the rest is…as they say: History (and Exam and MDM and the documentation require-ments thereof).
When a provider is confident that their coding is for ser-vices that are consistent with medically-accepted standards of practice compared to a Level of service, subjectivity is shored up. The chart in Appendix B is a visual tool that can help facilitate communication. It not all-inclusive and should be used for discussion purposed only.
Secret #1: Medical Necessity criteria is best explained in laymen’s terms that allows the physician to define the detail using their own advanced knowledge.
For example, in the subsequent visit hospital setting, it is reasonable to expect higher Levels of history and physical exam to be needed in the days immediately following a hospital admission. These higher levels most likely would not be medically necessary when the patient is stable and improving, particularly in the visits on days preceding discharge from the hospital. Simply stated, the provider needs to understand that a Level One hospital visit is for a patient who is getting better, a Level Two hospital visit is for a patient who isn’t getting better, and a Level Three for a patient who is rapidly declining. Once the provider is able to classify the patient into one of these Levels, the only thing left to ensure is that the documentation require-ments are met for the appropriate level. If a provider feels confident that a non-friendly peer would have to agree with him or her, the code is correct.
Likening the five base levels of service to the same logic in the Wong-Baker children’s pain chart can be helpful to start the conversation. Many will laugh when you say: “Doctor, this is to represent the patient’s pain…not yours in the documentation process!” Levity aside, most physi-cians readily understand that Levels Three to Five are reserved for actively “sick” patients (Levels One to Three in the hospital setting) and that the lower levels of service are reserved for patients with minor and/or well controlled conditions.
The approach here is to ask the physician about a common patient problem that he or she treats, and then to ask him or her what factors would make them more concerned about the patient or less concerned about the patient. Typically, the greater the concern, the higher the level of service.
Medical Necessity “Faces” E/M Coding Scale
Preventive 1 2 3 4 5
**Adapted from Wong-Baker “Faces” Pain Rating Scale

Unlock the Secret to E/M Coding
10 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Sick: Level Three Outpatient (Level One Inpatient)The lower level of service represented by a “sick” patient usually consists of a presenting problem that may be 2 minor, 1-2 stable chronic, 1-2 acute uncomplicated con-ditions. Typically the diagnosis is known and/or made during the encounter and future follow up is often classifi-able as routine. Usually, the patient is clinically responding as expected to treatment or is following a defined course.
z Patient returns with productive cough x 10 days for antibiotic
z Patient with choroidal revascularization to assess efficacy of anti-VEGF
z Patient with cystocele not requiring treatment z Return visit for patient with worsening plantar fasciitis z Patient with URI z Patient with well controlled hypertension and hypercholesterolemia
Sicker: Level Four Outpatient (Level Two Inpatient)The moderately high level codes represented by a “sicker” patient that has the physician concerned. It might be a comorbid problem or complication that is causing the additional concern. It might be that the patient is failing to respond as expected to treatment. The presenting prob-lem may be 2-3 stable chronic, chronic exacerbated, acute with systemic symptoms or injury. Typically the diagnosis is known but worsening/complicated or yet unknown and further testing is required to make a final diagnosis. A key clue to Level Four is the concern of the provider – which often results in future follow up that is classifiable as rou-tine or sooner.
z Patient with cough and chest pain x 2 weeks sent out for CXR
z Patient with choroidal revascularization on anti-VEGF but with new central vision loss
z Patient with cystocele and stress incontinence and to discuss options
z Patient in follow-up with stable angina, not tolerating medication
z Patient requiring closed treatment of new metatarsal fracture
z Patient with back pain and new vaginal discharge for STD testing
z Patient with well controlled asthma, hypertension, and hypercholesterolemia
Sickest: Level Five Outpatient (Level Three Inpatient)The highest level of service represents a patient with a worst-case prognosis. The presenting problem may be an illness or injury that poses a threat to life or bodily func-tion. Typically the patient’s situation is serious, imminent, and uncertain.
Examples:
z Severe exacerbation of CHF z Hospice patient with death imminent z Patient presents confused in diabetic ketoacidosis z Morphine Sulfate IVP ordered for chest pain not controlled by Nitro
z Patient brought by parents after a failed suicide attempt
z Patient post fall on ski slopes with extradural hematoma
Communicating Effectively with Documenting Providers“Clinical Documentation Improvement” (CDI) is a term being dropped with growing frequently---especially as we gear up to ICD-10. It refers to the process of physicians and providers augmenting their documentation to better adhere to medical coding requirements and the new Level of specificity required by ICD-10 codes. ICD-10 codes, like ICD-9-CM codes, authenticate the patient’s docu-mented diagnoses and therefore the patient’s medical need.
Further complicating matters, many providers cringe at the idea of CDI education. It requires much more than subject matter expertise ... it requires truly effective communica-tion. Without a physician’s buy-in, education is a very dif-ficult objective to meet. Communication barriers in the coder-physician relationship often include the difficulty of opposing points of interest.
As we move into these unprecedented times in healthcare, our physicians are more frustrated than ever. According to the 2012 Medscape Physician Compensation Report, half of all physicians already spend more than 5 hours a week on paperwork and other administrative activities. With so much effort devoted to non-clinical requirements and regulations, 46 percent of physicians also say they would NOT choose medicine again as a career. It’s simply too

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 11
hard to “buy in” when you see no correlation between the semantics required in medical documentation data ele-ments—and your true purpose in patient care.
The good news is that physicians want to learn, despite feeling frustrated, when the information is clinically rel-evant, organized, and personalized for them. Typically life-long learners, physicians are highly intelligent, with a deep appreciation for logic and reason. They are naturally intui-tive, some even feeling spiritually drawn to practice the art of medicine and healing. Generally hungry for and appre-ciative of tips and techniques in learning new skills, physi-cians crave correctness. Accurately documenting for coding and billing purposes can prove a annoying dichotomy; it is both a challenge to achieve correctness, while also an intrusion that takes away from patient time. As certified coders…we can help make it easier by giving providers the information they need in a meaningful way.
Secret #2: The best way to communicate with physicians is to ask questions that allow them to draw their own conclusions.
Teaching a physician about the code levels is like giving the natural-born artist a brush, paint, and canvas—explaining the basic use for each and getting out of the way. They are able to produce the art themselves once they have the basic tools and know what they are used for. To have a better understanding of the physician’s standpoint, it is important for you to ask questions. Make sure you ask questions that move the discussion forward and not questions that only promote a “yes or no” answer. Questions like “what made you more concerned about this patient encounter than the other one?” will have a better communication impact than a “did you understand what makes this a Level Four?” Your goal is to promote effective communication and asking well-designed questions will help you in achieving this goal. Sample questions include:
z Tell me about your worst patient case—how did the patient present? Was the patient at risk for lost life or bodily function?
z Would a non-friendly peer agree that the patient was “sicker”—albeit not at imminent risk for lost life or bodily function?
z Is it reasonable that this “sicker” patient needs to be seen in follow-up shortly?
z What lesser but related problem would have you less concerned?
Effective communication includes the way we listen to physicians. Asking questions and listening to the answers will help you steer the rest of the conversation. Sometimes, people are not listening because they are thinking about what they are going to say when the physician stops talk-ing. When physician is talking, give your full attention to what the he or she is saying. Only by listening will coders have a better chance in verifying if the information we are providing was successfully received.
It can be helpful to plan out what you are saying ahead of time. Having a clear idea of what you want to say will help you in presenting a well-structured and trustworthy mes-sage. It will also prevent you from passing a confusing mes-sage to the physician. In these cases, it is very helpful to have the actual documentation you’d like to discuss handy.
Example:“Doctor, I have reviewed this patient encounter and your superbill. You selected a Level Four. You saw this patient 1 month ago for premenopausal syndrome mood swings and prescribed Zoloft. You saw her again today in follow-up. You repeated a comprehensive history and exam. She is doing well with reduced mood swings and will con-tinue with sertraline 50 mg. You ask to see her back in 12 months or PRN if there is a change. I am concerned that an auditor might question the higher Level of service being billed because you are not seeing her back for 12 months and there are no other problems documented. What was it about this patient that put her at a higher level of concern to be coded at a Level Four?”
It is also important to watch your body language while talking with the physician. Communication is not just words: a lot of communication comes through non-verbal communication. The following body language mistakes to avoid are:
z Arms crossed: You are defensive. z Constant eye contact: You are aggressive. z Fidgeting: You are bored or impatient z Hunched posture: You lack confidence. z Little eye contact: You have low interest or lack confidence.
z Rubbing your nose or mouth: You are lying or unsure of yourself.
z Tapping: You are impatient or nervous. z Touching your face or hair: You are timid. z Watching the time: You are anxious to move on to something else.

Unlock the Secret to E/M Coding
12 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Don’t generalize information. Personal information is most meaningful. If you notice a pattern of possible medical necessity concerns, run a productivity report of the last one to three months of Outpatient visits that shows the top diagnosis codes used and the frequency of their use.
Conduct a physician interview to discuss what would make the physician more or less worried about a patient.
Example Dr. ABC, Urologist:
CodeCount of
Occurrence Short Description
790.93 35 Elvtd Prstate Spcf Antgn
592.0 31 Calculus Of Kidney
185 28 Malign Neopl Prostate
599.0 21 Urin Tract Infection Nos
600.00 20 Bph W/O Urinary Obs/Luts
598.9 13 Urethral Stricture Nos
599.71 12 Gross Hematuria
V25.2 12 Sterilization
607.84 10 Impotence, Organic Orign
789.00 10 Abdmnal Pain Unspcf Site
788.30 10 Urinary Incontinence Nos
Sample Interview Questions: z Do any of these pose a threat to life or bodily function within 24-48 hours? (Level Five)
z Under what circumstances would you need to see a patient back in follow-up sooner than is typically required? (Level Four)
z Which patient problems have you very concerned for the patient but do not pose an imminent threat to life or bodily function? (Level Four)
z Which of these can commonly be diagnosed on the first encounter and do not usually require a prompt follow-up? (Level Three)
z Which of these problems might you bring a patient back for a quick check, and on doing so discover no further medical management is needed? (Level Two)
z Which of these diagnoses are self-limited and require reassurance with no active medical management? (Level One)
z Would a non-friendly medical peer agree with your decisions?
Another technique is to run the same report and ask the physician which problems pose an imminent threat to life or bodily function and then ask him or her to rank each problem on a scale of 1-4, with 4 representing the “sicker” patients that “keep them up at night” and 1 representing patients about which they are not concerned. This can form the basis for a physician to define for him or herself what constitutes each level of service.

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 13
Example Dr. DEF, Dermatologist:
CodeCount of
Occurrence Short DescriptionImmanent Threat to Life/Function 4 3 2 1
702.0 99 ACTINIC KERATOSIS Yes/No
239.2 96 BONE/SKIN NEOPLASM NOS Yes/No
706.1 76 ACNE NEC Yes/No
706.8 56 SEBACEOUS GLAND DIS NEC Yes/No
216.3 47 BENIGN NEO SKIN FACE NEC Yes/No
702.19 45 OTHER SBORHEIC KERATOSIS Yes/No
228.01 42 HEMANGIOMA SKIN Yes/No
709.2 36 SCAR & FIBROSIS OF SKIN Yes/No
216.5 36 BENIGN NEO SKIN TRUNK Yes/No
216.4 33 BEN NEO SCALP/SKIN NECK Yes/No
709.09 29 OTHER DYSCHROMIA Yes/No
216.6 27 BENIGN NEO SKIN ARM Yes/No
692.9 24 DERMATITIS NOS Yes/No
V10.83 19 HX-SKIN MALIGNANCY NEC Yes/No
078.10 17 VIRAL WARTS NOS Yes/No
216.7 14 BENIGN NEO SKIN LEG Yes/No
459.32 13 CHR VENOUS HYPR W INFLAM Yes/No
454.8 12 VARIC VEIN LEG,COMP NEC Yes/No
690.10 12 SEBRRHEIC DERMATITIS NOS Yes/No
782.1 10 NONSPECIF SKIN ERUPT NEC Yes/No
454.1 10 LEG VARICOSITY W INFLAM Yes/No
459.81 10 VENOUS INSUFFICIENCY NOS Yes/No
Chapter 5: Combining ICD-10 CDI Training Sessions This type of CDI training format can be especially helpful when you combine it with ICD-10 training. This is a good way to maximize the educational use of the physician’s time. Using the AAPC ICD-10 Code Translator located at http://aapc.com/ICD-10/codes/index.aspx, which is based on the General Equivalency Mapping (GEM), you will be able to quickly see which codes inherently have addi-tional granularity and documentation requirements. (Note: always review mapping results in the official ICD-10 book before applying them.)

Unlock the Secret to E/M Coding
14 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Example Dr. GHI, Orthopedic Surgeon (Hand)
Code Count Description ICD-10 ConsiderationsV54.01 74 Removal Int Fixation Dev Z47.2
883.1 38 Open Wound Finger-Compl S61.229A
E918 36 Caught Between Objects W23.0XXA
816.12 35 Fx Distal Phal, Hand-Opn S62.523B Displaced Fracture Of Distal Pha-lanx Of Unspecified Thumb, Initial Encounter For Open Fracture
S62.526B Nondisplaced Fracture Of Distal Phalanx Of Unspecified Thumb, Initial Encounter For Open Fracture
S62.639B Displaced Fracture Of Distal Pha-lanx Of Unspecified Finger, Initial Encounter For Open Fracture
S62.669B Nondisplaced Fracture Of Distal Phalanx Of Unspecified Finger, Initial Encounter For Open Fracture
883.2 27 Open Wnd Finger W Tendon S61.19A Unspecified Open Wound Of Unspecified Thumb With Damage To Nail, Initial Encounter
S61.29A Unspecified Open Wound Of Unspecified Finger Without Damage To Nail, Initial Encounter
S66.529A Laceration Of Intrinsic Muscle, Fascia And Tendon Of Unspecified Finger At Wrist And Hand Level, Ini-tial Encounter
354.2 22 Ulnar Nerve Lesion G56.20
354.0 21 Carpal Tunnel Syndrome G56.00
883.0 20 Open Wound Of Finger S61.209A
813.42 19 Fx Distal Radius Nec-Cl S52.509A
727.03 16 Trigger Finger M65.30
727.05 14 Tenosynov Hand/Wrist Nec M65.849
726.32 13 Lateral Epicondylitis M77.00

Unlock the Secret to E/M Coding www.aapc.com 15
Code Count Description ICD-10 Considerations733.82 13 Nonunion of Fracture S42.29k Unspecified Fracture Of Upper End
Of Unspecified Humerus, Subse-quent Encounter For Fracture With Nonunion
S42.9XK Fracture Of Unspecified Shoulder Girdle, Part Unspecified, Subsequent Encounter For Fracture With Nonunion
S52.9XK Unspecified Fracture Of Unspecified Forearm, Subsequent Encounter For Closed Fracture With Nonunion
S52.9XM Unspecified Fracture Of Unspecified Forearm, Subsequent Encounter For Open Fracture Type I Or Ii With Nonunion
S52.9XN Unspecified Fracture Of Unspecified Forearm, Subsequent Encounter For Open Fracture Type Iiia, Iiib, Or Iiic With Nonunion
S62.9XK Unspecified Fracture Of Unspeci-fied Wrist And Hand, Subsequent Encounter For Fracture With Non-union
727.41 10 Ganglion Of Joint M67.419 Ganglion, Unspecified Shoulder
M67.429 Ganglion, Unspecified Elbow
M67.439 Ganglion, Unspecified Wrist
M67.449 Ganglion, unspecified hand
E920.9 10 Acc-Cutting Instrum Nos W45.8XXA
E928.9 10 Accident Nos X58.XXXA

Unlock the Secret to E/M Coding
16 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Chapter 6: Mastering a Good Coder-Physician RelationshipSecret #3: Coders, unlike any other position in healthcare, are capable of helping physicians. Physicians are increasingly told that they need to be afraid. They have been fighting tangible tigers—stiff regula-tory compliance, decreased fee schedules, and increasing expenses. The result is that it became easy to tune out the chatter. Communication that makes coding clinically rel-evant is probably the most important contribution a coder can make to keeping physicians happy—because they can spend more time doing what they enjoy most: patient care. This makes you highly valuable in today’s world of uncer-tainty and confusion and the ripple effect into the health-care communities is powerful!
It’s hard to want to help someone who is often frustrated, and perhaps even short tempered. Coders are sometimes shot as the messenger. It can be very helpful to remind ourselves why physicians deserve a break.
Becoming a physician requires a “character of commit-ment” to complete a lengthy training period where sacrifice is demanded on several Levels. When communicating with a physician, it is important to consider that during indoctrination to medical training and the Hippocratic Oath, the primary focus was on the “patient above all else.” Little or no mention of coding is made, which is a magi-cal, mythical, and far-off concept to the average medical student.
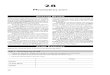
In order to better understand and communicate with phy-sicians, coders must appreciate the dedication, sacrifice, and time spent in their professional development.
Figure 1: Time Line to becoming a physician
2008 2023
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023
2008 - 2012Under-Grad
2012 - 2015Medical School
2019 - 2020Fellowship
2016 - 2023Residency
2019License to Practice
Fast Facts z 700K physicians in the US
{ 63% (442K) bill E/M services { 20% (and growing) are employed by hospitals
z 2012 average medical school grad debt = $161K z Within 6 years we will need 91,500 new doctors z 33% are in private practice From 57% in 2007 z On again, off again regulations (SRG, ICD-10) z Difficult rules (E/M, HIPAA, MU), high costs (malpractice)
“Medicine is the only profession that labours incessantly to destroy the reason for its own existence.” ~James Bryce, 1914
Let’s Help!The best coders have also mastered the art of communicat-ing with physicians in ways that produce positive results. Physicians needs coders in order to minimize their uncer-tainty on all the rules. A good coder helps make a physi-cian’s practice a better place to work. We are privileged in these unprecedented and problem plagued times to be an important part of the solution!

Unlock the Secret to E/M Coding
Unlock the Secret to E/M Coding www.aapc.com 17
References Citedwww.hhs.gov/afr/2013-hhs-agency-financial-report.pdf
Page 37 Evaluation and Management Services Guide www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/eval_mgmt_serv_guide-ICN006764.pdf
U.S. Bureau of Labor Statistics: www.bls.gov
H&HN: www.hhnmag.com/hhnmag/HHNDaily/HHNDailyDisplay.dhtml?id=1970001363 and Fierce Healthcare www.fiercehealthcare.com/story/hospitals-employing-32-more-physicians/2012-01-09
Dept. of Health and Human Services Office of Inspector General May 2012 https://oig.hhs.gov/
AMA: www.ama-assn.org//ama/pub/about-ama/our-people/member-groups-sections/medical-student-section/advocacy-policy/medical-student-debt/background.page
AAMC: www.aamc.org/newsroom/reporter/december2013/363844/word.html#.UsNX-fRDuSo
Accenture: www.govconexecutive.com/2011/06/accenture-only-one-third-of-physicians-to-remain-independent-by-2013/


Unlock the Secret to E/M Coding www.aapc.com 19
Appendix A
How
to E
ffec
tivel
y Te
ach
Eval
uatio
n an
d M
anag
emen
t in
Und
er O
ne H
our,
wri
tten
by
Step
hani
e Ce
cchi
ni, C
PC, C
EMC,
CH
ISP
© C
opyr
ight
AA
PC 2
007-‐
2012
26
Ex 95 DG ExamMM
Body Areas:
head
/face
ne
ck
back
ab
dom
en
geni
talia
ch
est/a
xilla
e/br
east
ea
ch e
xtre
mity
System
s:
cons
titut
iona
l
ey
es
EN
MT
card
iova
scul
ar
resp
irato
ry
gast
roin
test
inal
ge
nito
urin
ary
mus
culo
skel
etal
sk
in
neur
olog
ic
psyc
hiat
ric
hem
atol
ogic
, lym
phat
ic im
mun
olog
ic
Quick-‐Reference Cod
e Sheet
New
PT: D
efau
lt to
the
low
est L
EVEL
iden
tifie
d by
the
Hx,
Ex,
& M
DM
. Est PT: U
se th
e LE
VEL
iden
tifie
d by
the
best
2 o
f 3 o
n th
e H
x, E
x, &
MD
M (9
9211
not
a D
r Co
de)
Hx History ( 3 of 3)
HPI:
loca
tion
qual
ity
seve
rity
tim
ing
cont
ext
mod
fact
or
dura
tion
asso
. S&
S
ROS:
cons
tit
eyes
EN
MT
card
io
resp
ir
GI
GU
M
S sk
in
neur
o ps
ych
endo
he
mat
/lym
ph
alle
rg/i
mm
uno
PFSH
: pa
st
fam
ily
soci
al
Type
New
O
ut P
t LEVEL
Est P
t LEVEL
1 0
0 PF
1 2
1 1
0 EPF
2 3
4 or 1997:3 chronic
2-‐9
1 D
3 4
4 or 1997:3 chronic
10+
3 or2+ (Est.)
C 4 & 5 5
MDM M
edical Decision Making ( 2 of 3)
Num
ber of Bod
y Areas/Systems Exam
ined
Type
New
Out Pt
LEVEL
Est. Out
Patient
LEVEL
1 PF
1 2
2-‐7 Limited
EPF
2 3
2-‐7 Extended
D
3 4
8 (Systems on
ly)
C 4 & 5
5
NUMBER OF DX and
MANAGEM
ENT OPTIONS
Min
or =1 ea
. (m
ax 2
poi
nts)
Est.
sta
ble/
impr
oved
= 1 ea.
Est.
wor
seni
ng =2 ea
.
New
pro
blem
(S),
w/o
wor
kup
=3
New
pro
blem
, w w
orku
p=4 ea.
AMOUNT/CO
MPLEXITY OF DATA
: One Point Each:
Clin
ical
Lab
s te
st o
rder
ed o
r re
view
ed
CPT®
Med
icin
e Se
ctio
n Te
st-‐ o
rder
ed/r
evie
wed
CP
T® R
adio
logy
Sec
tion
Test
-‐ ord
ered
/rev
iew
ed
Dis
cuss
pat
ient
res
ults
w p
erfo
rmin
g /
cons
ultin
g D
r
Dec
isio
n ob
tain
old
rec
ords
or
addi
tiona
l hx
othe
r th
an p
t
Two Po
ints Each:
Revi
ew/s
umm
ariz
e da
ta o
ld r
ecor
ds/a
dd h
x o
ther
than
pt
Inde
pend
ent i
nter
pret
atio
n of
an
imag
e, tr
acin
g, s
peci
men
OVERALL RISK:
Th
e qu
ick
refe
renc
e gu
ide
belo
w s
how
s ex
cerp
ts fr
om th
e CM
S Ta
ble
of R
isk.
*R
emem
ber:
Ris
k is
bas
ed o
n th
e di
seas
e pr
oces
s an
ticip
ated
bet
wee
n th
e pr
esen
t en
coun
ter
and
the
next
one
.
Type
New
or
Est. Out
Pt
LEVEL
1 1
Clinical testing/m
anagem
ent exam
ples:
Veni
punc
ture
, X-‐r
ay, E
KG, U
/A, U
/S, r
est,
sup
erfic
ial
dres
sing
s, e
last
ic b
anda
ge, g
argl
es, e
tc.
Presenting Problem
Example:
1 m
inor
/ s
elf l
imite
d
SF
1 & 2
2 2
Clinical testing/m
anagem
ent exam
ples:
Biop
sy, p
ulm
onar
y fu
nctio
n, b
ariu
m e
nem
a, m
inor
su
rger
y w
ithou
t ris
k fa
ctor
s, O
TC d
rugs
, PT,
OT,
IV w
ithou
t add
itive
s, e
tc.
Presenting Problem
Example:
1 –
2 m
inor
, 1 s
tabl
e ch
roni
c /
1 ac
ute
unco
mpl
icat
ed
L 3
3 3
Clinical testing/m
anagem
ent exam
ples:
Stre
ss te
sts,
end
osco
pies
, car
diov
ascu
lar
imag
ing,
ce
ntes
is, c
lose
d Tx
of F
x, R
x dr
ug m
anag
emen
t, m
inor
sur
gery
with
ris
k fa
ctor
s, m
ajor
ele
ctiv
e su
rger
y w
ithou
t ris
k fa
ctor
s, th
erap
eutic
rad
iatio
n tx
, et
c.
Presenting Problem
Example: 1
chr
onic
exa
cerb
ated
/ 2
sta
ble
chro
nic
/ N
ew U
ndia
gnos
ed
with
unc
erta
in o
utco
me
/ A
cute
with
sys
tem
ic s
ympt
oms
/ ac
ute
com
plic
ated
inju
ry
M
4
4
4
Clinical testing/m
anagem
ent exam
ples:
Card
iova
scul
ar im
agin
g w
ith r
isk
fact
ors,
en
dosc
opie
s w
ith r
isk
fact
ors,
dis
cogr
aphy
, med
icat
ion
toxi
city
man
agem
ent,
maj
or s
urge
ry
with
ris
k fa
ctor
s, e
mer
genc
y su
rger
y w
ith r
isk
fact
ors,
etc
.
Presenting Problem
Example:
1+
chro
nic
seve
rely
exa
cerb
ated
/ Il
lnes
s or
inju
ry th
at p
oses
a
thre
at to
life
/ A
brup
t cha
nge
in n
euro
logi
cal s
tatu
s
H
5
Re
prin
ted
with
Per
mis
sion
: Q
uick
Ref
eren
ce C
ode
Shee
t © C
opyr
ight
200
6-‐20
12 S
teph
anie
Cec
chin
i, CP
C, C
EMC,
CH
ISP
Appendix A: E/M Code Selection (Reference Sheet)

20 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Appendix B
Appendix B: Medical Necessity Flow Chart

Unlock the Secret to E/M Coding www.aapc.com 21
Appendix C
Appendix CExercises Referenced in PresentationTrue or False?
1. Specialists must use 1997 guidelines for documentation.
2. “Shortness of breath” is the reason of the visit according to the patient during her statement of CC. Can this be counted in the CC and the ROS?
3. CMS specifically states positive findings of an exam cannot be documented by simply stating the exam find-ings were abnormal.
4. CC must be documented in a specific statement rather than implied.
5. Counseling topics must be documented when billing for counseling time of greater than 50% of the encounter.
Multiple Choice.
1. The statement “I jumped over a railing, fell and landed on both arms outstretched” is considered which of the following HPI statement?
A. Associated signs and symptoms
B. Modifying factors
C. Context
D. Quality
2. By CMS ‘95 guidelines, interpreted by MAC carriers, which requirement below could define a “detailed” exam
A. 4x4
B. 2–7 body systems
C. 2–4 body systems
D. All of the above
3. 1995 and 1997 documentation guidelines differ in what two elements of documentation:
A. History and Medical Decision Making
B. Exam and Medical Decision Making
C. Time and Medical Decision Making
D. History and Exam

22 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Appendix C
4. In the History of Present illness the doctor documents the patients has abdominal pain when eating greasy food. Which categories would this HPI would be scored in?
A. Duration, location
B. Severity, context
C. Location, context
D. Quality, timing
NOTES:

Unlock the Secret to E/M Coding www.aapc.com 23
Presentation
2014 CPT® Update
Unlock the Secret to E/M Coding: Medical Necessity Skills for Coders
Written by: Stephanie Cecchini, CPC, CEMC, CHISP, Approved ICD-10 Trainer
Presented by: [insert name of presenter]
1
2014 CPT® Update
• 8:30-8:45 Introduce Ourselves and the Topic• 8:45-10:00 DG Refresher: (with interactive examples)
– Quick Break• 10:15-10:30 Medical Necessity – What is it?• 10:30-10:45 How Sick is Sick?• 10:45-11:15 Who Says How Sick is Sick?• 11:15-12:00 ICD-10 Training (with interactive examples) • 12:00-12:15 Coder-Physician Relationship• 12:15-12:30 CEU Reference Number and Answer Questions
• In this workshop, you will learn:– Three little known secrets to accurate
E/M coding– The definitions of Medical Necessity for
purposes of accurate coding – How to clinically differentiate E/M
service Levels– Effective techniques for
communication with physicians regarding Medical Necessity
2
Agenda

24 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• [Insert Presenter Bio]
About the Presenter
3
2014 CPT® Update
• Medicare fee-for-service improper payments increased 18% to $36B in 2013 – The primary cause is insufficient documentation(63%). – The other cause is classified as Medical Necessity errors (37%)
• CMS 1995 and 1997 Documentation Guidelines are not statutes – Medical need for services rendered is the authoritative factor
• Medicare may deny payment for a service that the physician believes is clinically appropriate, but which is not reasonable and necessary
The Medical Necessity Problem
4

Unlock the Secret to E/M Coding www.aapc.com 25
Presentation
2014 CPT® Update
Only in Healthcare
5
2014 CPT® Update
• Coders are not Doctors but must make decisions about Medical Necessity– A coder might code correctly per the DGs….however, miscode if they
incorrectly interpret the severity of the patient’s problem – Coders are not medical peers to physicians
• Coders are often required to make decisions that involve MN– Challenging the medical need is not appropriate– Auditors may have limited access to a Medical Director or peer– A wrong step can lead to barriers in the coder-physician
relationship
What’s the Problem?
6

26 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• EHRs are producing more “false positives” to higher levels of service• Unvoiced concerns lead to over-payments and negative payer audits
– Audits projected to rise in 2014• 2013 CMS reported an error rate of 10.1% for FFS.
– This is an increase from 9.9% in 2012.– This exceeds the 10% threshold set by the Improper Payments
Elimination and Recovery Act of 2010 (IPERA)
Coder Silence is Damaging
7
2014 CPT® Update
• Without it Physicians can’t be paid properly …• Documentation requirements need to be met• Subjective criteria on Medical Necessity and DGs
– Codes are based on a scale of how sick a patient is– Codes are supported by documentation
• Solutions (and today’s objective topics):– Know the DGs and Medical Necessity with E/M– Learn to code based on how sick a patient is– Help the Physician to understand Good Documentation
“Meaningful” E/M Documentation
8

Unlock the Secret to E/M Coding www.aapc.com 27
Presentation
2014 CPT® Update
• Effective documentation is: – clinically relevant, – easy to navigate, – provides a solid record of the patient problem and their care. – Limits carry forward of old documentation – Adheres to the 1995 and 1997 Documentation Guidelines
• Carrier interpretations – Marshfield clinic model– 4x4
What is Good Documentation?
9
2014 CPT® Update
• The 3 Key Components
• Time may be used if the total time is documented and more than 50% of the encounter is spent in counseling or coordination of care
•
The DGs
10
1. History History of Present Illness (HPI)Review of Systems (ROS) Past, Family and Social History (PFS) 2. Exam 3. Medical Decision Making Number of Diagnoses and Treatment OptionsAmount and Complexity of DataOverall Risk

28 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• Handling documentation with Patients unable to give a history
• (ROS) and (PFSH) History taken from an earlier encounter
– May not be medically necessary
• A comprehensive service may be performed and documented but A comprehensive service is not always medically necessary or billable.
• Unless Preventive, a Chief Complaint (CC) must be identifiable
– This is the first step in establishing medical necessity.
• The patient’s stated reason for the visit– Location– Context– Duration– Quality– Modifying factors– Severity– Timing– Associated signs and symptoms
HPI
2014 CPT® Update
• The ROS may be supplied in any format: separate patient intake or questionnaire form within the HPI.
• ROS elements typically reference signs and symptoms, of which both positive and negative responses are considered. Auditors commonly watch for indications “pt denies fever,” “upon further questioning the…”).
• ROS should be medically necessary. – It may be considered necessary to
obtain a complete ROS when a patient presents as an initial new patient.
– It may not be considered necessary to repeat a complete review on every follow-up visit.
• Past history: The patient's past experiences with illnesses, operations, injuries and treatments, and medications.
• Family history: A review of medical events in the patient's family, including age at death, diseases which may be hereditary or place the patient at risk.
• Social history: An age-appropriate review of past and current activities, for example occupation, smoking, alcohol use (EtOH), sexual activity, marital status, etc.
ROS and PFS

Unlock the Secret to E/M Coding www.aapc.com 29
Presentation
2014 CPT® Update
HPI:locationqualityseverity timing
contextmod factordurationasso. S&S
ROS:constiteyesENMTcardiorespir
GIGUMSskin
neuropsychendo hemat/lymphallerg/immuno
PFSH:pastfamilysocial
Type
New Out Pt LEVEL
(x)Est Pt LEVEL
(x)1 0 0 PF 1 2
1 1 0 EPF 2 3
4 2 1 D 3 4
4 10 3 or2+ (Est.) C 4 & 5 5
CC: Headache. “I fell off my chair an hour ago and hit my head. I have a throbbing headache.” The patient states the pain is 8 out of 10. Patient denies any visual disturbances. Patient takes Zoloft 25 mg QD.
2014 CPT® Update
BP 120/80. The patient’s gait is normal. Some tenderness. Thereis no knee effusion. The medial and lateral collateral ligaments are intact.
14
Number of Body Areas/Systems Examined
Type
New Out Pt LEVEL
(x)
Est. Out Patient LEVEL (x)
1 PF 1 2
2‐7 limited EPF 2 3
2‐7 extended (4x4) D 3 4
8 (Systems only) C 4 & 5 5
Body Areas:• Head/Face• Neck• Back• Abdomen• Genitalia• Chest/axillae/breast
Systems: • Constitutional• Eyes• Ears, nose, mouth and throat• Cardiovascular• Respiratory• Gastrointestinal• Genitourinary• Musculoskeletal• Skin• Neurologic• Psychiatric• Hematologic, lymphatic immunologic
9

30 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
MDM: Number of Dx and Tx Options‐Minor =1 each (max 2)‐ Est. stable/improved = 1 each‐ Est. worsening =2 each‐ New problem, w/o workup =3 each (max 1)‐ New problem, w workup=4 each Example Type New or Established
Outpatient LEVEL
Minimal: 1 point as totaled from above
Uncomplicated, non-infected insect bite
Straight-forward 1 & 2
Limited: 2 points as totaled from above
Controlled HTN andtachycardia
Low 3Multiple: 3 points as totaled from above
New patient with migraineheadaches
Moderate 4Extensive: 4 + points as totaled from above
Patient seen today for f/uon OA knees and 1 yearTHR check. C/O knee pain.MRI ordered for possiblemeniscus tear. R/Osymptom of osteoarthritisand sprain
High 5
2014 CPT® Update
MDM: Amount and Complexity of DataOne Point Each: Clinical Labs test(s) ordered and/or reviewed CPT® Medicine Section Test(s)- ordered and/or reviewed CPT® Radiology Section Test(s)- ordered and/or reviewed Discuss patient results with performing/consulting Dr. Decision to obtain old records or add hx from other than pt
Two Points Each: Review & sum data from old records add hx from other than pt (2nd) interpretation of an image, tracing, specimen
TypeNew or Established Outpatient LEVEL
Minimal: 1 point as totaled from above
Straight-forward 1 & 2
Limited: 2 points as totaled from above
Low 3
Moderate: 3 points as totaled from above
Moderate 4
Extensive: 4 + points as totaled from above
High 5

Unlock the Secret to E/M Coding www.aapc.com 31
Presentation
2014 CPT® Update
CMS TABLE OF RISKOverall Risk between planned encounters
Any example listed from a row below for any of the three columns will equal a level of risk.1. Presenting Problem(s) 2. Diagnostic Procedure(s) Ordered 3. Management Options Selected Type
New or Established Outpatient LEVEL
• One self-limited or minor problem, eg cold, insect bite, tinea corporis
• Laboratory tests requiring venipuncture• Chest x-rays• EKG/EEG• Urinalysis• Ultrasound, eg, echocardiography• KOH prep
• Rest• Gargles• Elastic bandages• Superficial dressings
Minimal 1 & 2
• Two or more self-limited or minor problems• One stable chronic illness, eg, well controlled hypertension or non-insulin dependent diabetes, cataract, BPH• Acute uncomplicated illness or injury, eg, cystitis, allergic rhinitis, simple sprain
• Physiologic tests not under stress, eg, pulmonary function tests• Non-cardiovascular imaging studies with contrast, eg, barium enema• Superficial needle biopsies• Clinical laboratory testsrequiring arterial puncture• Skin biopsies
• Over-the-counter drugs• Minor surgery with no identified risk factors• Physical therapy• Occupational therapy• IV fluids without additives
Low 3
• One or more chronic illnesses with mild exacerbation, progression, or side effects of treatment• Two or more stable chronic illnesses• Undiagnosed new problem with uncertain prognosis, eg, lump in breast• Acute illness with systemic symptoms, eg, pyclonephritis, pneumonitis, colitis• Acute complicated injury, eg, head injury with brief loss of consciousness
• Physiologic tests under stress, eg, cardiac stress test, fetal contraction stress test• Diagnostic endoscopies with no identified risk factors• Deep needle or incisional biopsy• Cardiovascular imaging studies with contrast and no identified risk factors, eg arteriogram, cardiac catheterization• Obtain fluid from body cavity, eg, lumbar puncture, thoracentesis, culdocentesis
• Minor surgery with identified risk factors• Elective major surgery (open, percutaneous or endoscopic) with no identified risk factors• Prescription drug management• Therapeutic nuclear medicine• IV fluids with additives• Closed treatment of fracture or dislocation without manipulation
Moderate 4
• One or more chronic illnesses with severe exacerbation, progression, or side effects of treatment• Acute or chronic illnesses or injuries that pose a threat to life or bodily function, eg multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failure• An abrupt change inneurologic status, eg, seizure, TIA, weakness, or sensory loss
• Cardiovascular imaging studies with contrast with identified risk factors• Cardiac electrophysiological tests• Diagnostic Endoscopies with identified risk factors• Discography
• Elective major surgery (open, percutaneous or endoscopic) with identified risk factors• Emergency major surgery (open, percutaneous or endoscopic)• Parenteral controlled substances• Drug therapy requiring intensive monitoring for toxicity• Decision not to resuscitate or to de-escalate care because of poor prognosis
High 5
2014 CPT® Update

32 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• Cahaba Government Benefit Administrators®
– 95/97 – Not Further Publicized
• CGS Administrators, LLC – 95/97 – Some “extra wording” (i.e.
“contributory” not counted) http://cgsmedicare.com/pdf/Basics_of_Evaluation_and_Management.pdf
MAC Rules:
2014 CPT® Update
• First Coast Service Options, Inc.– 95/97 (version of Marshfield Clinic) – E/M interactive worksheet
http://medicare.fcso.com/EM/165590.asp
• Noridian Administrative Services, LLC
– 95/97 Not Further Publicized – Medical Necessity Article
https://www.noridianmedicare.com/provider/updates/docs/E-M_servicesdocumentation_and_level_of_service.pdf
MAC Rules:

Unlock the Secret to E/M Coding www.aapc.com 33
Presentation
2014 CPT® Update
• Noridian Administrative Services, LLC (FORMERLY Palmetto GBA)
– Palmetto used 95/97 Marshfield
• Noridian Administrative Services, LLC
– 95/97 Not Further Publicized – Medical Necessity Article
https://www.noridianmedicare.com/provider/updates/docs/E-M_servicesdocumentation_and_level_of_service.pdf
MAC Rules:
2014 CPT® Update
• National Government Services, Inc.– 95/97 Marshfield– Audit Form:
http://www.ngsmedicare.com/ngs/wcm/connect/d410740049c1dcef894cf9b8b8c8d5ce/1074_0412_EM_Documentation_Training_Tool.pdf?MOD=AJPERES&useDefaultText=0&useDefaultDesc=0
• Wisconsin Physicians Service Insurance Corporation
– 95/97 Not Further Publicized– References at:
http://www.wpsmedicare.com/j8macpartb/resources/provider_types/evalandmngmnt.shtml
MAC Rules:

34 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• NHIC, Corp. – 95/97 Marshfield– Audit form:
http://emuniversity.com/COW/NHIC.pdf
• Novitas Solutions, Inc.– 95/97 Marshfield with 4x4– 4x4 information: http://www.novitas-
solutions.com/cs/idcplg?IdcService=GET_FILE&RevisionSelectionMethod=LatestReleased&dDocName=00025767&allowInterrupt=1&Rendition=Web&IsXml=0
MAC Rules:
2014 CPT® Update
Discussion Exercise
99213
See Appendix C : T&F
1. Specialists must use 1997 guidelines for documentation.2. “Shortness of breath” is the reason of the visit according to the patient during her statement of CC.
Can this be counted in the CC and the ROS?3. CMS specifically states positive findings of an exam cannot be documented by simply stating the
exam findings were abnormal.4. CC must be documented in a specific statement rather than implied. 5. Counseling topics must be documented when billing for counseling time of greater than 50% of the
encounter.
See Appendix C: Multiple Choice

Unlock the Secret to E/M Coding www.aapc.com 35
Presentation
2014 CPT® Update
• Government: – Per the Social Security Act 42 U.S.C. § 1395y(a)(1)(A), “SSA” Medicare only
pays for medical items and services that are "reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member", unless there is another statutory authorization for payment.
– National coverage determinations (NCDs) and Local Coverage Determinations (LCDs). Section 522 of the Benefits Improvement and Protection Act (BIPA) defines an LCD as a decision by a Medicare carrier whether to cover a particular service in accordance with the SSA
What is Medical Necessity?
25
2014 CPT® Update
• “Health care services or products that a prudent physician would provide to a patient for the purpose of preventing, diagnosing, or treating an illness, injury, disease or its symptoms in a manner that is:
• (a) in accordance with generally accepted standards of medical practice; • (b) clinically appropriate in terms of type, frequency, extent, site and
duration; and • (c) not primarily for the convenience of the patient, physician, or other
health care provider.”
AMA
26

36 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• What is common acknowledged as “generally accepted”?– Standards that are based on credible scientific evidence published in
peer-reviewed, medical literature generally recognized by the relevant medical community;
– Physician specialty society recommendations;– The views of physicians practicing in the relevant clinical area.
“Generally Accepted”
27
2014 CPT® Update
1. How sick does a patient have to be in order to fall into one of the 5 Levels of care (Outpatient) or 3 Levels of care (Inpatient);– How sick is sick?
1. Who can authoritatively say how sick a patient is; – Who can say how sick is sick?
Leaves a Coder with Two Questions
28

Unlock the Secret to E/M Coding www.aapc.com 37
Presentation
2014 CPT® Update
1. Minimal: A problem that may not require the presence of the physician or other qualified health care professional, but service is provided under the physician’s or other qualified health care professional’s supervision.
2. Self-limited or minor: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status OR has a good prognosis with management/compliance.
3. Low severity: A problem where the risk of morbidity without treatment is low; there is little to no risk of mortality without treatment; full recovery without functional impairment is expected.
4. Moderate severity: A problem where the risk of morbidity without treatment is moderate; there is moderate risk of mortality without treatment; uncertain prognosis OR increased probability of prolonged functional impairment.
5. High severity: A problem where the risk of morbidity without treatment is high to extreme; there is a moderate to high risk of mortality without treatment OR high probability of severe, prolonged functional impairment.
CPT Nature of the Presenting Problem
29
2014 CPT® Update
• Example: – Number of Diagnoses and Management Options:
• A patient with a new problem is diagnosed during the same encounter with a problem that is more severe than a minor problem. This is worth “3” on the MDM scale of Number of Diagnoses and Management Options.
– Amount/Complexity of Data:• The physician ordered and reviewed a medical test in his office. This is worth “1”
on the Amount and Complexity of Data – Overall Risk:
• The problem requires a prescription medication, which the physician orders. – See the chart in your workbook on page 15 and review clinical example on page 16
MDM as a MN Driver?
30

38 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• What if the patient was sent by the physician to be worked up at an outside facility, and the patient returned with the test results for final diagnosis with the results on the same day?
• What if the provider decides that the risk of the problem is not classifiable as that associated with Prescription drug management, but rather with the risk associated with an acute illness or injury that poses a threat to bodily function (in this case vision)?
– In terms of code selection for Medical Necessity with an MDM driver, this could now support a Level Five new or established Outpatient patient.
• Another example :45 year old, otherwise healthy male returns for a non-resolved problem first seen 5 days ago ….a cough x 7 days which is now productive. This patient is also under the physician’s care for well controlled hypertension and hypercholesterolemia. The diagnosis today is URI. She reviews all the patient’s current medications and adds to it by ordering an antibiotic. No follow-up requested.
– MDM is moderate….is this a Level Four clinical example?
Answer is a Level Four, right? Well…
31
2014 CPT® Update
• Nature of the presenting problem --- still vague• MDM as a driver --- still not “a silver bullet• What’s left?
– The physician – SECRET #1
• Medical Necessity criteria is best explained in laymen’s terms that allows the physician to define the detail using their own advanced knowledge.
Who Can Say How Sick is Sick?
32

Unlock the Secret to E/M Coding www.aapc.com 39
Presentation
2014 CPT® Update*This chart should only be used for the purpose of guiding discussion: it references new outpatient visits
2014 CPT® Update
Scale of 1-5• Levels 3-5* are reserved for “sick” or injured patients.
– Lower levels are for patients who present with minor and/or well controlled condition/s.
*This presentation refers to levels of service for outpatient visits.

40 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• How sick is sick?– Scale of 1-3
• Level One hospital visit is for a patient who is getting better• Level Two hospital visit is for a patient who isn’t getting better• Level Three for a patient who is rapidly declining.
Hospital Patients
35
2014 CPT® Update
Sickest (5/3)
• Presenting Problem: An illness or injury that poses a threat to life, chronic severely exacerbated, abrupt change in neurological status– Typically the patient’s situation is serious, imminent, and uncertain• Severe exacerbation of CHF• Patient presents confused in diabetic ketoacidosis • Morphine Sulfate IVP ordered for chest pain not controlled by Nitro• Patient brought by parents after a failed suicide attempt• Patient post fall on ski slopes with extradural hematoma

Unlock the Secret to E/M Coding www.aapc.com 41
Presentation
2014 CPT® Update
Sick (3/1)
• Typical Presenting Problem: 1 –2 minor, 1-2 stable chronic, 1-2 acute uncomplicated– Typically the diagnosis is known and/or made during the encounter– Future follow up is often classifiable as routine
• Patient returns with productive cough x 10 days for antibiotic• Patient with choroidal revascularization to assess efficacy of anti-VEGF• Follow up Patient with cystocele not requiring treatment • Patient in follow up with stable angina and no new symptoms• Return visit for patient with worsening plantar fasciitis• Non pregnant female with resolving hyperemesis • Patient with well controlled hypertension and hypercholestorolemia
2014 CPT® Update
Sicker (4/2)
• Presenting Problem: 2-3 stable chronic, chronic exacerbated, acute with systemic symptoms or injury
– Typically the diagnosis is known and worsening/complicated or further testing is required– Future follow up is often classifiable as routine or sooner
• Patient with choroidal revascularization now with new central vision loss • Patient in follow up with stable angina, not tolerating medication • Patient with suspected cellulitis of the lower leg• Patient with heel ulcer and drainage

42 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• SECRET #2 – The best way to communicate with physicians is to ask questions that
allow them to draw their own conclusions.• Your goal is to promote effective communication
– Ask questions that are not answered with yes or no– “what made you more concerned about this patient encounter than the
other one?” versus • “did you understand what makes this a Level Four?”
CDI and Educating the Physician
39
2014 CPT® Update
• Tell me about your worst patient case---how did the patient present? Was the patient at risk for lost life or bodily function?
• Would a non-friendly peer agree that the patient was “sicker” ---albeit not at imminent risk for lost life or bodily function?
• Is it reasonable that this “sicker” patient needs to be seen in follow-up shortly?
• What lesser but related problem would have you less concerned?
Sample Questions
40

Unlock the Secret to E/M Coding www.aapc.com 43
Presentation
2014 CPT® Update
• Listen: Don’t think about what you will say next while the physician is talking • Have a clear idea of what you want to say so you can be organized in your delivery
– Example: • “Doctor, I have reviewed this patient encounter, and your superbill. You selected a
Level Four. You saw this patient 1 month ago for premenopausal syndrome mood swings and prescribed Zoloft. You saw her again today in follow-up. You repeated a comprehensive history and exam. She is doing well with reduced mood swings and will continue with sertraline 50MG. You ask to see her back in 12 months or PRN if there is a change. I am concerned that an auditor might question the higher Level of service being billed because you are not seeing her back for 12 months and there are no other problems documented. What was it about this patient that put her at a higher Level of concern to be coded at a Level Four?”
Effective Communication
41
2014 CPT® Update
• Body language mistakes to avoid are: – Arms crossed: You are defensive.– Constant eye contact: You are aggressive. – Fidgeting: You are bored or impatient – Hunched Posture: You lack confidence. – Little eye contact: You have low interest or lack confidence. – Rubbing your nose or mouth: You are lying or unsure of yourself.– Tapping: You are impatient or nervous. – Touching your face or hair: You are timid.– Watching the time: You are anxious to move on to something else.
Watch Your Body Language
42

44 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
• Always customize CDI– Run a productivity report of the last one to three months of Outpatient visits that
shows the top diagnosis codes used and the frequency of their use. – Ask Questions: Dr., what about these diagnoses make you more (i.e. 4) or less (i.e. 3)
concerned about a patient?• See Example Dr. ABC, Urologist: Workbook Page 23• See Example Dr. DEF, Dermatologist: Workbook Page 24
Provider Interview
43
2014 CPT® Update
• Do any of these pose a threat to life or bodily function within 24-48 hours? (Level Five)• Under what circumstances would you need to see a patient back in follow-up sooner than is
typically required? (Level Four)• Which patient problems have you very concerned for the patient but do not pose an imminent
threat to life or bodily function? (Level Four) • Which of these can commonly be diagnosed on the first encounter and do not usually require a
prompt follow-up? (Level Three)• Which of these problems might you bring a patient back for a quick check, and on doing so
discover no further medical management is needed? (Level Two)• Which of these diagnoses are self-limited and require reassurance with no active medical
management? (Level One) • Would a non-friendly medical peer agree with your decisions?
Sample Interview Questions
44

Unlock the Secret to E/M Coding www.aapc.com 45
Presentation
2014 CPT® Update
• The E/M CDI conversation can easily be conducted at the same time as ICD-10• Group discussion / Critical Thinking Exercise
– Review page 26 Example Dr. GHI, Orthopedic Surgeon (Hand)– This is a report of 2 months use of ICD-9 codes sorted by frequency.1. Which codes require the provider to consider additional documentation for granularity?2. What are the considerations you should make before training? 3. Would it make sense to discuss documenting requirements after discussing Medical
necessity? If so, should you discuss MDM first?
Combining ICD‐10 CDI Training Sessions
45
2014 CPT® Update
• SECRET #3 – Coders, unlike any other position in healthcare, are capable of helping
physicians.
Mastering a Good Coder-Physician Relationship
46

46 AAPC 1-800-626-CODE (2633) CPT® copyright 2013 American Medical Association. All rights reserved.
Presentation
2014 CPT® Update
Sir Luke Fildes’s 1891 painting ‘The Doctor.’
47
2014 CPT® Update
• 80% of those in pre-med will not be accepted to medical school• Medical school
– Average student financial debt in 2012 was $166K– The majority of students will graduate with debt of at least $150,000
Appreciating Physician Development

Unlock the Secret to E/M Coding www.aapc.com 47
Presentation
2014 CPT® Update
Growing Numbers Need Help• 700K physicians in the US
– 63% (442K) bill E&M services
– 20% (and growing) are employed by hospitals
• 63K fewer doctors than needed by 2015
• 33% are in Private practice ↓ From 57% in 2007
• 46% would NOT choose medicine again as a career
• On again, off again regulations (SRG, ICD-10),
• Difficult rules (E/M, HIPAA, MU), high costs (malpractice)
2014 CPT® Update
CEU Number is: [ Insert Number ]“Medicine is the only profession that labours incessantly to destroy the reason for its ownexistence.” ~James Bryce, 1914
About the Author:Stephanie Cecchini, CPC, CEMC, CHISP, AHIMA Approved ICD‐10 Trainer, VP Coding Operations joined Aviacode in 2012 where she continues hercommitment to best serve the revenue cycle management needs of physicians and the healthcare community. She is an executive Level consultant withsignificant healthcare business experience. Stephanie is an expert in clinical documentation requirements for coding and billing to Medicare, Medicaid and alllines of commercial payer business. She brings to her position more than eighteen years’ involvement in healthcare regulations including: coding and billingcompliance, HIPAA privacy, security, and transactions, and HITECH “meaningful use” compliance. Previously, Stephanie served as SVP at the American Societyof Health Informatics Managers, working to fill the needs of physicians adopting Health IT and at its sister organization, AAPC as VP, Product Management. Inprior roles she served as Chief Audit Officer for Parses, Inc., designing audit programs for payers and managing overpayment recovery. As a public speaker andpublished writer, she is a nationally respected advocate of fair and proper payment for medical services. Stephanie lives in Salt Lake City, Utah with herhusband Jim and their three children.
• Stephanie is LION (Linked In Open Network).
http://www.linkedin.com/in/StephanieCecchini
Questions?
50