Embed Size (px)
Citation preview
University of Groningen
Soft tissue sarcoma at the turn of the millenniumNijhuis, Paulus Henricus Antonius
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2001
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Nijhuis, P. H. A. (2001). Soft tissue sarcoma at the turn of the millennium: aspects of epidemiology,cytogenetics, diagnosis and treatment s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 03-12-2018

9
Chapter 1
Introduction and aim of the thesis
10 Introduction and aim of the thesis Chapter 1
Introduction
Soft tissue sarcomas (STS) can be defined as malignant tumors arising from the non-epithelial extra-skeletal tissue of the body, exclusive of the reticulo-endothelial systemand glia. Embryologically, these tumors are derived principally from mesoderm, exceptsome, which derive from the neuroectoderm [1]. The pathogenesis of most STS remainsunknown. Genetic factors (neurofibromatosis I and II, retinoblastoma, Li-Fraumeni syn-drome, Gardner�s syndrome), environmental factors (exposure to environmental car-cinogens as dioxin and some herbicides, and trauma, injury or ionizing radiation in thepast), and immunological factors (immunosuppression after transplant surgery) havebeen identified as etiological factors in STS development [1-11]. As in most other malig-nancies, it is very unlikely that only one of these various factors is causing the disease;a multifactorial etiology seems obvious.
STS are rare tumors, accounting for approximately 1% of all malignant tumors diag-nosed annually (8100 patients in the United States and 422 in the Netherlands) [12,13].There is a slight male preponderance and the incidence is increasing with age [14,15,16].As prognosis varies between the different histological types and even between subtypes,an adequate histopathological classification is crucial. The most recent classification ofsoft tissue tumors is the World Health Organization histological classification (1994),dividing these tumors into 15 categories [17].
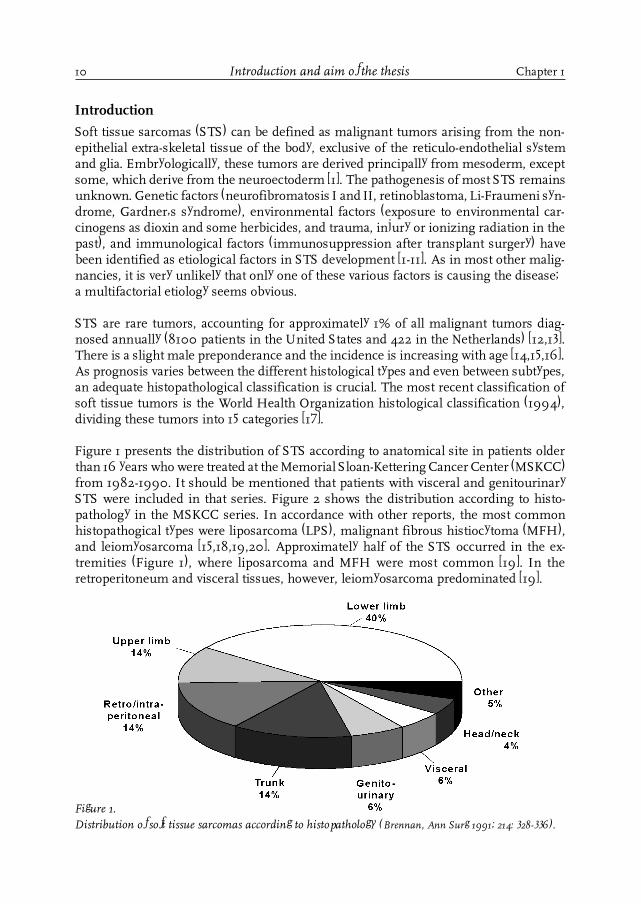
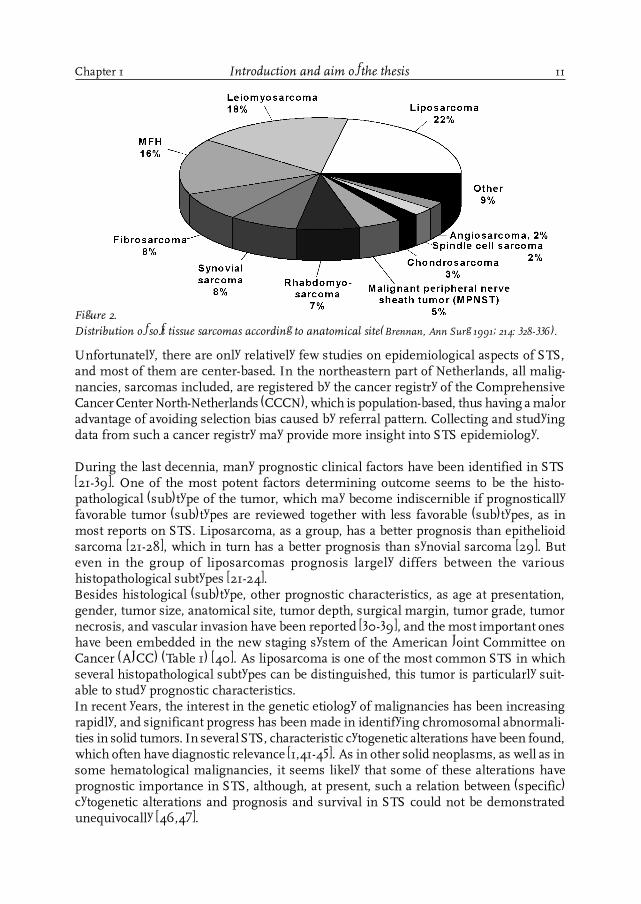
Figure 1 presents the distribution of STS according to anatomical site in patients olderthan 16 years who were treated at the Memorial Sloan-Kettering Cancer Center (MSKCC)from 1982-1990. It should be mentioned that patients with visceral and genitourinarySTS were included in that series. Figure 2 shows the distribution according to histo-pathology in the MSKCC series. In accordance with other reports, the most commonhistopathogical types were liposarcoma (LPS), malignant fibrous histiocytoma (MFH),and leiomyosarcoma [15,18,19,20]. Approximately half of the STS occurred in the ex-tremities (Figure 1), where liposarcoma and MFH were most common [19]. In theretroperitoneum and visceral tissues, however, leiomyosarcoma predominated [19].
Figure 1.Distribution of soft tissue sarcomas according to histopathology (Brennan, Ann Surg 1991; 214: 328-336).
11
Unfortunately, there are only relatively few studies on epidemiological aspects of STS,and most of them are center-based. In the northeastern part of Netherlands, all malig-nancies, sarcomas included, are registered by the cancer registry of the ComprehensiveCancer Center North-Netherlands (CCCN), which is population-based, thus having a majoradvantage of avoiding selection bias caused by referral pattern. Collecting and studyingdata from such a cancer registry may provide more insight into STS epidemiology.
During the last decennia, many prognostic clinical factors have been identified in STS[21-39]. One of the most potent factors determining outcome seems to be the histo-pathological (sub)type of the tumor, which may become indiscernible if prognosticallyfavorable tumor (sub)types are reviewed together with less favorable (sub)types, as inmost reports on STS. Liposarcoma, as a group, has a better prognosis than epithelioidsarcoma [21-28], which in turn has a better prognosis than synovial sarcoma [29]. Buteven in the group of liposarcomas prognosis largely differs between the varioushistopathological subtypes [21-24].Besides histological (sub)type, other prognostic characteristics, as age at presentation,gender, tumor size, anatomical site, tumor depth, surgical margin, tumor grade, tumornecrosis, and vascular invasion have been reported [30-39], and the most important oneshave been embedded in the new staging system of the American Joint Committee onCancer (AJCC) (Table 1) [40]. As liposarcoma is one of the most common STS in whichseveral histopathological subtypes can be distinguished, this tumor is particularly suit-able to study prognostic characteristics.In recent years, the interest in the genetic etiology of malignancies has been increasingrapidly, and significant progress has been made in identifying chromosomal abnormali-ties in solid tumors. In several STS, characteristic cytogenetic alterations have been found,which often have diagnostic relevance [1,41-45]. As in other solid neoplasms, as well as insome hematological malignancies, it seems likely that some of these alterations haveprognostic importance in STS, although, at present, such a relation between (specific)cytogenetic alterations and prognosis and survival in STS could not be demonstratedunequivocally [46,47].
Figure 2.Distribution of soft tissue sarcomas according to anatomical site(Brennan, Ann Surg 1991; 214: 328-336).
Chapter 1 Introduction and aim of the thesis
12
Advances in technology have resulted in an important progress in diagnostic tools inSTS. The introduction of the computer tomography scan (CT-scan) caused a major break-through in radiodiagnostics because, for the first time, it was possible to visualize thesoft tissues directly using X-rays [48]. Notwithstanding its possibilities, this techniquealso had its shortcomings (the use of X-rays, direct images limited to only two plains,only information on anatomy and not on metabolism). The development of the mag-netic resonance imaging (MRI) and the currently available spiral CT-scan overcame thefirst two shortcomings of the CT-scan [49,50], but still could not cope with the third one.The positron emission tomography scan (PET-scan) and the single photon emission to-mography (SPECT) made it possible to study the metabolism of tumors [51,52].As with all new technology-driven instruments, these challenging techniques can easilybe used inappropriately, resulting in significant health-care costs [53]. Therefore, thedevelopment of specific diagnostic guidelines is important, especially in rare tumors, asclinical and histopathological presentation widely varies, the experience in individualhospitals is limited, and treatment often is very complex, including many modalities.
In February 1983, a cooperative group for rare tumors, consisting of specialists in surgi-cal oncology, medical oncology, radiotherapeutic oncology and pathology from varioushospitals in the CCCN-region, recognized this problem and developed regional guide-
Introduction and aim of the thesis Chapter 1
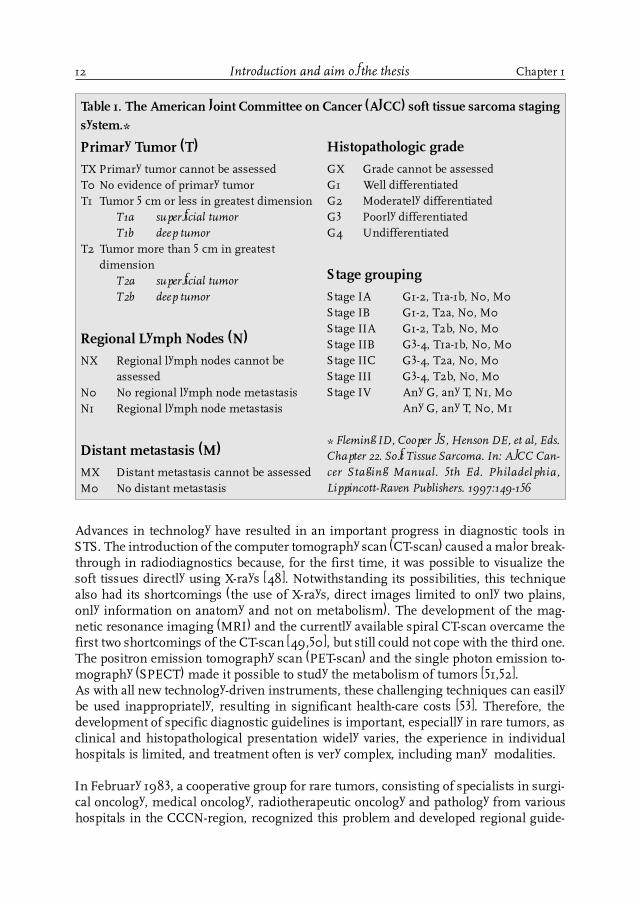
Table 1. The American Joint Committee on Cancer (AJCC) soft tissue sarcoma stagingsystem.*
Primary Tumor (T)
TX Primary tumor cannot be assessedT0 No evidence of primary tumorT1 Tumor 5 cm or less in greatest dimension
T1a superficial tumorT1b deep tumor
T2 Tumor more than 5 cm in greatestdimension
T2a superficial tumorT2b deep tumor
Regional Lymph Nodes (N)
NX Regional lymph nodes cannot beassessed
N0 No regional lymph node metastasisN1 Regional lymph node metastasis
Distant metastasis (M)
MX Distant metastasis cannot be assessedM0 No distant metastasis
Histopathologic grade
GX Grade cannot be assessedG1 Well differentiatedG2 Moderately differentiatedG3 Poorly differentiatedG4 Undifferentiated
Stage grouping
Stage IA G1-2, T1a-1b, N0, M0Stage IB G1-2, T2a, N0, M0Stage IIA G1-2, T2b, N0, M0Stage IIB G3-4, T1a-1b, N0, M0Stage IIC G3-4, T2a, N0, M0Stage III G3-4, T2b, N0, M0Stage IV Any G, any T, N1, M0
Any G, any T, N0, M1
* Fleming ID, Cooper JS, Henson DE, et al, Eds.Chapter 22. Soft Tissue Sarcoma. In: AJCC Can-cer Staging Manual. 5th Ed. Philadelphia,Lippincott-Raven Publishers. 1997:149-156
13
lines for the diagnosis and treatment of soft tissue tumors [54]. A few years later, theDutch Sarcoma Group initiated national guidelines for STS diagnosis and treatment[55]. Although compliance with such guidelines is important for various reasons (e.g.appropriateness of practice, health-care savings, and better outcome and survival [53,56-58]), and despite an increase in medical practice guideline development and dissemina-tion, compliance with such guidelines has often been surprisingly low. In malignantdisorders, reports on the adherence to such guidelines are very limited, whereas in softtissue tumors, nothing has been published on this item. Nevertheless, such informationseems very valuable for future guideline development and introduction.
Treatment of STS has changed dramatically during the second half of the last century.Prior to the 1950s and 1960s, most surgeons dealing with STS performed local resec-tions or shell-out procedures, which were associated with an unacceptable high localrecurrence rate of 60-95% [59-63]. In the same period, Bowden and Booher reportedlimb-saving techniques with a low local recurrence risk [64]. In the same year, 1958, thegroup of Stener published the same surgical principles and results [65,66]. Both groupsmight be considered true pioneers in modern STS treatment, because both recognizedthe infiltrative manner of sarcoma growth, explaining the high local recurrence rate aftershell-out procedures. Later, this high local recurrence rate was further explained byEnneking�s theory of sarcoma tumor growth pattern [67]. STS grow in a centrifugal fash-ion, resulting in the formation of an edematous pseudocapsule of compressed, normaltissue and a reactive zone of proliferating mesenchymal cells and neovascularization.Further tumor growth causes a continuous extent of microscopic tumor pseudopodsinto this pseudocapsule, where they form microscopic and macroscopic nodules (satel-lites). Especially in high-grade lesions, such satellites can also be found in surrounding�normal� tissue, far beyond the pseudocapsule (skip metastases). In extremities, wheremost of the STS are located, the tumor extends longitudinally, within the compartment,bounded by fibrous barriers (muscle fascia and aponeurosis, deep fascia and intermus-cular septae). Crossing these barriers is a late phenomenon, and is associated with high-grade lesions [67,68].
Based on these new insights, en-block resections of the entire compartment containingthe tumor or amputations were recommended, resulting not only in a drop of local re-currence rate to 5-30%, but also in a high amputation rate of 40-50% [60,61,68-70].Although these so-called �compartment resections� were widely adopted, the division ofsurgical oncology of the Groningen University Hospital performed only wide local resec-tions followed by external beam radiotherapy (EBRT) or amputation of the affected limb.
Modern STS management started at the end of the seventies and the beginning of theeighties. Suit and Lindberg were the first to demonstrate the importance of adjuvantradiotherapy in STS therapy [71,72]. Their results formed the basis of the famous Na-tional Cancer Institute (NCI) trial by Steven Rosenberg et al., a study that became one ofthe cornerstones in today�s state of the art STS treatment [70]. For the first time, a pro-spective randomized study showed that adequately performed local resection followedby high dose radiotherapy formed a reliable limb-saving treatment, comparable to am-putation with regard to local recurrence, disease-free and overall survival rates.
Chapter 1 Introduction and aim of the thesis
14
Unfortunately, the optimal treatment for locally advanced extremity sarcomas remainedan unsolved problem. One of the most promising approaches at that time was a multi-modality therapy, consisting of preoperative (intraarterial) chemotherapy, immediatelyfollowed by EBRT, and surgical resection. This technique was initiated by Morton andEilber [73], and later further developed by Eilber and co-workers at the UCLA School ofMedicine [74,75]. The sequence of the various therapies was based on the premise thatpreoperative treatment of micrometastases at the periphery of the tumor with intact bloodsupply would enable the surgeon to perform a local surgical procedure. In three sequentialtrials, Eilber et al. showed a high limb salvage rate of 95%, with a low local recurrencerate of approximately 10% [75]. In the early eighties, this treatment strategy was adoptedby the Groningen Sarcoma Working Party, which added postoperative EBRT to thetreatment protocol in case of a marginal resection or involvement of the surgical margin[76]. The multimodality treatment, as initiated by Morton and Eilber, has been associatedwith a substantial short-term morbidity, especially wound complications [75]. Althoughthere has been a growing awareness of potential long-term side-effects of intensified(multimodality) cancer treatment protocols, only very few reports have dealt with thelong-term complications and functional outcome after this intensive STS treatment [75,77-79].
Another way to decrease the number of amputations in locally advanced extremity STShas been hyperthermic isolated limb perfusion (HILP) with cytostatics agents. Severaldrugs have been used (melphalan, the standard drug for HILP in melanoma, doxorubicin,cisplatinum, and other agents), without improvement of local control or disease-freesurvival when compared to the other therapies, as intravenous or intraarterial adriamycinin combination with neoadjuvant radiotherapy followed by local resection [75,80-83].It was not until the early nineties, that significant progress was made by the addition oftumor necrosis factor-alpha (TNF-α) to melphalan in HILP for locally advanced extrem-ity STS [84]. This resulted in a high response rate and high limb salvage rates with anacceptable toxicity level [85]. In the early nineties, the Groningen Sarcoma Working Partychanged the treatment of locally advanced extremity STS in HILP with TNF-α, melphalan,with or without interferon-gamma (IFN-γ), with good results [85]. In 1998, this sarcomagroup published the results of a study on adjuvant EBRT (60-70 Gy) after HILP withmelphalan, TNF-α, and IFN-γ and delayed tumor resection of locally advanced extremitySTS with histopathological viable tumor after resection [86]. It was demonstrated thatthis was feasible and that the addition of EBRT increased local tumor control withoutincreasing treatment morbidity. Recently, Ham et al. highlighted several aspects of mod-ern surgical sarcoma treatment at the Groningen University Hospital [87].
Since the mid eighties, the cancer registry of the CCCN has registered all STS in theCCCN-region, and the Groningen Sarcoma Working Party discusses all sarcomas re-ferred to the Groningen University Hospital. In recent years, many aspects of these tumorshave been studied and reported by this sarcoma group, resulting in several theses [88-90]. Still a variety of questions remain unanswered. The goal of the present thesis is toget more insight into several aspects of this uncommon malignancy.
Introduction and aim of the thesis Chapter 1
15
References1. Enzinger FM, Weiss SW. General considerations. In: Enzinger FM, Weiss SW (Eds). Soft tissue tumors.
Third edition. St. Louis, Mosby, 1995: 1-16.2. Wiklund TA, Blomqvist CP, Raty J, et al. Postirradiation sarcoma: analysis of nationwide cancer registry
material. Cancer 1991; 68: 524-531.3. Mark RJ, Poen J,Tran LM, Fu YS, Selch MT, Parker RG. Postirradiation sarcoma: a single institution study and
a review of the literature. Cancer 1994; 73: 2653-2662.4. Zahm SH, Fraumeni JF, Jr. The epidemiology of soft tissue sarcoma. Semin Oncol 1997; 24: 504-514.5. Hardell L, Eriksson M. The association between soft tissue sarcomas and exposure to phenoxyacetic acids: A new
case-referent study. Cancer 1988; 62: 652-656.6. Kang H, Enzinger FM, Breslin P, et al. Soft tissue sarcoma and military service in Vietnam: a case-control
study. J Natl Cancer Inst 1987; 79: 693-699.7. Fingerhut MA, Halperin WE, Marlow DA, et al. Cancer mortality in workers exposed to 2,3,7,
8-tetrachlorodibenzo-p-dioxin. N Eng J Med 1991; 324: 212-218.8. Saracci R, Kogevinas M, Bertazzi PA, et al. Cancer mortality in workers exposed to chlorophenoxy herbicides
and chlorophenols. Lancet 1991; 338: 1027-1032.9. Eriksson M, Hardell L, Adami HO. Exposure to dioxins as a risk factor for soft tissue sarcoma: a population-
based case-control study. J Natl Cancer Inst 1990; 82: 486-490.10. McClay EF. Epidemiology of bone and soft tissue sarcomas. Semin Oncol 1989; 16: 264-272.11. Malkin D, Li F, Strong L, et al. Germ line P53 mutations in a familial syndrome of breast cancer, sarcomas, and
other neoplasms. Science 1990; 250: 1233-1238.12. Greenlee RT, Murray T, Bolden S, Wingo PA. Cancer statistics, 2000. CaCancer J Clin 2000; 50: 7-33.13. Incidence of cancer in the Netherlands 1996. Visser O, Coebergh JWW, Schouten LJ, Dijck JAAM (Eds). Utrecht,
Vereniging van Integrale Kankercentra 2000.14. Gustafson P. Soft tissue sarcoma. Epidemiology and prognosis in 508 patients. Acta Orthop Scand 1994,
65 (suppl 259), 1- 31.15. Harris M, Hartley AL, Blair V, et al. Sarcomas in North West England. I. Histopathological peer review.
Br J Cancer 1991, 64, 315-320.16. Jane MJ, Hughes PJ. Disease incidence and results of extremity lesion treatment: Mersey Region soft tissue
sarcomas (1975-1985). Sarcoma 1998, 2, 89-96.17. Weiss SW. Histopathological typing of soft-tissue tumors, second edition. (WHO international histopathological
classification of tumors). Berlin, Springer Verlag, 1994.18. Torosian MH, Friedrich C, Godbold J, Hajdu SI, Brennan F. Soft-tissue sarcoma: Initial characteristics and
prognostic factors in patients with and without metastatic disease. Sem Surg Oncol 1988, 4, 13-19.
Chapter 1 Introduction and aim of the thesis
Aim of the thesis
1. To provide more insight into epidemiological aspects of STS, based on a population-basedsurvey.
2. To study the impact of the histopathological heterogeneity on prognosis in one of the mostcommon STS, liposarcoma.
3. To evaluate the necessity of long-term follow-up, especially in case of intensive, multimodalitytreatment protocols, in order to determine long-term effects, which might interfere with theprimary goal of such therapies.
4. To investigate the adherence to (diagnostic) STS guidelines, and to evaluate the role ofcentralization in the diagnostic management of these rare tumors.
5. To look into the (near) future of STS treatment, and to evaluate the prognostic importanceof cytogenetic changes in these tumors.
16
19. Brennan MF, Casper ES, Harrison LB, et al. The role of multimodality therapy in soft-tissue sarcoma. Ann Surg1991; 214: 328-336.
20. Pollock RE, Karnell LH, Menck HR, Winchester DP. The National Cancer Data Base Report on soft tissuesarcoma. Cancer 1996, 78, 2247-2257.
21. Chang HR, Hajdu SI, Collin C, Brennan MF. The prognostic value of histologic subtypes in primary extremityliposarcoma. Cancer 1989; 64: 1514-1520.
22. Chang HR, Gaynor J, Tan C, Hajdu SI, Brennan MF. Multifactorial analysis of survival in primary extremityliposarcoma. World J Surg. 1990; 14: 610-618.
23. Zagars GK, Goswitz MS, Pollack A. Liposarcoma: outcome and prognostic factors following conservationsurgery and radiation therapy. Int J Rad Oncol Biol Phys 1996; 36: 311-319.
24. Pearlstone DB, Pisters PWT, Bold RJ, et al. Patterns of recurrence in extremity liposarcoma. Implications forstaging and follow-up. Cancer 1999; 85: 85-92.
25. Linehan DC, Lewis JJ, Leung D, Brennan MF. Influence of biologic factors and anatomic site in completelyresected liposarcoma. J Clin Oncol 2000; 18:1637-1643.
26. Enzinger FM, Weiss SW. Synovial sarcoma. In: Enzinger FM, Weiss SW (Eds). Soft tissue tumors. Thirdedition. St. Louis, Mosby, 1995: 757-785.
27. Heide HJL van der, Veth RPH, Pruszczynski M, Wobbes T, Hoesel QGCM van, Lemmens JAM. Synovialsarcoma: oncological and functional results. Eur J Surg Oncol 1998; 24: 114-119.
28. Lewis JJ, Antonescu CR, Leung DHY, Blumberg D, Healey JH, Woodruff JM, Brennan MF. Synovial sarcoma:A multivariate analysis of prognostic factors in 112 patients with primary localized tumors of the extremity.J Clin Oncol 2000; 18: 2087-2094.
29. Spillane AJ, Thomas JM, Fisher C. Epithelioid sarcoma: the clinicopathological complexities of this rare softtissue sarcoma. Ann Surg Oncol 2000; 7: 218-225.
30. Markhede G, Angervall L, Stener B. A multivariate analysis of the prognosis after treatment of soft-tissue tumors.Cancer 1982; 49: 1721-1733.
31. Reitan JB, Kaalhus O, Brennhovd IO, Sager EM, Stenwig AE, Talle K. Prognostic factors in liposarcoma.Cancer 1985; 55:2482-2490.
32. Potter DA, Kinsella T, Glatstein E, et al. High-grade soft tissue sarcomas of the extremities. Cancer 1986;58: 190-205.
33. Lawrence W Jr., Donegan WL, Natarajan N, Mettlin C, Beart R, Winchester D. Adult soft tissue sarcomas. AnnSurg 1987; 205: 349-359.
34. Singer S, Corson JM, Gonin R, Labow B, Eberlein TJ. Prognostic factors predictive of survival and localrecurrence for extremity soft tissue sarcoma. Ann Surg 1994; 219: 165-173.
35. Coindre JM, Terrier P, Bui N, et al. Prognostic factors in adult patients with locally controlled soft tissuesarcoma: A study of 546 patients from the French Federation of Cancer Centers Sarcoma Group. J Clin Oncol1996; 14: 869-877.
36. Heslin MJ, Woodruff J, Brennan MF. Prognostic significance of a positive microscopic margin in high-riskextremity soft tissue sarcoma: Implications for management. J Clin Oncol 1996; 14: 473-478.
37. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF. Analysis of prognostic factors in 1.041 patients withlocalized soft tissue sarcomas of the extremities. J Clin Oncol 1996; 14: 1679-1689.
38. Rydholm A. Prognostic factors in soft tissue sarcoma. Acta Orthop Scand 1997; 68 [suppl 273]: 148-155.39. Brooks AD, Heslin MJ, Leung DH, Lewis JJ, Brennan MF. Superficial extremity soft tissue sarcoma: an
analysis of prognostic factors. Ann Surg Oncol 1998; 5: 41-47.40. Fleming ID, Cooper JS, Henson DE, et al, Eds. Chapter 22. Soft Tissue Sarcoma. In: AJCC Cancer Staging
Manual. 5th Ed. Philadelphia, Lippincott-Raven Publishers. 1997:149-156.41. Molenaar WM, De Jong B, Buist J, Idenburg VJS, Seruca R, Vos AM, Hoekstra HJ. Chromosomal analysis and
the classification of soft tissue sarcomas. Lab. Invest 1989; 60: 266-274.42. Fletcher JA, Kozakewich HP, Hoffer FA, Lage JM, Weidner N, Tepper R, Pinkus GS, Morton CC, Corson JM.
Diagnostic relevance of clonal cytogenetic aberrations in malignant soft-tissue tumors. N Engl J Med 1991;324: 436-442.
43. Sreekantaiah C, Ladanyi M, Rodriguez E, Chaganti RSK. Chromosomal aberrations in soft tissue tumors:Relevance to diagnosis, classification, and molecular mechanisms. Am J Pathol 1994; 144: 1121-1134.
44. Fletcher CDM, Akerman M, Dal Cin P, et al. Correlation between clinicopathological features and karyotype inlipomatous tumors. A report of 178 cases from the Chromosomes and Morphology (CHAMP) CollaborativeStudy Group. Am J Pathol 1996; 148: 623-630.
Introduction and aim of the thesis Chapter 1
17
45. Plaat BEC, Hollema H, Molenaar WM, et al. Soft tissue leiomyosarcomas and malignant gastrointestinalstromal tumors: differences in clinical outcome and expression of multidrug resistance proteins. J Clin Oncol2000; 18: 3211-3220.
46. Choong PF, Mandahl N, Mertens F, et al. 19p+ marker chromosome correlates with relapse in malignant fibroushistiocytoma. Genes Chromosom Cancer 1996; 16: 88-93.
47. Plaat BEC, Muntinghe FLH, Molenaar WM, et al. Clinical outcome of patients with previously untreated softtissue sarcomas in relation to tumor grade, DNA ploidy and karyotype. Int J Cancer 1997; 74: 396-402.
48. Hounsfield GN. Computerized transverse axial scanning (tomography): Part I. Description of system. Br JRadiol 1973; 46: 1016-1022.
49. Budinger TF, Lauterbur PC. Nuclear Magnetic Resonance technology for medical studies. Science 1984;226: 288-298.
50. Hogeboom WR, Hoekstra HJ, Mooyaart EL, Freling NJ, Schraffordt Koops H. MRI and CT in the preoperativeevaluation of soft tissue tumors. Arch Orthop Trauma Surg 1991; 110: 162-164.
51. Kole AC, Nieweg OE, Ginkel RJ van, et al. PET with L-[1-Carbon-11]-tyrosine for the visualization of tumors andmeasurement of the protein synthesis rate. J Nucl Med 1997; 38: 191-195.
52. Kole AC, Nieweg OE, Ginkel RJ van, et al. Detection of local recurrence of soft tissue sarcoma with positronemission tomography using 18F-fluorodeoxy-glucose. Ann Surg Oncol 1997; 4: 57-63.
53. Walsh GL, Winn RJ. Baseline institutional compliance with NCCN guidelines: non-small-cell lung cancer. Oncology (Huntingt) 1997; 11: 161-170.
54. Richtlijnen voor diagnostiek en behandeling van premaligne en maligne aandoeningen in de IKN-regio 1992. R.Otter (Ed). Medische Advies Raad IKN. ISBN 90-74114-03-2. 394-399.
55. Geel AN van, Unnik JAM van, Keus RB. Diagnosis and treatment of soft tissue tumours: the Dutch nationwide-accepted consensus. Sarcoma 1998; 2: 183-191.
56. Grimshaw JM, Russell IT. Effect of clinical guidelines on medical practice: a systematic review of rigorousevaluations. Lancet 1993; 342: 1317-1322.
57. Wolfe CDA, Tilling K, Bourne HM, Raju KS. Variations in the screening history and appropriateness ofmanagement of cervical cancer in south east England. Eur J Cancer 1996; 32A: 1198-1204.
58. Tilling K, Wolfe CDA, Raju KS. Variations in the management and survival of women with endometrial cancerin south east England. Eur J Gynaec Oncol 1998; 19: 64-68.
59. Cantin J, McNeer GP, Chu FC, Booker RJ. The problem of local recurrence after treatment of soft tissuesarcoma. Ann Surg 1968; 168: 47-53.
60. Shiu MH, Castro EB, Hajdu SI, Fortner JC. Surgical treatment of 297 soft tissue sarcomas of the lowerextremity. Ann Surg 1975; 182: 597-602.
61. Simon MA, Enneking WF. The management of soft-tissue sarcomas of the extremities. J Bone Joint Surg1976; 58A: 317-327.
62. Abbas JS, Holyoko ED, Moore R, Karakousis CP. The surgical treatment and outcome of soft tissuesarcoma. Arch Surg 1981; 116: 765-769.
63. Markhede G, Angervall L, Stener B. A multivariate analysis of the prognosis after surgical treatment ofmalignant soft tissue tumors. Cancer 1982; 49: 1721-1733.
64. Bowden L, Booher RJ. The principles and technique of resection of soft parts for sarcoma. Surgery 1958; 44:963-977.
65. Stener B, Stener I. Malignant tumors of the soft tissues of the thigh. Acta Chir Scand 1958; 115: 457-475.66. Berlin Ö, Stener B, Angervall L, Kindblom LG, Markhede G, Oden A. Surgery for soft tissue sarcoma in the
extremities. A multivariate analysis of the 6-26-years prognosis in 137 patients. Acta Orthop Scand 1990;61: 475-486.
67. Enneking WF, Spanier SS, Malawer MM. The effect of the anatomic setting on the results of surgical proceduresfor soft parts sarcoma of the thigh. Cancer 1981; 47: 1005-1022.
68. Rydholm A. Surgical margins for soft tissue sarcomas. Acta Orthop Scand (suppl 273) 1997; 68: 81-85.69. Eilber FR, Mirra JJ, Grant TT, Weisenburger T, Morton DL. Is amputation necessary for sarcomas?
A seven-years experience with limb-salvage. Ann Surg 1980; 192: 431-437.70. Rosenberg SA, Tepper J, Glatstein E, et al. The treatment of soft tissue sarcomas of the extremities.
Prospective randomized evaluation of (1) limb-sparing surgery plus radiation therapy compared withamputation, and (2) the role of adjuvant chemotherapy. Ann Surg 1982; 96: 305-315.
71. Suit HD, Russell WO, Martin RG. Sarcoma of soft tissue: clinical and histopathologic parameters and responseto treatment. Cancer 1975; 35: 1478-1483.
Chapter 1 Introduction and aim of the thesis
18
72. Lindberg RD, Martin RG, Romsdahl MM. Surgery and postoperative radiotherapy in the treatment of soft tissuesarcomas in adults. Ther Nucl Med 1975; 123: 123-129.
73. Morton DL, Eilber FR, Townsend CM, Grant TT, Mirra J, Weisenburger TH. Limb salvage from amultidisciplinary treatment approach for skeletal and soft tissue sarcomas of the extremity. Ann Surg 1976;184: 268-278.
74. Eilber FR, Giuliano AE, Huth JF, et al. A randomized prospective trial using postoperative adjuvantchemotherapy (Adriamycin) in high grade extremity soft tissue sarcoma. Ann J Clin Oncol 1988; 11: 39-45.
75. Eilber FR, Eckhardt JJ, Rosen G, Fu YS, Seeger LL, Selch MT. Neoadjuvant chemotherapy and radiotherapy inthe multidisciplinary management of soft tissue sarcomas of the extremity. Surg Oncol Clin N Am 1993; 2:611-620.
76. Hoekstra HJ, Schraffordt Koops H, Molenaar WM, Mehta DM, Sleijfer DTh, Dijkhuis G, Oldhoff J.A combination of intraarterial chemotherapy, preoperative and postoperative radiotherapy, and surgery aslimb-salving treatment of primarily unresectable high-grade soft tissue sarcomas of the extremities. Cancer1989; 63: 59-62.
77. Jentzsch K, Binder H, Cramer H, et al. Leg function after radiotherapy for Ewing�s sarcoma. Cancer 1981; 47:1267-1278.
78. Brown AP, Fixen JA, Plowman PN. Local control of Ewing�s sarcoma: An analysis of 67 patients. Br J Radiol1987; 60: 261-268.
79. Stinson SF, DeLaney TF, Greenberg J, et al. Acute and long-term effects on limb function of combinedmodality limb-sparing therapy for extremity soft tissue sarcoma. Int J Radiat Oncol Biol Phys 1991; 21:1492-1499.
80. Krementz ET, Carter RD, Sutherland CM, Hutton I. Chemotherapy of sarcomas of the limbs by regional perfusion.Ann Surg 1977; 185: 555-564.
81. Hoekstra HJ, Schraffordt Koops H, Molenaar WM, Oldhoff J. Results of isolated regional perfusion in thetreatment of malignant soft tissue tumours of the extremities. Cancer 1987; 60: 1703-1707.
82. Klaase JM, Kroon BBR, Benckhuijsen C, Van Geel AN, Albus-Lutter ChE, Wieberdink J. Results of regionalisolated perfusion with cytostatics in patients with soft tissue tumors of the extremities. Cancer 1989; 64: 616-621.
83. Ginkel RJ van, Schraffordt Koops H, Vries EGE de, Molenaar WM, Uges DR, Hoekstra HJ. Hyperthermicisolated limb perfusion with cisplatin in four patients with sarcomas of soft tissue and bone. Eur J Surg 1996; 22:528-531.
84. Lienard D, Delmotte JJ, Renard N, Ewalenko P, Lejeune FJ. High-dose recombinant tumour necrosis factor-alpha in combination with interferon gamma and melphalan in isolation perfusion of the limbs for melanomaand sarcoma. J Clin Oncol 1992; 10: 52-60.
85. Eggermont AMM, Schraffordt Koops H, Lienard D, Kroon BBR, Van Geel AN, Hoekstra HJ, Lejeune FJ.Isolated limb perfusion with high dose tumor necrosis factor-a in combination with interferon-? and melphalanfor nonresectable extremity soft tissue sarcomas: a multicenter trial. J Clin Oncol 1996; 14: 2653-2665.
86. Olieman AFT, Pras E, Ginkel RJ van, Molenaar WM, Schraffordt Koops H, Hoekstra HJ. Feasibility andefficacy of external beam radiotherapy after hyperthermic isolated limb perfusion with TNF-α and melphalanfor limb-saving treatment in locally advanced extremity soft-tissue sarcoma. Int J Rad Oncol Biol Phys1998; 40: 807-814.
87. Ham SJ, Graaf WTA van der, Pras E, Molenaar WM, Berg E van den, Hoekstra HJ. Soft tissue sarcomasof the extremities. A multi-modality diagnostic and therapeutic approach. Cancer Treatment Reviews 1998,24, 373-391.
88. Olieman AFT. Hyperthermic isolated limb perfusion: aspects of morbidity and efficacy. Thesis UniversityGroningen, The Netherlands, Enschede, ISBN 90-367-0986-5.
89. Ham SJ. Current concepts and surgical aspects of extremity bone and soft tissue sarcoma. Thesis UniversityGroningen, The Netherlands, Wageningen, ISBN 90-367-1069-3.
90. Plaat BEC. Soft tissue sarcomas: histopathology and cytogenetics in relation to diagnosis, treatment and clinicaloutcome. Thesis University Groningen, The Netherlands, Enschede, ISBN 90-367-1165-7; 1: 41-54.
Introduction and aim of the thesis Chapter 1