Embed Size (px)
Citation preview

1
University of Minnesota Medical Center Community Health Needs Assessment (CHNA) Implementation Plan
University of Minnesota Medical Center, Fairview and University of Minnesota Amplatz Children’s
Hospital provide world class, state-of-the-art patient care. The medical center was ranked as the top
hospital in the Twin Cities metro area by U.S. News & World Report in 2012. Together, the medical
center and children’s hospital have 1,600 licensed beds, employ nearly 7,000 people and serve hundreds
of thousands of patients each year. Areas of specialization include organ and blood and marrow
transplantation, heart disease care and prevention, cancer care, the neurosciences and behavioral health.
The medical center and hospital were created in 1997 as a result of a merger between University of
Minnesota Hospital and Clinic and Fairview Health Services. As a division of Fairview, they’re part of a
statewide network of hospitals, primary care and specialty care clinics, home care and hospice services,
pharmacies, senior housing and long-term care facilities.
This implementation plan summarizes the process to date and priorities established for University of
Minnesota Medical Center, Fairview to sustain and develop community benefit programs that 1) address
prioritized needs from the 2012 Community Health Needs Assessment (CHNA) conducted by the medical
center’s CHNA Steering Committee with assistance from Fairview Health Services Community Health
Department and 2) respond to additional identified community health needs.
Target Areas and Populations Fairview Health Services identified the community and assessment area as the population within the zip
codes that comprise the Primary Service Area for University of Minnesota Medical Center, Fairview. The
entire population within this area is included in the assessment; we did not limit our assessment to only
Fairview patients. See appendix A for a map of the assessment area.
How the Implementation Strategy was Developed The medical center’s implementation strategy was developed based on the findings and priorities
established by its CHNA Steering Committee.
University of Minnesota Medical Center, Fairview, along with Fairview Community Health, provided
leadership for the 2012 CHNA. The medical center reached out to members of the community in the
fourth quarter of 2011, asking a diverse group of community leaders to represent the community by
becoming a member of the CHNA Steering Committee. The following are members of that Steering
Committee:
Tom Clancy, University of Minnesota School of Nursing
Diane Cross, Board Member, University of Minnesota Medical Center, Fairview
Connie Delaney, University of Minnesota School of Nursing, and Board Member,
University of Minnesota Medical Center, Fairview
Sandra Eliason, M.D., Fairview Clinics
Ann Ellison, Director, Fairview Community Health
Mohammed Hassan, M.D., University of Minnesota Physicians
Carrie Link, MD University of Minnesota Department of Family Medicine and
Community Health
Donna McAlpine, University of Minnesota School of Public Health
Gretchen Musicant, Commissioner, Minneapolis Department of Health and Family Support
Sahra Noor, Director, Department of Community Health, University of Minnesota
Medical Center, Fairview

2
Marge Page, Vice President, University of Minnesota Medical Center, Fairview
Hiba Sharif, Department of Community Health, University of Minnesota Medical Center,
Fairview
Carolyn Wilson, President, University of Minnesota Medical Center, Fairview
Major Needs and How Priorities Were Established Both qualitative and quantitative data was gathered in the assessment process. The qualitative data
included:
Focus groups of three populations (mothers, seniors, vulnerable)
Web surveys
Key stakeholder interviews with elected officials, community leaders, physicians and members of
community-based agencies.
Quantitative data included:
Mortality data
Hospital utilization data
Emergency room data
Community Need Index (CNI) scores which are based on underlying socio-economic indicators
of health. Causation has been shown between high CNI scores and inappropriate emergency
room admission for ambulatory sensitive conditions. See appendix B for a map of CNI scores for
the assessment area.
The assessment resulted in a number of themes. The themes identify specifically what University of
Minnesota Medical Center, Fairview community members need to maintain or improve their health
and/or specific medical conditions that require attention. The six top themes that emerged are:
Health information and education
Mental health
Diabetes
Low birth weight/infant mortality
Heart disease
Cultural competency
These six themes were discussed by the Steering Committee members and then prioritized using a Need
Prioritization Worksheet and Criteria, see appendix C. As a result of the discussion, the group reclassified
both “healthcare information and education” and “cultural competency” to be used as strategies
throughout all action planning rather than as individual action items. The prioritization, by the Steering
Committee, resulted in the following top health needs for the community:
1. Mental health
2. Heart disease
A review of current community benefit programs found that the medical center is meeting existing
community needs through provision of charity care, Medicaid services, health professional education
programs, as well as participation in the Health Commons, the Healthy Kids & Communities initiative
and numerous community education and health events. These activities were determined to be valuable
priorities for the medical center’s implementation strategy.
3
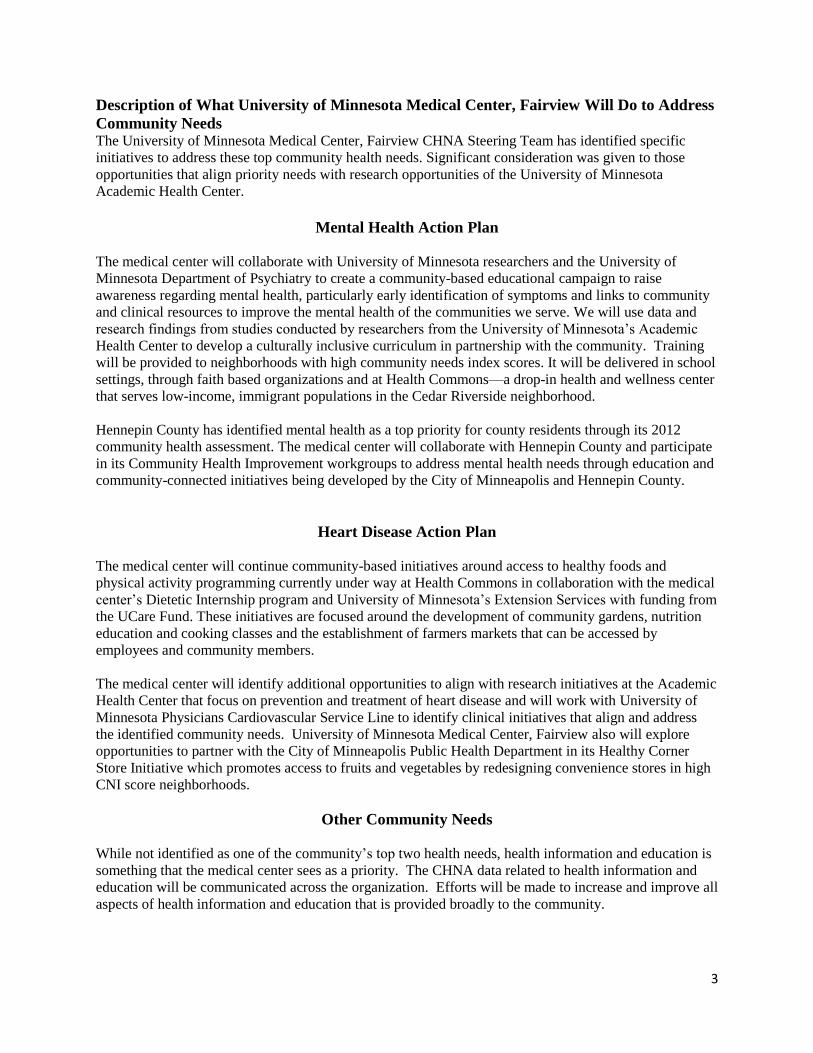
Description of What University of Minnesota Medical Center, Fairview Will Do to Address
Community Needs The University of Minnesota Medical Center, Fairview CHNA Steering Team has identified specific
initiatives to address these top community health needs. Significant consideration was given to those
opportunities that align priority needs with research opportunities of the University of Minnesota
Academic Health Center.
Mental Health Action Plan
The medical center will collaborate with University of Minnesota researchers and the University of
Minnesota Department of Psychiatry to create a community-based educational campaign to raise
awareness regarding mental health, particularly early identification of symptoms and links to community
and clinical resources to improve the mental health of the communities we serve. We will use data and
research findings from studies conducted by researchers from the University of Minnesota’s Academic
Health Center to develop a culturally inclusive curriculum in partnership with the community. Training
will be provided to neighborhoods with high community needs index scores. It will be delivered in school
settings, through faith based organizations and at Health Commons—a drop-in health and wellness center
that serves low-income, immigrant populations in the Cedar Riverside neighborhood.
Hennepin County has identified mental health as a top priority for county residents through its 2012
community health assessment. The medical center will collaborate with Hennepin County and participate
in its Community Health Improvement workgroups to address mental health needs through education and
community-connected initiatives being developed by the City of Minneapolis and Hennepin County.
Heart Disease Action Plan
The medical center will continue community-based initiatives around access to healthy foods and
physical activity programming currently under way at Health Commons in collaboration with the medical
center’s Dietetic Internship program and University of Minnesota’s Extension Services with funding from
the UCare Fund. These initiatives are focused around the development of community gardens, nutrition
education and cooking classes and the establishment of farmers markets that can be accessed by
employees and community members.
The medical center will identify additional opportunities to align with research initiatives at the Academic
Health Center that focus on prevention and treatment of heart disease and will work with University of
Minnesota Physicians Cardiovascular Service Line to identify clinical initiatives that align and address
the identified community needs. University of Minnesota Medical Center, Fairview also will explore
opportunities to partner with the City of Minneapolis Public Health Department in its Healthy Corner
Store Initiative which promotes access to fruits and vegetables by redesigning convenience stores in high
CNI score neighborhoods.
Other Community Needs
While not identified as one of the community’s top two health needs, health information and education is
something that the medical center sees as a priority. The CHNA data related to health information and
education will be communicated across the organization. Efforts will be made to increase and improve all
aspects of health information and education that is provided broadly to the community.

4
Next Steps for Priorities For each of the priority areas listed above, the medical center will work with the CHNA Steering
Committee and community partners to:
Identify any related activities being conducted by others in the community that could be built
upon.
Develop measurable goals and objectives to evaluate the effectiveness of the any interventions.
Build support within the community for the identified initiatives.
Develop detailed work plans.
Priority Needs Not Being Addressed and the Reasons
The needs of our community are many and diverse. To provide focus, the priority areas were
selected where the medical center, with its partners at University of Minnesota Physicians and
University of Minnesota, can have the greatest impact due to our particular strengths and
expertise.
Resources The work of the action plans will be supported by a 1.8 dedicated community health staff and $73,000 for
programming.
Approval Each year, University of Minnesota Medical Center, Fairview’s Board will review the prior fiscal year’s
Community Benefit Report and approve the Community Benefit Implementation Strategy for addressing
priorities identified in the most recent Community Assessment and other plans for community benefit.
This report was prepared for the Nov. 9, 2012 meeting of the Patient Care Committee of the Board and
was approved at that meeting.

Appendices
A. Primary Service Area Map
B. Community Need Index (CNI) Score Map
C. Need Prioritization Worksheet and Criteria
D. Definition of Community – Zip Codes by Hospital PSA
E. Qualitative Data Tools and Questions
F. Top Ten Health Conditions by Population and Hospital

Appendix A: Primary Service Area Map
University of Minnesota Medical Center, Fairview/
University of Minnesota Amplatz Children’s Hospital
Primary Service Area
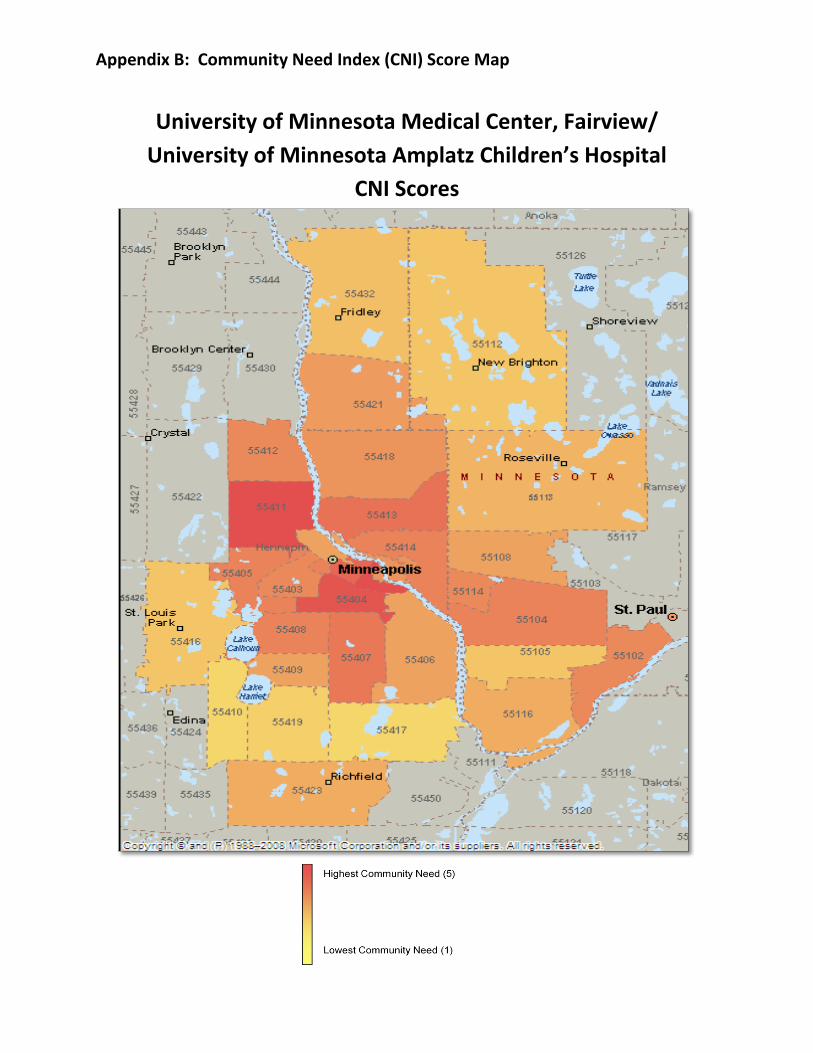
Appendix B: Community Need Index (CNI) Score Map
University of Minnesota Medical Center, Fairview/
University of Minnesota Amplatz Children’s Hospital
CNI Scores

Need Prioritization Worksheet
Criterion and Considerations Guide
Criteria #1: Is the need health related?
Considerations:
To what degree is the need health related?
Criteria #2: Is the need tied to Community Need Index (CNI) scores or similar measure of vulnerability?
Considerations:
To what degree is the need tied to CNI scores or other measure such as the percentage of school Free and
Reduced Lunch (FRL) participants (e.g. A community may have a low CNI score, but a school within that
community may have a high percentage of students who qualify for FRL).
The Community Need Index (CNI) Scores were developed by Catholic Healthcare West and Thompson Reuters.
Their underlying data is used to create an objective measure of socio-economic barriers to health care access
among populations and their effect on hospital admissions. CNI Scores range from a 5 (highest health
disparity/highest community need) to a 1 (lowest health disparity/lowest community need). CNI Scores provide a
high-level measure of community need and allow for comprehensive comparative analysis to be made on many
levels ranging from individual zip code comparison to regional or multi-state comparisons.
Criteria #3: Is the need tied to assessment or otherwise documented?
Considerations:
To what degree is the need tied to assessment (i.e. where did the need fall on your list of priorities)?
Are there contributing factors that may indicate the need for more immediate intervention (i.e. the need may fall
lower on the assessment, but there are additional considerations that make it a higher priority)?
Criteria #4: What is the magnitude of the need?
Considerations:
How many persons does the need affect, either actually or potentially?
Criteria #5: What is the seriousness of the consequences?
Considerations:
What degree of disability or premature death occurs?
What are the potential burdens to your community such as economic or social burdens?
What happens if we don’t respond?
Criteria #6: What is the feasibility of addressing?
Considerations:
Is it amenable to intervention? Is the problem preventable?
Are there scientifically feasible (evidence-based) interventions available?
Is intervention acceptable to the community (i.e. are there economic, social, cultural or political issues that may
influence the communities ability to address the health need)?
Does intervention have the potential to produce measurable outcomes?
Are there adequate technology, knowledge, human and financlal resources to effect change?
Criteria #7: Does the need tie to Fairview Strategy?
Considerations:
Fairview Strategy is defined as prevention, awareness and treatment of conditions related to cardiovascular,
orthopedics, oncology, mothers/children and behavioral health.

Appendix D: Definition of Community – Zip Codes by Hospital Primary Service Area, 2012 Fairview Lakes Medical Center Fairview Ridges Hospital University of Minnesota
Medical Center, Fairview/ Amplatz Children’s Hospital
Zip Code Community Zip Code Community Zip Code Community
55012 Center City 55020 Elko 55102 St. Paul Downtown
55013 Chisago City 55024 Farmington 55104 Midway
55014 Lino Lakes 55044 Lakeville 55105 MacGroveland
55025 Forest Lake 55054 New Market 55108 Falcon Heights
55032 Harris 55068 Rosemount 55112 New Brighton
55038 Hugo 55121 Eagan 55113 Roseville
55045 Lindstrom 55122 Eagan 55114 Como/Hwy 280
55056 North Branch 55123 Eagan 55116 Highland Park
55063 Pine City 55124 Apple Valley 55401 Mpls – North Loop
55067 Rock Creek 55306 Burnsville 55402 Mpls – Downtown
55069 Rush City 55337 Burnsville 55403 Mpls – Loring
55073 Scandia 55372 Prior Lake 55404 Mpls – Franklin
55074 Shafer 55378 Savage 55405 Mpls – Cedar
55079 Stacy Fairview Southdale Hospital 55406 Mpls – East Lake
55084 Taylors Falls Zip Code Community 55407 Mpls – Phillips
55092 Wyoming 55035 Hopkins 55408 Mpls – LynLake
Fairview Northland Med Ctr. 55317 Chanhassen 55409 Mpls – Harriet
Zip Code Community 55318 Chaska 55410 Mpls – Linden Hills
55017 Dalbo 55331 Excelsior 55411 Mpls – Near North
55309 Big Lake 55343 Hopkins 55412 Mpls – Camden
55330 Elk River 55344 Eden Prairie 55413 Mpls – Central NE
55371 Princeton 55345 Minnetonka 55414 Mpls – SE
55398 Zimmerman 55346 Eden Prairie 55415 Mpls – Downtown
56313 Bock 55347 Eden Prairie 55416 St. Louis Park
56329 Foley 55386 Victoria 55417 Mpls – Nokomis
56330 Foreston 55391 Wayzata 55418 Mpls – Northeast
56353 Milaca 55409 Mlps – Harriet 55419 Mpls – SW
56357 Oak Park 55410 Mlps – Linden Hills 55421 Columbia Heights
56358 Ogilvie 55416 St. Louis Park 55423 Richfield
56363 Pease 55417 Mpls – Nokomis 55432 Fridley
Fairview Range Regional Health Services
55419 Mpls – SW 55454 Cedar Riverside
Zip Code Community 55420 East Bloomington 55455 University
55703 Angora 55423 Richfield
55709 Bovey 55424 Edina
55710 Britt 55425 Bloomington
55719 Chisolm 55426 St. Louis Park
55723 Cook 55431 Bloomington
55738 Forbes 55435 Edina
55742 Goodland 55436 Edina
55746 Hibbing 55437 Bloomington
55751 Iron 55438 Bloomington
55765 Elmer 55439 Edina
55768 Mountain Iron
55769 Nashwauk
55775 Pengilly
55781 Side Lake

Appendix E: Qualitative Data Tools & Questions
Focus Group Notes—Fairview Health Services 2012 CHNA Fairview Health Services Community Health Needs Assessment Focus Group Summary Hospital: Name of Group: Date Held: Summary by: Questions:
1. What current health issues trouble you and your family?
2. What is the number one health issue for you or (your clients) your family?
3. What roadblocks do you experience when you are working to maintain your health?
4. Now tell us what roadblocks you experience when seeking healthcare from a professional?
5. To whom do you turn or where do you go when you need help with a health issue?
6. What is needed in our community to help you maintain or improve your health?
7. What is the role of the hospital to help you or others maintain or improve your health?
8. What do you see as your role in maintaining or improving your health?

Appendix E: Qualitative Data Tools & Questions
Stakeholder Interview Summary—Fairview Health Services 2012 CHNA
Fairview Community Health Needs Assessment 2012 Fairview Health Services Community Health Needs Assessment Stakeholder Interview Summary Hospital: Name of Individual: Date Held: Summary by: Background: 1. What do you believe to be the number one health issue in our community? 2. What are the difficulties, challenges and roadblocks faced by community members when they
seek healthcare from a professional? 3. When community members seek help about a health issue, where do you think they go for help? 4. What do you think is needed in your community to help individuals like yourself maintain or
improve your health? 5. What do you see as the health systems/hospitals role? 6. What do you see as your role in these improvements?
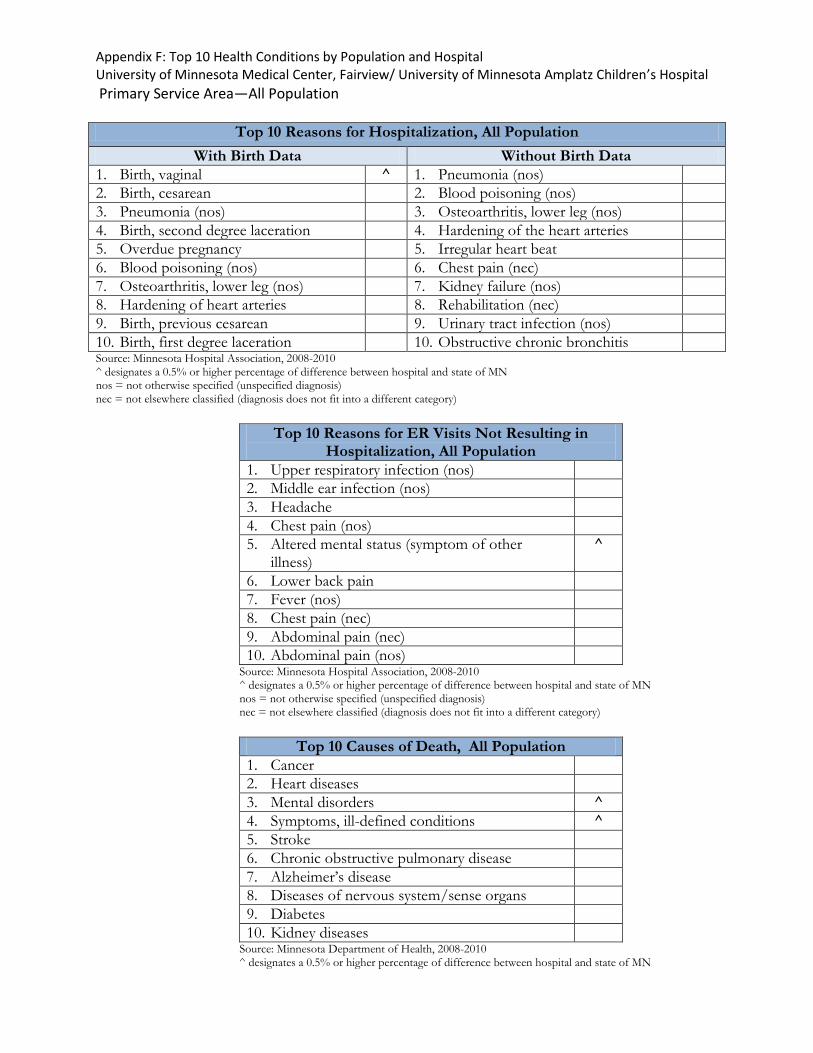
Appendix F: Top 10 Health Conditions by Population and Hospital University of Minnesota Medical Center, Fairview/ University of Minnesota Amplatz Children’s Hospital
Primary Service Area—All Population
Top 10 Reasons for Hospitalization, All Population
With Birth Data Without Birth Data
1. Birth, vaginal ^ 1. Pneumonia (nos)
2. Birth, cesarean 2. Blood poisoning (nos)
3. Pneumonia (nos) 3. Osteoarthritis, lower leg (nos)
4. Birth, second degree laceration 4. Hardening of the heart arteries
5. Overdue pregnancy 5. Irregular heart beat
6. Blood poisoning (nos) 6. Chest pain (nec)
7. Osteoarthritis, lower leg (nos) 7. Kidney failure (nos)
8. Hardening of heart arteries 8. Rehabilitation (nec)
9. Birth, previous cesarean 9. Urinary tract infection (nos)
10. Birth, first degree laceration 10. Obstructive chronic bronchitis Source: Minnesota Hospital Association, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN nos = not otherwise specified (unspecified diagnosis) nec = not elsewhere classified (diagnosis does not fit into a different category)
Top 10 Reasons for ER Visits Not Resulting in Hospitalization, All Population
1. Upper respiratory infection (nos)
2. Middle ear infection (nos)
3. Headache
4. Chest pain (nos)
5. Altered mental status (symptom of other illness)
^
6. Lower back pain
7. Fever (nos)
8. Chest pain (nec)
9. Abdominal pain (nec)
10. Abdominal pain (nos) Source: Minnesota Hospital Association, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN nos = not otherwise specified (unspecified diagnosis) nec = not elsewhere classified (diagnosis does not fit into a different category)
Top 10 Causes of Death, All Population
1. Cancer
2. Heart diseases
3. Mental disorders ^
4. Symptoms, ill-defined conditions ^
5. Stroke
6. Chronic obstructive pulmonary disease
7. Alzheimer’s disease
8. Diseases of nervous system/sense organs
9. Diabetes
10. Kidney diseases Source: Minnesota Department of Health, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN
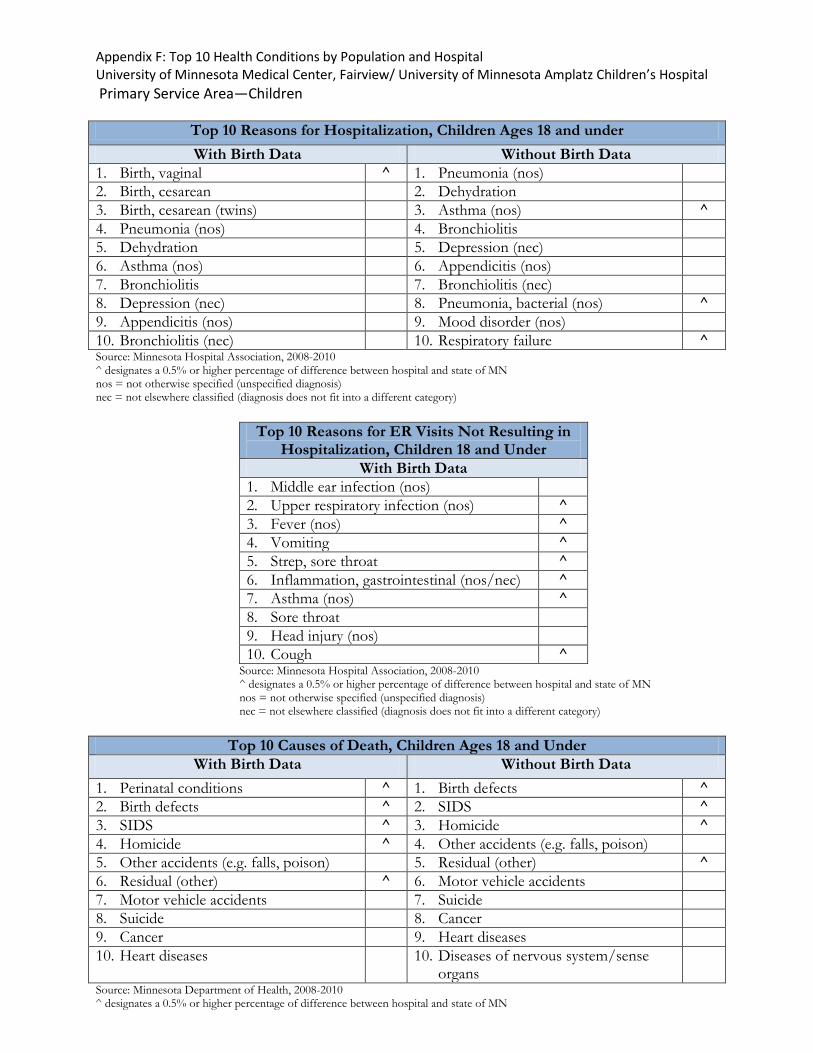
Appendix F: Top 10 Health Conditions by Population and Hospital University of Minnesota Medical Center, Fairview/ University of Minnesota Amplatz Children’s Hospital
Primary Service Area—Children
Top 10 Reasons for Hospitalization, Children Ages 18 and under
With Birth Data Without Birth Data
1. Birth, vaginal ^ 1. Pneumonia (nos)
2. Birth, cesarean 2. Dehydration
3. Birth, cesarean (twins) 3. Asthma (nos) ^
4. Pneumonia (nos) 4. Bronchiolitis
5. Dehydration 5. Depression (nec)
6. Asthma (nos) 6. Appendicitis (nos)
7. Bronchiolitis 7. Bronchiolitis (nec)
8. Depression (nec) 8. Pneumonia, bacterial (nos) ^
9. Appendicitis (nos) 9. Mood disorder (nos)
10. Bronchiolitis (nec) 10. Respiratory failure ^ Source: Minnesota Hospital Association, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN nos = not otherwise specified (unspecified diagnosis) nec = not elsewhere classified (diagnosis does not fit into a different category)
Top 10 Reasons for ER Visits Not Resulting in Hospitalization, Children 18 and Under
With Birth Data
1. Middle ear infection (nos)
2. Upper respiratory infection (nos) ^
3. Fever (nos) ^
4. Vomiting ^
5. Strep, sore throat ^
6. Inflammation, gastrointestinal (nos/nec) ^
7. Asthma (nos) ^
8. Sore throat
9. Head injury (nos)
10. Cough ^ Source: Minnesota Hospital Association, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN nos = not otherwise specified (unspecified diagnosis) nec = not elsewhere classified (diagnosis does not fit into a different category)
Top 10 Causes of Death, Children Ages 18 and Under
With Birth Data Without Birth Data
1. Perinatal conditions ^ 1. Birth defects ^
2. Birth defects ^ 2. SIDS ^
3. SIDS ^ 3. Homicide ^
4. Homicide ^ 4. Other accidents (e.g. falls, poison)
5. Other accidents (e.g. falls, poison) 5. Residual (other) ^
6. Residual (other) ^ 6. Motor vehicle accidents
7. Motor vehicle accidents 7. Suicide
8. Suicide 8. Cancer
9. Cancer 9. Heart diseases
10. Heart diseases 10. Diseases of nervous system/sense organs
Source: Minnesota Department of Health, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN

Appendix F: Top 10 Health Conditions by Population and Hospital University of Minnesota Medical Center, Fairview/ University of Minnesota Amplatz Children’s Hospital
Primary Service Area—Seniors
Top 10 Reasons for Hospitalization, Ages 65 and Over
1. Pneumonia (nos)
2. Blood poisoning (nos)
3. Irregular heart beat
4. Osteoarthritis, lower leg (nos)
5. Urinary tract infection (nos)
6. Kidney failure (nos) ^
7. Hardening of the heart arteries
8. Obstructive chronic bronchitis
9. Stroke (nos)
10. First heart attack Source: Minnesota Hospital Association, 2008-2010
^ designates a 0.5% or higher percentage of difference between hospital and state of MN nos = not otherwise specified (unspecified diagnosis) nec = not elsewhere classified (diagnosis does not fit into a different category)
Top 10 Reasons for ER Visits Not Resulting in Hospitalization, Ages 65 and Over
1. Chest pain (nos)
2. Chest pain (nec) ^
3. Dizziness and giddiness
4. Fainting
5. Urinary tract infection (nos)
6. General discomfort, fatigue (nec)
7. Nose bleed
8. Limb pain ^
9. Head injury (nos) ^
10. Headache ^ Source: Minnesota Hospital Association, 2008-2010 ^ designates a 0.5% or higher percentage of difference between hospital and state of MN nos = not otherwise specified (unspecified diagnosis) nec = not elsewhere classified (diagnosis does not fit into a different category)
Top 10 Causes of Death, Ages 65 and Over
1. Cancer
2. Heart diseases
3. Mental disorders ^
4. Symptoms, ill-defined conditions ^
5. Stroke
6. Chronic obstructive pulmonary disease
7. Alzheimer’s disease
8. Diseases of the nervous system/sense organs
9. Kidney diseases
10. Accidental falls Source: Minnesota Department of Health, 2008-2010
^ designates a 0.5% or higher percentage of difference between hospital and state of MN
![Neurobiology of Pain2010ASPMN.pptx [Read-Only] · 9/7/2010 1 Neurobiology of Pain Miles Belgrade, MD Fairview Pain Management Center University of Minnesota Medical center We’ve](https://img.pdfslide.us/doc/110x75/5ac65e007f8b9aa0518e85e6/neurobiology-of-read-only-1-neurobiology-of-pain-miles-belgrade-md-fairview-pain.jpg)