Embed Size (px)
Citation preview
UNIVERSITY OF KHARTOUM
The Graduate College
Medical& Health Studies Board
CLINICOPATHOLOGICAL STUDY OF COLORECTAL CANCERS IN SUDANESE PATIENTS
By Dr. Asma Mukhtar Shammet Ahmed
M.B.B.S. Faculty of Medicine (U of K) 1996
A thesis submitted in partial fulfillment for the requirements
of the degree of clinical MD in Pathology of the University of Khartoum
August 2005
Supervisor
Dr.Mohammed Mohammed Osman, M.B.B.S, MD. Pathology
Assistant Professor of Pathology Department of pathology
Faculty of Medicine University of Khartoum
Π
:قال اهللا تعالى
) رب العالمينقل إن صالتى و نسكي ومحياي و مماتي هللا ( صدق اهللا العظيم
)162( اآلية -سورة األنعام
CONTENTS
Dedication………………………………………………………………..I
Acknowledgment……………………………………………………….II
Abbreviations…………………………………………………………..III
English abstract………………………………………..………………IV
Arabic abstract……………………………………..………………….VI List of tables………………………………………………………….VIII
List of figures………………………………………………………… IX
CHAPTER ONE INTRODUCTION AND LITRATURE REVIEW………………...……1
1.1. Definition…………………………………….…………………….2
1.2. Normal anatomy…………………………………………….……2
1.3. Epidemiology……………………………………………….…….4
1.4. Aetiology and pathogenesis…………………………….………5
1.5. Genetics……………………………………………..…………….8
1.6. Localization………………………………………….…………....9
1.7. Metastasis and mode of spread……………………….………10
1.8. Diagnosis………………………………………………….……..10
1.9. Pathologic diagnosis………………………….………………..15
1.10. Treatment………………………………...……………….……25
1.11. Prognosis…………………………………………...………….27
1.12. Recurrence…………………………………...……………….28
OBJECTIVES……………………………………………………..….29
CHAPTER TWO METHODOLOGY……………………………………………………..30
CHAPTER THREE RESULTS…………………………………………………...…………32
CHAPTER FOUR DISCUSSION…………………………………………..……………..54
CONCLUSION……………………………………...…………………59
RECOMMENDATION……………………………..…………………60
REFERENCES……………………………………...…………….…..61
APPENDIX (questionnaire)
I
DEDICATION
To the soul of my brother,
To my parents & sisters with great love.
II
ACKN0WLEDGEMENT
I would like to express my deep thank to my supervisor Dr.
Mohammed Mohammed Osman for his continuous guidance,
generous advice, encouragement& co-operation throughout this
work.
I am also grateful to my parents & sisters who were always
there whenever I needed them.
Many thanks & best wishes to Dr. Mahdi Moh. Ahmed
Shammad, consultant dermatologist for his valuable advices
throughout the preparation this study.
I wish to thank Dr. Moh. Abd Elhameed, the director of the
laboratories in Ibn Sina Hospital, for making the records at the
histopathology lab available for this analysis.
Thanks also to the technicians at the histopathology lab& to
the staff at the statistic unit in Ibn Sina Hospital for their help to get
the patients’ records& histopathology slides.
I would like to thank Ms. Widad Abd El Magsoud who helped
me to print out this work.
Lastly my thanks to every one who helped me to do this
study.
III
List of Abbreviations
ACS : American Cancer Society.
AGCC : American Joint Committee on Cancer.
APC-gene : Adenomatous Polyposis Coli-gene.
CAP : College of American Pathologists.
CEA : Carcinoembryonic Antigen.
CRC : Colorectal Cancer.
CT : Computed Tomography.
DCBE : Double Contrast Barium Enema.
DCC-gene : Deleted in Colon Cancer-gene.
DNA : Deoxyribonucleic Acid.
FAP : Familial Adenomatous Polyposis.
FOBT : Faecal Occult Blood Test.
5-FU : 5-Fluorouracil.
GCC-B1TM : Guanylyl Cyclase C-B1TM protein.
MSI-H. gene: Microsatellite Instability gene with High frequency.
TEM : Transanal Endoscopic Microsurgery.
TNM system: Tumor Node Metastasis system.
UICC : Union Internationale Center Le Cancer.
WHO : World Health Organization.
IV
ABSTRACT
Colorectal cancer is an important tumor of the GIT arising
from the epithelial lining the inner surface of the colon& rectum&
from the crypts of Liberkϋhn.
This is a retrospective study conducted on Sudanese patients
during the period from January 2001 to December 2004 at Ibn
Sina Hospital, Khartoum, Sudan.
The study aimed to determine the histopathological pattern of
CRC, & to show the correlation between the histopathological type
of the tumor& the age, sex, residency distribution, & clinical
presentation. comprised 100 patients, of which 56 were males&
44 were females with a ratio of 1.1: 1 to each other. The age for all
patients ranges between 14- 85 years.
In this study there was a high proportion of early onset tumor
(33% of cases were < 40 years), & left sided subsite distribution of
CRC (77% of cases were in the rectum, sigmoid colon, & recto-
sigmoid junction).
Rectal bleeding represented the majority (76%) of the
symptoms of CRC. The duration of symptoms varied from one to
twelve months with the majority of patients (61.2%) having
symptoms < 6 months.
V
By reviewing the slides, only five histological types were
identified. There were 74(74%) adenocarcinoma, 13(13%)
mucinous adenocarcinoma, 7(7%) signet ring cell carcinoma,
5(5%) papillary carcinoma, & one (1%) anaplastic carcinoma.
In conclusion, we share many epidemiological features of
developing countries for CRC. These include left subsite
distribution& early-onset CRC. We stress the significance of the
public health education& national screening program regarding
CRC to improve the outcome.
VI
حةملخص االطرو
يعتبرسرطان القولون و المستقيم من اهم االورام التي تصيب الجهاز الهضمي
وهو ينمو من الخاليا المبطنة للغشاء الداخلي للقولون و المستقيم و من جريبات . لالنسان
.ليبرخون
ضي دراسة الي الوراء عن سرطان القولون و المستقيم في المر هده الدراسة
في مستشفي ابن سيناء 2004 وحتي ديسمبر2001 سودانيين في الفترة من ينايرال
هده الدراسة هو بحث التغييرات المرضية في االنسجة في سرطان و الغرض من.بالخرطوم
القولون و المستقيم و ايضا بحث عالقة كل من العمر، الجنس و المسكن مع نوع سرطان
.القولون و المستقيم
و نسبة . من النساء44 من الرجال و 56 مريض منهم 100الدراسة تضمنت
، و متوسط اعمار المرضي يتراوح ما 1.1: 1 نسبة المرض في الرجال مقارنة بالنساء هي
. سنة85 سنة الي 14بين
من % 33( و لقد وجدنا في هده الدراسة بان هدا المرض يحدث مبكرا بين السودانيين
في كل % 77(وثه في الجانب االيسر من القولونو يتركز حد) تحت سن االربعينالمرضي
و قد كان نزف ). من المستقيم، القولون السيني، و منطقة التحام المستقيم مع القولون السيني
تراوحت %). 76(ي مرضي سرطان القولون و المستقيم من االعراض الغالبة علالمستقيم
ية المرضي كانت فترة اعراضهم ي اثني عشر شهرا، بينما غالبفترة االعراض ما بين شهر ال
.عن الستة اشهرتقل
VII
من هدا السرطان، و قد كان بالرجوع الي الشرائح تم التعرف علي خمسة انواع
مرضي بالسرطان الغددي 13، %)74(ا لديه سرطان غددي مريض74 تقسيمها كاالتي
مرضي لديهم السرطان الحليمي 5، %)7( مرضي بالسرطان الخاتمي 7، %)13 (المخاطي
%).1(، و مريض واحد بالسرطان المتحول او االرتدادي%)5(
الخصائص و لقد خلصت هده الدراسة الي ان السودان يشارك الدول النامية في بعض
و تركزه البيئية لسرطان القولون و المستقيم و التي تتمثل في الحدوث المبكر لهدا المرض،
و ايضا تطرقت . في الجانب االيسر من القولون مما يتطلب المزيد من البحث لمعرفة االسباب
الدراسة الي اهمية التثقيف الصحي و برنامج الفحص الطبي الدوري لسرطان القولون و
.ستقيم من اجل الوصول الي نتائج افضلالم
VIII
LIST OF TABLES
Table Page
(1) Sex distribution& male to female incidence rate ratios for
cancer of the colon& rectum among the studied
group……..............................................................................
37
(2) Presenting symptoms of colorectal cancer among the studied
group …………………………………………………………….
38
(3)Grading of colorectal cancer among the studied group……… 39
IX
LIST OF FIGURES
Figure Page
(1) Age distribution of colorectal cancer among the studied
group…………………………………………………………
40
(3) Sex Distribution in colorectal cancer among the studied
group ………………………………….……………………..
41
(3) Age specific incidence rate of colorectal cancer in males
& females among the studied group…………………..
42
(4) Residence distribution of colorectal cancer among the
studied group………………………………………………..
43
(5) Subsite distribution of colorectal cancer among the
studied group……………………………………………...
44
(6) Histological patterns (Diagnosis) of colorectal cancer
among the studied group………………………………….
45
(7) Relationship between the diagnosis& different age
groups among the studied group……………………….
46
(8) Relationship between the diagnosis & sex among the
studied group………………….……………………………
47
(9)-(14) Colored slides of some types of colorectal cancer… 48-53

X
1
INTRODUCTION & LITERATURE REVIEW
Colorectal cancer (CRC) is a major health problem
throughout the world, with the highest incidence rates in North
America, Western Europe, Australia and Newsland.(1)It is the fourth
most common internal malignancy and is second to carcinoma of
the lung as a cause of cancer death.(2)
Virtually 90%-98% of all cancers in the large bowel are
adenocarcinoma.(1,3,4,5)The remainder are neoplasms of the
neuroendocrine cells, mainly carcinoid tumors; direct invasion of
the colon and rectum by other visceral malignancies, such as
carcinoma of the prostate, urinary bladder and uterus; metastatic
tumors, such as malignant melanoma;(4)lymphomas and
mesenchymal tumors.(6)
Colorectal cancer usually occurs over the age of 50 years.(4)
In Sudan it was reported to affect younger age group and about
30% of the lesions were of the mucoid & undifferentiated types.(7)
The main precursor lesion for CRC is adenoma, which is
readily detected& treated by endoscopic techniques. While most of
adenomas are polypoid, flat and depressed lesions may be more
prevalent than previously recognized.(8) Non neoplastic polyps
(hyperplastic, juvenile, hamartomatous, and lymphoid polyps) are
2
not considered precancerous unless they occur in polyposis
syndromes (juvenile polyposis and hyperplastic polyposis).(6,9,10,11)
1.1.Definition:
Colorectal cancer (CRC) is a disease in which cells in the
colon or rectum become abnormal & divide without normal control
or order, forming a mass called tumor.(12)It arises from the
epithelium lining the inner surface of the colon &rectum and from
the crypts of Leiberkühn.(13)
1.2.Normal Anatomy:
Normally the large bowel comprises the terminal 1-1.5m of
the gastrointestinal tract and is subdivided into: cecum, ascending
(right) colon, transverse colon, descending (left) colon, sigmoid
colon, and rectum. The hepatic flexure is at the junction of the
ascending and the transverse colon, and the splenic flexure is at
the junction of the transverse and descending colon. The rectum
forms the distal 8-15cm of extraperitoneal large bowel.
Histologically, the large bowel wall is composed of 4 layers which
are (from lumen outwards):(14) mucosa, submucosa, muscularis
externa, and serosa (or, in the rectum, perimuscular tissue).The
mucosa has 3 components: epithelium, lamina propria, and
muscularis mucosa. The mucosal surface is covered by a single
3
layer of low columnar to cuboidal epithelium which is composed of
absorptive cells (with basally located nuclei, mucin negative
acidophilic cytoplasm, and apical striations) and goblet cells
(contain mucin granules). Crypts of Leiberkühn open into the
mucosal surface. They have tubular shape and arranged in parallel
to each other, and their epithelium contains mature absorptive
cells, undifferentiated precursor cells, goblet cells, endocrine cells,
and paneth cells. Both the precursor and the endocrine cells
predominate at the base of crypts. The paneth cells are identified
by their numerous eosinophilic secretory granules, and they are
only present in the cecum and right colon.(14)
The lamina propria consists of connective tissue cells &
fibers. It contains blood vessels, lymphatics, nerves &lymphoid
follicles which extend from the mucosa through the muscularis
mucosa into the submucosa.(14)
The submucosa composed of loose connective tissue contains
cells similar to those in the lamina propria, and also contains the
Meissner’s plexus.(14)
The muscularis externa includes a circular inner layer and a
longitudinal outer layer of muscles, with the myenteric plexus of
Auerbach between them.(14)
4
The serosa is composed of a single layer of flattened to
cuboidal mesothelial cells and the subjacent fibroblastic tissue.
The large bowel is supplied by branches of the superior mesenteric
artery (from the cecum to the splenic flexure) and the inferior
mesenteric artery (distal to the splenic flexure). The lower portion
of the rectum is irrigated by the middle and inferior rectal arteries,
which are branches of the internal iliac artery (14).
The lymphatic drainage of the colon is mainly through the
mesentery into the paracolic lymph group, then to intermediate
nodal group, to central group, and finely to the paraortic chain. The
lymphatic drainage of rectum is toward the inferior mesenteric
artery nodes, the superior haemorroidal chain, the hypogastric and
the common iliac nodes.(14)
1.3. Epidemiology:
Colorectal cancer is an important health problem. There are
one million new cases diagnosed worldwide each year and
approximately half a million death (15), making this cancer the fourth
most common incident cancer and cause of death throughout the
world. The developed countries account for >63% of the total
global incidence. High-risk areas include North America, Europe
and Australia. Central and South America, Africa and Asia are
5
areas with low risk factors.(16)CRC is slightly more common in
males. Sporadic cases of CRC occur over the age of 50 years(4),
with peak incidence at 60-70 years & fewer than 20% occur before
the age of 50 years. When CRC is found in a young person, pre-
existing ulcerative colitis or one of the polyposis syndromes must
be suspected.(3)
1.4. Etiology & Pathogenesis:
CRC either occur on a preexisting adenoma or on a normal
mucosa without evidence of adenomatous precursors.(3) The exact
cause of CRC is unknown, but there are many risk factors which
include:
1- Age and sex: CRC is more common in males above the age of
50 years.(4,17)
2- Inflammatory bowel diseases: as chronic ulcerative colitis (U.C)
is associated with increased risk of CRC. The lesion that occurs
in U.C. tend to be flat and invasive, and is difficult to be detected
endoscopically at an early stage.(4)So patients with U.C. are
commonly screened every one to two years by colonoscopy &
biopsy to look for dysplasia.(18)
3- Family history of CRC or adenomatous polyps: In general, closer
familial relationship to affected relatives, younger age of affected
6
relatives, and larger number of affected relatives all increase the
risk of CRC.(18)About 5%-10% of patients with CRC have an
inherited genetic abnormality that causes the cancer. These
abnormalities are Familial Adenomatous Polyposis (FAP) &
Hereditary Non Polyposis Colorectal Cancer (HNPCC), and they
should be excluded by careful family history.(19)
• Familial Adenomatous Polyposis (FAP): An autosomal
dominant syndrome that result from defect in the
adenomatous polyposis coli (APC) gene.(20)It is characterized
by presence of hundreds of polyps which occur at young age
and develop into CRC by the age of 40 years if preventive
surgery is not done.(21,22)About 1% of all CRC are due to this
syndrome.(19)
• Hereditary Nonpolyposis Colorectal Cancer (HNPCC): Is an
autosomal dominant syndrome that is a result of germline
mutations in mismatch repair genes (genes that code for
proteins responsible for correcting errors during DNA
replication). It is characterized also by presence of few polyps,
but not hundreds, at young age & then developed into
malignancy between the ages of 40 & 50 years.(23)
4- Dietary factors: Research is going on the role of dietary factors
such as red meat especially overcooked or processed, high fat
7
intake, low fiber diet, high refined carbohydrates, decreased
intake of protective micronutrients, obesity, alcohol
consumption, & deficiency of calcium & folate. All these factors
increase the incidence of CRC risk.(16,24,25,26,27,28,29,30,31,32) It is
theorized that reduced fiber content lead to decreased stool
bulk, increased fecal transit time in the bowel, and altered
bacteria flora of the intestine. Potentially toxic byproducts of
carbohydrate degradation are therefore present in higher in the
small stools and are held in contact with the colonic mucosa for
longer period of time. Moreover high cholesterol intake in the
red meat enhances the synthesis of bile acids by the liver,
which, in turn, may be converted into potential carcinogens by
intestinal bacteria. Refined diet also contains less vitamin A, C,
and E, which may act as oxygen scavengers.(3)
5- Other risk factors:
- It has been reported that the use of aspirin,
postmenopausal female hormone therapy, and oral
contraceptive pills are associated with low risk for
CRC.(33,34,35,36,37,38)
- Low physical activity & cigarette smoking are associated
with high tendency to develop CRC.(39,40,41,42,43,44)
8
- Infection with Helicobacter pylori, cytomegalovirus, or
human polyoma virus JCV was reported to be associated
with CRC.(45-47)
- Hyperinsulinaemia is associated with increased risk of
endometrial, colorectal, & breast carcinoma. The insulin
acts as growth factor for tumor formation.(48)
However 75% of all CRC occur in people with no known
predisposing factors for the disease. This makes early detection
and management with different screening modalities is an
important mean for significant reduction in CRC incidence and
mortality.(17)
1.5. Genetics of CRC:
Most CRC occurs sporadically in absence of well-defined
familial syndromes (3), while the remainder of CRC occur in patient
with inherited germline defects.(4) Regardless of the inciting event,
there are two pathogenically distinct pathways for the development
of CRC(49), both of which involve stepwise accumulation of multiple
mutations. However the genes involved and mechanisms by which
the mutations accumulate are different.(3)These pathways are:
(1) Adenoma-carcinoma sequence: characterized by chromosomal
instability that result in accumulation of mutations in a series of
9
oncogenes and tumor suppresser genes. These genes include:
APC gene, K-RAS gene, SMAD2&SMAD4 genes, and
P53gene.(3)
(2) Microsatellite Instability Pathway: characterized by genetic
lesions in DNA mismatch repair genes. It is involved in 10%-
15% of sporadic cases & in the HNPCC syndrome.(3)
1.6. Localization:
Most CRC are located in the sigmoid colon and rectum, but
there is evidence in changing distribution in the recent years, with
increased proportion of more proximal carcinoma.(50) Molecular
pathology has also shown site differences: tumors with high levels
of microsatellite instability (MSI-H) or RAS proto-oncogene
mutations are more frequently located in the cecum, ascending
colon & transverse colon.(51,52,53)
1.7. Metastasis & Mode of spread:
Colorectal cancer arises in the mucosa and tends to
spread to other organs through one of the following routes:(54)
(1) Direct extension of the tumor through all layers of the colon
wall to the adjacent structures or organs.
10
(2) Haematogenous: through the blood to the liver
(commonly), lungs, brain, adrenals, kidney, bone and others.
This route is associated with poor prognosis.
(3) Lymphatic: through the submucosal blood vessels to the
regional lymph nodes.
(4) Transcelomic: through the peritoneal cavity (54).
1.8. Diagnosis:
Clinical picture:
The presentation of large bowel malignancy generally falls
into three categories: insidious onset of chronic symptoms, acute
onset of intestinal obstruction, or acute perforation. The most
common is that of the insidious onset of chronic symptoms(2),
which are:
Rectal bleeding, chronic anaemia, change in bowel habits,
abdominal or rectal pain.(54) Less common symptoms include
weight loss, palpable mass, malaise, fever, symptoms of urinary
tract involvement, mucus discharge, obstruction or perforation of
the colon, acute appendicitis (from obstruction of the appendiceal
lumen by a cecal tumor) or signs of distant metastasis to the liver,
lungs or brain.(2,54)Rectal bleeding is visible in lesions of the
sigmoid colon and rectum, and will be the cause of anaemia
11
.Alteration in bowel habits(constipation &diarrhoea)are more
common with left colon or more distal tumors, because of narrow
lumen and more solid stool that traverse the segment containing
the tumor. Abdominal pain is crampy or constant.(54) Left-sided
obstructing lesions may present with cramping abdominal pain
associated with nausea & vomiting.(2) Presence of peritonitis
indicates colonic perforation. Palpable mass, signs of distant
metastasis and weight loss are associated with poor prognosis.(54)
Screening:
Screening means checking for health problem before they
cause symptoms.(12) Because early detection greatly influence
survival in CRC, mass population screening has been
recommended in many high-risk populations. High-risk patients
include patients over 40 years of age, patients with Familial
Adenomatous Polyposis (FAP) and Hereditary Non Polyposis
Colon Cancer (HNPCC), and patients with chronic ulcerative colitis
(U.C).(4)Currently, it is estimated that screening of average risk
people over the age of 50 would reduce the mortality of CRC by
50%.(55)
Screening for sporadic CRC is unsatisfactory. Several
different screening methods have been advocated (4):
12
a) Faecal Occult Blood Testing(FOBT) annually: Fecal Occult
Blood Test is nonspecific test that fail to detect many small
cancers and precancerous lesions.(56)But a positive annual or
biannual FOBT that is followed by complete diagnostic
evaluation of the colon will reduce the number of deaths caused
by CRC.(57),(58)
b) Flexible sigmoidoscopy every five years: Is an examination of
the rectum &lower colon using sigmoidoscope.(12)The
effectiveness of this method as a screening tool depends on its
ability to detect cancers & adenomatous polyps in average risk
asymptomatic patients with negative FOBT.(59) If sigmoidoscopy
detects polyps, it should be followed by colonoscopy.(60) FOBT
annually accompanied by sigmoidoscopy every five years is
recommended by American Cancer Society (ACS)&other
experts.(61)
c) Double Contrast Barium Enema(DCBE)every five to 10 years:
Is series of X-Rays of the entire colon & rectum.(12) The efficacy
of barium enema in preventing CRC has not been
evaluated.(59)Single-column barium enema is less sensitive than
DCBE, so if it is used as a screening tool, it should be combined
with flexible sigmoidoscopy.(18)If lesions are detected by barium
enema the patient require colonoscopy.(59)
13
d) Colonoscopy every 10 years: Colonoscopy is examination of
rectum & entire colon using colonoscope.(12) It allows detection
& removal of premalignant & malignant lesions through out the
entire colon & rectum(12,59), and so reduces deaths from CRC.(62)
e) Genetic testing: Is recommended only for: (1) Those with
familial polyposis syndrome & HNPCC to see whether they
have the inherited genetic defect. (2) Patients with sporadic
CRC who satisfy the Amsterdam Criteria for HNPCC,(4) which
are: a) At least 3 family members with CRC, at least 2 being
first degree relatives. b) At least 2 generations with CRC. c) At
least one CRC patient younger than 50 years old at diagnosis.
Over 70% of families that meet these criteria have genetic
mutations associated with HNPCC.(63)
There are new tests under study for CRC screening:
(1) Virtual Colonoscopy (Computed Tomographic Colonoscopy).
(2) Genetic testing of stool sample.(12)
Diagnostic Studies:
Colonoscopy with biopsies is best; proctosigmoidoscopy
gives limited data due to shorter length of scope, and DCBE is
useful but requires colonoscopy if lesions are seen.(1)Brush
cytology has been described as useful in diagnosis of rectal
14
cancer, but now is not recommended because of high cost & rare
false positive diagnosis.(4)
Lab Studies:
Complete blood count with differential, showing anaemia in
right-sided tumors due to chronic blood loss; chemistry panel
including liver and renal functions.(1)
Preoperative Studies:
Chest X-Ray (CXR); serum Carcinoembryonic Antigen
(CEA) level; metastatic search if suspected; abdominal CT &
radionuclide scanning are costy, so have no role in majority of
patients.(1)
1.9. Pathologic diagnosis:
The diagnosis of CRC is established by histologic
examination of a biopsy specimen which obtained endoscopically
or, rarely, intraoperatively when the endoscopy is impossible
because of tight strictures.(4)
Gross:
CRC may be exophytic/fungating with predominantly
intraluminal growth, endophytic/ulcerative with predominantly
intramural growth, diffusely infilterative/linitis plastica with subtle
endophytic growth, and annular with circumferential involvement of
15
the colorectal wall & constriction of the lumen.(6) Right-sided colon
cancers tend to be polypoid, exophytic masses that project from
the wall into the lumen. Left-sided colon cancers tend to be annular
with mucosal ulceration & thickening of the wall causing luminal
narrowing. Rectal cancers are exophytic or ulcerative.(4) But
overlap among these types is common.(6)
The incidence trends of CRC differ for each subsite (64) as
follows: the cecum & ascending colon, 22%; transverse colon,11%;
descending colon, 6%; rectosigmoid, 55%; &other sites, 6%.(3) In
other words about 50% of CRC occurs in the rectosigmoid
area.(14)
In cross section, grayish white tissue is seen replacing the
bowel wall. Highly mucinous tumors have a gelatinous, glaring
appearance, with mucus separating the layers of the bowel wall.(14)
Histological types:
The internationally accepted histologic classification of CRC
proposed by the World Health Organization (WHO) is
recommended by the College of American Pathologists (CAP) and
is usually used in pathology reports.(65,66) Medullary carcinoma,
which previously classified as an undifferentiated carcinoma, has
been added to the revised WHO classification.(67)
16
* World Health Organization classification of colorectal
carcinoma:(6)
- Adenocarcinoma insitu/severe displasia.
- Adenocarcinoma.
- Mucinous (colloid) adenocarcinoma.
- Signet-ring cell carcinoma.
- Squamous cell (epidermoid) carcinoma.
- Adenosquamous carcinoma.
- Small cell (oat-cell) carcinoma.
- Medullary carcinoma.
- Undifferentiated carcinoma.
- Others (e.g. papillary carcinoma).
Adenocarcinoma:
About 85% of CRC are well and moderately differentiated
Adenocarcinoma. These are composed of irregularly infiltrating
malignant glands. The cells are columnar & have elongated “cigar-
shaped” nuclei. The invasive tumor is surrounded by a
desmoplastic response. There is focal necrosis & variable mitotic
activity.(4)
17
Mucinous adenocarcinoma:
Comprises 10% of CRC and include signet-ring cancers.
The mucinous adenocarcinoma is characterized by extracellular
mucin with the tumor cells floating in it.(68)The definition of
mucinous carcinoma is variable: some say that 50% of the lesion
must be mucinous(66), where as others say that 75% of the lesion
must be mucinous.(69,70)
Signet-ring cell carcinoma:
Defined by the presence of >50% of tumor cells with
prominent intracytoplasmic mucin.(71) It can occurs in the mucin
pools of mucinous adenocarcinoma.(6) Signet-ring carcinoma has a
poor prognosis.
Squamous/Adenosquamous cancers:
Are very rare & are associated with U.C, schistosomiasis,
and pelvic irradiation.(14)To classify a lesion as adenosquamous
carcinoma, occasional foci of squamous differentiation must be
present.(6) Certain criteria must be present to diagnose primary
CRC as squamous or adenosquamous: (1) No other sites of
squamous carcinoma in the body. (2) No involvement of
colacogenic or squamous-lined mucosa.(72)
18
Small cell carcinoma:
Rare and is about <1% of CRC. It is a malignant
neuroendocrine tumor that is similar histologically & biologically to
small cell (oat cell) carcinoma of the lung. As signet-ring
carcinoma, the small cell carcinoma has unfavorable
prognosis.(67,68)
Medullary carcinoma:
Uncommon & about 1% of CRC.(68) It is non-gland forming
carcinoma that previously had been classified as undifferentiated
carcinoma by the WHO system, but now known to be associated
with microsatellite instability and/or HNPCC syndrome.(67)
Histologically medullary carcinoma has pushing borders & is
composed of uniform, rounded cells which have small to medium-
sized nuclei & prominent nucleoli. It exhibits numerous mitosis &
brisk lymphocytic infiltrate.(68,73) Medullary carcinoma has a good
prognosis.(74)
Undifferentiated carcinomas:
These are tumors lack morphological evidence of
differentiation beyond that of epithelial tumor and have variable
histological features.(75)
19
Unusual forms of CRC:
Are very rare &for example:
Papillary carcinoma: the carcinoma forms papillations with
fibrovascular cores & epithelial tufts.(67)
Spindle cell (sarcomatoid or metaplastic) carcinoma.(76)
Clear cell adenocarcinoma: resemble renal cell adenocarcinoma,
but differentiated from it by presence of high level of
Carcinoembryonic Antigen (CEA) in the former.(14),(77)
Basaloid (colacogenic) carcinoma: similar to it is anal
counterpart,& has been reported on a few occasions in the
colorectum.(14)
Carcinoid tumor: of the large bowel is more common in the
rectum.(14) It is composed of small & uniform cells with rounded
nuclei with granular chromatin. The cells arranged in nests or
trabecular pattern.(4)
Adenocarcinoma-carcinoid tumor: are very rare in the colorectum.
Composed of approximately equal amounts of adenocarcinoma &
well differentiated carcinoid tumor.(4)
Choriocarcinomatous differentiation: rare cases of
adenocarcinoma with areas of choriocarcinoma have been
reported.(68)
20
Lymphomas: are less frequent than in the small intestine &
stomach.(14)
Staging:
Pathologic staging is an expression of the degree of invasion
& metastatic spread of the tumor.(4) It is based on the size of the
primary lesion, its extent of spread to regional lymph nodes, and
the presence or absence of distant metastasis.(3)
Three different systems for staging CRC have been developed
over years(4):
(1) Duke’s System(78)*: is the simplest & is widely used in
Europe.(4)
• Duke’s Classification of carcinoma of the colon & rectum:
Stage A: cancer restricted to colorectal wall.
Stage B: the cancer invades outside the muscularis externa.
Stage C: cancer with positive nodes.
Stage D: distant metastasis.
(2) Astler-Coller System (79)**: Modified Duke’s System. It is used in
the United States in addition to the Duke’s System. It provides
better distinction between minimally invasive tumors in term of
their nodal status.(4)
21
** Astler-Coller Classification of carcinoma of the colon and
rectum:
Stage A: lesion limited to the mucosa.
Stage B1: lesion involves muscularis propria, but does not
penetrate through it; uninvolved nodes.
Stage B2: lesion penetrates through the muscularis propria,
uninvolved nodes.
Stage C1: extending into the muscularis propria, but not
penetrating through it; involved nodes.
Stage C2: penetrating through the muscularis propria;
Involved nodes.
Stage D: distant metastatic spread
(3)TNM (Tumor, Node, Metastasis) System(80)***: This system
had been advocated by American Joint Committee on Cancer
(AJCC) and Union Internationale Contre Le Cancer
(UINCC),and is recommended by the College of American
Pathologists (CAP).(65,81)It is more accurate, but too
cumbersome for general use.(4) Currently the TNM system is
widely used, & is internationally accepted.(67)
22
*** TNM Classification of carcinoma of the colon & rectum:
T: primary tumor.
TX: primary tumor can not be assessed.
Tis: carcinoma insitu (intraepithelial) or intramucosal
(lamina propria invasion).
T1: tumor invades submucosa.
T2: extending into the muscularis propria, but not penetrating
through it.
T3: penetrating through the muscularis propria into the serosa
into non-peritonealized paracolic or perirectal tissues.
T4: tumor directly invades other organs or structures and/or
perforates visceral peritoneum.
N: regional lymph nodes.
NX: regional lymph nodes can not be assessed.
N0: no regional lymph node metastasis.
N1: metastasis in 1 or 3 lymph nodes.
N2: metastasis in 4 or more lymph nodes.
M: distance metastasis.
MX: distant metastasis can not be assessed.
M0: no distant metastasis.
M1: distant metastasis.
23
Stage grouping:
Stage 0 Tis N0 M0
Stage I T1 N0 M0
T2 N0 M0
Stage ІΙ T3 N0 M0
T4 N0 M0
Stage ΙΙΙ any T N1 M0
any T N2 M0
Stage ΙV any T any N M1
Tumor Grading:
Grading of a tumor is an expression of the aggressiveness
of the neoplasm. It is based on the degree of differentiation of the
tumor cells&the number of the mitosis within the tumor.(3)
The histological grading of CRC is evaluated subjectively.
Although a number of grading systems have been suggested in
the literature, there is no single accepted standard for grading. The
number of grades & the criteria in each differ among the various
grading schemes. In some systems, grades are defined on the
basis of a single microscopic feature, such as the degree of gland
formation, &in others the grades based on a number of features.(67)
However, most systems stratify tumors into three or four grades as
follows:
24
GRADE 1: well differentiated. The glandular structure is
> 95% of the tumor,(6) & is composed of simple tubule
with easily discerned nuclear polarity.(68)
GRADE 2: moderately differentiated. The glands are 50% - 95%
of the tumor,(6) & are irregular with barely discernable
or lost nuclear polarity.(68)
GRADE 3: poorly differentiated. The glandular structure is
5%-50%(6) or absent with loss of the nuclear polarity.(68)
GRADE 4: undifferentiated,(67) & the glandular structure is <5% of
the tumor.(6)
Mucinous adenocarcinoma & signet ring cell carcinomas are
considered poorly differentiated (grade 3). Medullary carcinoma
with MSI-H appears undifferentiated.(6)
In general a two-typed grading system based solely on
proportion of gland formation (> or < 50% glands formation) would
be expected to reduce interobservor variability. This system is as
follows:
LOW GRADE: include the well differentiated& moderately
differentiated tumors.(58)
HIGH GRADE: include poorly differentiated & undifferentiated
tumors.(82)
25
So the use of a two-typed grading system for CRC is
advisable, & such system has been recommended by colorectal
working group of a 1999 Consensus Conference sponsored by the
College of American Pathologists (CAP).(83)
1.10.Treatment:
The three main types of treatment for CRC are surgery,
radiation therapy, and chemotherapy.(19) Surgery includes
segmental resection of the tumor with adequate margins along with
potentially involved lymph nodes.(4)
Newer targeted therapies called monoclonal antibodies are
now beginning to be used as well. Depending on the stage of the
cancer, two or more types of treatment may be used at the same
time, or one after the other.(19)
♦ Early stage colon cancer:
Surgery is initial therapy for choice for localized, potentially
curable cases.(1) It is either open surgery (colectomy with
colostomy) or laproscopic resection.(4,84)
Postoperative radiation and adjuvant chemotherapy with
5-Fluorouracil (5-FU) reduce the risk of recurrence.(85,86)
26
• Early stage rectal cancer: Also surgery is the main treatment. Transanal endoscopic
microsurgery (TEM) is now preferred form of local treatment for
rectal polyps & stage І rectal cancer that are small & near the
anus.(4,84) A low anterior resection is for cancers near the upper
part of the rectum.(19) For cancers in the lower part of the rectum,
abdominoperitoneal resection with colostomy is done.(4,19) The
surgery should be followed by chemoradiation which improve
survival and local control of the tumor.(87)
Most studies regimens consist of surgery and postoperative
chemotherapy with 5-FU & mitomycin within 6 weeks, followed by
radiation plus concurrent chemotherapy.(88)
• Metastatic cancer:
Is treated by surgery (after preoperative evaluation),
postoperative radiation (for palliative treatment of symptoms), and
systemic chemotherapy with various 5-FU based regimens.(1)
• New developments in treatment of CRC:
- Drugs being developed to enhance the tumor-killing ability of
radiation therapy & chemotherapy, and stop the angiogenesis.
- Gene therapy.
- Immunotherapy: enhances the body’s immune system to kill
tumor cells.
27
- Monoclonal antibodies to identify tumor cells for destruction or
prevent their division.
- Vaccines: cause the body to produce more antibodies to kill
cancer cells.(89)
1.11. Prognosis:
The 5-year crude survival rate after curative resection for
CRC ranges between 40%-60%. Local recurrence and/or regional
lymph node metastasis occur in over 90% of the failure cases.(14)
The prognosis of CRC is affected by a number of clinical
variables, pathological features, oncogenetic, molecular, &
immunological variables. The pathologic stage & the factors
affecting it remain the most prognostic factors.(90) The 5-year
survival rate are ~90% for Duke’s A, 5o-65% for Duke’s B, and
15-25% for Duke’s C.(14,90)
Poor prognostic factors include: elevated CEA level, which is
the only consistently predictive clinical feature; mucinous & signet
ring pattern on histology; bowel wall/ regional lymph node/
perineural invasion; evidence of bowel obstruction or
perforation;(1)DNA ploidy; DCC gene deletion; P53 & Ki-ras
mutation;(91) mucin associated antigens;(92) growth factors &
receptors expression.(93)
28
1.12. Recurrence:
Is manifested by occurrence of symptoms after
treatment,(94)& can be:
(1) Locoregional: the recurrence is in or around the anastomotic
site. It results from positive surgical margins.(4)
(2) Peritoneal metastasis: result from seeding of the peritoneal
cavity by the tumor prior to surgery.(4)
(3) Distant metastasis: may manifest in lymph nodes more
proximal to those in the field of initial surgery&elsewhere in
the body due to haematogenous spread.(4)
Recurrence is best detected by: serial serum assays for
CEA, CT scans, radionuclide liver scans, & regular colonoscopy in
the first year after surgery.(4,14)
Recently, a new blood test for detection of recurrence has
been announced. This test is called GCC-B1TM.It tests for the
presence of the protein guanylyl cyclase C in the blood, which is
normally only found in the intestine. This test has the ability to
detect 90%-100% of CRC metastasis.(95)
29
OBJECTIVES
General objectives:
To study the pattern of patients with CRC in Khartoum State,
Sudan; from January 2001 through to December 2004 with view to
determine various epidemiological & clinicopathological features of
this malignancy.
Specific objectives:
1- To determine the histopathological patterns of CRC.
2- To determine the residency distribution, clinical presentation &
relation of CRC with age & sex.
30
METHODOLOGY
2.1. Study design:
A descriptive retrospective study.
2.2. Study field:
Ibn Sina Hospital at Khartoum, Sudan. It is specified for
renal & gastrointestinal diseases. It receives patients from different
regions of Sudan for diagnosis & management.
2.3. Study Population:
All cases of colorectal cancer presented to Ibn Sina Hospital
between January 2001 through to December 2004.
2.4. Inclusion Criteria:
Colorectal cancer patients who under-went endoscopic and
histopathological studies for diagnosis, with or without laboratory
and radiological studies.
2.5. Exclusion Criteria:
Colorectal cancer patients who had no histopathological
slides in the histopathology lab of the hospital.
2.6. Tools of data collection:
Data were collected from the patients’ request forms into a
predesigned questionnaire with detailed history and investigations.
The patients in this study had been diagnosed by histological
31
examination of surgical or endoscopic biopsies which had been
processed to provide slides for microscopic examination. The
processing include fixation (in 10% formalin), dehydration (by
different concentrations of alcohol), clearing (using xylene), &
impregnation (with paraffin wax). Then the tissues were blocked by
transferring them from the final wax bath into a mold filled with
molten wax. The block was then quickly cooled. The tissue was cut
by microtome, & the cut sections were flooded on a mounting bath.
Then the sections were mounted on an ordinary slides, put in a hot
oven or hot plate to remove the wax & finally stained by routine H
& E method. The slides of the histopathological diagnosis for
patients were collected& reviewed to: confirm the CRC diagnosis;
determine the histopathological type of the tumor using the WHO
classification of CRC; and grade the tumor using the well
differentiated, moderately differentiated, poorly differentiated,
&undifferentiated Grading System.
2.7. Statistics:
The data were analyzed using computer S.P.S.S program,
version 10.
32
RESULTS
There were 123 patients with CRC during the 4 years study.
When the slides reviewed, 23 patients had no available slides & so
were excluded from this study. The remainders (100 cases) were
analyzed.
3.1. Characteristics of the studied patients:
3.1.1. Age distribution: The ages ranged from 14-85 years with a mean of 49.89±
16.86.Thirty-three (33%) patients were below 40 years of age. The
youngest patient was 14 years old. The peak age of incidence was
> 60 years (Figure 1).
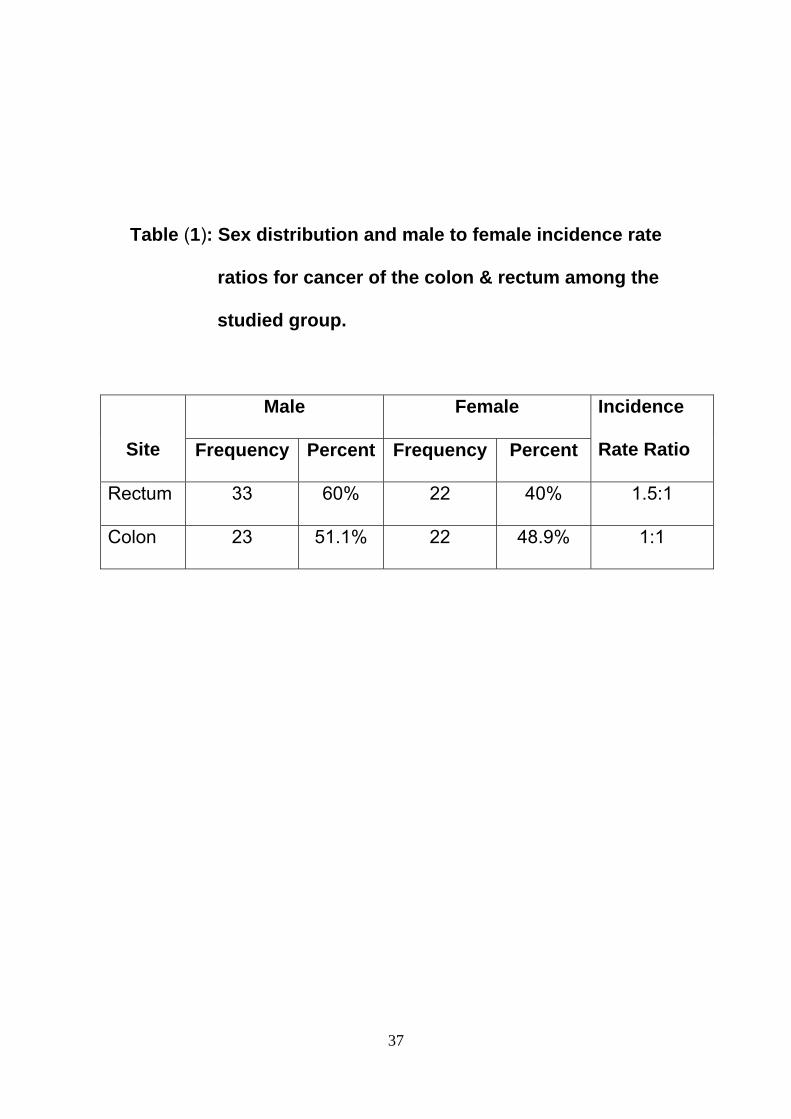
3.1.2.Sex distribution:
Fifty-six (56%) patients were males compared to 44 (44%)
females (Figure 2). The colon cancer cases were 45 cases, while
those of the rectum were 55 cases. The 45 colon cancer cases
distributed almost equally between males & females (23 males &
22 females), where as rectal cancers (55 cases) encountered more
among males (33 cases) compared to females (22 cases). As a
result of these findings, the male to female incidence rate ratio
(R.R) for colon cancer was 1:1 and for rectal cancer was 1.5:1. For
all CRC it was 1.1:1 (Table 1).
33
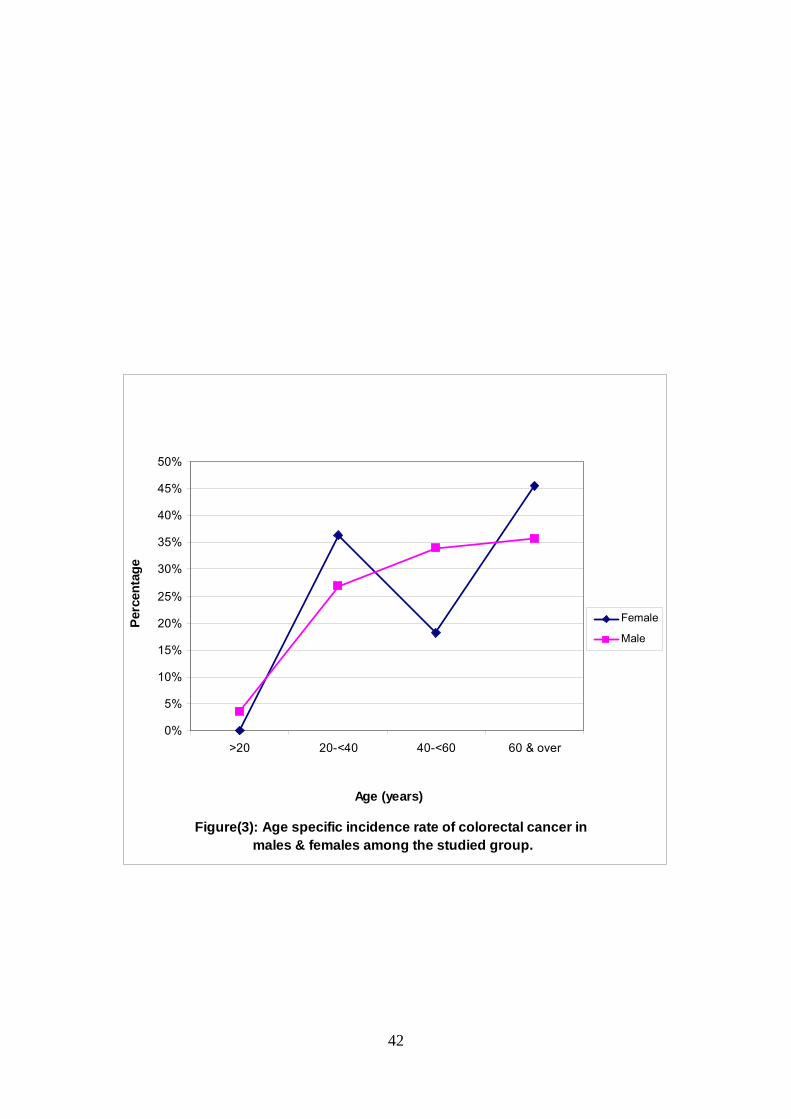
The incidence rate for males increases slowly with age until
reaching peak at the age of 60 & over, while females had two
peaks, one at the age group 20-<40, & the other at the age group
60 & over (Figure 3).
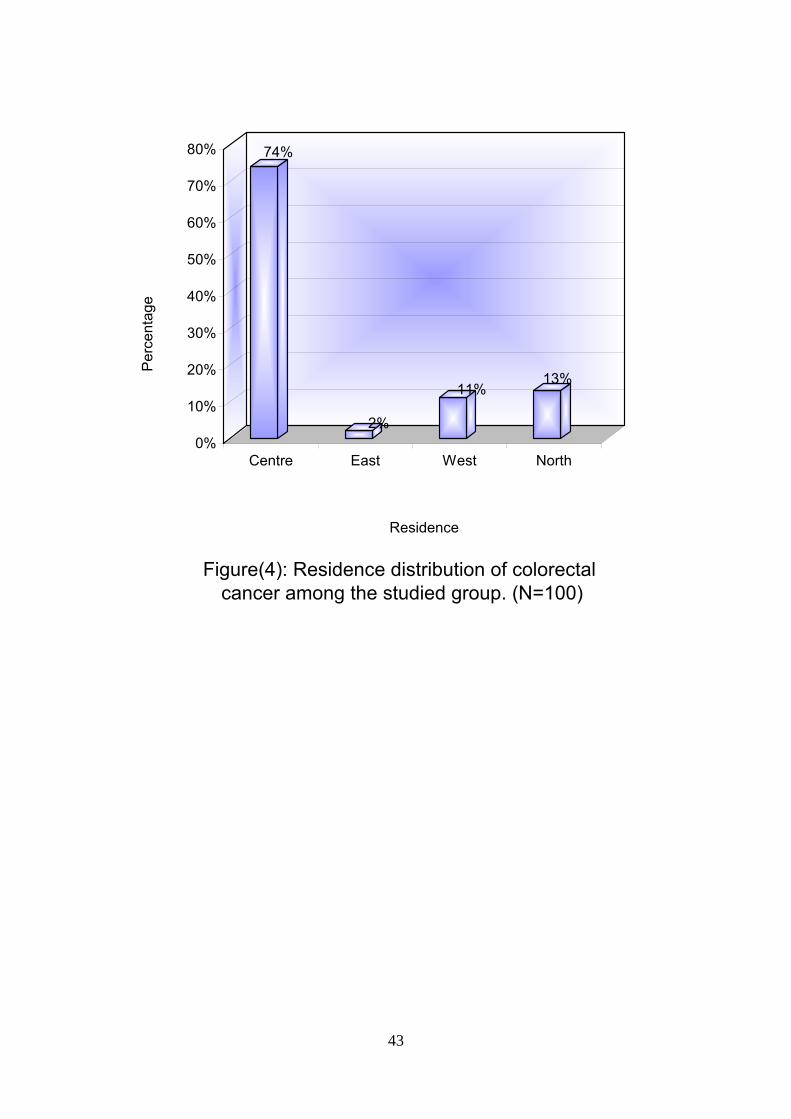
3.1.3.Residency distribution in CRC:
As regard to residency, seventy-four (74%) patients were
from the middle of Sudan (more than two thirds of them were
from Khartoum), thirteen (13%) patients were from the North,
eleven (11%) patients were from the West, two (2%) patients were
from the East, and no one was from the South (Figure 4).
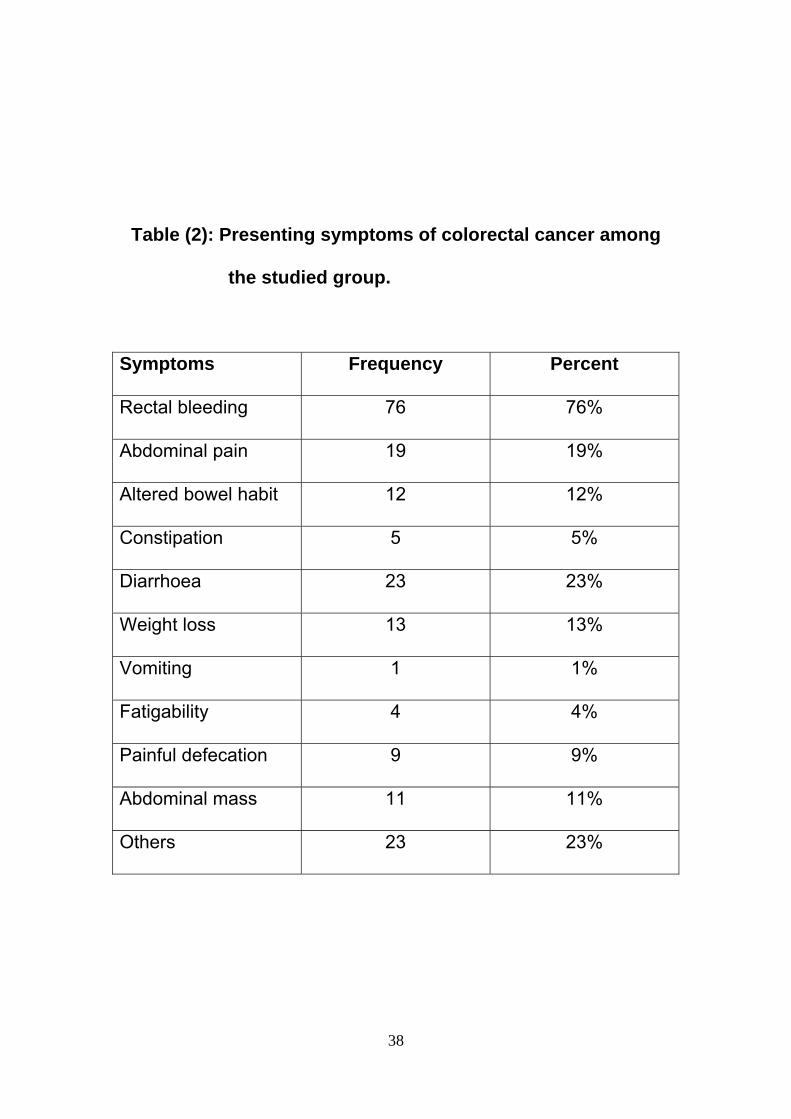
3.2. Distribution of the clinical symptoms in the
studied patients:
Table 2 shows the various presentations of CRC in the
studied patients. Rectal bleeding represented the majority (76%) of
the symptoms. About 90% of patients with rectal cancer presented
with frank rectal bleeding on presentation. The duration of the
symptoms varied from one to twelve months in the majority of
patients. Among the total, 61.2% of patients had symptoms ≤6
months duration, while 38.7% of patients had symptoms of >6
months.
34
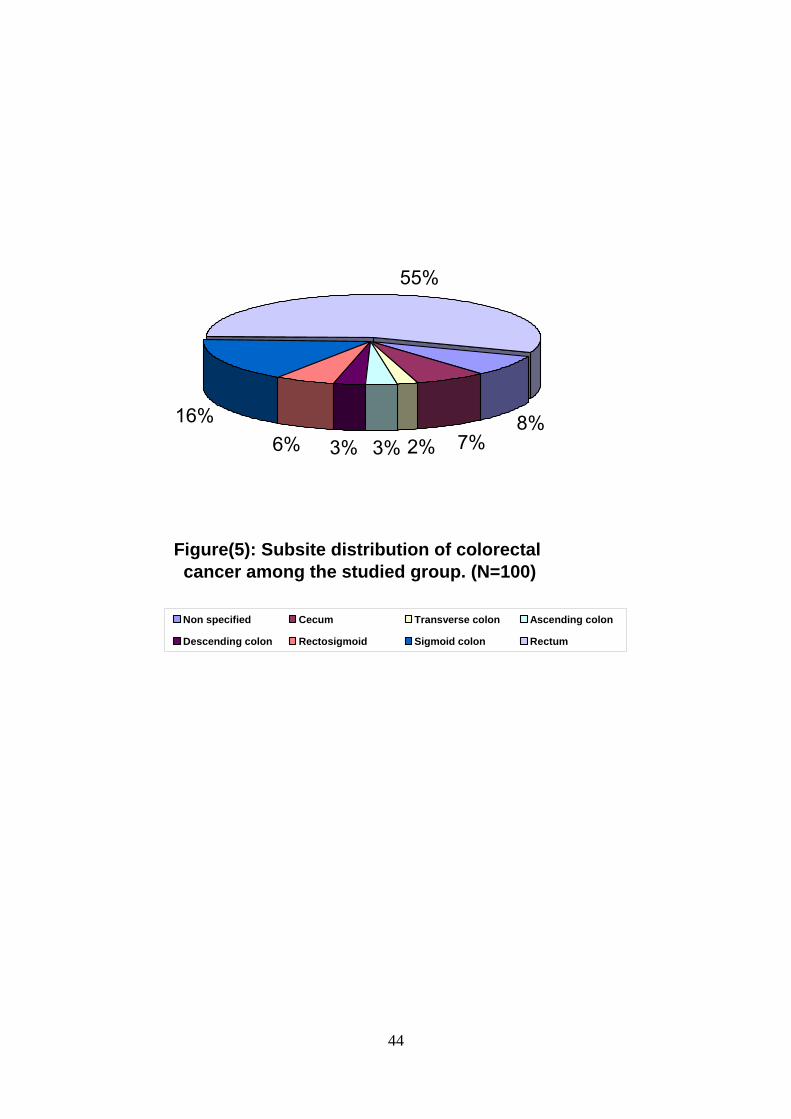
3.3. Subsite distribution of CRC in the studied
patients:
The majority of the tumors arising from the rectum, sigmoid
colon & rectosigmoid junction (77%), the transverse colon was the
least involved site (2%) (Figure 5).
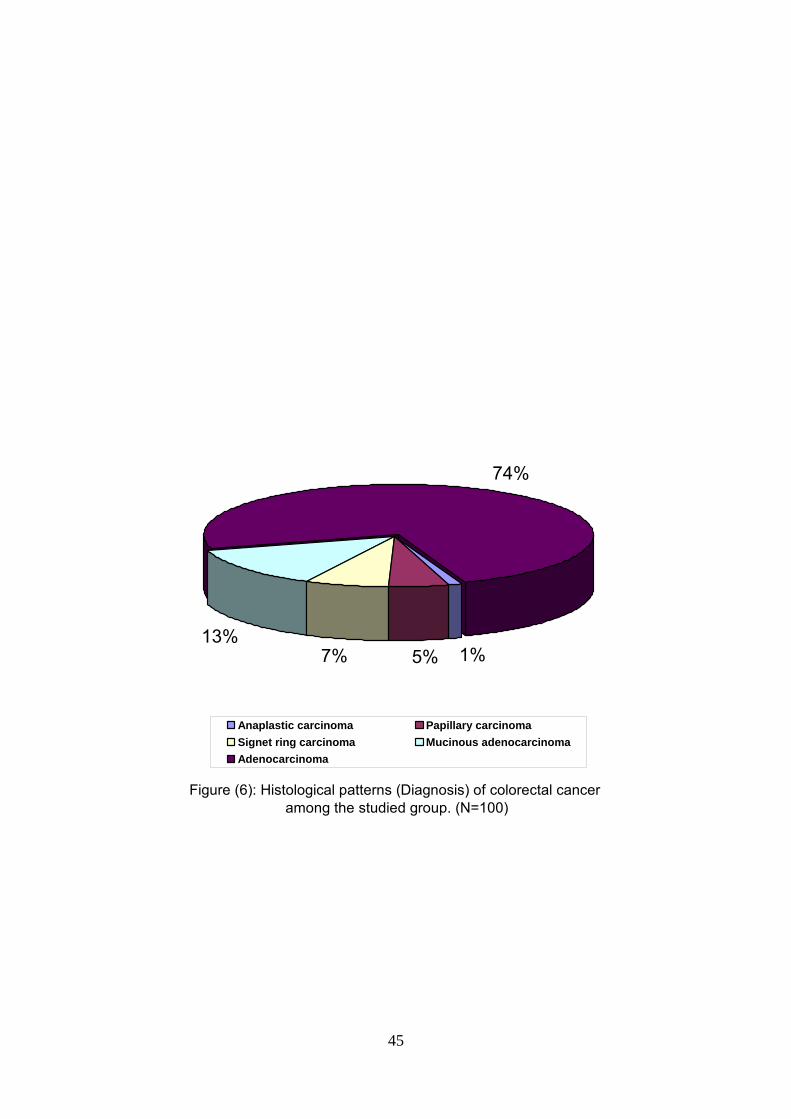
3.4 . Histopathological characteristics of CRC in the
studied patients:
3.4.1.Histological patterns:
The diagnosis of CRC in this study is based on
histopathological examination of endoscopic biopsies, combined
with U.S. examination. The serum level of CEA had been reported
in only 3 patients.
Adenocarcinoma was the most common tumor seen in 74%
of cases. 13 (13%) were Mucinous adenocarcinoma, 7 (7%) Signet
ring cell carcinoma, 5 (5%) Papillary carcinoma, & 1 (1%)
anaplastic carcinoma. (Figure 6).
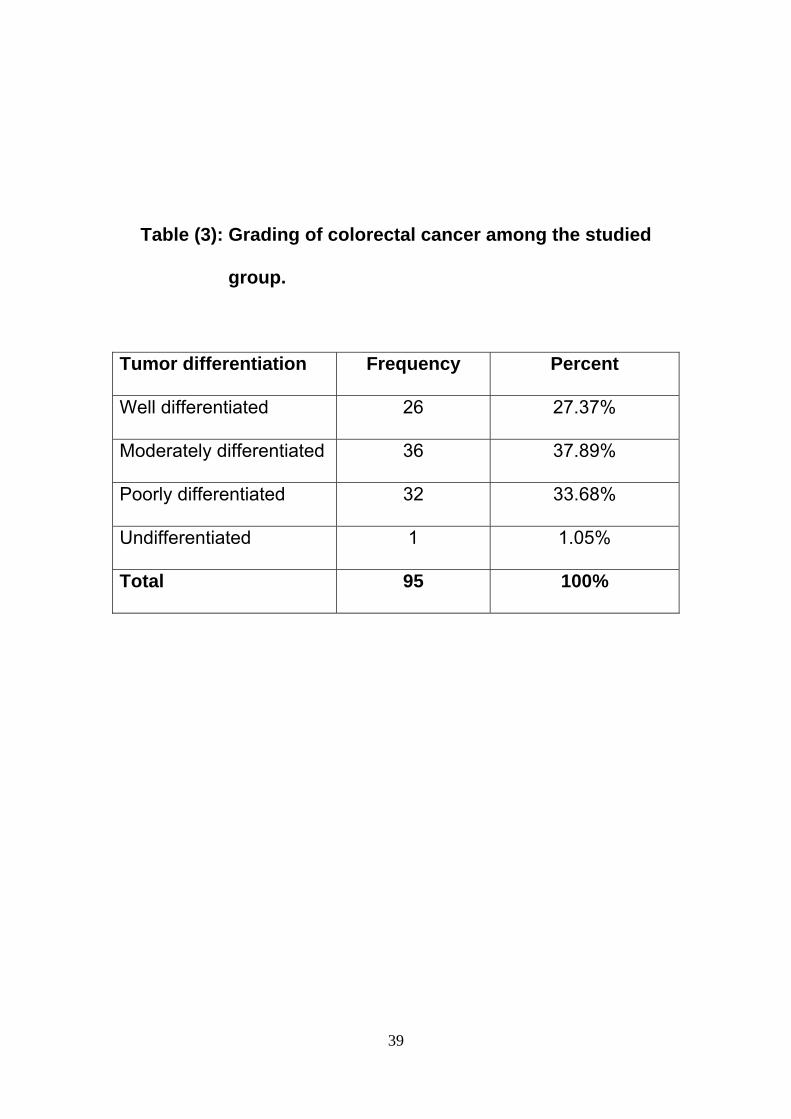
3.4.2.Grading:
The moderately differentiated adenocarcinoma represented
the majority of CRC cases (38.3%), followed by the poorly
differentiated adenocarcinoma, & then the well-differentiated
adenocarcinoma became the least (Table 3).
35
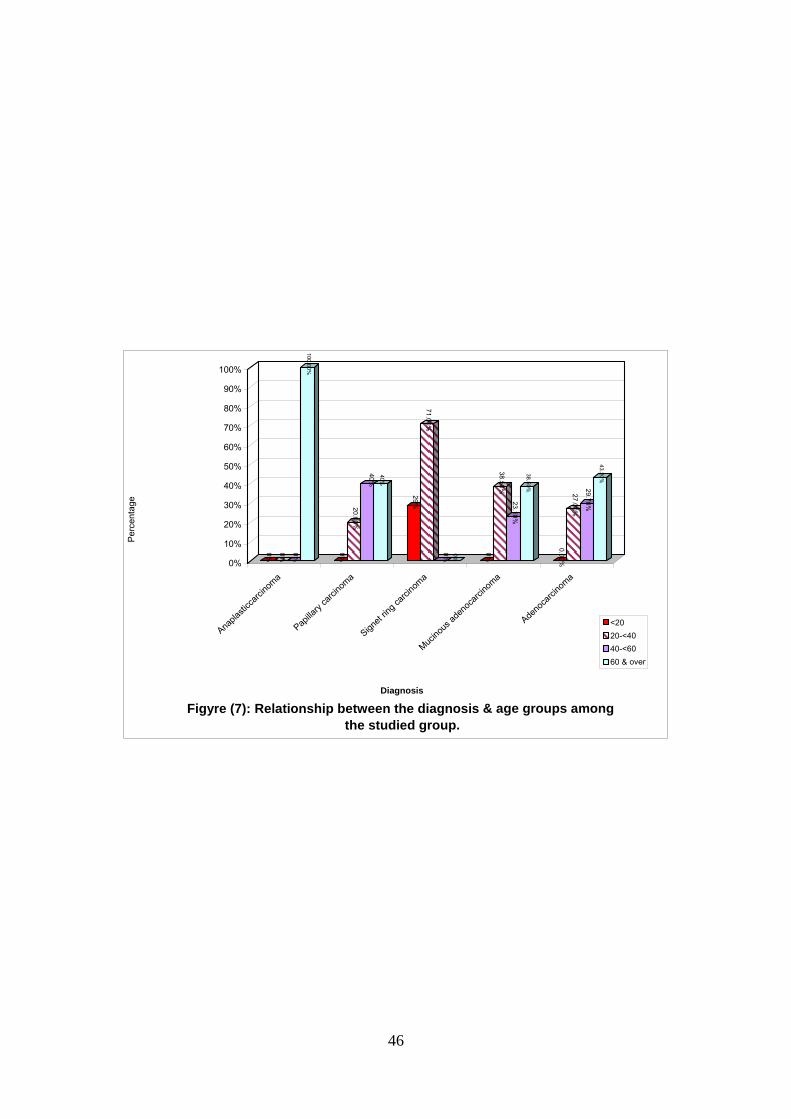
3.5. Relationship between the histological patterns of
CRC & the age groups in the studied patients:
The adenocarcinoma was predominant (43.2%) among
those ≥ 60 years of age compared to the other age groups. The
mucinous type was highest (40%) and equally distributed between
the age groups 20-<40 & ≥ 60 years. The signet ring carcinoma
was more common (71%) among the age group 20-<40 years.
Finally the anaplastic type was found to be confined to the age
group ≥ 60 years (Figure 7).
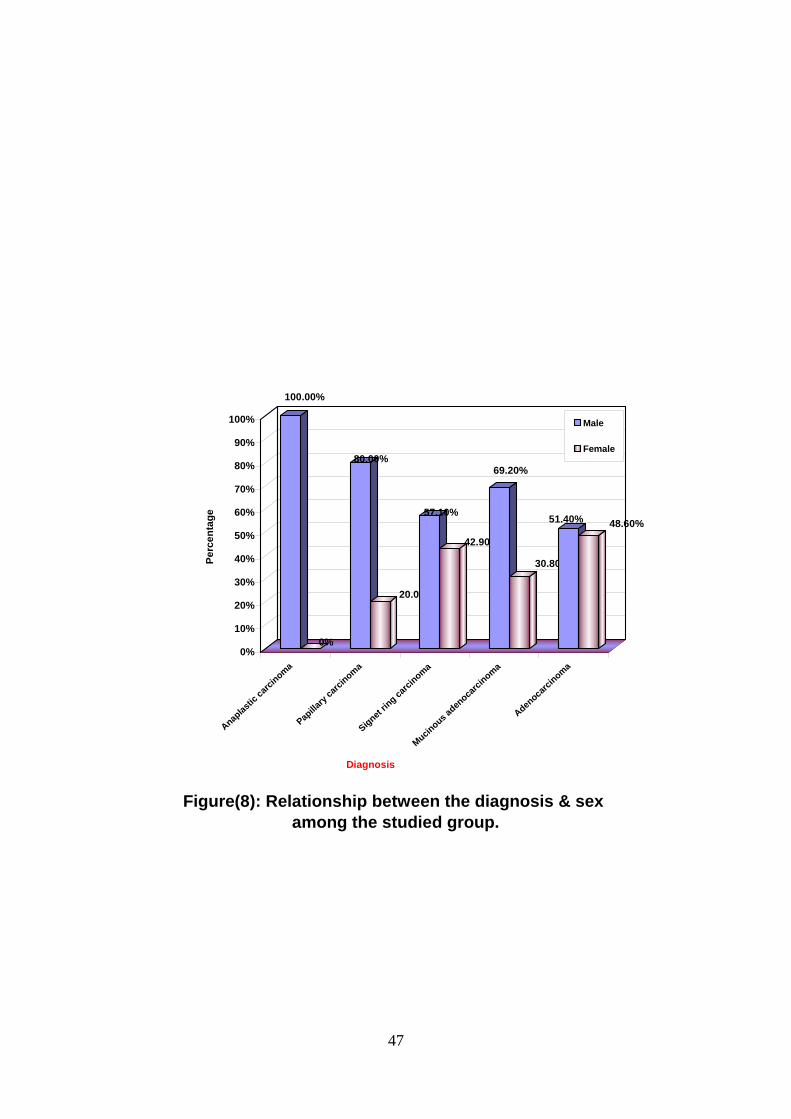
3.6. Relationship between the histological patterns &
the sex in the studied patients:
All the histological types of CRC were found to be more in
males than females. No female was reported with the anaplastic
type (Figure 8).
In the present study 3 patients were reported as cases of
recurrence of CRC, one patient with signet ring cell carcinoma &
the other two with well-differentiated adenocarcinoma.
Metastasis was reported in one patient.
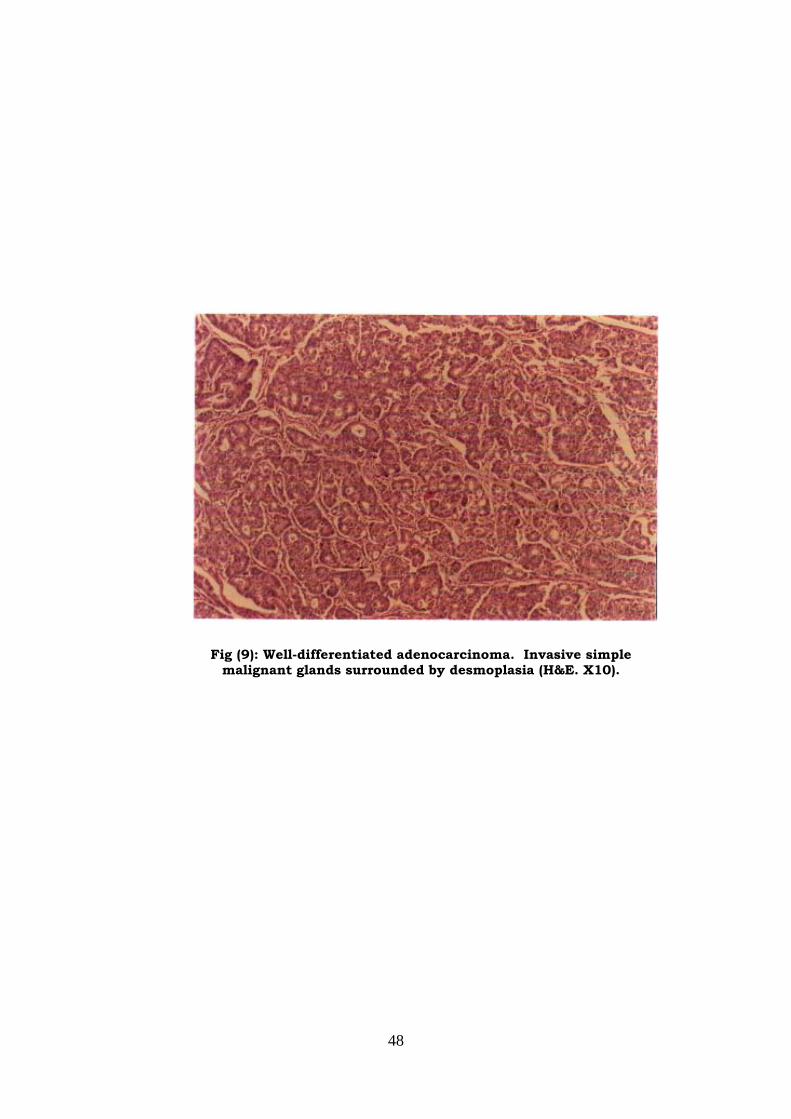
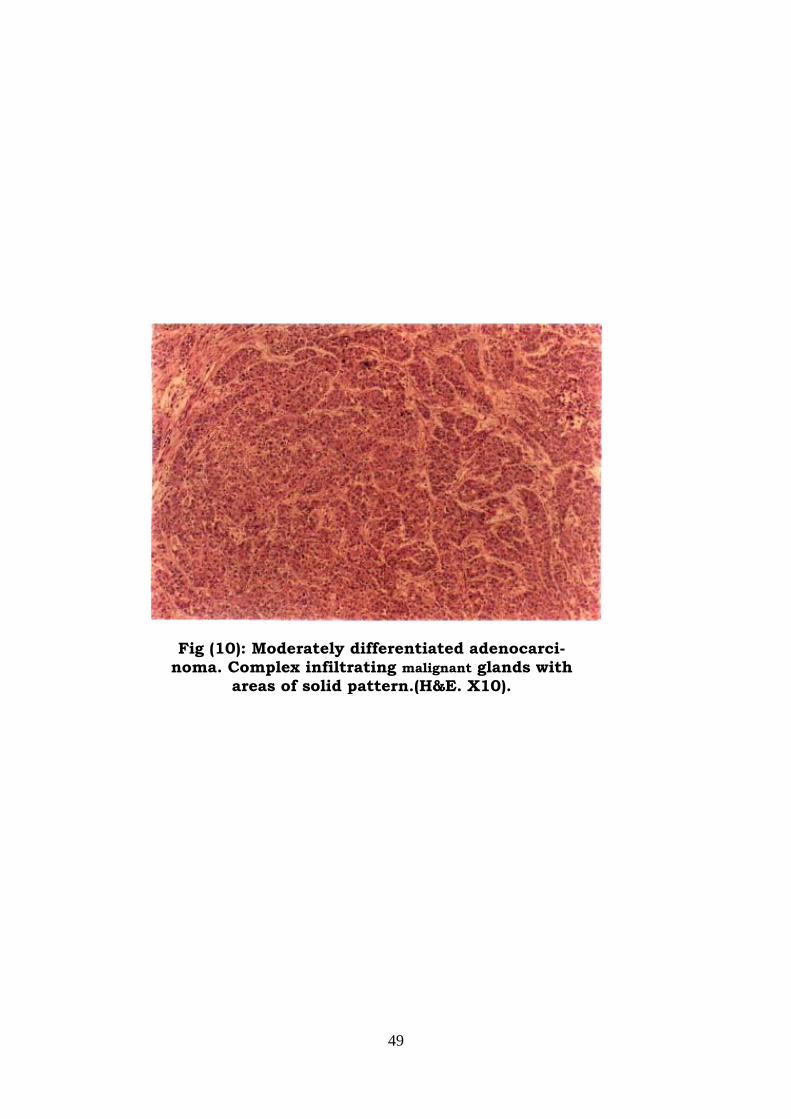
Histology of tissue biopsies was shown in (Figures 9, 10,
11, 12, 13& 14 ) as well differentiated adenocarcinoma,
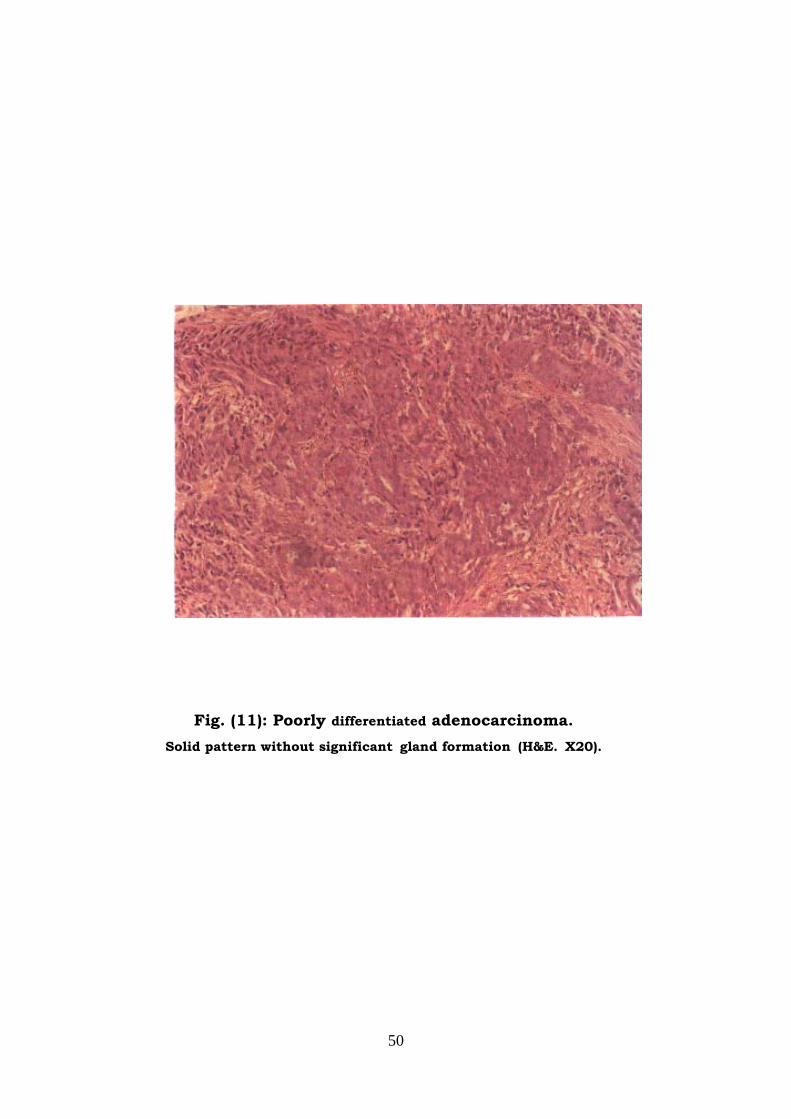
36
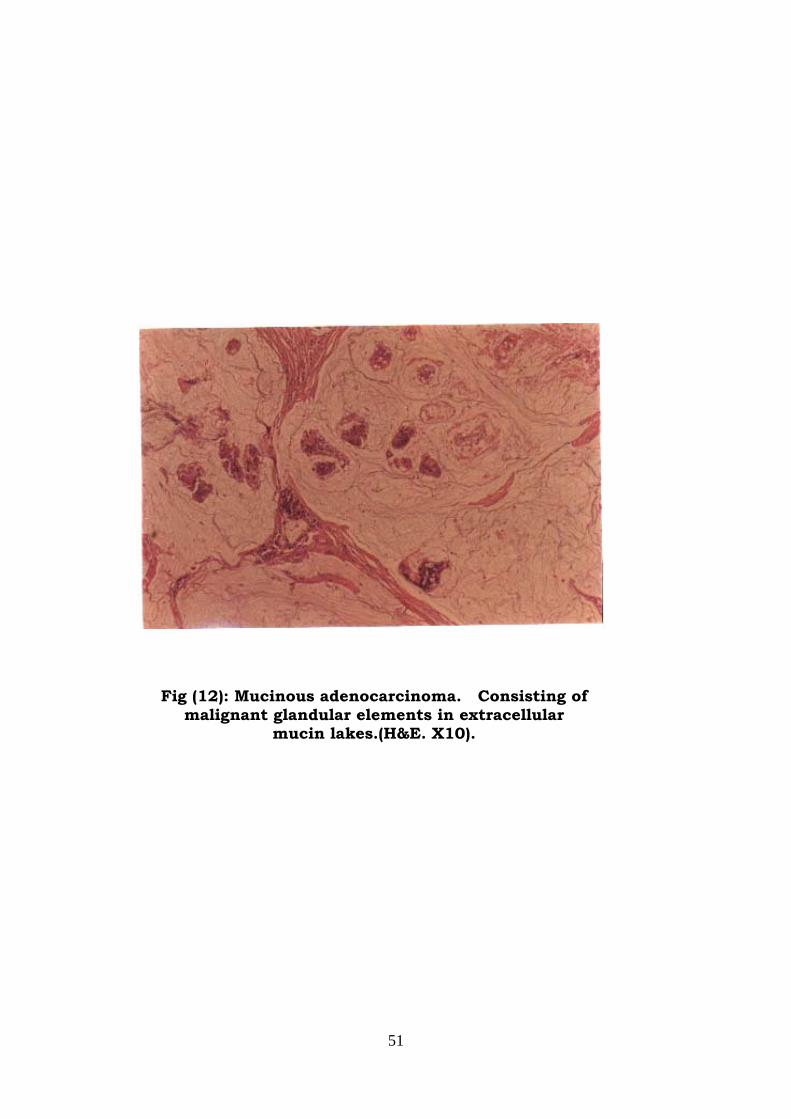
moderately differentiated adenocarcinoma, poorly differentiated
adenocarcinoma, mucinous adenocarcinoma, signet ring cell
carcinoma & papillary carcinoma, respectively.
37
Table (1): Sex distribution and male to female incidence rate
ratios for cancer of the colon & rectum among the
studied group.
Male Female
Site Frequency Percent Frequency Percent
Incidence
Rate Ratio
Rectum 33 60% 22 40% 1.5:1
Colon 23 51.1% 22 48.9% 1:1
38
Table (2): Presenting symptoms of colorectal cancer among
the studied group.
Symptoms Frequency Percent
Rectal bleeding 76 76%
Abdominal pain 19 19%
Altered bowel habit 12 12%
Constipation 5 5%
Diarrhoea 23 23%
Weight loss 13 13%
Vomiting 1 1%
Fatigability 4 4%
Painful defecation 9 9%
Abdominal mass 11 11%
Others 23 23%
39
Table (3): Grading of colorectal cancer among the studied
group.
Tumor differentiation Frequency Percent
Well differentiated 26 27.37%
Moderately differentiated 36 37.89%
Poorly differentiated 32 33.68%
Undifferentiated 1 1.05%
Total 95 100%

40
40%
27%31%
2%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Perc
enta
ge
60&over 40-<60 20-<40 <20
Age (years)
Figure(1): Age distribution of colorectal cancer among the studied group. (N=100)
41
Figure(2): Sex distribution of colorectal cancer among the studied group. (N=100)
Female44%
Male56%
42
Figure(3): Age specific incidence rate of colorectal cancer in males & females among the studied group.
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
>20 20-<40 40-<60 60 & over
Age (years)
Perc
enta
ge
Female
Male
43
74%
2%
11%13%
0%
10%
20%
30%
40%
50%
60%
70%
80%P
erce
ntag
e
Centre East West North
Residence
Figure(4): Residence distribution of colorectal cancer among the studied group. (N=100)
44
Figure(5): Subsite distribution of colorectal cancer among the studied group. (N=100)
8%7%2%3%3%6%
16%
55%
Non specified Cecum Transverse colon Ascending colon
Descending colon Rectosigmoid Sigmoid colon Rectum
45
Figure (6): Histological patterns (Diagnosis) of colorectal cancer among the studied group. (N=100)
1%5%7%13%
74%
Anaplastic carcinoma Papillary carcinomaSignet ring carcinoma Mucinous adenocarcinomaAdenocarcinoma
46
0% 0% 0%
100.00%
0%
20.00%
40%40%
29%
71.00%
0% 0%
0%
38.50%
23.10%
38.50%
0.00%
27.00%
29.70%
43.20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Perc
enta
ge
Anapla
sticc
arcino
ma
Papilla
ry ca
rcino
ma
Signet
ring c
arcinom
a
Mucinou
s ade
noca
rcino
ma
Adeno
carci
noma
Diagnosis
Figyre (7): Relationship between the diagnosis & age groups among the studied group.
<2020-<4040-<6060 & over
47
100.00%
0%
80.00%
20.00%
57.10%
42.90%
69.20%
30.80%
51.40% 48.60%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Perc
enta
ge
Anaplas
tic ca
rcinoma
Papilla
ry ca
rcinoma
Signet rin
g carci
noma
Mucinous a
denoca
rcinoma
Adenoca
rcinoma
Diagnosis
Figure(8): Relationship between the diagnosis & sex among the studied group.
Male
Female
48
Fig (9): Well-differentiated adenocarcinoma. Invasive simple malignant glands surrounded by desmoplasia (H&E. X10).
49
Fig (10): Moderately differentiated adenocarci-noma. Complex infiltrating malignant glands with
areas of solid pattern.(H&E. X10).
50
Fig. (11): Poorly differentiated adenocarcinoma. Solid pattern without significant gland formation (H&E. X20).
51
Fig (12): Mucinous adenocarcinoma. Consisting of malignant glandular elements in extracellular
mucin lakes.(H&E. X10).
52
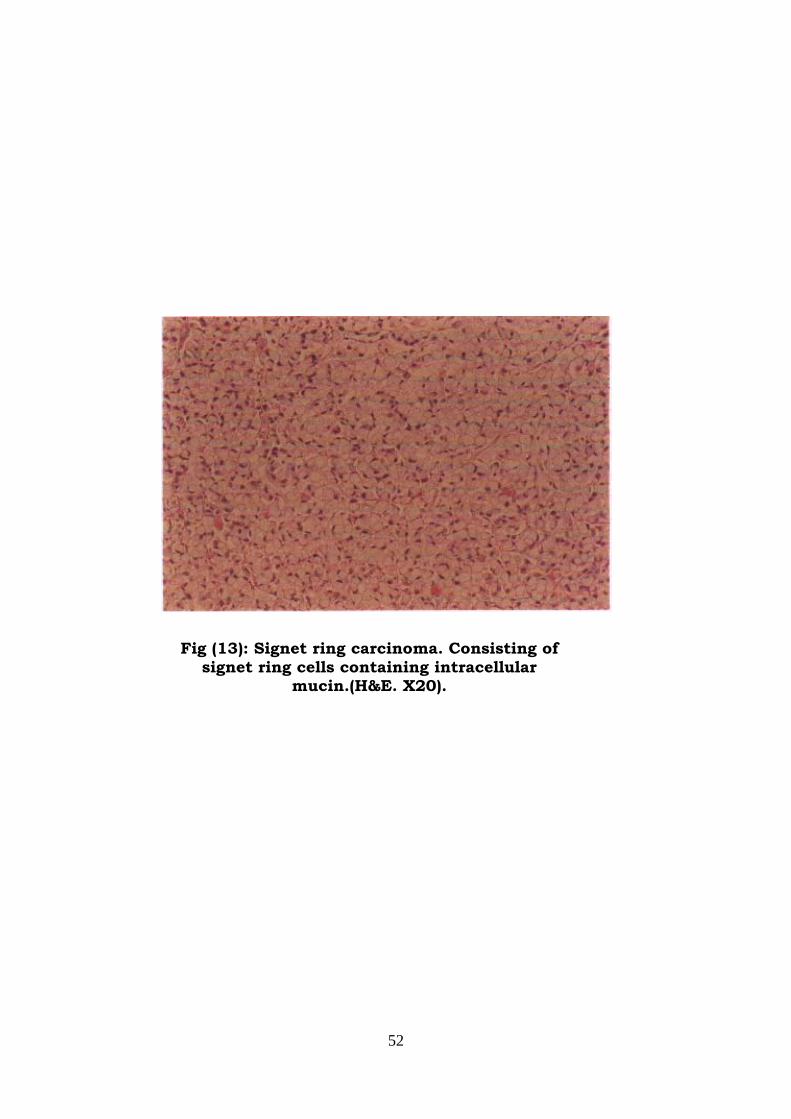
Fig (13): Signet ring carcinoma. Consisting of signet ring cells containing intracellular
mucin.(H&E. X20).
53
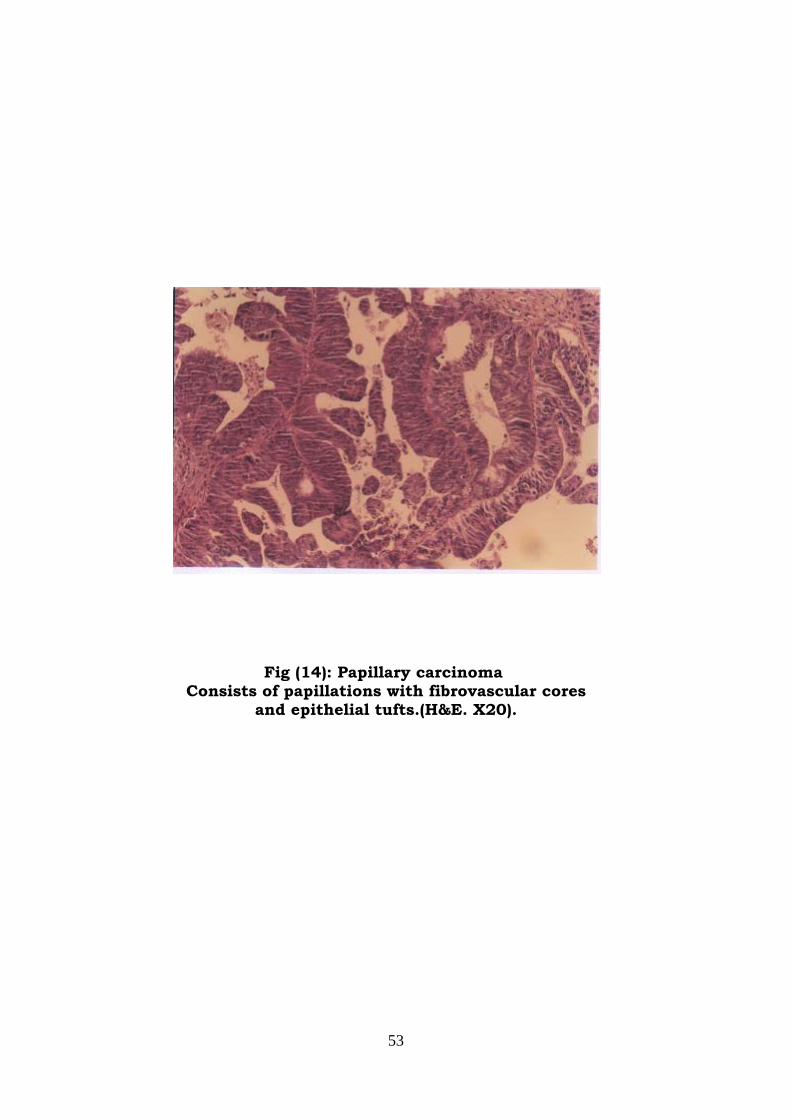
Fig (14): Papillary carcinoma Consists of papillations with fibrovascular cores
and epithelial tufts.(H&E. X20).
54
DISCUSSION
This is a descriptive retrospective study about CRC in
Sudanese patients. It was carried in the period from January 2001
to December 2004 & includes analysis of 100 cases.
The epidemiology of CRC has generated more interest
recently due to new developments in genetics and molecular
biology of this disease. The epidemiological pattern of the disease
varies markedly between different population groups.(96)
The incidence of CRC has been of great interest to many
workers particularly in African countries, were it has been reported
to be relatively lower than in affluent societies.(7) The World Health
Organization(WHO) forsees the overall global situation in respect
to CRC will be worsen.(97) During the latter years in Sudan, there
has been a significant increase not in the total number of cancers
but also in the cancers of the large bowel. The socioeconomic
changes & urbanization, which take place in Sudanese society,
entails characterization of this cancer, which is usually linked with
economic development.
In Sudan as in most developing countries, there is at
present no reliable statistical information on absolute cancer rates.
55
As our study was limited to registered data, many difficulties were
faced in the interpretation of the results due to undetailed history,
histopathological diagnosis & staging of the neoplasia. As a result
of this, our study indicated that 74% were adenocarcinoma, in
contrast to what accepted globally that, up to 98% of CRC are
adenocarcinoma.(16) But in general the adenocarcinoma
represented the majority (74%) of histopathological patterns of
CRC in this study. Other histological types seen were signet ring
carcinoma (7%), mucinous carcinoma (13%), papillary carcinoma
(5%) & anaplastic carcinoma (1%). No cases of anaplastic or
papillary carcinoma were reported in reviewed local studies.
In this study, our results are in accordance with the literature
regarding the occurrence of high number of cases among
males.(16,17) It was reported that CRC has a different sex
distribution with nearly similar incidence between the males &
females for colon cancer and a male preponderance for rectal
cancer.(16) This is almost the same trend encountered with males
to females incidence rate ratio for colon & for rectal cancer in this
study. The high incidence of rectal cancer in males can also be
explained by the fact that Sudanese females are very shy & very
reluctant to specific examination as proctoscopy & sigmoidoscopy.
56
Another important features highlighted by the study is the
resemblance of our data with those from developing countries
regarding the early age of onset of CRC & left side subsite
preponderance,(98,99,100,101,102) compared to late age at diagnosis &
right side cancer (proximal shift) in the developed countries.(103)
Early age of incidence is a characteristic in developing countries.
Under age of 40, there are more than one-third of cases in
Egypt,(99) 21.4% in Saudi Arabia,(104) & 17% in Philippine,(102)
compared to 3.6% in USA,(105) & 7.6% in Canada,(106) In our study
only four patients were reported to have history of U.C. & all the
four were young patients. This in addition to another young patient
with positive family history of CRC. But these can not fully explain
the early incidence of CRC.
In the present study, left side preponderance is clear as 77%
of cases in the rectum, rectosigmoid junction, & sigmoid colon. In
addition to 2% of cases in the descending colon. The proximal shift
in developed countries is not clearly discussed in the literature,
although some relate it to possibly more effective screening in the
right side, or to real reduction In rectal cancer incidence.(103)
In this study the incidence rate for males increases with age,
at first rapidly till the age group 20-<40 years, then slowly until
reaching a peak at the age group 60 years & over. While females
57
had two peaks, one at the age group 20-<40 years & the other at
the age group 60 years & over. Both of the females’ peaks were
higher than those of males. This compared to a study done in
Yemen in which both sexes showed their peak incidence at the
age group 55-<65 years, but the peak for males was higher than
that for females.(107)
Regarding the residency, most of the patients (74%) were
from the central region of Sudan, of them about two thirds were
from Khartoum. No one was found to be from the South. These
may be due to the following factors:
(1) Most of the Sudanese are clustered in the big towns.
(2) There is discrepancy between the number of doctors,
particularly specialists, & the populations they serve.
(3) Because of difficulty in the transportation, many patients,
especially from the rural regions, are unlikely to reach
hospitals.
(4) Finally, the shortage in medical services & the war situations in
Southern Sudan prevented southern patients from reaching
hospital.
The racial history of the patients was not found in the
records, so was not analyzed.
58
The majority of patients present with symptoms of bleeding
per rectum (76%), diarrhoea (23%), abdominal pain (19%), weight
loss (13%) & altered bowel habits (12%) in various combinations.
While acute obstruction & perforation were not features, as this
hospital deals with elective operations only. The duration of
symptoms varies from one month to one year in the majority of
patients, with a median of 6 month of the total duration. In fact
>50% of patients had symptoms < 6-month duration & this can be
explained by the fact that: most of the patients in this study
presented with rectal bleeding, which is the symptom that make
patient to seek medical advice.
The majority of patients in this study present with tumors at
early stages of differentiation (moderately & well differentiated),
while few number present with poorly & undifferentiated tumors.
This may be due to increase awareness of cancer & improved
facilities for diagnosis.
In this study anaplastic carcinoma show the highest
incidence in males, while in females adenocarcinoma show the
highest incidence. Signet ring carcinoma was predominant in the
younger age group compared to other age groups, while
anaplastic carcinoma & adenocarcinoma were predominant in the
age group 60 years & over.
59
CONCLUSION
• Only 5 histological variants were identified in this study i.e.
adenocarcinoma, mucinous carcinoma, signet ring carcinoma,
papillary carcinoma, & anaplastic carcinoma.
• CRC is not an uncommon disease in this part of the world as
used to be considered previously.
• Despite limitation in the background history, detailed
histopathological diagnosis & staging, the study indicated that
developing countries characteristics as the presence of relatively
high proportion of early onset tumor & left-sided preponderance
are clear.
60
RECOMMENDATIONS
• Further in-depth studies should be carried out to address the
possible community-related risk factors of this cancer & to know
the causes of early-onset CRC.
• Education of the public about the nature of the disease & about
the warning signs of CRC. And to achieve this; efficient use of
press & audiovisual media is necessary. • Execution of screening programs for early detection & better
outcome. • Detailed histopathological diagnosis & staging, & improvement
of cancer reporting & registering activities. • The request form should be designed to contain detailed history
about the patient. • Construction of a bowel clinic for the lower gastrointestinal
problems.
61
REFERENCES
1. www.oncolink.upenn.edu. Colorectal cancers general
information. December 2001.
2. Norton JA, Bollinger RR, Chang AE, Lowry SF, Mulvihill SJ,
Pass HI. Colorectal polyps and cancer. Surgery: Basic science
and clinical evidence. New York: Springer-verlag; 2001. P. 701-
707.
3. Kumar V, Abbas Ab.K, Fausto N. Colorectal carcinoma.
Robbins & Cotran, Pathologic Basis of Diseases. 7th edi.
California: Elseiver Saunders Company; 2005. P. 864-867.
4. Chandrasoma P, Dalton P. Colorectal adenocarcinoma.
Gastrointestinal Pathology. Los Angles: Asimon & Schuster
Company; 1999. P. 339-359.
5. www.nci.gov. Genetics of colorectal cancer. National Cancer
Institute. May 2005.
6. Hamilton AS, Aaltonen AL. Tumors of the colon & rectum.
World Health Organization classification of tumors, Pathology
and genetics of tumors of the digestive system. France, Lyon:
International Agency for Research on Cancer (IARC); 2000. P.
103-119.
62
7. Elmasri SH, Boulos PB. Carcinoma of the large bowel in
Sudan. Br J Surg 1975; 62: 284-286.
8. Zauber AG, O’Brien MJ, Winawer SJ. On finding flat
adenomas: is the search worth the gain? Gastroenterology
2002; 122 (3): 839-840.
9. Howe JR, Mitros FA, Summers RW. The risk of gastrointestinal
carcinoma in familial juvenile polyposis. Ann Surg Oncol 1998;
5 (8): 751-756.
10. Jeevaratnam P, Cottier DS, Browett PJ. Familial giant
hyperplastic polyposis predisposing to colorectal cancer: a new
hereditary bowel cancer syndrome. J Pathol 1996; 179 (1): 20-
25.
11. Rashid A, Houlihan PS, Booker S. Phenotypic and molecular
characteristics of hyperplastic polyposis. Gastroenterology
2000; 119 (2): 323-332.
12. www.cancer.gov/ publications. Colorectal cancer screening.
Cancer facts by National Cancer Institute. 2004 September.
13. Fraser J. Malignant disease of the large intestine. Br J Surg
1973; 25: 647-668.
14. Rosi J. Normal anatomy of the large bowel. Ackerman’s
Surgical Pathology. 8th edi. New York: Mobsy company; 1996.
P. 729-730.
63
15. Poyle P, Leon ME. Epidemiology of colorectal cancer. Br Med
Bull 2002; 64: 1-23.
16. The World Cancer Research Fund, The American Institute for
Cancer Research. Food, Nutrition and the Prevention of
Cancer: a global perspective. The World Cancer Research
Fund and the American Institute for Cancer Research.
Washington (DC): Banta Book Group; 1997.
17. Agency for Health Care Policy and Research (AHCPR).
Colorectal cancer screening: Executive Summary. Silver Spring:
AHCPR Publication Clearinghouse: Publication No. 97-0302:
2002.
18. Winawer SJ, Fletcher RH, Miller L, Godlee F, Stolar MH,
Mulrow CD. Colorectal cancer screening: clinical guideline and
rationale. Gastroenterology 1998; 114: 625.
19. www.cancer.org. What are the risk factors for colorectal cancer
& how colorectal cancer treated? Cancer reference information
by American Cancer Society. 2005 January.
20. Leppert M, Dobbs M, Scambler P, O’Connell, Nakamura Y,
Stauffer D. The gene for familial polyposis coli maps to the long
arm of chromosome 5. Science 1987; 238: 1411-1413.
64
21. Arvanitis ML, Jagelman DG, Fazio VW, Lavery IC, McGannon
E. Mortality in patients with familial adenomatous polyposis. Dis
Colon Rectum 1990; 33: 639-642.
22. Vasen HF, Griffioen G, Offerhaus GJ, Den Hartog Jager FC.
The value of screening and central registration of familial
adenomatous polyposis. A study on families in the Netherlands.
Dis Colon Rectum 1990; 33: 227-230.
23. Burke W, Petersen G, Lynch P, Botkin J, Daly M, Garber J.
Recommendations for follow-up care in individuals with an
inherited predisposition to cancer. I. Hereditary nonpolyposis
colon cancer. JAMA 1997; 277: 915-919.
24. Givannucci E, Willett WC. Dietary factors and risk of colon
cancer. Ann Med 1994; 26: 443.
25. Newcomb PA, Storer BE, Marcus PM. Cancer of the large
bowel in women in relation to alcohol consumption: a case
control study in Wisconsin (United States). Cancer Causes
Control 1993; 4 (5): 405-411.
26. Meyer F, White E. Alcohol and nutrients in relation to colon
cancer in middle-aged adults. Am J Epidemiol 1993; 138 (4):
225-236.
65
27. Potter JD, McMichael AJ. Diet and cancer of the colon and
rectum: a case control study. J Natl Cancer Inst 1986; 76 (4):
557-569.
28. Zheng W, Anderson KE, Kushi LH. A prospective cohort study
of intake of calcium, vitamin D and other micronutrients in
relation to incidence of rectal cancer among post menopausal
women. Cancer Epidemiol Biomarkers Prev 1998; 7 (3): 221-
225.
29. Givannucci E, Stampfer MJ, Colditz GA. Multivitamin use,
folate, and colon cancer in women in the Nurses’ Health Study.
Ann Intern Med 1998; 129 (7): 517-524.
30. Michels KB, Givannucci E, Joshipura KJ. Prospective study of
fruit and vegetable consumption and incidence of colon and
rectal cancers. J Natl Cancer Institute 2000; 92 (21): 1740-
1752.
31. Terry P, Giovannucci E, Michels KB. Fruit, vegetables, dietary
fiber, and risk of colorectal cancer. J Natl Cancer Institute 2001;
93 (7): 525-533.
32. Alberts DS, MartÃnez ME, Roe DJ. Lack of effect of a high-
fiber cereal supplement on the recurrence of colorectal
adenomas. Phoenix Colon Cancer Prevention Physicians’
Network. N Engl J Med 2000; 342 (16): 1156-1162.
66
33. Martin C, Connely A, Keku TO, Mountcasite SB, Galanko J,
Woosley JT. Nonsteroidal anti-inflammatory drugs, apoptosis
and colorectal adenomas. Gastroenterology 2002; 323: 140-
145.
34. Dilleo A, Messa C, Carallini A, Linsalala M. Estrogen and
colorectal cancer. Curr Drug Target Immune Endocr Metabol
Disord 2001; 1: 1-12.
35. Fernadez E, La Vecchia C, Franceschi S, Braga C, Talamini R,
Negri E. Oral contraceptive use and risk of colorectal cancer.
Epidemiology 1998 May; 9 (3): 295-300.
36. Stürmer T, Glynn RJ, Lee IM. Aspirin use and colorectal
cancer: post-trial follow-up data from the Physicians’ Health
Study. Ann Intern Med 1998; 128 (9): 713-720.
37. Grodstein F, Newcomb PA, Stampfer MJ. Postmenopausal
hormone therapy and the risk of colorectal cancer: a review and
meta-analysis. Am J Med 1999; 106 (5): 574-582.
38. Terry MB, Neugut AI, Bostick RM. Risk factors for advanced
colorectal adenomas: a pooled analysis. Cancer Epidemiol
Biomarkers Prev 2002; 11 (7): 622-629.
39. Fridenreich CM, Orenstein MR. Physical activity and cancer
prevention: etiological evidence and biological mechanisms. J
Nutr 2002; 132 (suppl): 3456-3464.
67
40. Kuper A, Boffetta P, Adami HO. Tobacco use and cancer
causation: Association by tumor type. J Intern Med 2002; 252:
206-224.
41. Chao A, Thun MJ, Jacobs EJ. Cigarette smoking and
colorectal cancer mortality in the cancer prevention study II. J
Natl Cancer Inst 2000; 92 (23): 1888-1896.
42. Terry P, Ekbom A, Lichtenstein P. Long-term tobacco smoking
and colorectal cancer in a prospective cohort study. Int J
Cancer 2001; 91 (4): 585-587.
43. White E, Jacob EJ, Daling JR. Physical activity in relation to
colon cancer in middle-aged men and women. Am J Epidemiol
1996; 144 (1): 42-50.
44. Fridenreich CM. Physical activity and cancer prevention: from
observational to intervention research. Cancer Epidemiol
Biomarkers Prev 2001; 10 (4): 287-301.
45. Harkins L, Volk AL, Samanta M, Mikolaenko, Britt WJ, Bland
KI. Specific localization of human cytomegalovirus nucleic acid
and protein in human colorectal cancer. Lancet 2002; 360:
1557-1563.
68
46. Enam S, Del Valle L, Lara C, Gan DD, Ortiz-Hidalgo C,
Palazzo JP. Association of human papilloma virus JCV with
colon cancer: evidence for interaction of viral t- antigen and
beta catenine. Cancer Res 2002; 62: 7093-7101.
47. Hartwich A, Konturek SJ, Pierzchalski P, Zuchowicz M, Labza
H, Konturek PC. Helicobacter pylori infection, gastrin,
cyclooxygenase-2 and apoptosis in colorectal cancer. nIt J
Colorectal Dis 2001; 16: 202-210.
48. Gupta K, Krishnaswamy G, Karnad A, Peiris AN. Insulin: a
novel factor in carcinogenesis. Am J Med Sci 2002; 323: 140-
145.
49. Jass JR. Pathogenesis of colorectal cancer. Surgery Cli N Am
2002; 82: 891.
50. Thomas RM, Sobin LH. Gastrointestinal cancer. Cancer 1995;
75: 154-170.
51. Jass JR, Do KA, Simms LA, Lino H, Wynter C, Pillay SP, et al.
Morphology of sporadic colorectal cancer with DNA replication
errors. Gut 1998; 42: 673-679.
52. Rashid A, Zahurak M, Goodman SN, Hamilton SR. Genetic
epidemiology of mutated K-ras proto-oncogene, altered
suppressor genes, and microsatellite instability in colorectal
adenoma. Gut 1999; 44: 823-826.
69
53. Tang WY, Elantan J, Lee YS, Goh HS, Smith DR. C-Ki_ ras
mutations in colorectal adenocarcinoma from a country with a
rapidly changing colorectal cancer incidnce. Br J Cancer 1999;
81: 237-241.
54. Hardy DJ, Kora SJ, Pass I Harvey. Carcinoma of the colon
and rectum. Hardy’s, Textbook of Surgery. 2cond eddition.
Philadelphia. J.B. Lippincott company. 1988: 609-616.
55. Trowbridge B, Burt RW. Colorectal cancer screening. Surg Clin
North Am 2002; 82: 932-943.
56. Rockey DC, Koch J, Cello JP, Sanders LL, McQuaid K.
Relative frequency of upper gastrointestinal lesions in patients
with positive fecal occult-blood tests. N Engl J Med 1998; 339:
153-159.
57. Hardcastle JD, Chamberlain JO, Robinson MH, Amar SS,
Balfour. Randomized co trial of fecal- occult-blood screening for
colorectal cancer. Lancet 1996; 348: 1472-1477.
58. Mandel JS, Bond JH, Church TR, Snover DC, Bradley GM,
Schuman LM. Reducing mortality from colorectal cancer by
screening for fecal occult blood. Minnesota Colon Cancer
Control Study. N Engl J Med 1993; 328: 1365-1371.
70
59. Read TE, Kodner IJ. Colorectal Cancer: Risk Factors and
Recommendations for Early Detection. Am Fam Phy 1999; 59
(11): cover article.
60. Read TE, Read JD, Butterly LF,. Importance of adenoma 5mm
or less in diameter that is detected by sigmoidoscopy. N Engl J
Med 1997; 336: 8-12.
61. Byers T, Levin B, Rothenberger D, Dodd GD, Smith RA.
American Cancer Society guidelines for screening and
surveillance for early detection for colorectal polyps and cancer:
update 1997. CA Cancer J Clin 1997; 47: 154-160.
62. Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Gottlieb LS,
Sternberg SS. Prevention of colorectal cancer by colonoscopic
polypectomy. N Engl J Med 1993; 329: 1977-1981.
63. Burt RW. Familial risk and colorectal cancer. Gastroenterology
Clin North Am 1996; 25: 793-803.
64. Cancer Epidemiology Services. Colorectal cancer in New
Jersey: colorectal cancer subsites. Cancer surveillance
program. New Jersey, 2001 March.
71
65. Compton CC. Updated protocol for examination of specimen
removed from patients with carcinomas of the colon & rectum,
excluding carcinoid tumors, lymphomas, sarcomas and tumors
of the veriform appendix: a basis for check lists. Arch Path Lab
Med 2000; 124: 1016-1025.
66. Jass JR, Sobin LH. Histological typing of intestinal tumors.
World Health Organization International Histological
Classification of Tumors, 2nd ed. New York: Springer-Verlag;
1989.
67. Willett CG, Compton CC. Pathology and staging. Cancer of the
lower gastrointestinal tract. Hamilton: B.C.Decker Inc; 2001.
P. 53-81.
68. Sternberg SS. Carcinoma of the Large intestine & Rectum.
Diagnostic Surgical Pathology, 3rd ed. Philadelphia: A wolters
Kluwer Company; 1999. P. 1436-1442.
69. Sacki O, Atkin WS, Jass JR. Mucinous carcinoma of the
rectum. Histopathology 1987; 11: 295-272.
70. Symonds DA, Vickery AL. Mucinous carcinoma of the colon
and rectum. Cancer 1976; 37: 1891-1900.
72
71. Sasaki S, Masaki T, Umetani N, Futakawa N, Ando H, Muto T.
Characteristics in primary signet-ring cell carcinoma of the
colorectum, from clinicopathological observations. Jap J Clin
Oncol 1998; 28: 202-206.
72. Comer TP, Beahrs OH, Dockerty MD. Primary squamous cell
carcinoma and adenocarcinoma of the colon. Cancer 1971; 28
(11): 1111-1117.
73. Jass JR, In: Fletcher CDM. Diagnostic histopathology of
tumors. New York: Churchill Livingstone; 1995. P. 243-274.
74. Jesserun J, Romero-Guadarrama M, Manivel JC. Medullary
adenocarcinoma of the colon: clinicopathologic study of11
cases. Hum Pathol 1999; 30: 843-848.
75. Tortola S, Marcuello E, Gonzalez I, Reyes G, Arriba R, Aiza G,
et al. P53 & K-ras gene mutations correlate with tumor
aggressiveness, but are not of routine prognostic value in
colorectal cancer. J Clin Oncol 1999; 17: 1375-1381.
76. Isimbaldi G, Sironi M, Assi A. Sarcomatoid carcinoma of the
colon. Report of the second case with immunohistochemical
study. Pathol Rest Pract 1996; 192: 483-487.
77. Rubio CA. Clear cell adenocarcinoma of the colon. J Clin
Pathol 1995; 48: 1142-1144.
73
78. Dukes CE. The classification of the rectum. J Pathol Bacteriol
1932; 35:322-332.
79. Astler VA, Coller FA. The prognostic significance of direct
extension of carcinoma of the colon & rectum. Ann Surg 1954;
139: 846-852.
80. Beahrs OH, Henson DE, Hulter RV. Colon and rectum: AJCC
Manual for staging of cancer, 4th ed. Philadelphia: JB Lippincott;
1992. P. 75-82.
81. Fleming ID, Cooper JS, Henson DE. AJCC manual for staging
of cancer, 5th ed. Philadelphia: PA Lippincott Raven; 1997.
82. Blenkinsopp WK, Stewart-Brown S, Blesovsky L.
Histopathology reporting in large bowel cancer. J Clin Pathol
1981; 34: 509-513.
83. Compton CC, Fieling LP, Burgart LJ. Prognostic factors in
colorectal cancer. College of American Pathologists consensus
statement. Arch Pathol Lab Med 2000; 124: 979-994.
84. Franklin ME JR, Rosenthal D, Norem RF. Prospective
evaluation of laproscopic colon resection for adenocarcinoma. A
multicenter study. Surg Endosc 1995; 9: 811-816
74
85. Iwamoto RJ. Emerging strategies in radiation therapy for
colorectal cancer: intraoperative and stereotactic radiation
therapy. Colorectal Cancer. Meniscus Educational Institute,
1998; 14-23.
86. Peters M, Haller D. Therapy for early-stage colorectal cancer.
Oncology 1999; 13: 307-315.
87. Ohno S, Tomoda M, Tomiaski S. Improved surgical results
after combining preoperative hyperthermia with chemotherapy
and radiotherapy for patients with carcinoma of the rectum. Dis
Colon Rectum 1997; 40: 401-406.
88. Pazdur RL, Coia L, Wagman L. Cancer Management: A
Multidisciplinary Approach. Colorectal and anal cancer. New
York: 1999. P. 149-175.
89. www.radiologyinfo. Colorectal cancer therapy. Radiology
informations. Radiologic society of North America (RSNA).
2005.
90. www.sgpgi.ac.in/path/seminar/ccaprog.html. Pathology seminars,
SGPGIMS: Prognostic factors in colorectal cancer. India, 1999.
91. Burt R. Update on genetic advances in colorectal cancer. Pract
Gastroenterol- 1997; 21: 9-15.
75
92. Nakamori S, Kameyama M, Imaoka S. Increased expression of
sialyl lewisx antigen correlates with poor survival in patients with
colorectal carcinomas. Clinicopathological & immunohistoch-
emical study. Cancer Res 1993; 53: 3632.
93. Steele RJ, Kelly P, Ellul B, Eremin O. Epidermal growth factor
receptor expression in colorectal cancer. Br J Surg 1990; 77:
1352.
94. Peethambaram P, Weiss M, Loprinzi CL. An evaluation of
preoperative follow-up tests in colon cancer patients treated for
cure. Oncology 1997; 54: 287-292.
95. http://www.patient.cancerConsultants.com. New Colorectal
Cancer Screening Method Approved for Human Testing. Colon
Cancer News. 2003.
96. Schottenfld D. The epidemiology of cancer: an overview.
Cancer 1981; 47: 1095-1108.
97. World Health Organization. The World Health Report 1998. Life
in the 21st century. A vision for all. Geneva: WHO; 1998.
98. Abdel-Rahman SZ, Soliman AS, Bondy ML, Omar S, El-
Badwey SA. Inheritance of the 194 Trp and the 399 Gln
variants alleles of the DNA repair gene XRCCI are associated
with increased risk of early-onset colorectal cancer in Egypt.
Cancer Lett 2000; 159: 79-86.
76
99. Abu-Zaid AA, Khfagy W, Maizoul OM, Alaa A, Mostafa I.
Colorectal cancer in Egypt. Dis Colon Rectum 2002; 45: 1255-
1260.
100. Kim DW, Bang YJ, Hro DS, Kim NK. Colorectal cancer in
Korea: characteristics and trends. Tumori 2002; 88: 262-265.
101. Ayyub MI, Al-Radi AO, Khazeindar AM, Nagi AH, Massiyar IA.
Clinicopathological trends in colorectal cancer in tertiary care
hospitals. Saudi Med J 2002; 23: 160-163.
102. Kaw LL, Puzalan CK, Crisostomo AC, Bowyer MW, Wharry
DC. Surgical patlology of colorectal cancer in Filipinos:
implications for clinical practice. J Am Coll Surg 2002; 195: 188-
195.
103. Takada H, Ohsawa T, Iwamoto S, Yoshida R, Nakaro M,
Imadokuomo. Changing site distribution in Japan. Dis Colon
Rectum 2002; 45: 1244-1254.
104. Mansour I, Zahrani IH, Abdul-aziz S. Colorectal cancer in
Saudi Arabia. Saudi Med J 2002; 23: 322-327.
105. Keswani SG, Boyle MJ, Maramll JP, Mains L, Wilk SM, Hunt
JP. Colorectal cancer in patients younger than 40 years of age.
Am Surg 2002; 68: 871-876.
77
106. Holowaty EJ, Marrett CD, Parkes R, Fehringer G. Colorectal
cancer in Ontario 1971-1996: subsites and morphology.
Surveillance unit, division of preventive oncology, Ontario
(Canada): Cancer Care Ontario; 1998.
107. Basaleem HO, Al-Sakkaf KA. Colorectal cancer among Yemeni
patients: characteristics and trends. Saudi Med J 2004; 25(8):
1002-1005.
78
بسم اهللا الرحمن الرحيم
University of Khartoum The Graduate College
Medical & Health Studies Board Questionnaire
Colorectal cancer
• Lab. No.:.................... 1- Name:........................................................ 2- Age (in years):........................................................ 3- Sex: 1- Male 2- Female
4- Tribe: ..……………………………………..…..........
5- Residence: ………………………………………..
6- Clinical remarks: 1- Rectal bleeding. 2- Diarrhoea. 3- Constipation
4- Fatigability 5- Abdominal pain 6- Weight loss
7- Others: ……………………………………………….
7- Diagnosed by: a. Endoscopy and biopsy: 1- Yes 2- No
Type: ……………………… ………………………….
a. Surgical: 1- Yes 2- No
Type: ……………………… ……………………….
9- Histopathology: Gross: ……………………………………………..
Microscopy: …………………………………………
Diagnosis: ……………………………………………
Stage and grade: ……………………………………
10. Other investigations: - C.B.C: ………………………………….…………………
- Barium enema: ……………………………………………
- U/S: ………………………………………………..………
- C. T scan: …………………………………………………




















![Bowel Elimination Si.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../kdm_slide_bowel_elimination.pdfPrimary organ of bowel elimination ... Small bowel series Barium enema. ... Sigmoid](https://img.pdfslide.us/doc/110x75/5adf17e77f8b9ac0428bbfc8/bowel-elimination-sippt-read-only-ocwusuacidocwusuacidkdmslidebowel.jpg)