Embed Size (px)
Citation preview
FETAL ALCOHOL SPECTRUM DISORDERS:RELEVANCE TO FOSTER CARE.
Understanding, Identifying, and Helping theHighest Risk Babies, Children, & Caregivers
Ann Streissguth Fetal Alcohol & Drug Unit
University of Washington Medical SchoolSeattle
http://depts.washington.edu/fadu/1-20-05
FETAL ALCOHOL SPECTRUM DISORDERS:RELEVANCE TO FOSTER CARE
Ann Streissguth 9:30-10:30Nancy Whitney 10:30-10:50Break 10:50-11:10Therese Grant 11:10-12:00Julie Gelo 12:00-12:30Group Discussion 12:30-1:30Adjourn 1:30
- IN GRATITUDE -THIS RESEARCH FUNDED BY:
National Institute on Alcohol & AlcoholismCenters for Disease Control
Indian Health ServiceSpencer Foundation, Thrasher Foundation
UW Alcoholism & Drug Abuse InstituteFoundations Fund for Research in PsychiatryUW Medical Student Research Training PrgmUW Royalty Research Fund, Dana Foundation
Center for Substance Abuse PreventionMarch of Dimes, Robert Wood Johnson
Washington State DSHS
This Work is Done by a TeamThis Work is Done by a Team-- In GratitudeIn Gratitude -- My Colleagues:My Colleagues:
•• David Smith & Ken Jones, 1973David Smith & Ken Jones, 1973
•• Jim Hanson, John Graham, Sterling Clarren, Jon Aase Jim Hanson, John Graham, Sterling Clarren, Jon Aase •• Paul Paul LemoineLemoine, Philippe Dehaene, Philippe Dehaene
•• Donald Martin, Donald Martin, Helen Barr, Paul Sampson, Fred BooksteinHelen Barr, Paul Sampson, Fred Bookstein
•• Joan Martin, Sharon L. Ramey, Cindy Herman, Betty DarbyJoan Martin, Sharon L. Ramey, Cindy Herman, Betty Darby
•• Heather C. Olson, Robin Heather C. Olson, Robin LaDueLaDue, , Paul Connor, Janet HugginsPaul Connor, Janet Huggins
•• Therese Grant, Cara Ernst, Pam PhippsTherese Grant, Cara Ernst, Pam Phipps
•• David David HaynorHaynor Christine Gleason, Raymond Christine Gleason, Raymond SzeSze
•• Kieran OKieran O’’Malley, Kay Kelly, Eric SchnapperMalley, Kay Kelly, Eric Schnapper
““23,000 children (Birth to age 5)23,000 children (Birth to age 5)are accepted into are accepted into
Child ProChild Protective Services each year.tective Services each year.
Case files are opened on nearlyCase files are opened on nearly5,000 with child abuse & neglect5,000 with child abuse & neglect
-
WASHINGTON STATEWASHINGTON STATE
Seattle Times, Dec 3, 2004: Debra Seattle Times, Dec 3, 2004: Debra RonnholmRonnholm & Rep. Ruth & Rep. Ruth KajiKaji
““Therapeutic treatment available forTherapeutic treatment available foronly 250 of the 4,800 childrenonly 250 of the 4,800 children
designated to need help.designated to need help.
State Budget is only $7 million State Budget is only $7 million per year for neglected & abused infantsper year for neglected & abused infants
Approximately 1% of state fundingApproximately 1% of state fundingfor correctionsfor corrections ““
-
WASHINGTON STATEWASHINGTON STATE
Seattle Times, Dec 3, 2004: Debra Seattle Times, Dec 3, 2004: Debra RonnholmRonnholm & Rep. Ruth & Rep. Ruth KajiKaji
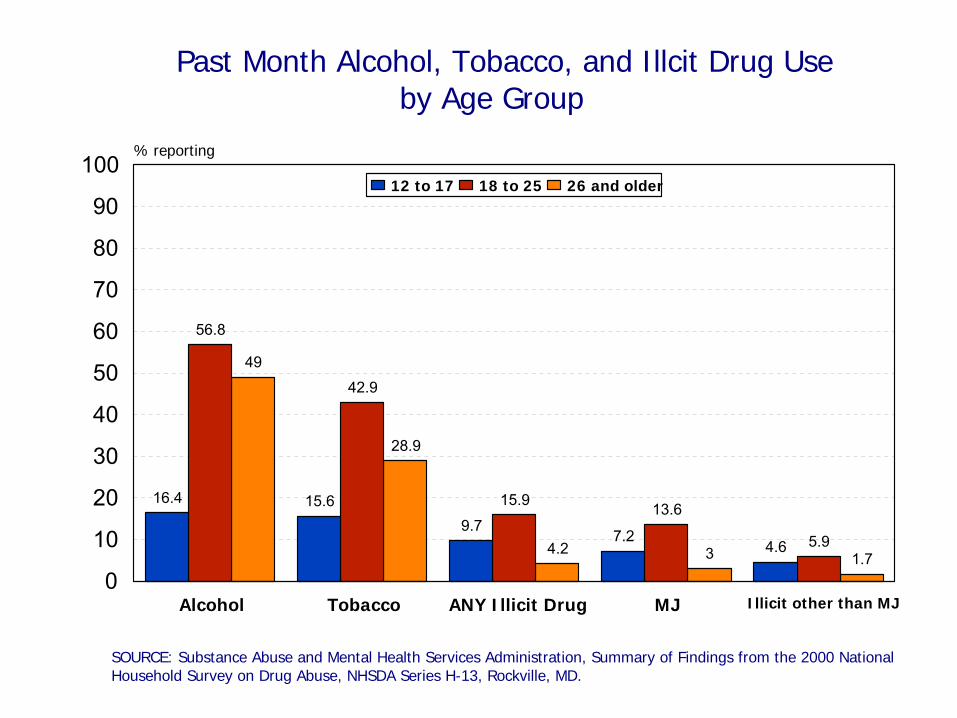
Past Month Alcohol, Tobacco, and Illcit Drug Use by Age Group
SOURCE: Substance Abuse and Mental Health Services Administration, Summary of Findings from the 2000 National Household Survey on Drug Abuse, NHSDA Series H-13, Rockville, MD.
16.4 15.69.7
7.24.6
56.8
42.9
15.9 13.6
5.9
49
28.9
4.2 3 1.7
Alcohol Tobacco ANY Illicit Drug MJ Illicit other than MJ0
10
20
30
40
50
60
70
80
90
100% reporting
12 to 17 18 to 25 26 and older
BOTH THE MOTHERBOTH THE MOTHERAND THE INFANTAND THE INFANT
ARE OUR TARGETSARE OUR TARGETS
For Prevention and Intervention:
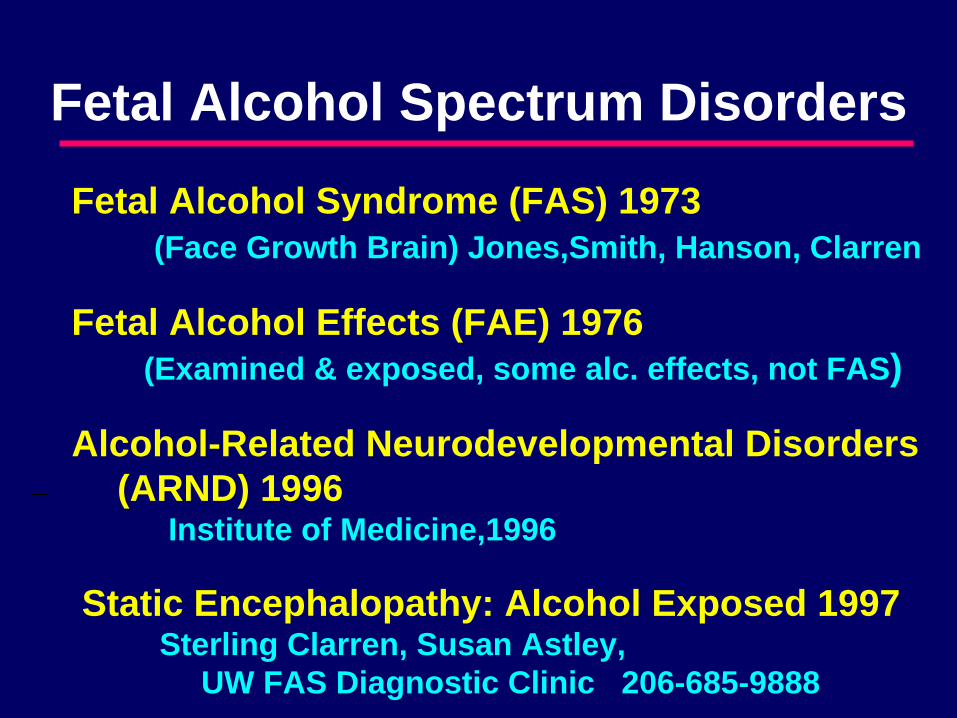
Fetal Alcohol Spectrum Disorders
Fetal Alcohol Syndrome (FAS) 1973(Face Growth Brain) Jones,Smith, Hanson, Clarren
Fetal Alcohol Effects (FAE) 1976(Examined & exposed, some alc. effects, not FAS)
Alcohol-Related Neurodevelopmental Disorders (ARND) 1996
Institute of Medicine,1996
Static Encephalopathy: Alcohol Exposed 1997Sterling Clarren, Susan Astley,
UW FAS Diagnostic Clinic 206-685-9888
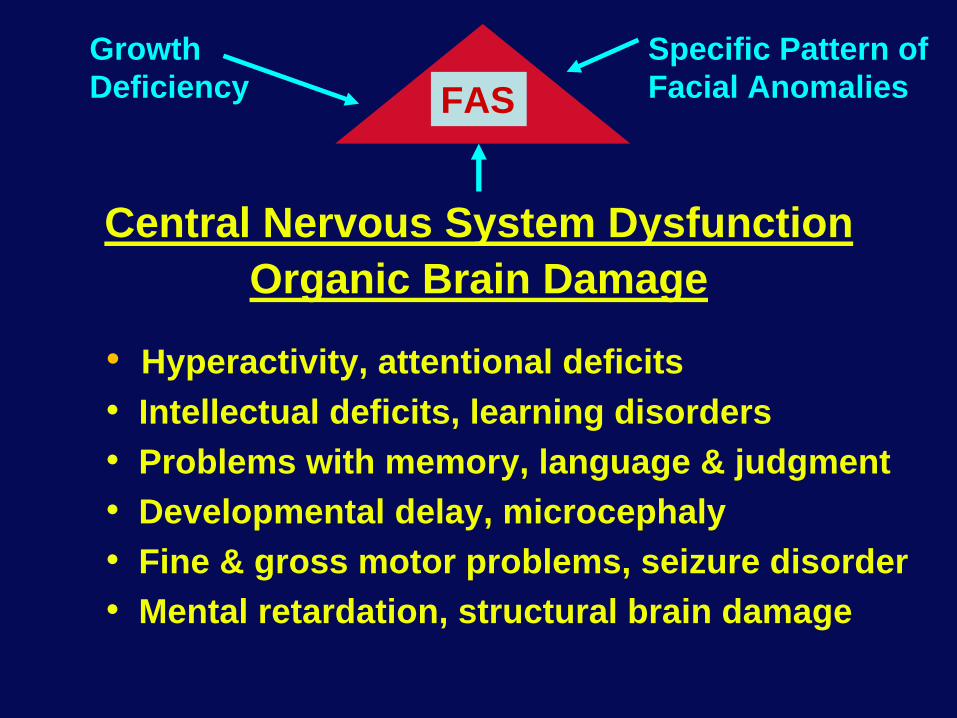
FAS
Central Nervous System Dysfunction Organic Brain Damage
• Hyperactivity, attentional deficits• Intellectual deficits, learning disorders• Problems with memory, language & judgment• Developmental delay, microcephaly• Fine & gross motor problems, seizure disorder• Mental retardation, structural brain damage
Growth Deficiency
Specific Pattern of Facial Anomalies
FAE
Central Nervous System Dysfunction Organic Brain Damage
• Hyperactivity, attentional deficits• Intellectual deficits, learning disorders• Problems with memory, language & judgment• Developmental delay, microcephaly• Fine & gross motor problems, seizure disorder• Mental retardation, structural brain damage
ARND
Central Nervous System Dysfunction Organic Brain Damage
• Hyperactivity, attentional deficits• Intellectual deficits, learning disorders• Problems with memory, language & judgment• Developmental delay, microcephaly• Fine & gross motor problems, seizure disorder• Mental retardation, structural brain damage
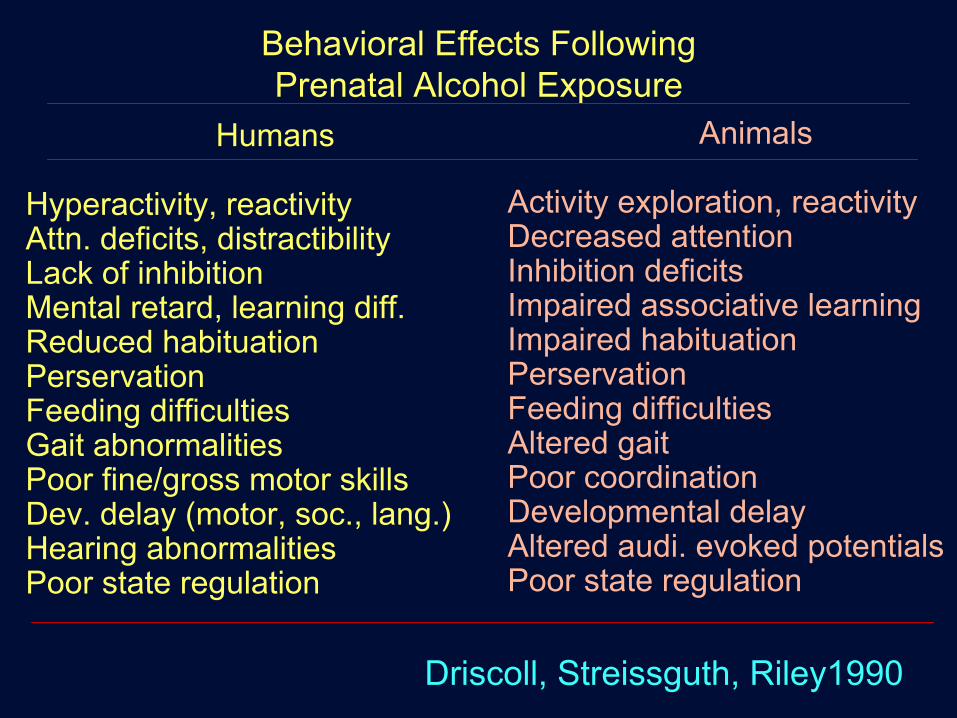
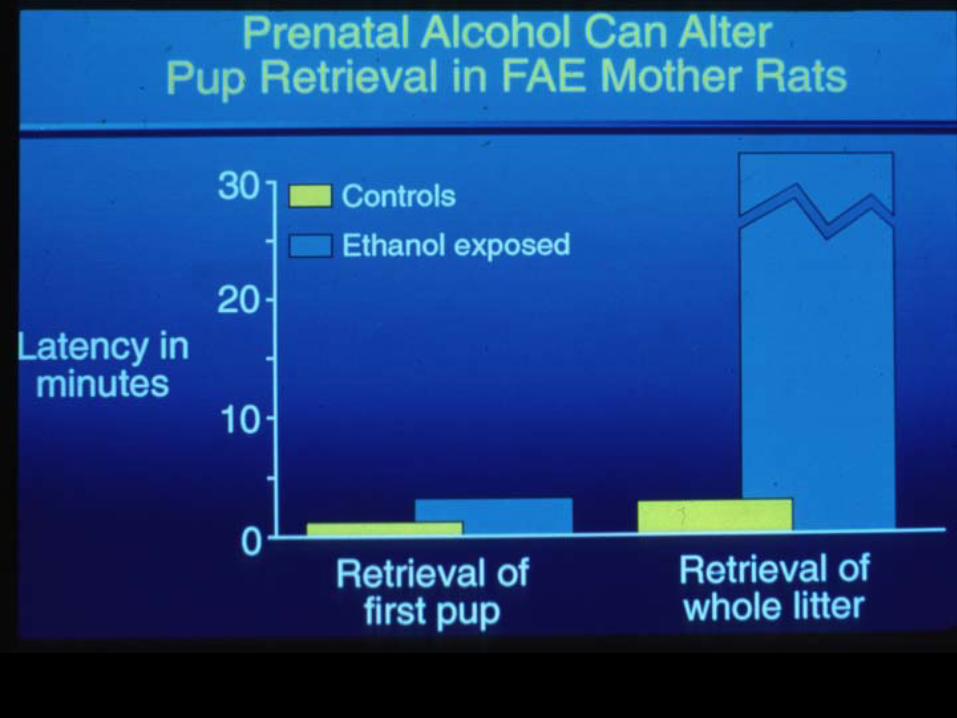
Behavioral Effects Following Prenatal Alcohol Exposure
Humans
Hyperactivity, reactivityAttn. deficits, distractibilityLack of inhibitionMental retard, learning diff.Reduced habituationPerservationFeeding difficulties Gait abnormalitiesPoor fine/gross motor skillsDev. delay (motor, soc., lang.)Hearing abnormalitiesPoor state regulation
Animals
Activity exploration, reactivityDecreased attentionInhibition deficitsImpaired associative learningImpaired habituationPerservationFeeding difficultiesAltered gaitPoor coordinationDevelopmental delayAltered audi. evoked potentials Poor state regulation
Driscoll, Streissguth, Riley1990

YASR, BSI
Behavioral Ratings
Alcohol & Drug Use
Delivery Day 1
BrazeltonNeonatal
Scale
NaturalisticObservations
HumanEmbryology
MedicalRecords
Neuro-pathology
DysmorphologyExam
BaselineSuckingPressure
OperantHeadturningor Sucking
Bayley Mental &Motor Exam
Behavior RatingsMeasurementsParent Interview
Health HxProblems
Environment
NIMH AttentionBattery
Memory batteryCognitive/Motor
BatteryMeasurementsPhotographs
Behavior RatingsHealth InterviewAdolescent
questionnaireParent Interview
Health HxProblemsEnvironment
WISC-R (IQ)WRAT-RNeurobehavioralBattery
CPT VigilanceMeasurementsPhotographs
Behavior RatingsParent Interview
Health HxProblemsEnvironment
WPPSI (IQ)Fine Motor TestTPT Tactual
Performance TestGross Motor TestVigilance TestActivityAssessmentMeasurements
PhotographsBehavior RatingsParent Interview
Health HxProblemsEnvironment
DysmorphologyExam
Hospital Lab Mail Lab
MaternalInterviewat Home
v v
Home
CaldwellHOME
at 12 MonthsTeacher ratings
(Myklebust)at 8 Years
Teacher ratings-Behavior-Academics
AchievementTest Scores
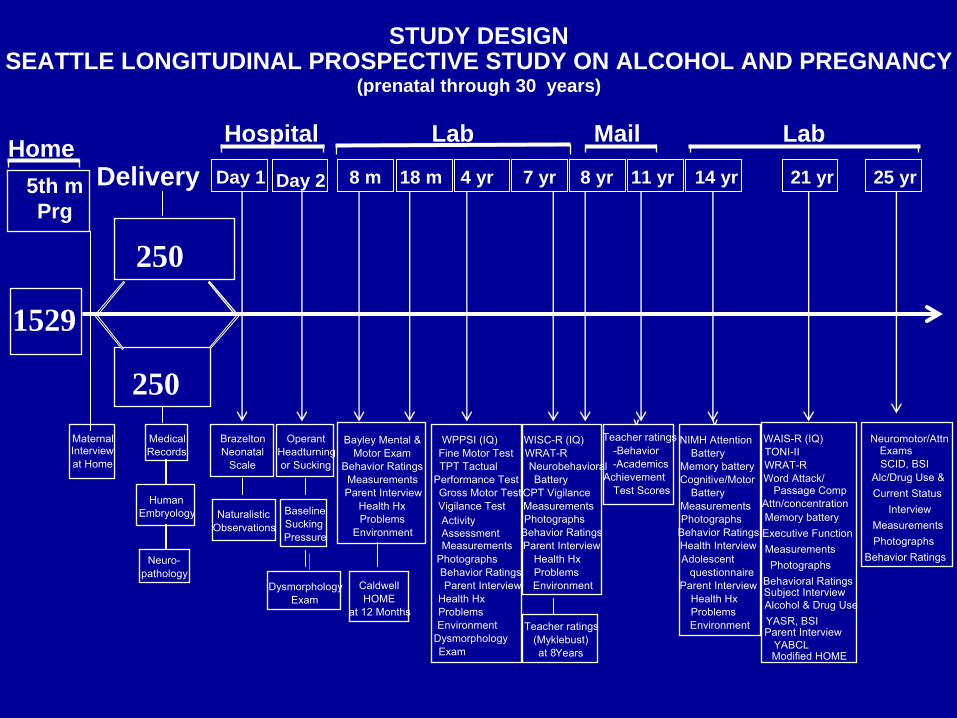
STUDY DESIGNSEATTLE LONGITUDINAL PROSPECTIVE STUDY ON ALCOHOL AND PREGNANCY
(prenatal through 30 years)
WAIS-R (IQ)TONI-IIWRAT-RWord Attack/
Passage Comp Attn/concentrationMemory batteryExecutive FunctionMeasurementsPhotographs
Subject Interview
Parent InterviewYABCLModified HOME
Neuromotor/Attn
SCID, BSIAlc/Drug Use &
Exams
Current Status
MeasurementsPhotographs
Behavior Ratings
Interview
Day 2 8 m 18 m 4 yr 7 yr 8 yr 11 yr 14 yr 21 yr 25 yr
250
1529
250
5th mPrg
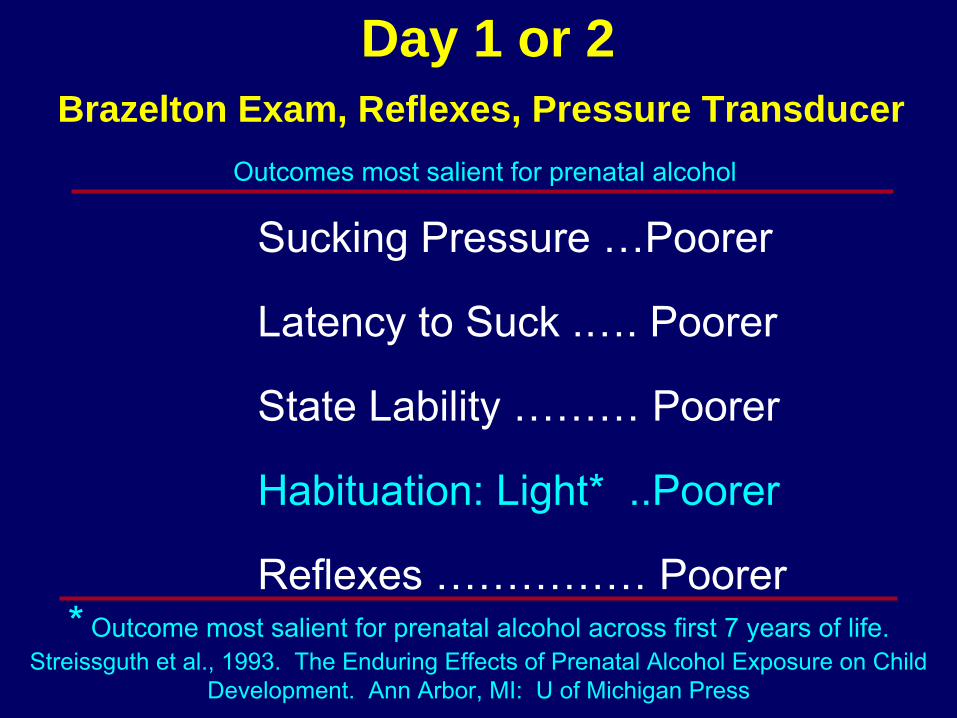
Brazelton Exam, Reflexes, Pressure Transducer
Day 1 or 2
Sucking Pressure …Poorer
Latency to Suck .…. Poorer
State Lability ……… Poorer
Habituation: Light* ..Poorer
Reflexes …………… Poorer* Outcome most salient for prenatal alcohol across first 7 years of life.
Streissguth et al., 1993. The Enduring Effects of Prenatal Alcohol Exposure on Child Development. Ann Arbor, MI: U of Michigan Press
Outcomes most salient for prenatal alcohol
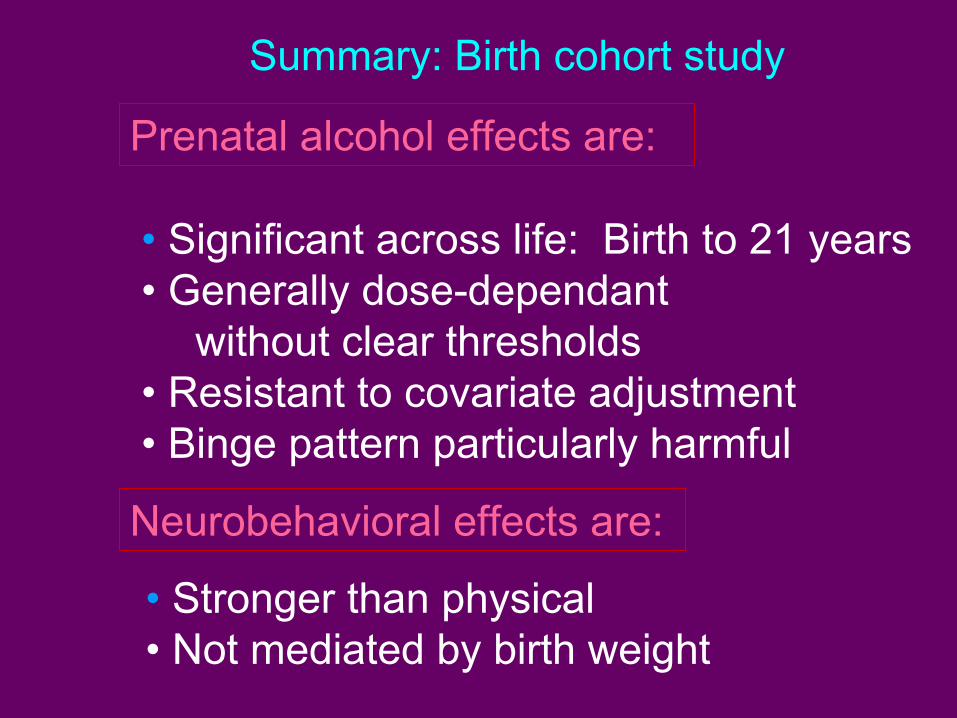
Summary: Birth cohort study
• Significant across life: Birth to 21 years• Generally dose-dependant
without clear thresholds• Resistant to covariate adjustment• Binge pattern particularly harmful
Prenatal alcohol effects are:
Neurobehavioral effects are:
• Stronger than physical• Not mediated by birth weight
• Excessive cell death• Reduced cell proliferation• Migrational errors in brain development• Inhibition of nerve growth factor• Disruption of neurotransmitters
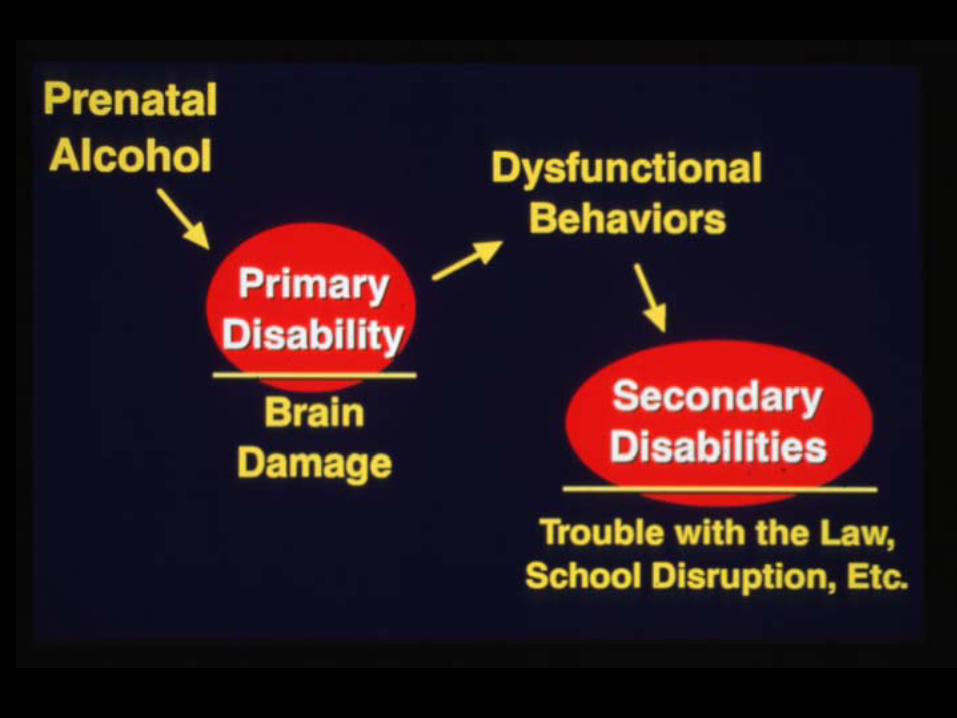
HOW DOES ALCOHOL CAUSEBRAIN DAMAGE?
ALCOHOL CAUSES:CAUSES:

SECONDARY DISABILITIES IN Fetal Alcohol Spectrum Disorders
• Not raised in a stable, nurturant home*• Not diagnosed at an early age* • 72% experienced sexual or physical abuse• Changing households every two to three years• Not receiving Developmental Disabilities Services(All were born to mothers who abused alcohol)
RISK FACTORS
For Secondary Disabilities in FASD
PROTECTIVE FACTORS
• Living in a stable & nurturant home• Receiving an early diagnosis
MULTIVARIATE ANALYSES SHOWEDTWO STRONG
PROTECTIVE FACTORS
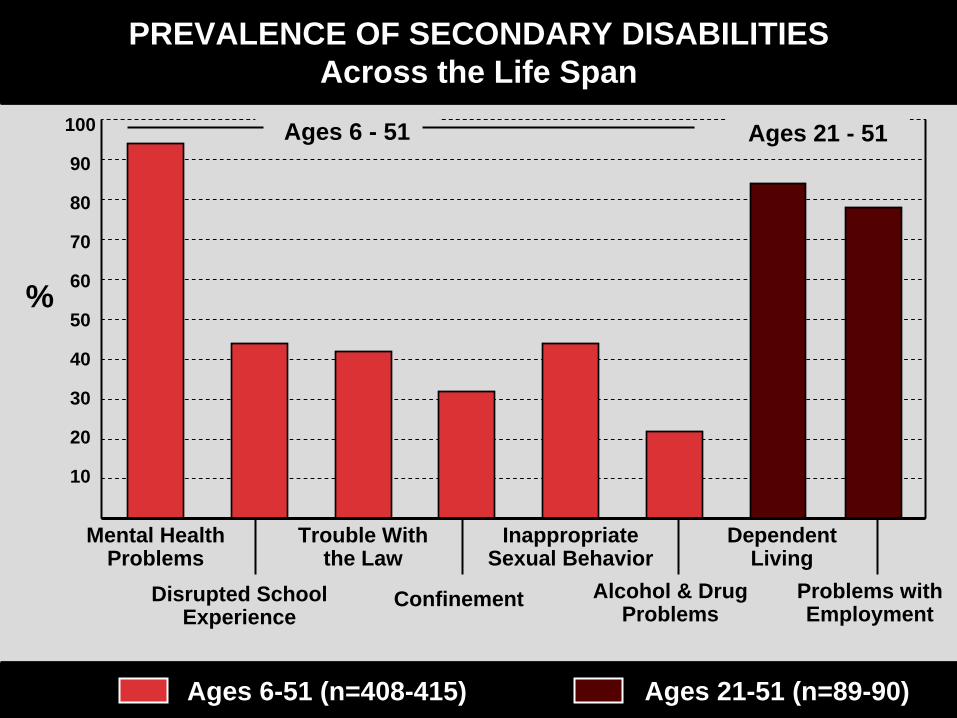
PREVALENCE OF SECONDARY DISABILITIESAcross the Life Span
100
90
80
70
60
50
40
30
20
10
Ages 6-51 (n=408-415) Ages 21-51 (n=89-90)
%
Mental Health Problems
Disrupted School Experience
Trouble With the Law
Confinement
Inappropriate Sexual Behavior
Alcohol & Drug Problems
Dependent Living
Problems with Employment
Ages 6 - 51 Ages 21 - 51
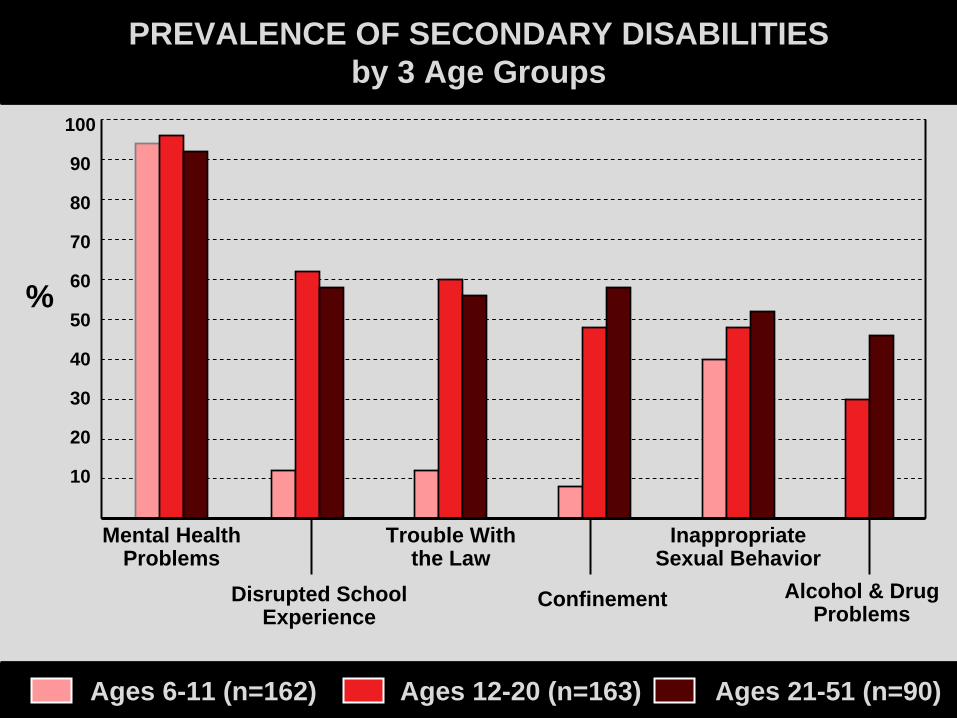
PREVALENCE OF SECONDARY DISABILITIESby 3 Age Groups
100
90
80
70
60
50
40
30
20
10
Ages 6-11 (n=162) Ages 12-20 (n=163) Ages 21-51 (n=90)
%
Mental Health Problems
Disrupted School Experience
Trouble With the Law
Confinement
Inappropriate Sexual Behavior
Alcohol & Drug Problems
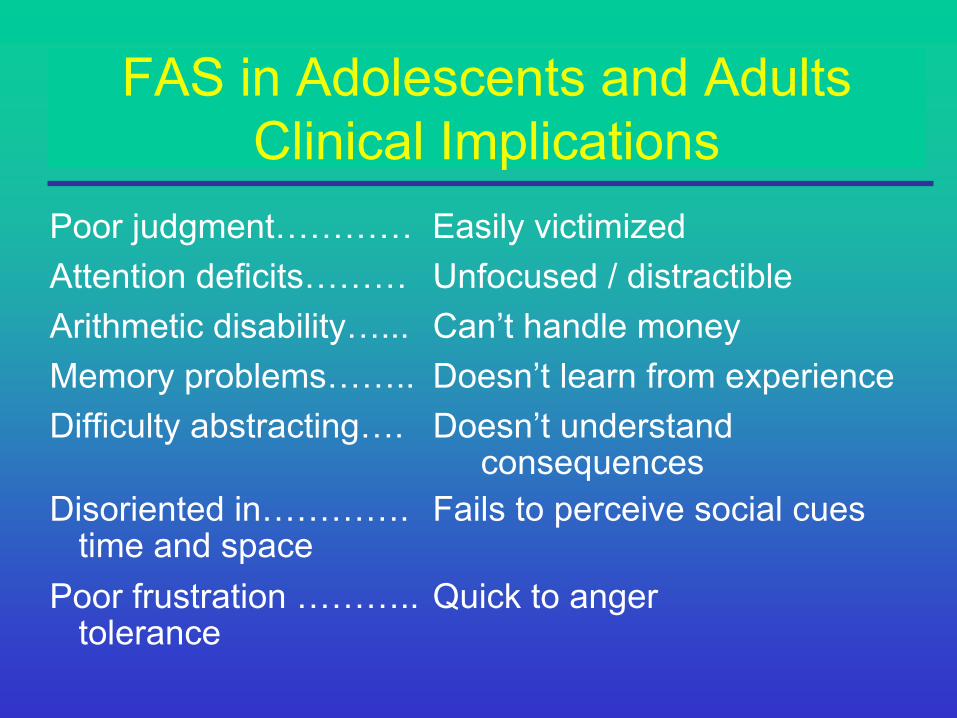
FAS in Adolescents and AdultsClinical Implications
Poor judgment………… Easily victimizedAttention deficits……… Unfocused / distractibleArithmetic disability…... Can’t handle moneyMemory problems…….. Doesn’t learn from experienceDifficulty abstracting…. Doesn’t understand
consequencesDisoriented in…………. Fails to perceive social cues
time and spacePoor frustration ……….. Quick to anger
tolerance
1. Ask if their mother had an alcohol1. Ask if their mother had an alcoholproblem?problem?
2. Ask if they sometimes 2. Ask if they sometimes do the same do the same dumb things over and over?dumb things over and over?
3. Ask if they have trouble managing 3. Ask if they have trouble managing money?money?
4. Give an informant the FABS 4. Give an informant the FABS 5. Help them get help.5. Help them get help. -
IF YOU HAVE A CLIENT LIKE THIS:
DETECTION

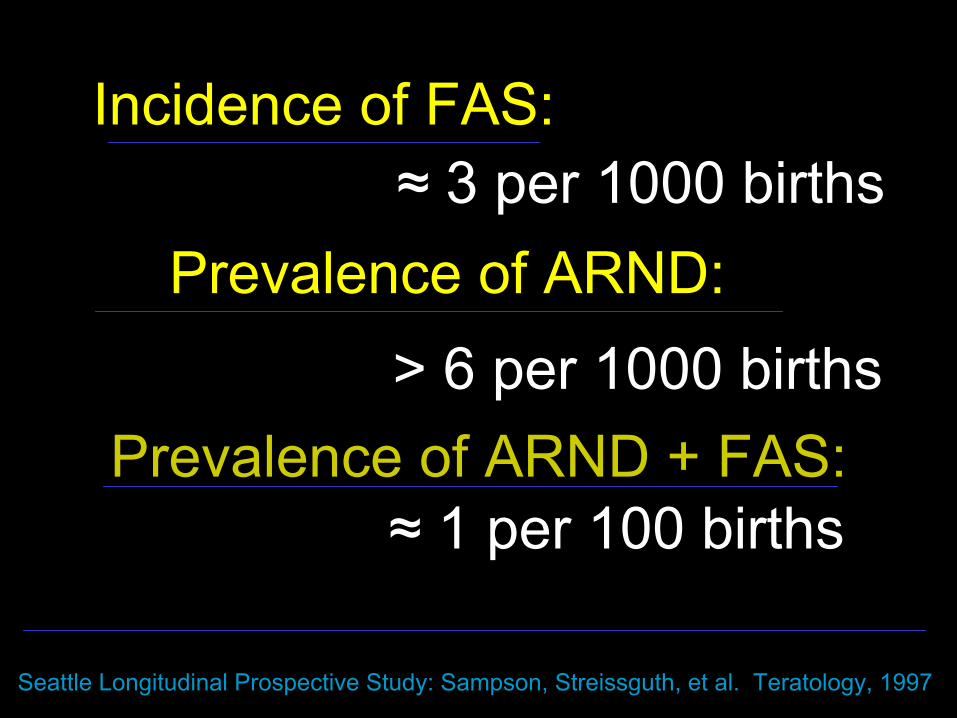
Incidence of FAS:
Prevalence of ARND: ≈ 3 per 1000 births
> 6 per 1000 births
Seattle Longitudinal Prospective Study: Sampson, Streissguth, et al. Teratology, 1997
Prevalence of ARND + FAS:≈ 1 per 100 births
100
80
60
40
20
0
%
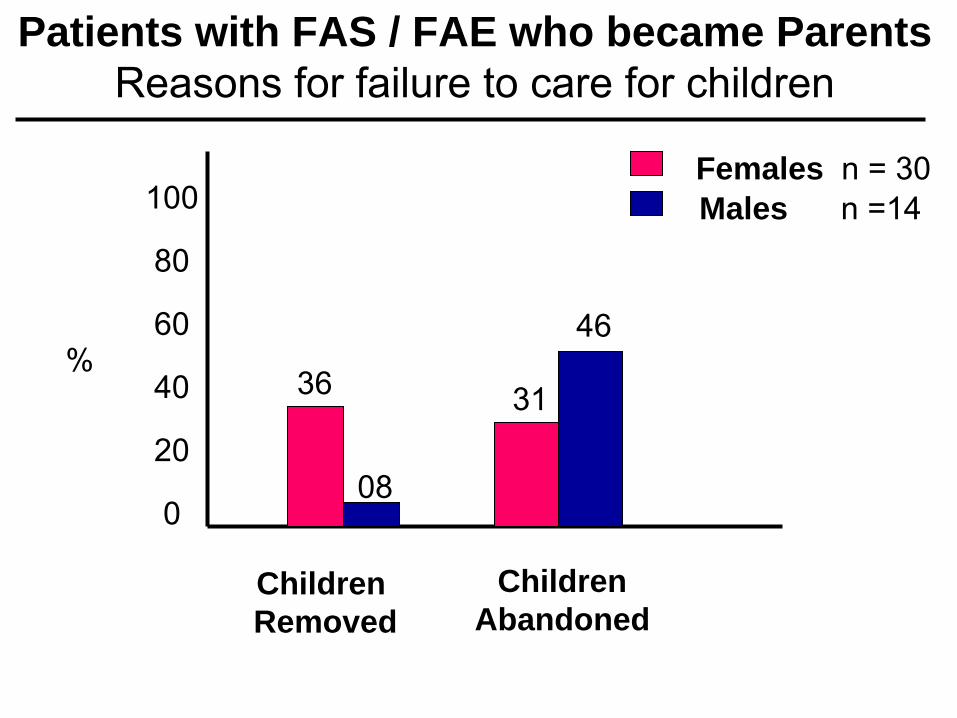
Males n =14
36
08
31
46
Patients with FAS / FAE who became ParentsReasons for failure to care for children
ChildrenRemoved
ChildrenAbandoned
Females n = 30
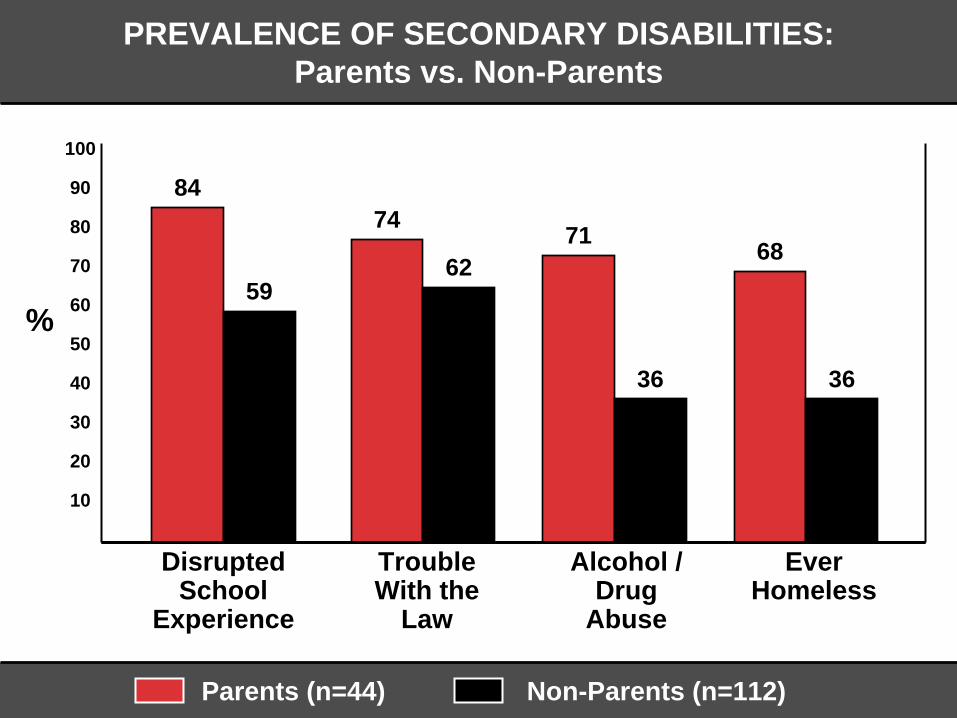
PREVALENCE OF SECONDARY DISABILITIES:Parents vs. Non-Parents
100
90
80
70
60
50
40
30
20
10
Parents (n=44) Non-Parents (n=112)
%
DisruptedSchool
Experience
Trouble With the
Law
Alcohol /Drug
Abuse
EverHomeless
84
59
74
6271
36
68
36
DETECTION
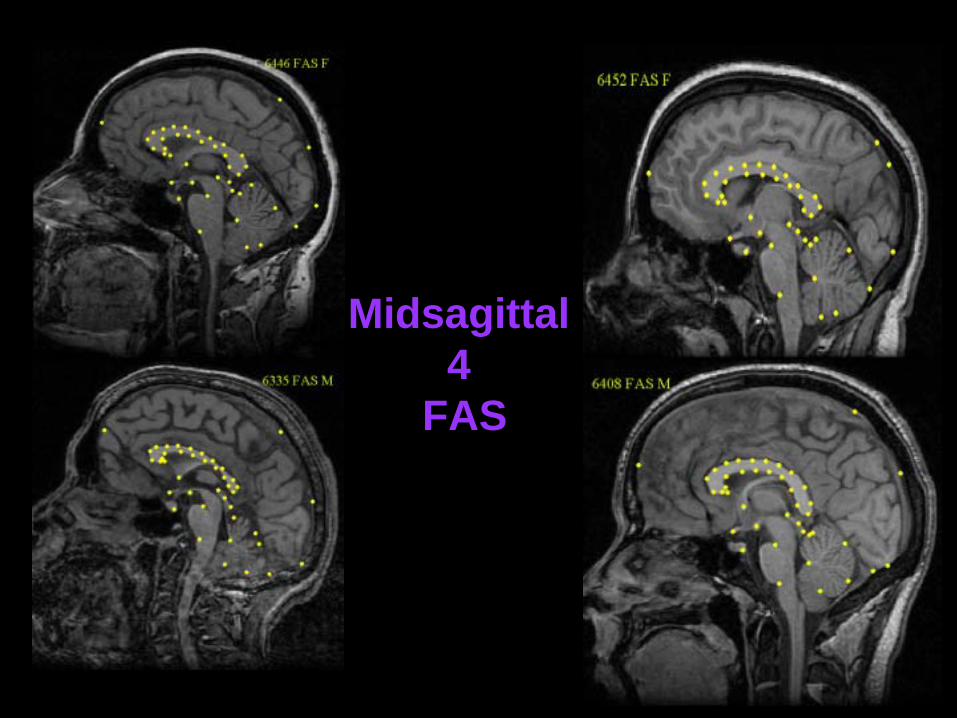
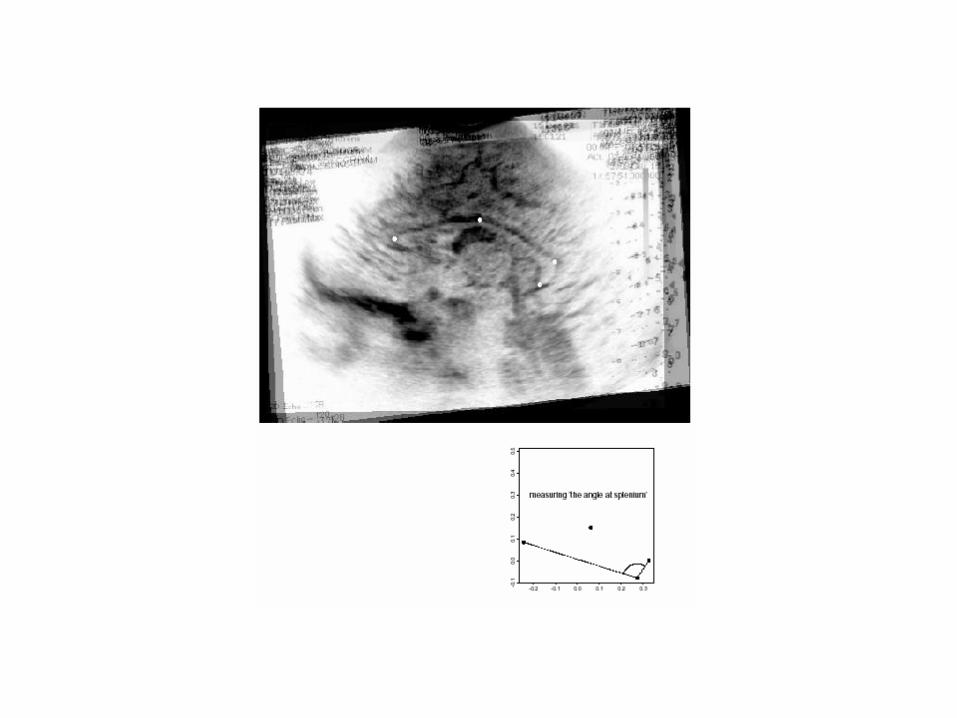
Midsagittal4
FAS
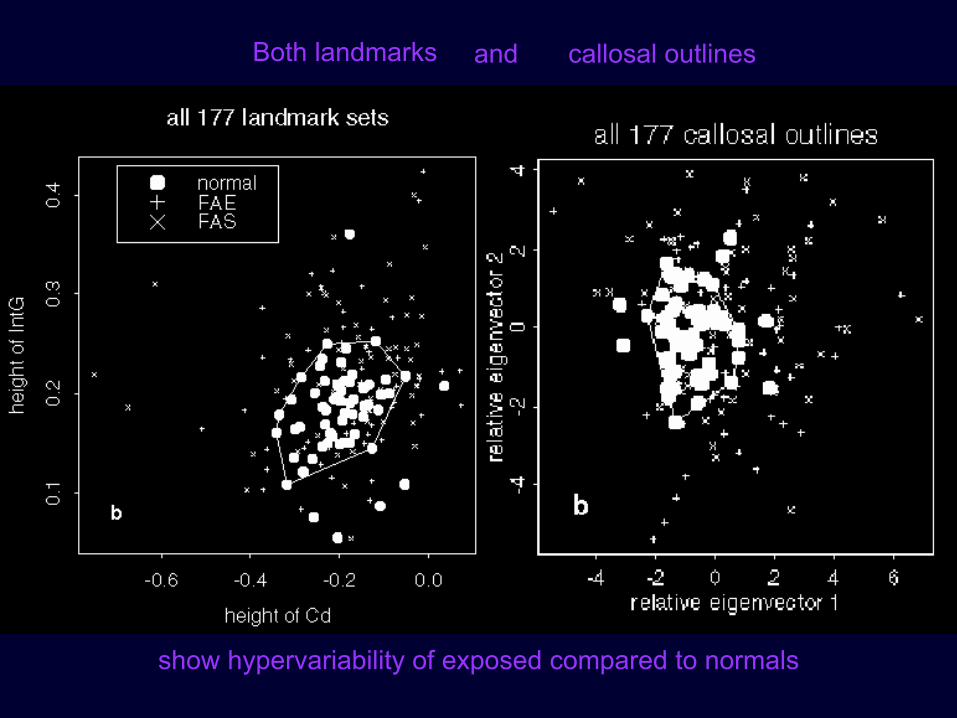
Both landmarks callosal outlinesand
show hypervariability of exposed compared to normals
Midline Corpus Midline Corpus CallosumCallosuma a NeuroanatomicNeuroanatomic FocusFocus
of Fetal Alcohol Damageof Fetal Alcohol Damage **
100/117 (exposed detected) = 85% sensitivity100/117 (exposed detected) = 85% sensitivity49/60 (unexposed not detected) = 82% specificity49/60 (unexposed not detected) = 82% specificity
FAS vs. FAE = indistinguishableFAS vs. FAE = indistinguishableThe finding is for The finding is for HYPERVARIABILITY of SHAPEHYPERVARIABILITY of SHAPE,,
Not for mean size or volumesNot for mean size or volumes
** Bookstein, Sampson, Connor, Streissguth, 2002 Bookstein, Sampson, Connor, Streissguth, 2002 New Anatomist;New Anatomist;Bookstein et alBookstein et al, 2001, 2001 TeratologyTeratology
Corpus Corpus CallosumCallosum Shape and Shape and Neuropsychological Deficits Neuropsychological Deficits **90 adult males : 30 FAS, 30 FAE, 30 unexposed90 adult males : 30 FAS, 30 FAE, 30 unexposed
Bookstein, Streissguth, Sampson, Connor, Barr. Bookstein, Streissguth, Sampson, Connor, Barr. 2002 2002 NeuroImageNeuroImage
Excess shape variation in exposed patients relates to: Excess shape variation in exposed patients relates to:
•• Thinner CC with deficits in motor functionThinner CC with deficits in motor function•• Thicker CC with deficits in executive functionThicker CC with deficits in executive function
12 min MRI, 5 hr. test battery12 min MRI, 5 hr. test battery
Two different profiles of behaviorTwo different profiles of behavior
BEHAVIORAL PHENOTYPE: FASDPoor EXECUTIVE FUNCTION*
1. Difficulty organizing stored informationto plan future activities
2. Difficulty regulating and sequencing behavior 3. Difficulty inhibiting responses4. Lack of cognitive flexibility
(Wisconsin Card Sort, Stroop, Trails, Ruff’s Figural Fluency, Consonant Trigrams)
*Connor, Sampson,Bookstein, Barr & Streissguth 2000Developmental Neuropsychology
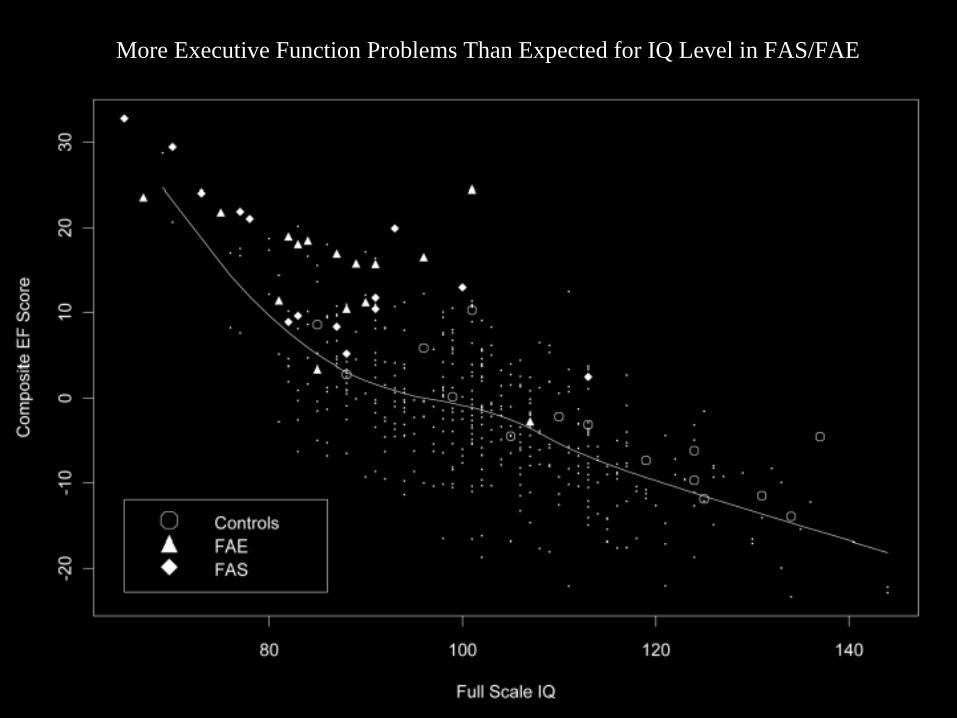
PMore Executive Function Problems Than Expected for IQ Level in FAS/FAE
BEHAVIORAL PHENOTYPE: FASDPoor Habituation: *
Difficulty Modulating Incoming Stimuli
1. Gets overstimulated in social situation (as in a crowded room, or among strangers)
2. Overreacts to situations with surprisingly strong emotional reactions
3. Displays rapid mood swings set off by seemingly small events
4. Has poor attention spans5. Has trouble completing tasks
*Fetal Alcohol Behavioral Scale (FABS), parent report, Streissguth Book 1997
Fetal Alcohol Spectrum DisordersFetal Alcohol Spectrum Disordersare Birth Defectsare Birth Defects
caused by caused by prenatalprenatal alcohol,alcohol,
andand
Compounded Compounded postnatallypostnatallyby the consequences of by the consequences of
a mother who abuses alcohol.a mother who abuses alcohol.
KEEP IN MIND:
How can we detect and help families at risk in our own
communities?

- Screen & detect high risk mothers, at pregnancy and delivery
- Be especially alert to mothers and babies with FASD
- Get both mothers and babies into early interventions
- Keep data on what happens
In Our Communities We Must:
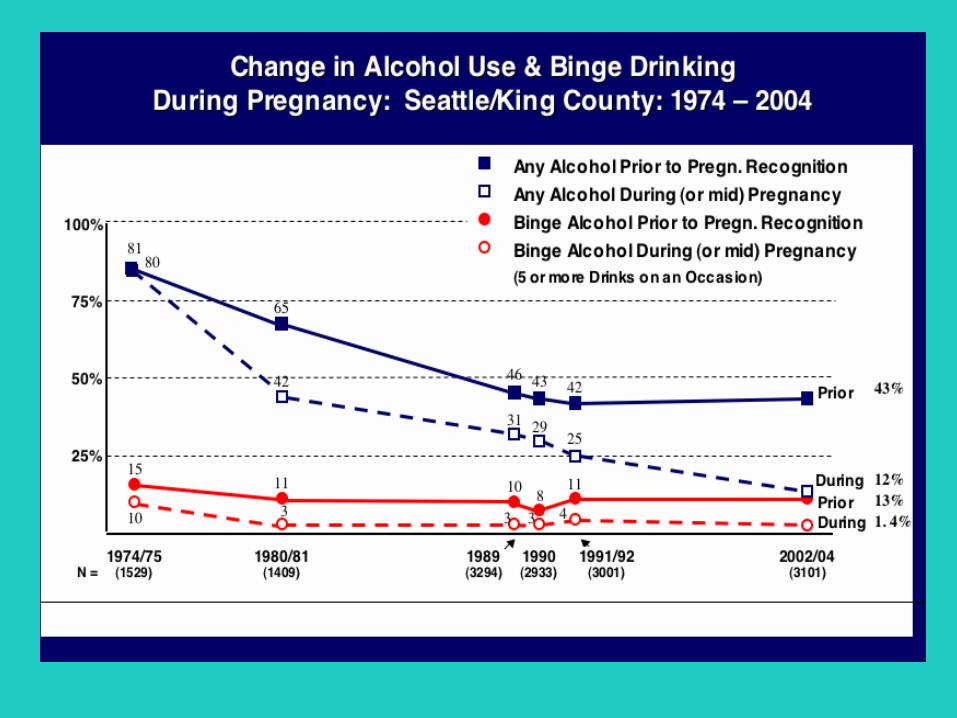
Best predictor of poorchild & adult outcomes
BARC *Calculated from self-reported
frequency of 4 - 5 or more drinks per drinking occasion
*Binge Alcohol Rating CriteriaBarr & Streissguth, 2001.


Fetal Alcohol Spectrum DisordersARE NOT HOPELESS
• An early Diagnosis • Stable, Nurturant, Good Quality Home• Freedom from Personal Violence • Appropriate Institutional Supports
Can prevent secondary disabilities and enhance adult employment and independence
1. Get an early diagnosis for babies1. Get an early diagnosis for babies2. Get help for alcohol2. Get help for alcohol--abusing momsabusing moms3. Get babies into early intervention3. Get babies into early intervention4. Enlist family/peer support4. Enlist family/peer support
-
WELLNESS FOR MOTHER/CHILD
1. Get a diagnosis if FASD suspected1. Get a diagnosis if FASD suspected2. Join an FASD support group2. Join an FASD support group3. Get baby into early interventions3. Get baby into early interventions4. Get trainings from foster4. Get trainings from foster--care care progrmprogrm5. Help child be the best they can be5. Help child be the best they can be6. Watch child for developmental cues6. Watch child for developmental cues7. Provide learning opportunities but7. Provide learning opportunities but
avoid overavoid over--stimulatingstimulating child w/ FASDchild w/ FASD-
WELLNESS FOR CAREGIVERS
““IT IS IN THE SHELTERIT IS IN THE SHELTEROF EACH OTHEROF EACH OTHER
THAT THE PEOPLE LIVETHAT THE PEOPLE LIVE””
-
--IRISH PROVERB--