Embed Size (px)
Citation preview

CalciphylaxieCalciphylaxie
Klinik für Kardiologie und Intensivmedizin
Vincent Brandenburg
University Hospital RWTH Aachen, GermanyNephrologist
Dpt of Cardiology
Weimar, Dezember 2014

Calciphylaxis (CUA)- rare (Orpha.net # ORPHA280062),
- life-threatening syndrome,
- media calcifications of cutaneous vessels (~100µm),
- progressive, very painful lesions / ulcerations,
- reduced quality of life, high mortality,
Definition Calciphylaxie –Calcific Uremic Arteriolopathy, CUA

Medial calcification and intimal thickeningMedial calcification and intimal thickening


www.calciphylaxie.de

Calciphylaxis registry – acknowledgment

The German Calciphylaxis Registrywww.calciphylaxie.de
Baseline questions via online questionnaire:
- patient data (age, sex, cv disease, kidney disease, PTex…) 15
- lab data (creatinine, phos., calc., PTH, CRP, Hb, albumin…) 12
- dialysis modality 9
- medications (renal, cv) 24
- clinical data about CUA 6+ free text
66 items

Underlying renal disease; n = 211
Type of Kidney Disease
75%
4% 2%1%
11%
7% HDPDCKD without DialysisTransplantNo CKDn. a.
ASN Renal Week Atlanta 2014

Male / female ratio
ASN Renal Week Atlanta 2014

Total serum calcium [mmol/L] at time of registration
ASN Renal Week Atlanta 2014
> 2,4 mmol/L< 2,1 mmol/L
2,1 – 2,4mmol/L

Calciphylaxis Registry: PTH levels [pg/mL]
0
10
20
30
40
50
60
1 2 3 40
5
10
15
20
25
30
35
1 2 3 4
Calciphylaxis registryMarch 2012
NDT educational online surveyFebruary 2012
0 – 150150 - 300
300 - 600> 600
0 – 150150 - 300
300 - 600> 600
àRelevant differences between perception (right) andregistry „reality“ (left) regarding PTH levels
PTH
ASN Renal WeekAtlanta 2014

Role of vitamin K antagonist usage and CUA:Potential causalityHayashi M et al; NDT 2012
à Clear association between VKA usage and calciphylaxis: Causality?
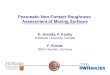
A case-control study ofcalciphylaxis in JapaneseESRD patients
Results of using the multivariate logisticregression model to identify predictors ofCUA at the time of diagnosis
Brandenburg V; on file
Prevalence of coumadin usageIn German CUA patients
Wafarin therapy
yes53%
no47%
n. a.1%
Proportion of patients with and withoutwarfarin therapy in patients included inthe German CUA registry, n=211

Seite 13
Calciphylaxie - EVOLVEJürgen Floege et al.
ASN 2014
iPTH
(pg/
mL)
0
400600800
1200140016001800
Time (months)0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
200
800
Median iPTH CinacalcetPlacebo

Seite 14
Calciphylaxie - EVOLVEJürgen Floege et al.
ASN 2014
Cumulative Incidence Plot of Time to Calciphylaxis Adverse Event

Seite 15
Calciphylaxie - EVOLVEJürgen Floege et al.
ASN 2014

Therapeutical OptionsPathophysiology
PTH/Calcium/phosphate/Vitamin DPossible treatments
High PTHHigh bone remodeling
• Calcimimetics• Non calcium-based Phosphate
binders• Active vitamin D analogs• Bisphosphonates• Surgical parathyroidectomy
High Ca, P and Ca x PNormal/low PTHNormal/low bone remodeling
• Strict control of serum phosphate• No calcium-based phosphate binders• Low calcium dialysate (< 1.25 mM)
Acting on extracellular matrixmineralization
• STS• Bisphosphonates
Acting on extracellular matrixremodeling (growth and adhesion)
• Blocking endothelin receptor ?• Statins ?

Therapeutical OptionsPathophysiology
Hypercoagulation statesPossible treatments
Decreased activity of vitamin Kdependent inhibitors by Warfarin(MGP, OPN, ON, Gas-6)
• Stop Warfarin• Use of alternative anticoagulants
Treatment induced procoagulantstate
• Decrease or stop (CNI)
Protein C and/or S deficiency • Anticoagulation (without warfarin)• Vitamin K supplementation
Anti-phospholipid syndrome • Treatment of the associated pathologies
Endothelial dysfunction • Sodium thiosulfate (NO andantithrombotic properties
• Hyperbaric O2-therapy

Therapeutical OptionsPathophysiology Possible treatment
Redox mechanism STS and its antioxidant effects (glutathion)Proinflammatory mechanisms• Cytokines• Macrophage activation
Bisphosphonates (anti-inflammatory)•Avoid skin biopsy (unless necessary)
Tissue ischemia • STS (vasodilatating effects)• Hyperbaric oxygen• Correcting anemia• Decreasing hypotensive drugs• Restoring vessel permeability
(angioplasty)Secondary mechanisms• Trauma, infection, malnutrition
• Minimizing some acts (surgery,transports)
• Avoid subcutaneous injections• Local treatment• Avoid skin biopsy• Antibiotics• Optimizing nutritional status (parenteral)
Paraneoplasic mechanisms • Pain treatment

Although critical – treat!
After 4 months