Embed Size (px)
Citation preview

1
Jon Chilingerian, Ph.D
Email: [email protected]
Managing Clinics, Care Processes and the
Physics of Patient Flow
September 20, 2013
Brandeis UniversityThe Heller School for
Social Policy & Management
LEUVEN CASE (B)
University Hospital Leuven, Belgium
Chilingerian 2013
2
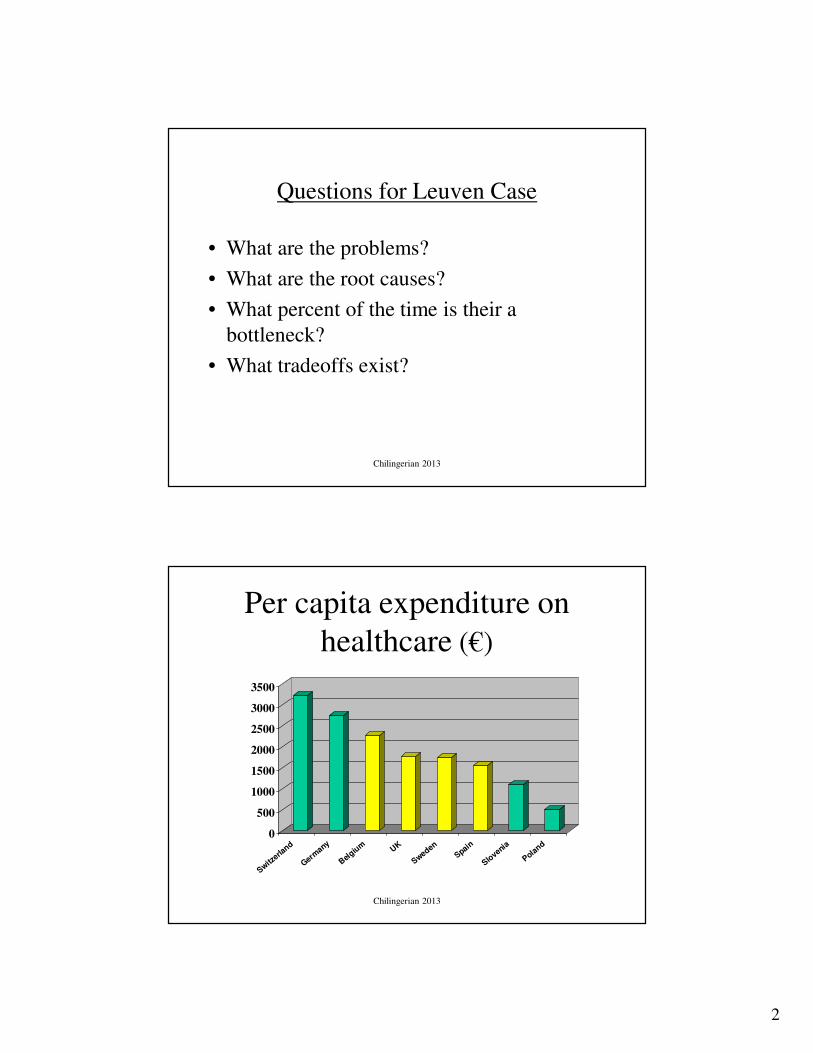
Questions for Leuven Case
• What are the problems?
• What are the root causes?
• What percent of the time is their a
bottleneck?
• What tradeoffs exist?
Chilingerian 2013
Per capita expenditure on
healthcare (€)
0
500
1000
1500
2000
2500
3000
3500
Switzerla
nd
Germany
Belgiu
m UK
Sweden
Spain
Slovenia
Poland
Chilingerian 2013

3
University Medical Center Leuven, Belgium
• Annual budget: 450 million €
• 1.800 beds
• 7000 employees
– 5500 FTE
– 1000 physicians
• 500 consultants
• 500 residents
• Activities / year
– 63.000 admissions
– 540.000 in-hospital days
– 450.000 outpatients
– 50.000 emergencies
Chilingerian 2013
-30000
-25000
-20000
-15000
-10000
-5000
0
5000
1995 1996 1997 1998 1999 2000
year
profit / loss
forecast
Financial results (1000 €)
Chilingerian 2013

4
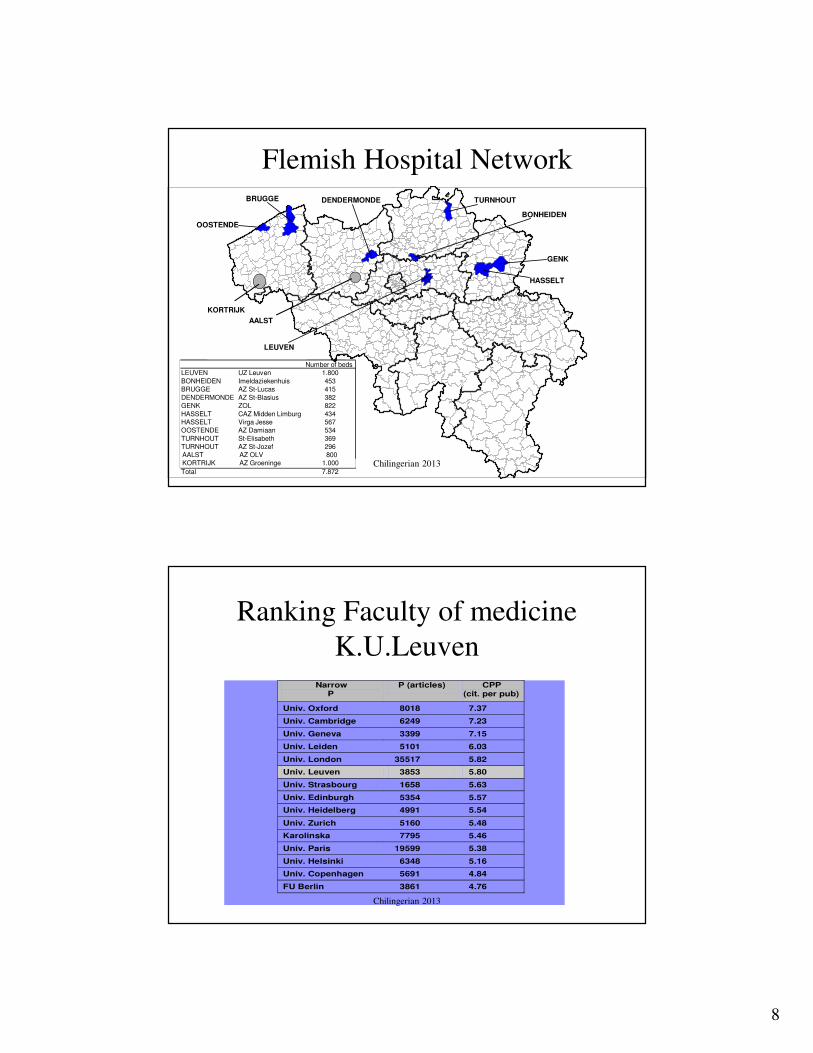
Flemish Hospital Network
DENDERMONDE
LEUVEN
BONHEIDEN
TURNHOUT
GENK
HASSELT
BRUGGE
OOSTENDE
Number of beds
LEUVEN UZ Leuven 1.800
BONHEIDEN Imeldaziekenhuis 453
BRUGGE AZ St-Lucas 415
DENDERMONDE AZ St-Blasius 382
GENK ZOL 822
HASSELT CAZ Midden Limburg 434
HASSELT Virga Jesse 567
OOSTENDE AZ Damiaan 534
TURNHOUT St-Elisabeth 369
TURNHOUT AZ St-Jozef 296
Total 7.872
AALST
KORTRIJK
AALST AZ OLV 800
KORTRIJK AZ Groeninge 1.000 Chilingerian 2013
1997 1998
Circumcision 131 180
Tooth extraction (general anesthesia) 44 558
Coronary Artery Bypass Surgery 465 560
Laparoscopic cholecystectomy 258 342
Inguinal Hernia 280 348
Appendectomy 202 235
Transtympanal draining using prothesis 246
Discus hernia 181 217
Adenoidectomy 281
Sample of Services
Chilingerian 2013

5
1997
Liver 25
Heart
Lung
Kidney 125
Pancreas
Donor prelevation 65
Transplants
Chilingerian 2013
Chronology
Events
Operational
Organisational
Strategic
Alliances,
Networking
Care Program
Choices
1998 - 1999
Change project
(McKinsey)
Change project
2000
Implementation phase
Implementation phase
2001 and on
Annual Department plan
Annual Department plan
Strategic Implementation
Chilingerian 2013
6
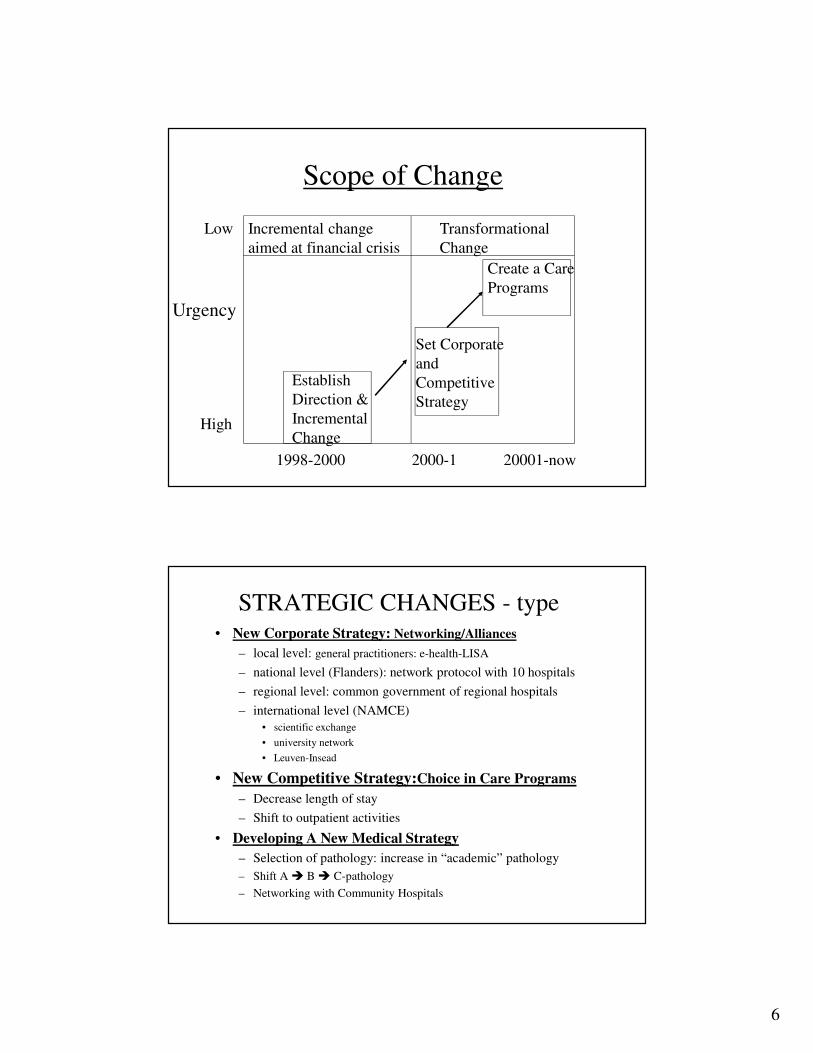
Scope of Change
Urgency
Low
High
Incremental change
aimed at financial crisis
Transformational
Change
Establish
Direction &
Incremental
Change
Create a Care
Programs
Set Corporate
and
Competitive
Strategy
1998-2000 2000-1 20001-now
STRATEGIC CHANGES - type• New Corporate Strategy: Networking/Alliances
– local level: general practitioners: e-health-LISA
– national level (Flanders): network protocol with 10 hospitals
– regional level: common government of regional hospitals
– international level (NAMCE)
• scientific exchange
• university network
• Leuven-Insead
• New Competitive Strategy:Choice in Care Programs
– Decrease length of stay
– Shift to outpatient activities
• Developing A New Medical Strategy
– Selection of pathology: increase in “academic” pathology
– Shift A � B � C-pathology
– Networking with Community Hospitals
7
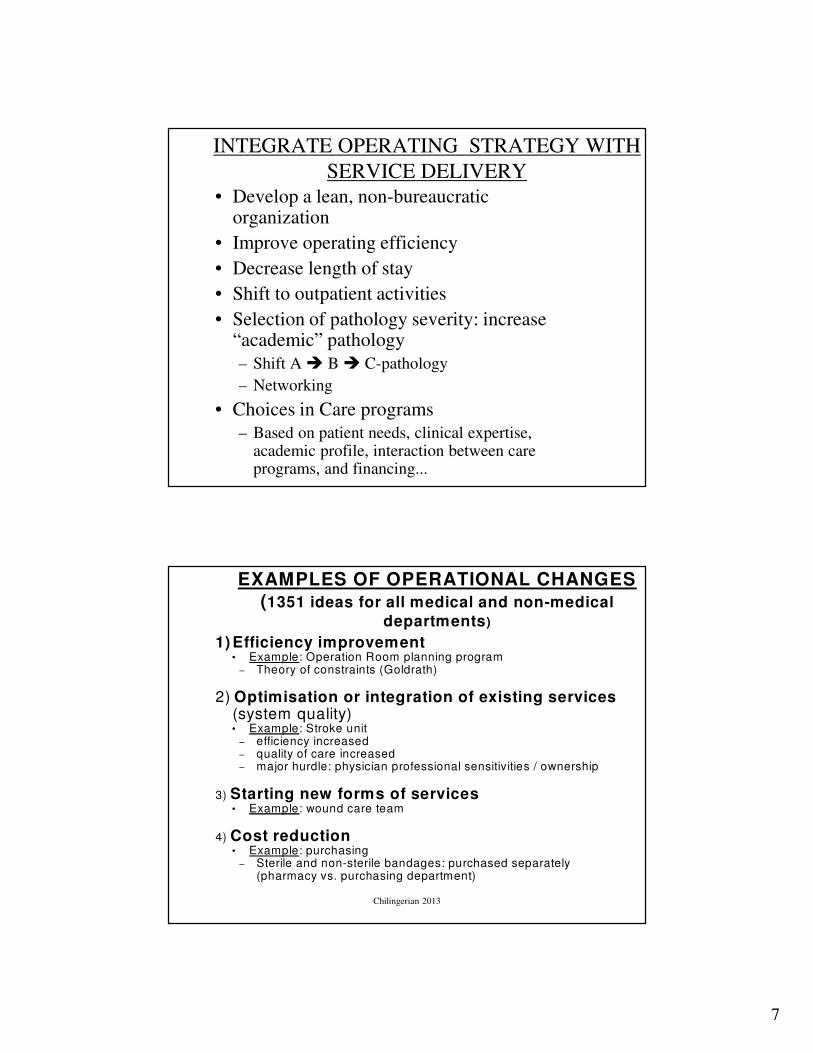
INTEGRATE OPERATING STRATEGY WITH
SERVICE DELIVERY
• Develop a lean, non-bureaucratic organization
• Improve operating efficiency
• Decrease length of stay
• Shift to outpatient activities
• Selection of pathology severity: increase “academic” pathology
– Shift A � B � C-pathology
– Networking
• Choices in Care programs
– Based on patient needs, clinical expertise, academic profile, interaction between care programs, and financing...
1) Efficiency improvement• Example: Operation Room planning program
– Theory of constraints (Goldrath)
2) Optimisation or integration of existing services(system quality)• Example: Stroke unit
– efficiency increased– quality of care increased– major hurdle: physician professional sensitivities / ownership
3) Starting new forms of services• Example: wound care team
4) Cost reduction• Example: purchasing
– Sterile and non-sterile bandages: purchased separately (pharmacy vs. purchasing department)
EXAMPLES OF OPERATIONAL CHANGES (1351 ideas for all medical and non-medical
departments)
Chilingerian 2013
8
Flemish Hospital Network
DENDERMONDE
LEUVEN
BONHEIDEN
TURNHOUT
GENK
HASSELT
BRUGGE
OOSTENDE
Number of beds
LEUVEN UZ Leuven 1.800
BONHEIDEN Imeldaziekenhuis 453
BRUGGE AZ St-Lucas 415
DENDERMONDE AZ St-Blasius 382
GENK ZOL 822
HASSELT CAZ Midden Limburg 434
HASSELT Virga Jesse 567
OOSTENDE AZ Damiaan 534
TURNHOUT St-Elisabeth 369
TURNHOUT AZ St-Jozef 296
Total 7.872
AALST
KORTRIJK
AALST AZ OLV 800
KORTRIJK AZ Groeninge 1.000 Chilingerian 2013
Ranking Faculty of medicine
K.U.LeuvenNarrow
P P (articles) CPP
(cit. per pub)
Univ. Oxford 8018 7.37
Univ. Cambridge 6249 7.23
Univ. Geneva 3399 7.15
Univ. Leiden 5101 6.03
Univ. London 35517 5.82
Univ. Leuven 3853 5.80
Univ. Strasbourg 1658 5.63
Univ. Edinburgh 5354 5.57
Univ. Heidelberg 4991 5.54
Univ. Zurich 5160 5.48
Karolinska 7795 5.46
Univ. Paris 19599 5.38
Univ. Helsinki 6348 5.16
Univ. Copenhagen 5691 4.84
FU Berlin 3861 4.76
Chilingerian 2013
9
League of European Research-
Intensive Universities
Chilingerian 2013
NAMCE (network of academic
medical centers Europe)
• Collaboration with INSEAD
• getting new ideas on hospital management
• discussing, validating new evolutions
• scientific work on hospital management
• exchange of experiences with other European
centers
Chilingerian 2013
10
What were the elements of
organizational change?
• Strategic Re-direction
• New Board of Directors
• Delayering
• Care Programs
• New management Practices– Yearly department plans
– New incentive scheme for MD’s
– Steering committee for Medical Decision Making
– Activity Based Budgets
– Limited Appointment of Medical Chairs: 5-year with evaluation
– Computer Aided Operating Room Scheduling
CULTURE CHANGE
� Basic idea: create a customer-oriented rather than a provider-oriented organisation
� 1) creation of medical-surgical divisions
� 2) creation of mixed management teams
� purpose: link the hospital domains in a structural way
� Method
� MD: clinical director
� nurse: nursing manager
� economic/administrative: administrative manager
� Implication: Separation of professional and organisational responsibility
Chilingerian 2013

11
1. Mental health care
2. Mother and child
3. General surgery
4. Rehabilitation
5. Thorax
6. General internal medicine
7. Abdomen
8. Oncology
9. Critical care
10. Head / neck / neuro
11. Medical diagnostical services
HOW? CLUSTER MEDICAL-SURGICAL DIVISIONS
Chilingerian 2013
Organization chart UMC Leuven
Division abdomenDivision general surgeryDivision rehabilitationDivision oncologyDivision head / neck / neuro
Clinical Director Director Finance/Admin.
Division mental health
Division medical diagnosticsDivision Mother and Child
Clinical Director Director HR
Division thorax
Division general internal medicineDivision Critical Care
Clinical Director Chief Medical Doctor Nursing Director
CEO
Board of Trustees, Hospital Dean, faculty of Medicine
Vice-ChancellorChairman of the Board
Chancellor University
Board of trustees, University
Chilingerian 2013

12
Care Program Concept
Chilingerian 2013
Strategy?
• Medical specialities (e.g., emergency services,
oncology, transplantation, hypertension, etc.) and
clinical activities (admission, investigation,
therapy, recovery, etc) are the sources of your
advantage.
• Most hospitals can perform similar activities better
than their rivals—
– this is called the operating strategy
• Few hospitals offer different services and few
perform different activities from rivals, or perform
them in unique ways—
– this is called strategic positioning

13
Clinical Activities
Admission
Investigation Therapy Recovery
How can these be done
differently? Can these become
positioned as better services?
Chilingerian 2013
250 CARE PROGRAMS
Hypertension
Inflammatory intestinal diseases
Abdominal wall hernia
Gastric-oesophageal reflux
Prostate tumour
...
C
a
r
e
p
r
o
g
r
a
m
A care program consists of the
coordinated delivery of all
services provided to a group of
patients with similar pathology
and similar care pattern

14
ACTIVITY CENTER
Hospitalisation
Operation
Quarters
Administration medical
staff
Financial
Division
Human
Resources
Ho
sp.
On
colo
gy
Ho
sp.
HK
-EN
T-S
tom
ato
Ho
sp.
IG-N
euro
-Der
mato
...
OK
A 1
OK
A 2
OK
A P
elle
nb
erg
OK
A M
ate
rn
ity Q
ua
rter
...
Ad
min
istr
ati
on
Med
ica
l S
taff
Acc
ou
nti
ng
An activity center is a provider of clinical* or non-clinical* services to a care program. They constitute the
operational units in which the means of the departments are concentrated.
* Medical, paramedical or nursing services
** Administrative or technical services
Sa
lary A
dm
inis
tra
tio
n
Pers
on
nel
Ad
min
istr
ati
on
Com
mu
nic
ati
on
Tra
inin
g
Operating Strategies: Alignment of
Activities/FunctionsTypes of Activity
Centers
Radiology SICU
• Physician
Services Nurse Beds• ...O.R.
C
a
r
e
P
r
o
g
r
a
m
Cardiovascular Disease
Transplantation
Orthopaedic disease
Labs
Patient
Management
Practice
Management

15
Concept of ‘Care Programs’
• Which care programs make us distinctive? Innovative, Effective, and Efficient
• Which care programs are most profitable?
• In which care programs are our patients extremely satisfied?
• In which care programs are our physicians, nurses, and other care providers extremely satisfied?
• Which activities in the care program add customer value?
• Which physicians are on the best practice frontier?
Chilingerian 2013
8
REFLECTIONS ABOUT CARE PROGRAMS
Source : McKinsey
High
Low
Profile
Financial
attractiveness
Non profitable
Profitable
?
?
?
?
?
X
For care program x, how can we :
• Increase financial attractiveness ? (i.e. decrease length-of-stay; decrease RX / lab utilisation)
• Increase the profile ?
• Attract more patients?
Chilingerian 2013
16
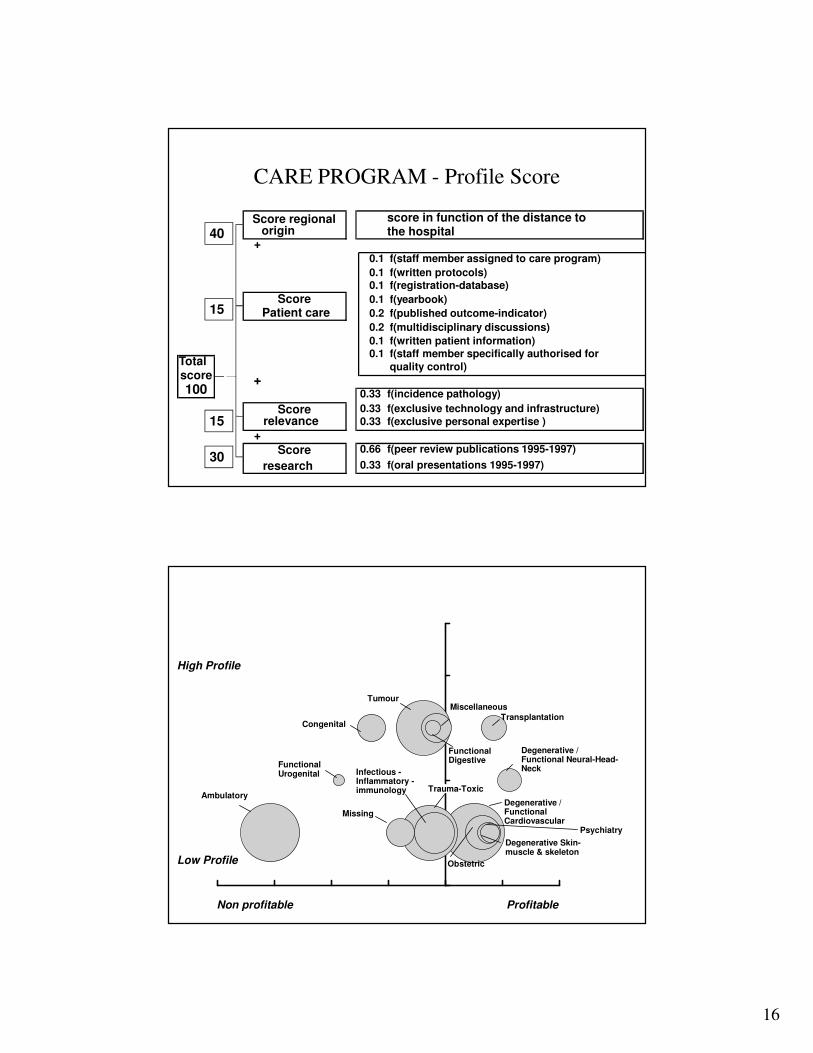
CARE PROGRAM - Profile Score
Score regional score in function of the distance to origin the hospital
+0.1 f(staff member assigned to care program)
0.1 f(written protocols)0.1 f(registration-database)
Score 0.1 f(yearbook)
Patient care 0.2 f(published outcome-indicator)
0.2 f(multidisciplinary discussions)
0.1 f(written patient information)0.1 f(staff member specifically authorised for
Total quality control)score +100 0.33 f(incidence pathology)
Score 0.33 f(exclusive technology and infrastructure)
relevance 0.33 f(exclusive personal expertise )
+
Score 0.66 f(peer review publications 1995-1997)
research 0.33 f(oral presentations 1995-1997)
40
15
15
30
Exhibit 21
Position of Clusters of Care Programs UMCL
TransplantationCongenital
Tumour
Functional Digestive
Miscellaneous
Degenerative / Functional Neural-Head-NeckFunctional
Urogenital
Degenerative Skin-muscle & skeleton
Degenerative / Functional Cardiovascular
Psychiatry
Infectious -Inflammatory -immunology Trauma-Toxic
Obstetric
Missing
Ambulatory
Non profitable
Low Profile
Profitable
High Profile

17
15
All care programs
0
25
50
75
100
-100% -90% -80% -70% -60% -50% -40% -30% -20% -10% 0% 10% 20% 30% 40% 50%
Financiële aantrekkelijkheid***
Pro
file
rin
g**
Eigen zorgprogramma's Top Klinisch Gedeelde zorgprogramma's Top Klinisch UZ exploitatie 1997Eigen zorgprogramma's Expert Gedeelde zorgprogramma's Expert Eigen zorgprogramma's niet bepaaldEigen zorgprogramma's Basis Gedeelde zorgprogramma's Bas is Gedeelde zorgprogramma's niet bepaald
h i
niet kostendekkend kostendekkend
Chilingerian 2013
Medical staff
Dept.-own AC’s (i.e..
endoscopy)
ii
Nursing manager
Administrative manager
Physician
(Clinical director, head of the Division)
Division Management
Gastroenterology
Physician (Head of the Dept.)
Nurses
Abdom. surgery Urology Hospitalisation Consultation
AC-Responsible
NursingStaff
”Departments" Department-specific - AC
...
Divisional Structure
18
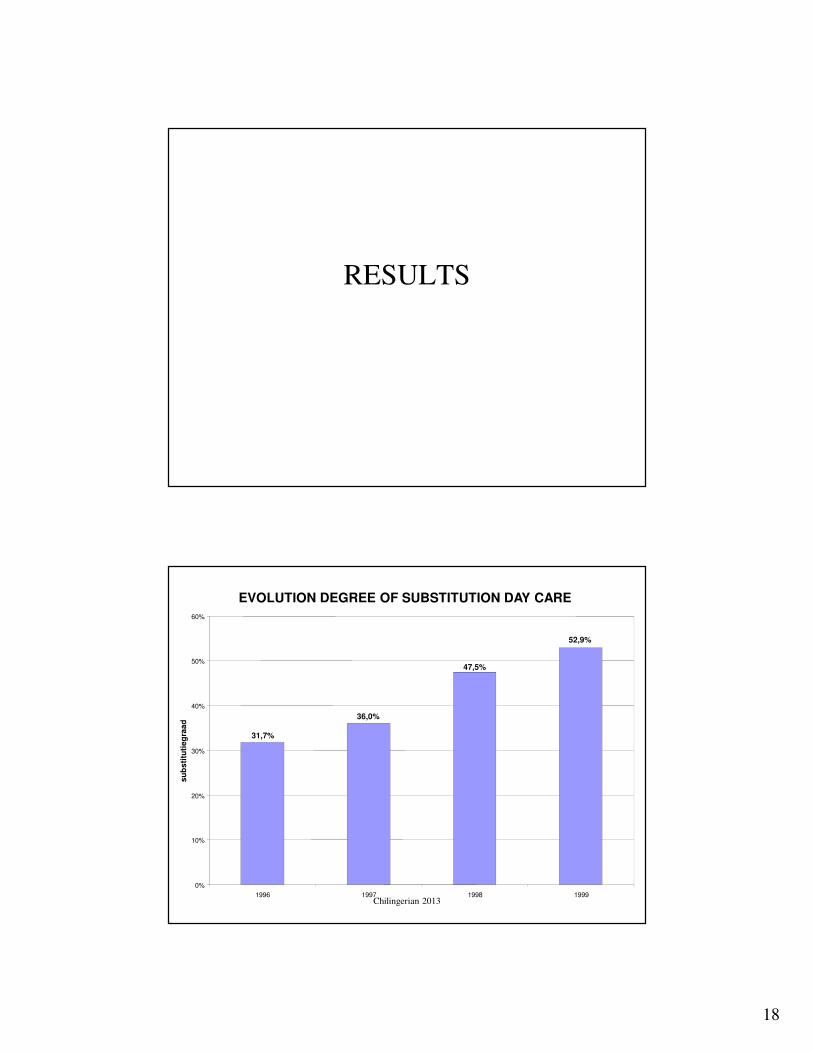
RESULTS
EVOLUTION DEGREE OF SUBSTITUTION DAY CARE
31,7%
36,0%
47,5%
52,9%
0%
10%
20%
30%
40%
50%
60%
1996 1997 1998 1999
su
bs
titu
tie
gra
ad
Chilingerian 2013

19
STRATEGIC CHANGES – RESULTS: USED BEDS
1.000
1.100
1.200
1.300
1.400
1.500
1.600
1.700
1.800
1.900ja
n/9
6m
rt/9
6m
ei/9
6ju
l/9
6se
p/9
6n
ov/9
6ja
n/9
7m
rt/9
7m
ei/9
7ju
l/9
7se
p/9
7n
ov/9
7ja
n/9
8m
rt/9
8m
ei/9
8ju
l/9
8se
p/9
8n
ov/9
8ja
n/9
9m
rt/9
9m
ei/9
9ju
l/9
9se
p/9
9n
ov/9
9ja
n/0
0m
rt/0
0m
ei/0
0ju
l/0
0se
p/0
0n
ov/0
0ja
n/0
1
Chilingerian 2013
0
2
4
6
8
10
12
1996 1997 1998 1999 2000
Len
th o
f sta
y (
days)
EVOLUTION LENGTH OF STAY 1997-2000: -15-20 %
Chilingerian 2013
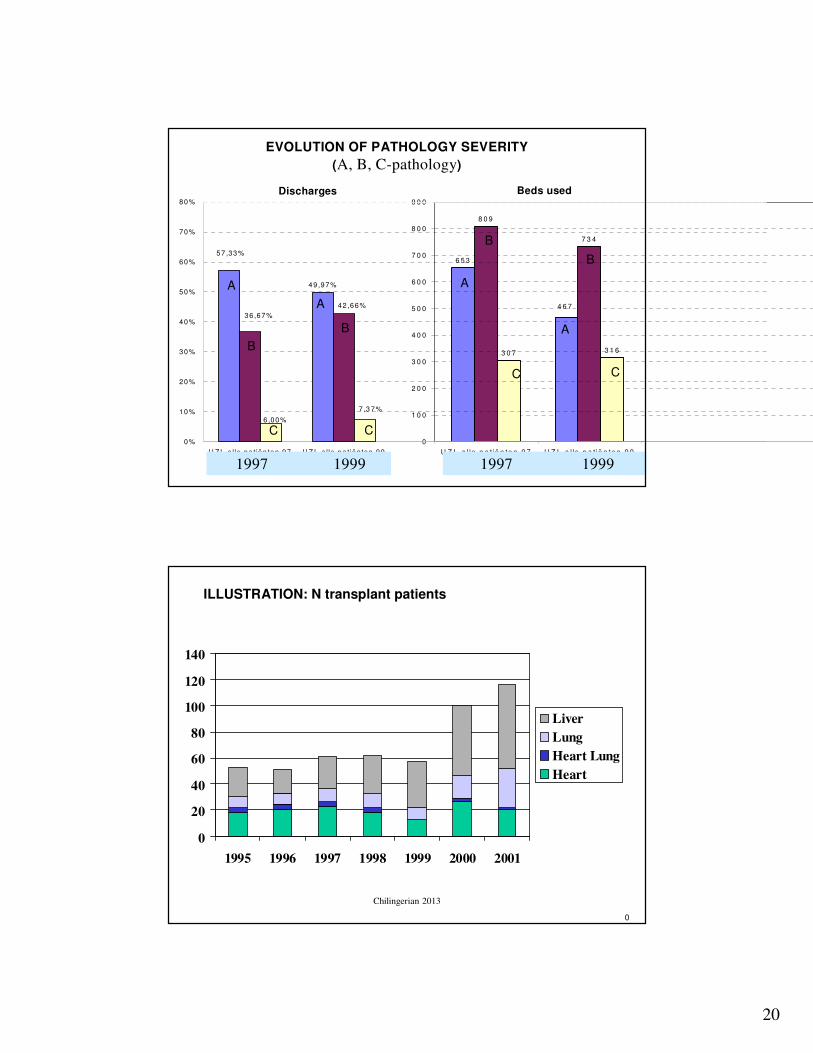
20
6 5 3
8 0 9
7 3 4
3 0 7 3 1 6
4 6 7
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
6 0 0
7 0 0
8 0 0
9 0 0
U Z L a l le p a t ië n te n 9 7 U Z L a l le p a t ië n te n 9 9
49 ,97%
57,33%
42,66%
36,67%
6,00%
7,3 7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
U Z L a lle pa tiën ten 97 U Z L a lle pa tiën ten 99
1997 1999 1997 1999
EVOLUTION OF PATHOLOGY SEVERITY
(A, B, C-pathology)
Discharges Beds used
A
B
C
A
A
A
B
B
B
CC
C
0
ILLUSTRATION: N transplant patients
0
20
40
60
80
100
120
140
1995 1996 1997 1998 1999 2000 2001
Liver
Lung
Heart Lung
Heart
Chilingerian 2013

21
Financial results (1000 €)
-30000
-20000
-10000
0
10000
20000
30000
1997 1998 1999 2000 2001 2002 2003
year
profit / loss
forecast
Director
Finance/Admin.
Helmut
OR Coordinator
Division Abdomen
Peter
Clinical Director
Karin
Chair Cardiac Surgery
Chair Transplant
Committee
Christophe
MICU
Division General
Internal Medicine
Other Clinical
Directors
Dean, Faculty of
Medicine
Marcel
Chief Medical Doctor
Chair General
Internal Medicine
Karel
Chair Hepatology
Chief Internal Med.
Luc
Chair Transplant
Surgery
Transplant
Coordinator
Division Critical Care
Maria
Chair
Anesthesiology
Bart
Chair SICU
Division Thorax
Director HR
Nursing Director
Jan
CEO
Board of Trustees
Vice-Chancellor
Chairman of the
Board
Chancellor University
Partial Organization Chart – Leuven Medical Center

22
Unintended Consequences
• Selective Investment and Growth of Care Programs—based on patient needs, core expertise, academic profile, interaction between care programs, and payment and financing
– Capacity Problems: surgical cancellations
– Political Problems: inside and outside
– Increased Conflicts among physicians and caregivers
• Was this strategic shift financially sustainable in the Belgian Healthcare system?
Chilingerian 2013
Surgical Patient Flow
Flow of
ER
Patients
Flow of
Transplant
Patients
OR SICUGeneral
Beds
Average
daily
discharge
Flow of
Elective
Patients
Capacity 307 hrs/day 56 beds 1782 beds
Utilization 238 hrs 55 beds 1427 beds
Variability +/- 103 surgical hrs. +/- 4.1 days +/- 189 patient days
85%
.7%
100%
80%
14.3%
20%

23
Cardiac Surgery activities as influenced
by ICU capacity (2001)
April May June
• N beds 18.25 20.5 22.5
• N cardiac surgeries postponed 29 21 12
• N patients refused 69 59 27
Chilingerian 2013
In 2002, Bart, the Chair of the SICU requested 20 new SICU beds
at a cost of €3 million. Though an analysis revealed a 40% chance
of a bottleneck on any given day, the clinical leaders were reluctant
to add capacity because of an anomaly in the information.
Conclusion: More Beds
Chilingerian 2013
24
More Beds?
When the Chair of Internal Medicine
proposed the MICU (medical intensive care
unit) as a buffer, the chair of the SICU had
quipped, “You are messing up my strategy
to obtain more beds. I do not need your
MICU beds, let me handle this!”
Chilingerian 2013
Questions for Leuven Case
• What are the underlying problems?
– What are the root causes?
• Describe the best ways to schedule the OR?
• Explain these Tables:
7-9; 11; 18; 19; & 20
Chilingerian 2013

25
Solutions??
Chilingerian 2013
nursing days
0%5%
10%15%20%25%30%35%40%45%50%55%
19
97
A
19
98
A
19
99
A
20
00
A
19
97
B
19
98
B
19
99
B
20
00
B
19
97
C
19
98
C
19
99
C
20
00
C
* opsplitsing I-nI op basis van geëxtrapoleerd MVG-profiel 1997
SHIFT OF PATHOLOGY SEVERITY
(A, B, C- pathology)
A-care B-care C-care

26
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
A (gelijkgesteld aan 1) B C
Pathologiezwaarte
Mu
ltip
lic
ati
efa
cto
r
Kosten Inkomsten
Differential growth in cost and revenue with a shift from A to C
pathology: Medical Imaging
N nursing days in ICU by
transplant patients
0
200
400
600
800
1000
1200
1995 1996 1997 1998 1999 2000
Liver
Lung
Heart Lung
Heart
Chilingerian 2013

27
1997, UZL A-care C-care C vs A
Intensive care bed 0,1 7,9 79
Non-ITE bed 6,1 20,8 3,41
Total 6,2 28,7 4,63
Length of stay (days)
Unintended consequence 1: Cost increaseC-care requires more beds, especially ICU beds
Chilingerian 2013
Protracted Critical Illness (PCI) Patients in SICU (LOS > 21 days)
Year No. PCI patients
(%)
Capacity utilization
(%)
Mortality
(%)
1995 7.0 34 20
1996 7.7 40 26
1997 9.0 46 16
1998 9.9 47 19
1999 10.5 49 18
2000 10.0 47 18
Chilingerian 2013
28
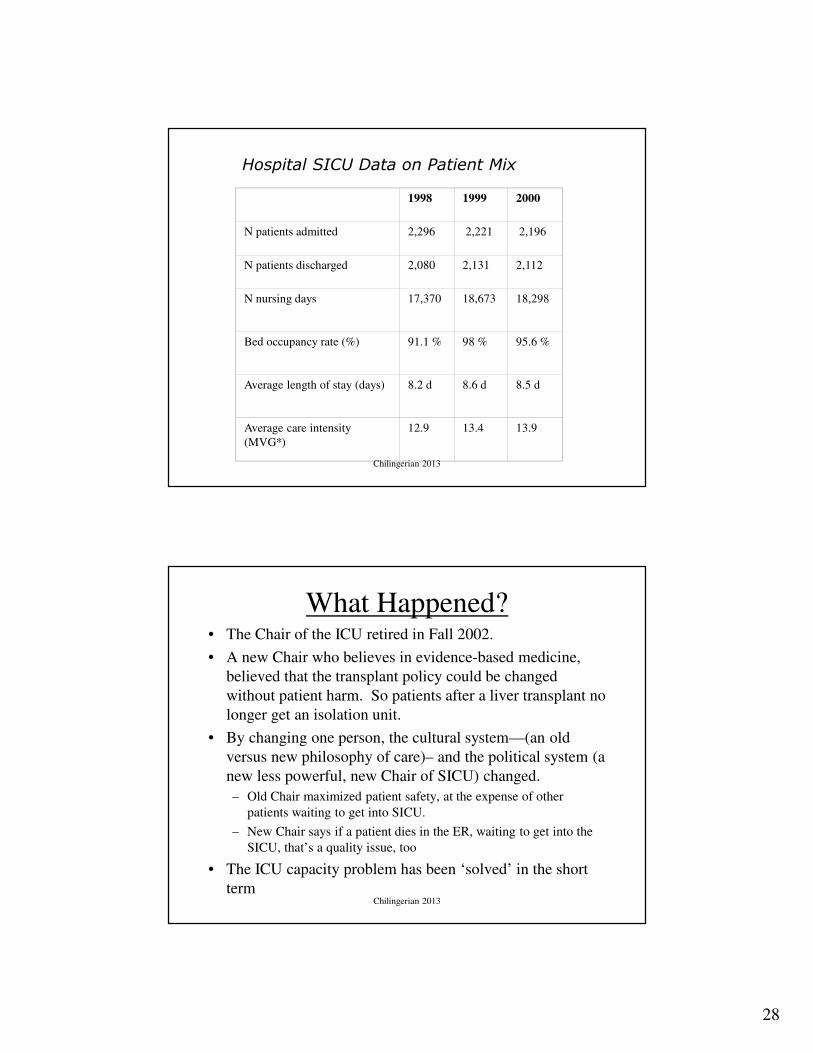
Hospital SICU Data on Patient Mix
1998 1999 2000
N patients admitted 2,296 2,221 2,196
N patients discharged 2,080 2,131 2,112
N nursing days 17,370 18,673 18,298
Bed occupancy rate (%) 91.1 % 98 % 95.6 %
Average length of stay (days) 8.2 d 8.6 d 8.5 d
Average care intensity
(MVG*)
12.9 13.4 13.9
Chilingerian 2013
What Happened?• The Chair of the ICU retired in Fall 2002.
• A new Chair who believes in evidence-based medicine,
believed that the transplant policy could be changed
without patient harm. So patients after a liver transplant no
longer get an isolation unit.
• By changing one person, the cultural system—(an old
versus new philosophy of care)– and the political system (a
new less powerful, new Chair of SICU) changed.
– Old Chair maximized patient safety, at the expense of other
patients waiting to get into SICU.
– New Chair says if a patient dies in the ER, waiting to get into the
SICU, that’s a quality issue, too
• The ICU capacity problem has been ‘solved’ in the short
termChilingerian 2013

29
Technical system (or current strategic
design)
• What is the mission, strategy, goals, and
constraints?
• Why are they doing this? values? Incentives
• Who is involved: people, roles, & responsibilities
• How is it being done? Key processes (decision
making, communication, etc)
• How are activities structured (differentiated, integrated
and coordinated) ?
Does this design work? Is there alignment or fit
between strategy and the parts?
Chilingerian 2013
Congruence Model
Executive
Leadership
Mission&
Strategy
Critical
Tasks
Culture &
Informal
Structure
People
Formal
Structure
ORGANIZATIONAL
PERFORMANCE
30
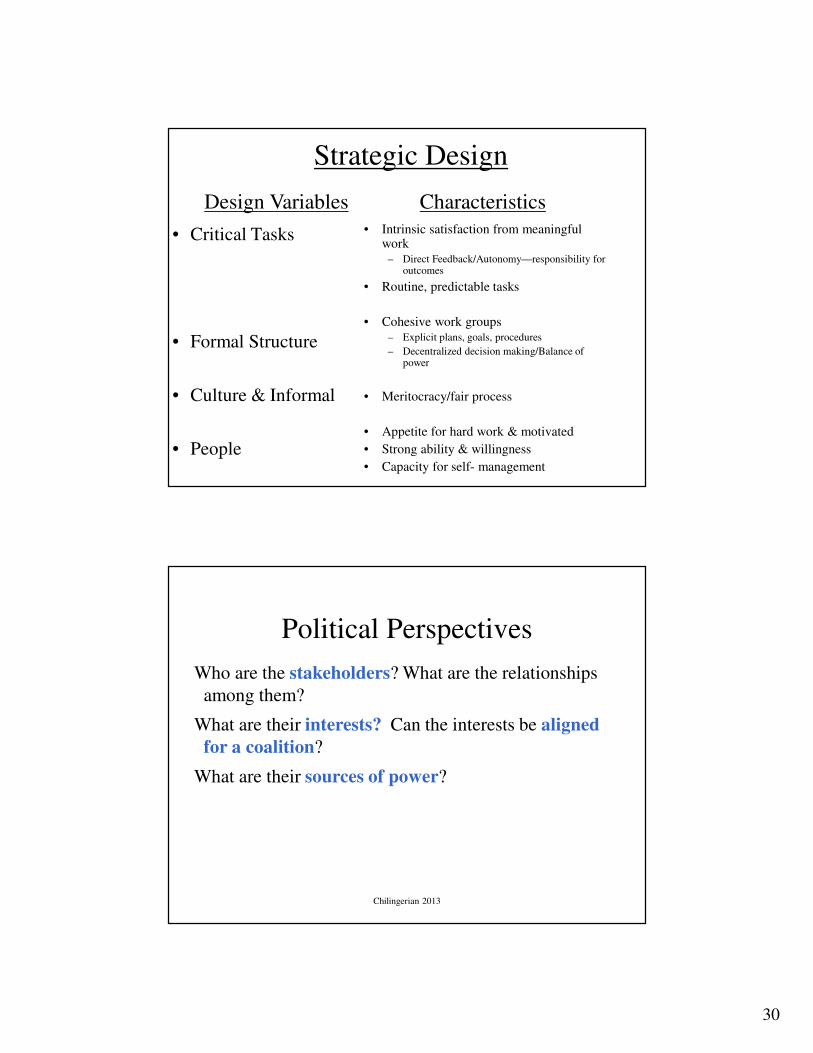
Strategic Design
• Critical Tasks
• Formal Structure
• Culture & Informal
• People
• Intrinsic satisfaction from meaningful work
– Direct Feedback/Autonomy—responsibility for outcomes
• Routine, predictable tasks
• Cohesive work groups– Explicit plans, goals, procedures
– Decentralized decision making/Balance of power
• Meritocracy/fair process
• Appetite for hard work & motivated
• Strong ability & willingness
• Capacity for self- management
Design Variables Characteristics
Political Perspectives
Who are the stakeholders? What are the relationships
among them?
What are their interests? Can the interests be aligned
for a coalition?
What are their sources of power?
Chilingerian 2013
31
What shared values, mindsets, beliefs and assumptions
do people have regarding what the organization is all
about? Are they consistent across people and areas?
What implications do these values and assumptions have?
Are they good or bad for performance?
Cultural Perspective
Chilingerian 2013
Where are the bottlenecks?
feedback
Technical System
Cultural System
Political SystemCapacity
constraintPhysician Behavior
AssumptionsLeadership
& decision
making
overload
overload
Chilingerian 2013

32
Explain capacity problems work
in the three systems
• Technical System
• Social & Cultural System
• Political System
Chilingerian 2013
33
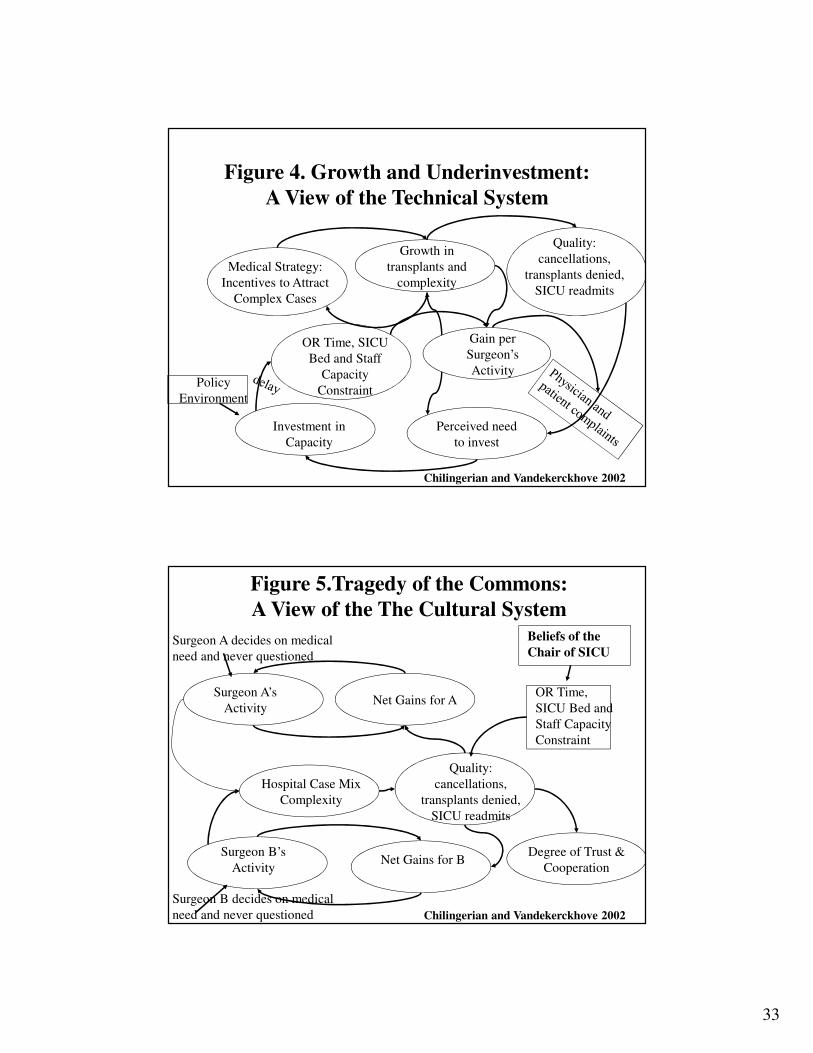
Figure 4. Growth and Underinvestment:
A View of the Technical System
Chilingerian and Vandekerckhove 2002
Growth in
transplants and
complexity
Gain per
Surgeon’s
Activity
Quality:
cancellations,
transplants denied,
SICU readmits
OR Time, SICU
Bed and Staff
Capacity
Constraint
Investment in
Capacity
Perceived need
to invest
Policy
Environment
Medical Strategy:
Incentives to Attract
Complex Cases
Figure 5.Tragedy of the Commons:
A View of the The Cultural System
Surgeon A’s
Activity
Hospital Case Mix
Complexity
Surgeon B’s
Activity
OR Time,
SICU Bed and
Staff Capacity
Constraint
Surgeon A decides on medical
need and never questioned
Surgeon B decides on medical
need and never questioned Chilingerian and Vandekerckhove 2002
Beliefs of the
Chair of SICU
Quality:
cancellations,
transplants denied,
SICU readmits
Net Gains for B
Net Gains for A
Degree of Trust &
Cooperation

34
Figure 6. Shifting the Burden:
A View of the Political System
Delay
Surgical Cancellations,
and Queues
SICU
Availability
Develop More Service
Capacity
Deterioration of
Service Quality and
Physician Morale
Political Power
& Influence
Perceived
unfairness
Chilingerian and Vandekerckhove 2002
Demand for
SICU
• Dangers of arrogant leadership, an inability to challenge physician autonomy, bureaucratic silos, & a culture of finger pointing
• Need for a strategic service vision based on real strengths of care programs—
– identify a unique and valuable position, choose what not to do, choose a unique combination of activities
• Once strategy has been developed, the strategy must be aligned with the operations and embodied into everything the organization does
Takeaways: Leuven turnaround
Chilingerian 2013

35
• Think in terms of long-term relationships with physicians team members—align interests
– Avoid reliance on authority—build commitment to shared clinical goals
• Institute Fair process to deeply engage physicians & teach them develop their own strategic service vision
– How? Focus on diagnosing the strategic problems: separating facts from assumptions
• Invest in clinical agendas to build partnerships not to make deals
– value different perspectives, set high standards
– prevent them from making strategic mistakes
– Be honest in letting them know how things are going
Takeaways: Leuven turnaround
36
Thank you
The Heller School for
Social Policy &
Management
Chilingerian 2013

37
Care Program Activity System
RN Hiring
RN Cross Training
Multi-speciality wards
& Operational planners
REDUCED LOS &
UNNECESSARY
ANCILLARY
SERVICES
Technology
choices
Selection of Services
(Offered/Not Offered)
Standardized
OR Slots
Transfer PricesMD Hiring/Attitudes
MD
Incentive
Plan
Reward MD
Efficient Practices
Test
Turnaround
time
INCREASED
ADMISSIONS
Target Patient
Segments
Chilingerian 2013
























![Appendectomy Case Report[1]](https://img.pdfslide.us/doc/110x75/546ff242b4af9fc2738b45a1/appendectomy-case-report1.jpg)

