Embed Size (px)
Citation preview

Rodent Surgery
University Animal Care * The University of Arizona
www.UAC.arizona.edu
Why?
Non-compliance leads to reporting to USDA and
PHS
Changes in Program are required
This class is in response to PHS concerns
Goal of Research and Animal Welfare: A good surgical outcome
Pre-operative preparation and surgical support Asepsis, or sterile technique, which is used to reduce the chance of
infection: o Surgery room set-up, instrument/tool sterilization, and surgeon
preparation
Appropriate anesthesia o Includes selection of drugs and anesthetic monitoring
Good surgical technique o Includes gentle tissue handling, correct use of surgical instruments and
adequate knowledge of anatomy and procedure being performed
Adequate post-operative care and pain management Consistent recordkeeping
o Identifies trends that that can be used for surgical refinements o Necessary for documentation of scientific data
o Prior IACUC approval of all procedures; all changes approved by amendment prior to implementation.
The Guide Requires:
Aseptic technique be followed for all survival surgical procedures. This includes “practice” surgeries. The manner in which asepsis is achieved varies by species.
Surgical Aseptic
Technique
Creating and Maintaining a
controlled environment free of
bacteria, viruses and fungi
Also known as Sterile
Technique
5
Office of Responsible Conduct of Research
IACUC Policies, Procedures,
and Guidance's: http://orcr.arizona.edu/iacuc/procedures
Expired Medical materials
Prohibited: Anesthesia, Analgesia, Euthanasia
Other Medical Materials: May be used in Non-survival /
acute procedures, but MUST get approval from IACUC
prior

IACUC Policies, Procedures,
and Guidance's: Rodent Surgery & Instrument Sterilization
http://orcr.arizona.edu/sites/orcr.arizona.edu/files/304%20
Rodent%20Surgery.pdf
Use of Drugs and Compounds in Animal Studies (incl.
Non-Pharmaceutical Grade)
http://orcr.arizona.edu/sites/orcr.arizona.edu/files/210%20
Use%20of%20Compounds%20in%20Animals.pdf
Surgery Area Set up. The Guide (page 144):
“The design of a surgical facility should accommodate
the species to be operated on and the complexity of the procedure to be performed.”
For most rodent survival surgery, “an animal procedure
laboratory is recommended; the space should be
dedicated to surgery…and appropriately managed to
minimize contamination from other activities conducted
in the room at other times.”
Setting Your Lab Up For
Surgery
Select an area that has the least traffic
Dedicate it for at least the day before and day of
surgery. Best to do permanent dedication.
Select an area distant to prep area to minimize
contamination.
Use of LF Bench for surgery excellent.
Use of Fume hood good for prep
Preparation of Surgery
Area
Day before surgery remove anything from the
area that is not applicable for surgery.
If shelves above, remove everything from
them.
Spray area with a disinfectant—Accel,
Clidox, Versaclean, whatever you have,
Day of—respray the area.
Lay out a disposable, sterile drape on surgical
area. May need two—one for where
instruments will be; one for animal.

Put up a Stop Sign!
Important to minimize traffic in the surgery area.
Let lab members know not to walk by during
surgery.
No visitors/staff leaning close without caps and
masks.
No touching of the sterile field or instruments without sterile gloves.
Instrument and Device
Preparation
Use of sterile disposable instruments and drapes
are encouraged, when possible.
For non-disposable instruments, prior to
sterilization, make sure instruments and devices
are clean, with no blood or debris on them.
(Should have been cleaned following previous surgery.)
Instrument Preparation
Place instruments in a “peel open” pouch, wrap them in brown paper, or place them in an instrument tray wrapped with a cloth drape or brown paper. o Instruments can be singly wrapped, or complete sets of
instruments can be wrapped. o If autoclaving or using gas sterilization, the wrapping material
must be permeable. Steam or gas cannot permeate a tightly sealed metal container or something wrapped in aluminum foil.
Sterilization methods
o Autoclaving:
Some materials such as PE-10 tubing can be autoclaved by placing in a small container of water. Wrapped supplies require 30 minutes at 121 deg C (250 deg F)
Dry heat sterilization at 340oF/170oC for 1 hour, 320oF/160oC for 2 hours or 300oF/150oC for 3 hours:
Instruments must be dry and must be held at the correct temperature for the entire period.
o Sterilization with ethylene oxide gas [ETO; performed by UAC for a fee]
o Vaporized hydrogen peroxide [VHP; performed by UAC for a fee]
o Ionizing radiation [usually only performed by a commercial service]
o Cold sterilization for devices that cannot be sterilized as above, such as operating microscopes and stereotactic devices.
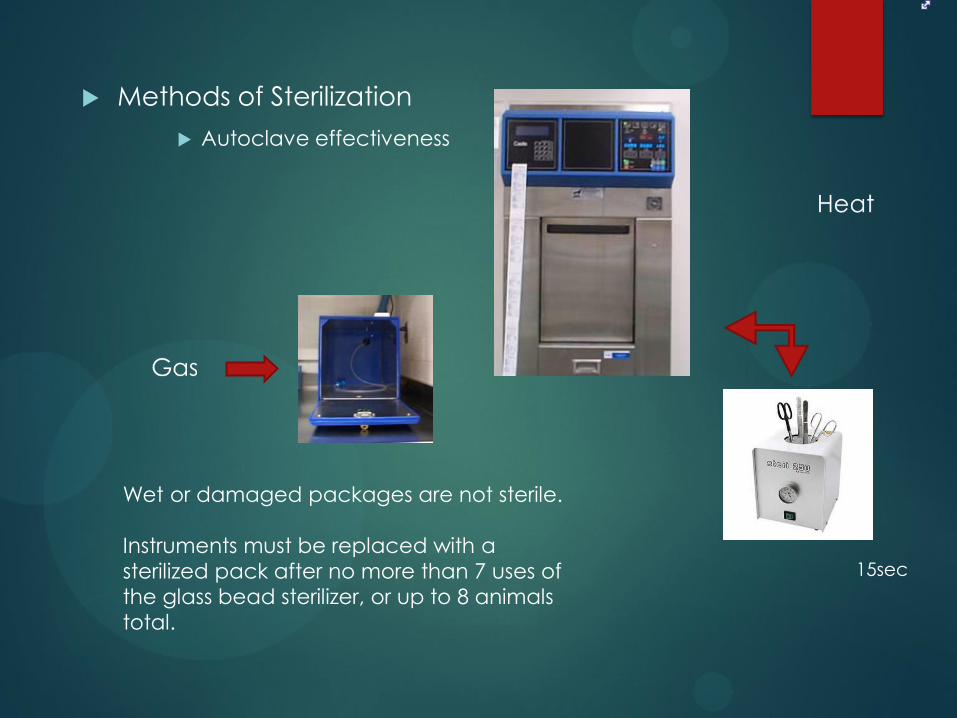
Methods of Sterilization
Autoclave effectiveness
15sec
Wet or damaged packages are not sterile.
Instruments must be replaced with a
sterilized pack after no more than 7 uses of
the glass bead sterilizer, or up to 8 animals
total.
Patient Preparation
Whenever possible, a surgical assistant should be responsible for preparing animals for surgery, as this is a mostly non-sterile process.
Ensure animal is apparently healthy.
Induce anesthesia as described in the approved IACUC protocol.
Apply sterile, ophthalmic ointment to the eyes to prevent drying, if anesthesia will last for more than 20 minutes.
Administer pre-op fluids, e.g., warm 0.9% sterile saline, as described in your protocol.
Administer analgesia, as described in your protocol.
Patient Preparation
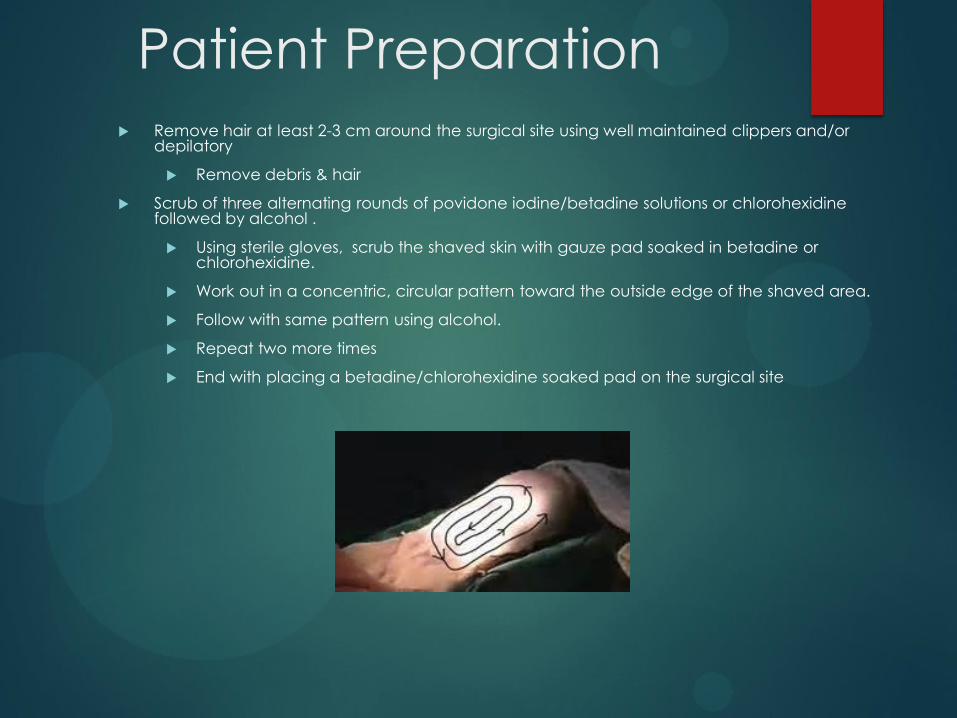
Remove hair at least 2-3 cm around the surgical site using well maintained clippers and/or depilatory
Remove debris & hair
Scrub of three alternating rounds of povidone iodine/betadine solutions or chlorohexidine followed by alcohol .
Using sterile gloves, scrub the shaved skin with gauze pad soaked in betadine or chlorohexidine.
Work out in a concentric, circular pattern toward the outside edge of the shaved area.
Follow with same pattern using alcohol.
Repeat two more times
End with placing a betadine/chlorohexidine soaked pad on the surgical site
• Three scrubs with chlorhexidine may be substituted. The third gauze pad soaked in chlorhexidine should be left in place, as above.. Finish by spraying area with betadine spray.
Wipe area with Soapy solution (Betadine)
*Start at center (Incision Site) & work in a circular pattern out to borders
Rinse with Warm Sterile Water or Alcohol
Repeat 2 more times
Spray with Betadine and cover for surgery
Surgical Preparation: The
Surgeon and Assistants
Surgical Attire
Cap
Mask
Clean lab coat
or surgical scrubs
Surgeon’s Prep
Surgeon preparation is required for survival
surgery, or for a non-survival surgery that opens a
body cavity and lasts for more than 3 hours.
Remove jewelry from the hands and wrists, tie
back long hair and roll up long sleeves.
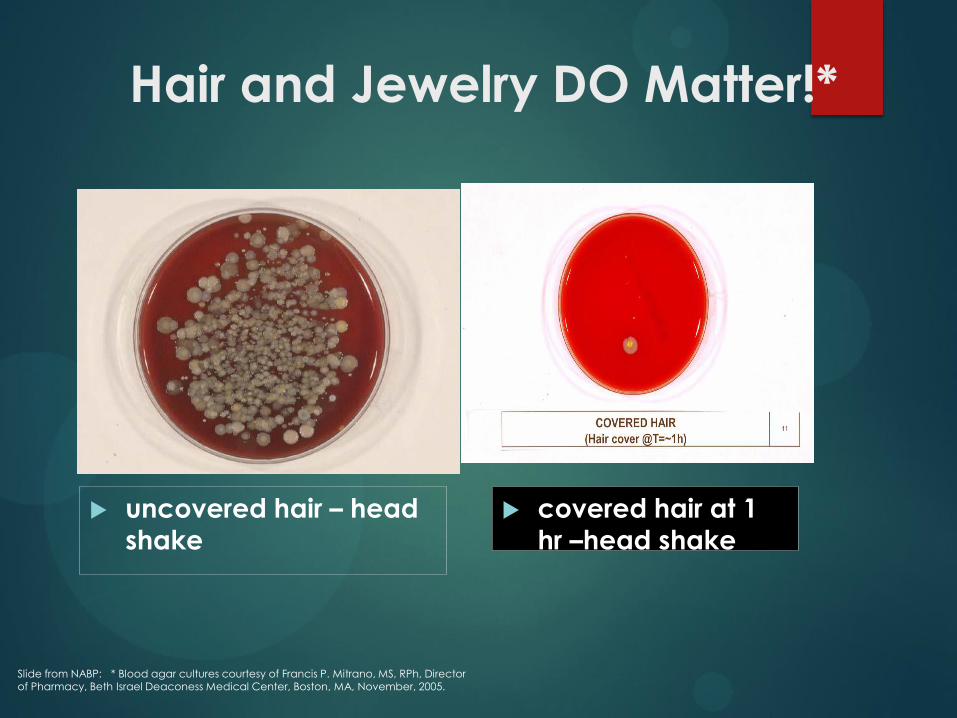
Hair and Jewelry DO Matter!*
covered hair at 1 hr –head shake
uncovered hair – head shake
Slide from NABP: * Blood agar cultures courtesy of Francis P. Mitrano, MS, RPh, Director of Pharmacy, Beth Israel Deaconess Medical Center, Boston, MA, November, 2005.
Importance of the surgical
mask
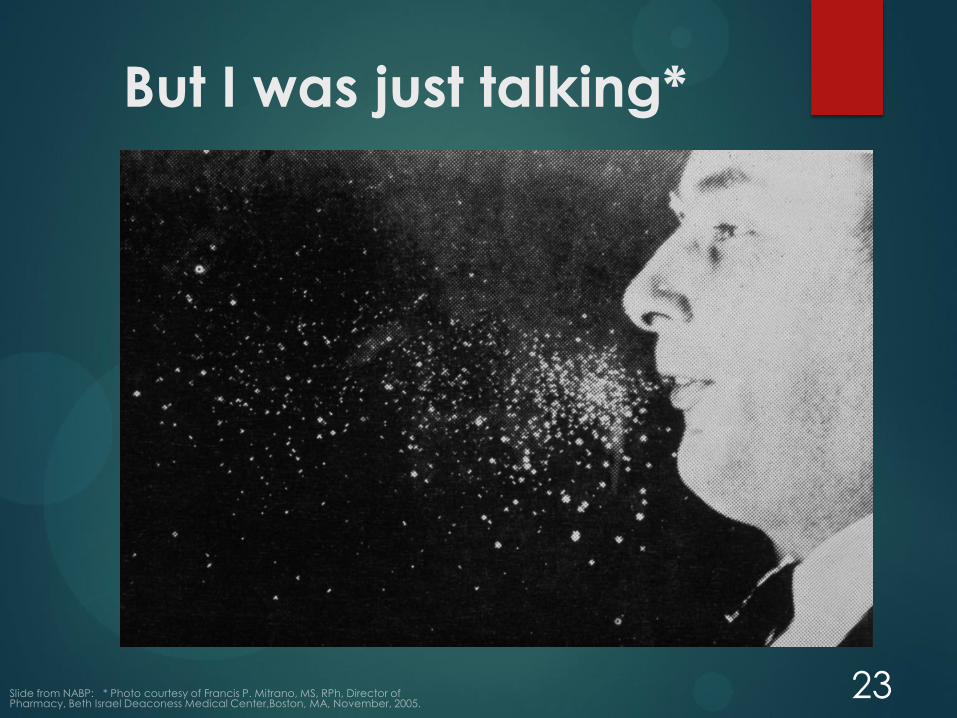
But I was just talking*
23
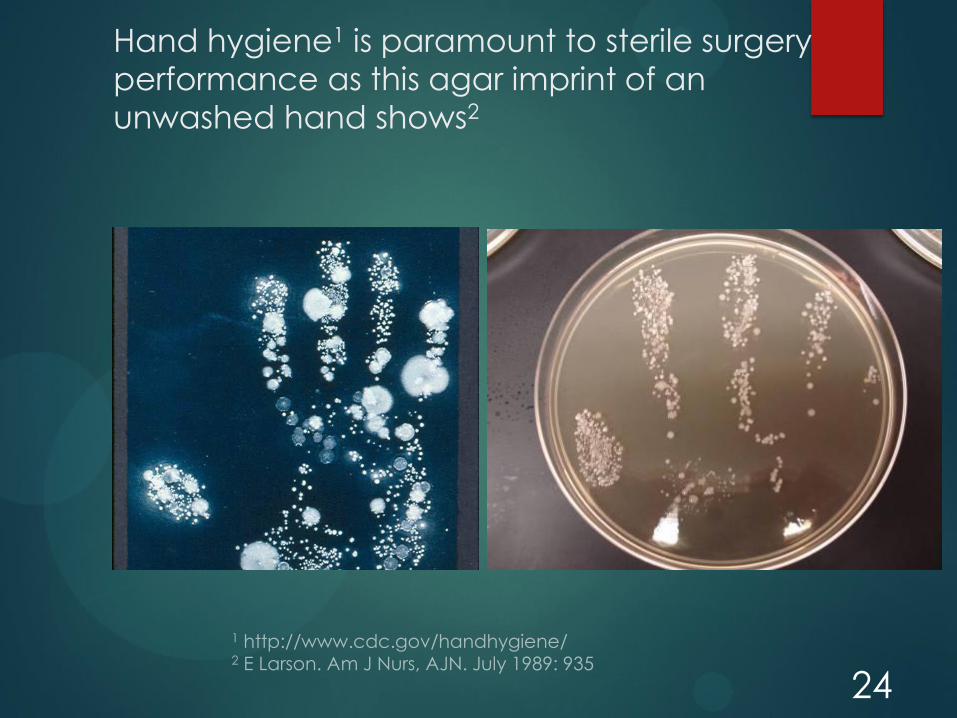
Hand hygiene1 is paramount to sterile surgery
performance as this agar imprint of an
unwashed hand shows2
24
Surgical Scrub for Hands
Surgical scrub and rinse:
5-10 minutes
Start with Fingers
Work towards the elbows
Hand Drying Technique
• Dried with a sterile hand towel
• Starting with the fingers and working to the elbows.
• Once dry, don sterile gloves

Maintaining Sterility
• Sterilely prepared people are Only allowed to
handle sterile objects
• IF a person touches an item that is not sterile .. STOP …
immediately change gloves
• Remember, only the sterile area prepared on your lab
bench or table is sterile!
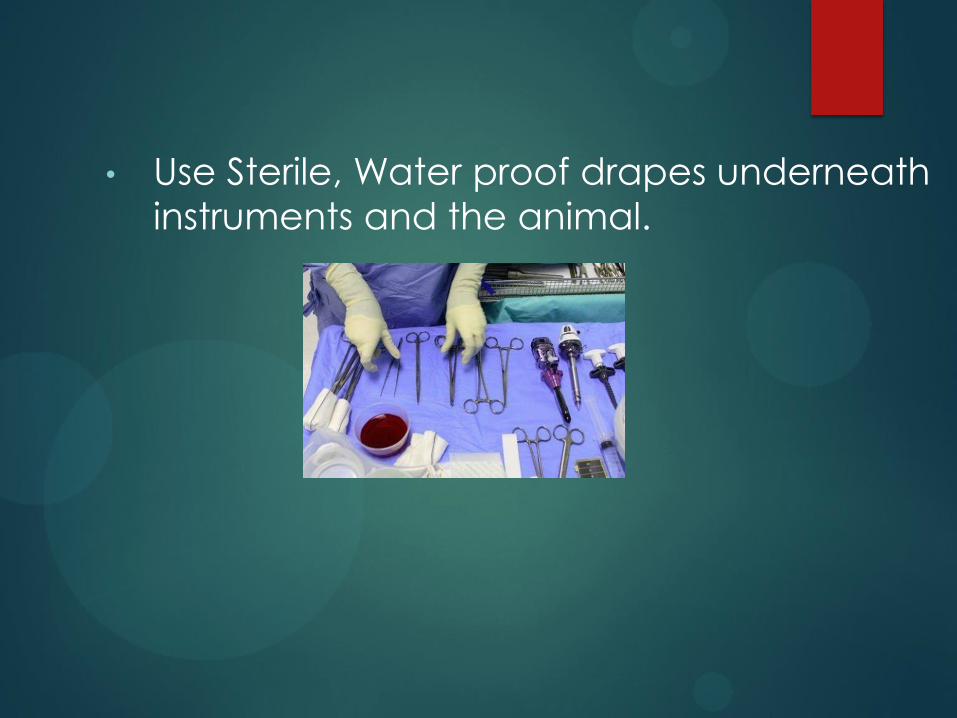
• Use Sterile, Water proof drapes underneath
instruments and the animal.
Glad Wrap Drapes
Glad’s Press’n Seal provides a sterile, inexpensive and effective method to cover the surgical field.
Although this is a food/grocery item, tests were negative for the presence of any microorganisms and organic material.
The sticky part is placed on the (entire) animal, which allows easy monitoring due to the see-through nature of this material.
Make sure the nose is exposed to avoid suffocation.
“Good Surgical Technique”
Asepsis
Correct depth of anesthesia
Warm patient
Gentle Tissue Handling
Minimal Dissection of Tissue
Appropriate use of Instruments
Effective Hemostasis
Correct use of Suture Materials & Patterns
During a procedure
Be sure to check on the animal at regular and
FREQUENT intervals
Depth of Anesthesia
Absence of a pedal withdrawal reflex
Supplement anesthesia if necessary
Warmth of the animal subject
Surgery >15-20 min – NEED contact heat source
Cloth between animal and device
Heat source: Water
circulating blanket.
Heat Source
Tissue Handling
Gentle: Handle tissues gently.
Keep tissues moist, especially if surgery is prolonged.
Minimize the creation of tissue pockets and unnecessary
dissection.
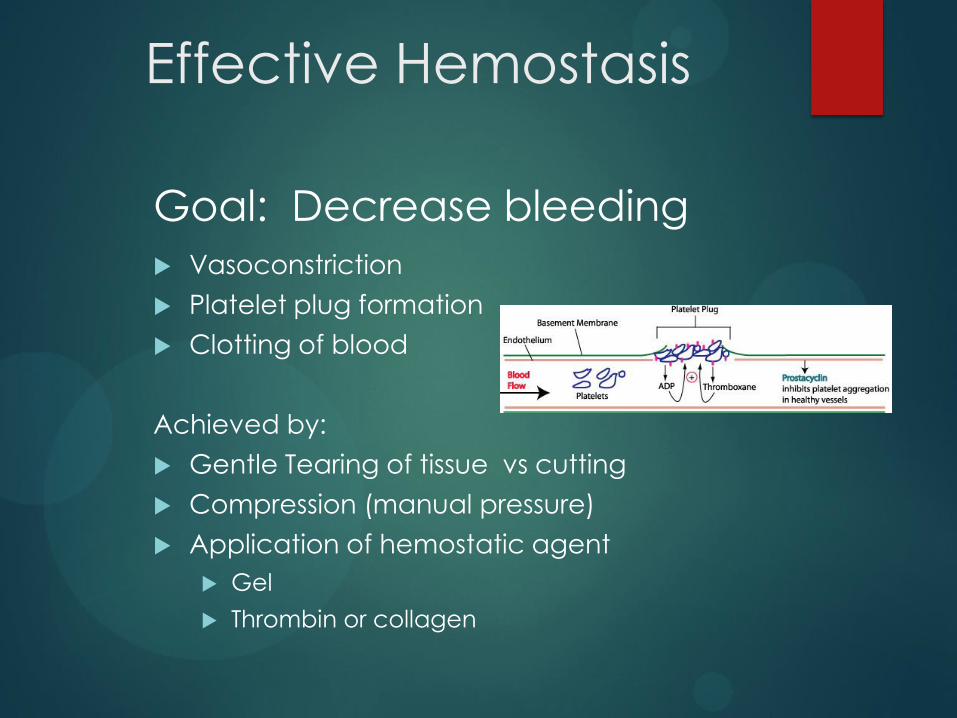
Effective Hemostasis
Goal: Decrease bleeding
Vasoconstriction
Platelet plug formation
Clotting of blood
Achieved by:
Gentle Tearing of tissue vs cutting
Compression (manual pressure)
Application of hemostatic agent
Gel
Thrombin or collagen
Tissue Closure
Tissue apposition
Decreases wound dehiscence
Improves wound healing
Proper application of suture & clip use and removal
Suture
Monofilament strongly recommended – add to
protocol as option
UAC veterinarians will be requiring that protocols
currently using other suture types move to
monofilament use at the time of protocol renewal
Suture Type
Why monofilament?
• Non-absorbable
• Less local tissue reaction to suture itself
• Does not wick material into the healing incision
• Readily accessible, many fine sizes
• Size: • Use finest size, commensurate with natural strength of
tissue
• Reinforce with retention sutures
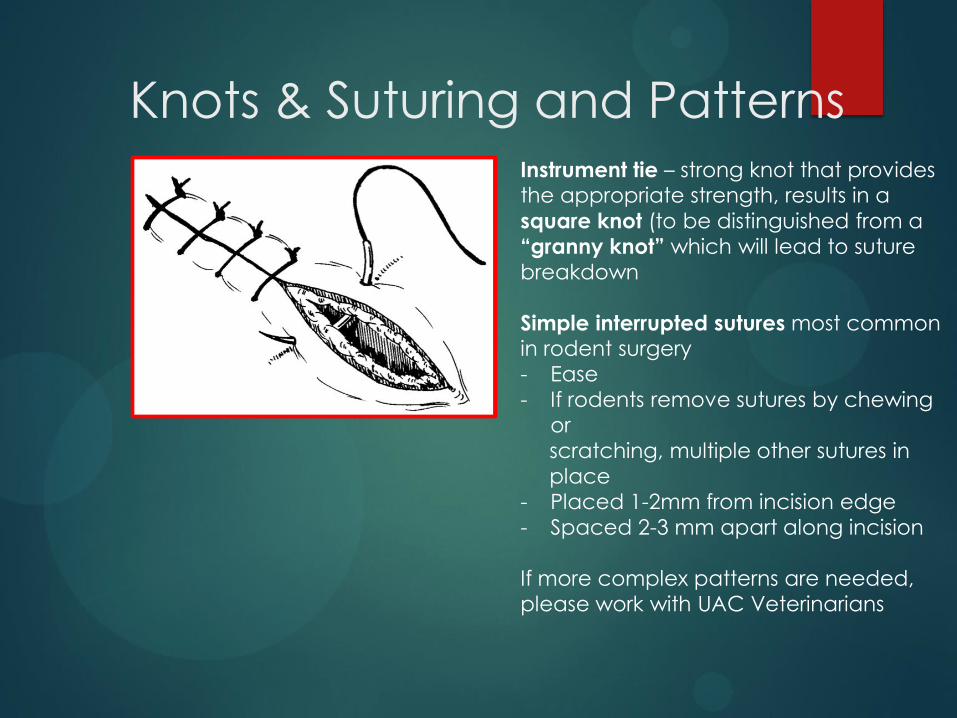
Knots & Suturing and Patterns Instrument tie – strong knot that provides the appropriate strength, results in a
square knot (to be distinguished from a
“granny knot” which will lead to suture
breakdown
Simple interrupted sutures most common in rodent surgery
- Ease
- If rodents remove sutures by chewing
or
scratching, multiple other sutures in
place
- Placed 1-2mm from incision edge
- Spaced 2-3 mm apart along incision
If more complex patterns are needed,
please work with UAC Veterinarians
Proper suture technique
http://www.youtube.com/watch?v=6P0rYS6LeZw
Recovery
Recover in warm recovery cage
Half warmed - half normal
Bedded with towel or drapes (not bedding)
Return only after moving normally
Provide warmed fluids:1-2 ml/100gm BW, SubQ, IP
OR in wetted food, or diet/hydration gel
Monitor
Post Op Procedures
Antibiotics: Systemic vs Local vs None
Not a substitute for proper aseptic surgery!
Minimum 48 hours Analgesia: Read your protocol for the
approved analgesic type. Follow what is written in the protocol. Document when and how much analgesic
was given per animal.
Monitor for Pain
Should be Bright, Alert and Active (BAA)
If depressed, anorectic, sluggish: evaluate (pain/infection)
Analgesics may cause pica - observe
Post Op Monitoring
Food & Fluid Intake:
Easy to access: Long sipper tubes, food placed on
cage bottom
Soften food with water
Provide a ‘gel’ diet to increase eating and drinking
Must acclimate 2 or more days prior to surgery
May contain the analgesics
Monitor Incision
Wound clips or sutures must be removed 10-14
days post surgery
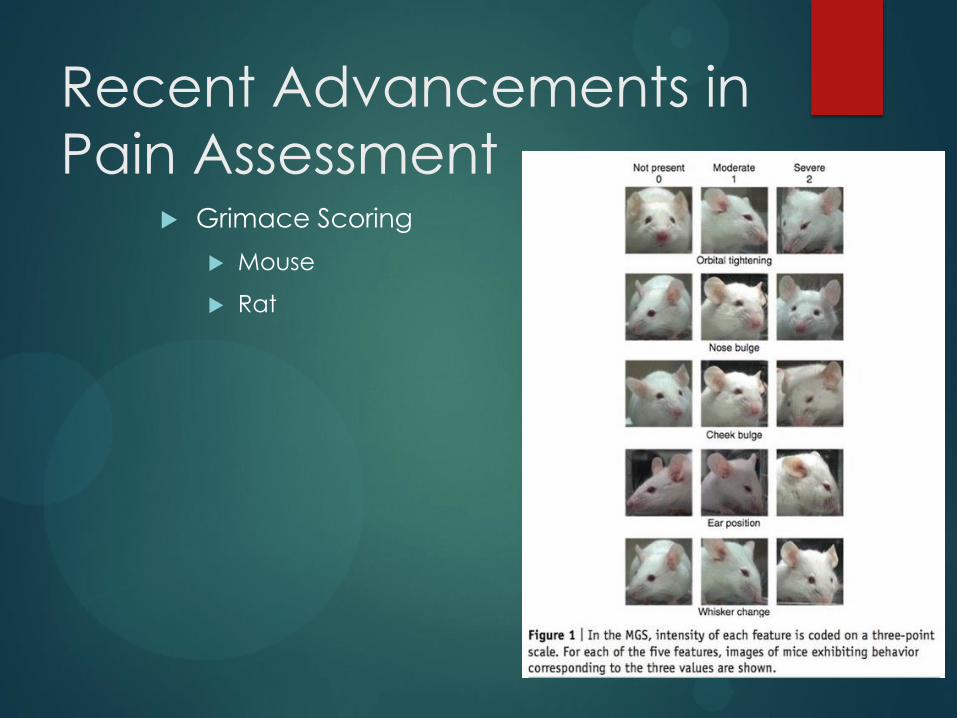
Recent Advancements in
Pain Assessment
Grimace Scoring
Mouse
Rat

Record Keeping and
approvals
Maintaining up to date records
Surgery
Post-Operative
Drug storage and usage
Submission of IACUC Amendment for ANY
change in the protocol/personnel
Documentation
Training
Surgical Records
Post-Op care
Records
Surgical/anesthetic and post-op records required that document what surgeries were performed on what animals
Analgesics need to be documented
who gave what when
Types:
Dedicated lab notebook that stays in the procedure area (lab)
Recorded in surgeon’s lab notebook – not preferred when multiple people help with post-op monitoring
Loose leaf sheets/sleeve protectors that can be stored in the vivaria where animals originate/are housed post-op – retained after study
Common Problems Surgical area:
Not dedicated
Not cleaned Non-sterile Prep of animals
Breaking sterility during the surgery: watch using devices that are not sterile. Such as drills, Stereotactic devices, operating microscopes.
No analgesics given or do not follow protocol standards. Not documenting analgesic administration.
Minimal monitoring Post-op
Not calling us with questions!
626-6702


2
PROPERTIES OF SUTURE Physical Construction of Suture Suture is any strand of material used to approximate the tissue edges and give artificial support while the tissue heals naturally. When considering a type of suture, there are three things that you need to consider. This information should be indicated somewhere on the packaging of the suture:
1. Absorbable or Non-absorbable 2. Natural or Synthetic 3. Braided (Multifilament) or Monofilament
ABSORBABLE Absorbable sutures are designed to break down over a specific time frame and be absorbed by the body. They are used when temporary support is required and the healing tissue will eventually support itself. Absorption occurs by:
- Phagocytosis and proteolysis in natural suture. - Hydrolysis in synthetic suture.
NON-ABSORBABLE: Non-absorbable sutures are designed to either be left permanently in the body or are to be removed after a certain healing period. Permanently placed, non-absorbable sutures are generally used in tissue where even though healing may occur; the new tissue may never have the needed strength to support itself. The effective tensile strength of such sutures remains high over time. When used to close skin, non-absorbable sutures are usually removed in 10-14 days, but this may vary by location and situation. NATURAL SUTURE MATERIALS Natural sutures are made from animal or plant materials. Their protein composition can elicit the most pronounced tissue reaction (inflammation) of any suture material. Their useful strength in tissue varies from a few days with Plain Catgut to several months for Silk, and can vary with the individual. SYNTHETIC SUTURE MATERIAL Sutures can be made from synthesizing a wide variety of polymers. Synthetic materials cause less tissue reaction than natural fibers, therefore their strength and absorption rate (for absorbable suture) is more uniform and predictable in all individuals. BRAIDED (MULTIFILAMENT) This construction involves several filaments or strands being braided or twisted together. This results in a strong suture that is flexible and easy to handle. Multifilament sutures pass less easily through tissue than smooth monofilaments and the resulting "tissue drag" can cause tissue trauma. Suture manufacturers have addressed this issue by coating many of the braided sutures, thus reducing the degree of “tissue drag.” The surface of a suture must be compatible with specific tissue application and have the desired knotting characteristics and capabilities. A rough suture surface can cause trauma and cutting of surrounding tissues, both of which are undesirable. Therefore, selection of materials should consider both the structure of the tissue and the surface of the suture. In principle, a suture with a rough surface can be tied with fewer knots than one with a smooth surface as knots are less likely to slip. Care must be exercised with the tying of all types of suture.
3
MONOFILAMENT This type of suture construction results in a single strand or filament. The surface is very smooth and passes easily through tissue. However, they can be difficult to handle and tie as they are less flexible than braided sutures. Most monofilaments also have “memory.” This memory results in a suture that holds the shape it had in the package, making it more difficult to work with. Some memory can be relaxed, but is not effective in all sutures.
CHOOSING THE SUTURE The following principles should guide the surgeon in suture selection: 1. WHEN A WOUND HAS REACHED MAXIMAL STRENGTH, SUTURES ARE NO LONGER NEEDED. THEREFORE
a. Tissues that ordinarily heal slowly, such as fascia and tendons, should usually be closed with nonabsorbable sutures. An absorbable suture with extended (up to 6 months) wound support may also be used.
b. Tissues that heal rapidly, such as stomach, colon, and bladder, may be closed with absorbable
sutures. 2. FOREIGN BODIES IN POTENTIALLY CONTAMINATED TISSUES MAY CONVERT CONTAMINATION TO INFECTION. THEREFORE
a. Avoid multifilament sutures, which may convert a contaminated wound into an infected one.
b. Use monofilament or absorbable sutures in potentially contaminated tissues. 3. WHERE COSMETIC RESULTS ARE IMPORTANT, CLOSE AND PROLONGED APPOSITION OF WOUNDS AND AVOIDANCE OF IRRITANTS WILL PRODUCE THE BEST RESULT. THEREFORE
a. Use the smallest inert monofilament suture materials such as nylon or polypropylene.
b. Avoid skin sutures and close subcuticularly, whenever possible.
c. Under certain circumstances, to secure close apposition of skin edges, a topical skin adhesive such as Dermabond Topical Skin Adhesive, or Vetbond may be used.
4. FOREIGN BODIES IN THE PRESENCE OF FLUIDS CONTAINING HIGH CONCENTRATIONS OF CRYSTALLOIDS MAY ACT AS A NIDUS FOR PRECIPITATION AND STONE FORMATION. THEREFORE
a. In the urinary and biliary tract, use rapidly absorbed sutures. 5. REGARDING SUTURE SIZE
a. Use the finest size, commensurate with the natural strength of the tissue.
b. If the postoperative course of the patient may produce sudden strains on the suture line, reinforce it with retention sutures. Remove them as soon as the animal’s condition is stabilized.
4
In summary, when choosing the suture, consider that many factors contribute to the choice of materials and techniques for wound closure. The final choice is often a compromise of several of those factors and may be combined with personal preference based on past experience. Thus, consider…
How long is the suture to be wholly or partially responsible for the strength of the wound? How does the suture material affect the tissue and the process of healing? How great is the risk of infection? Is absolute fixation needed or is certain mobility acceptable, or even desirable? What dimension of suture is necessary to obtain the desired degree of fixation? What strength of suture is required? Is the material flexible enough for the given purpose and is it possible to knot it in the space
provided?
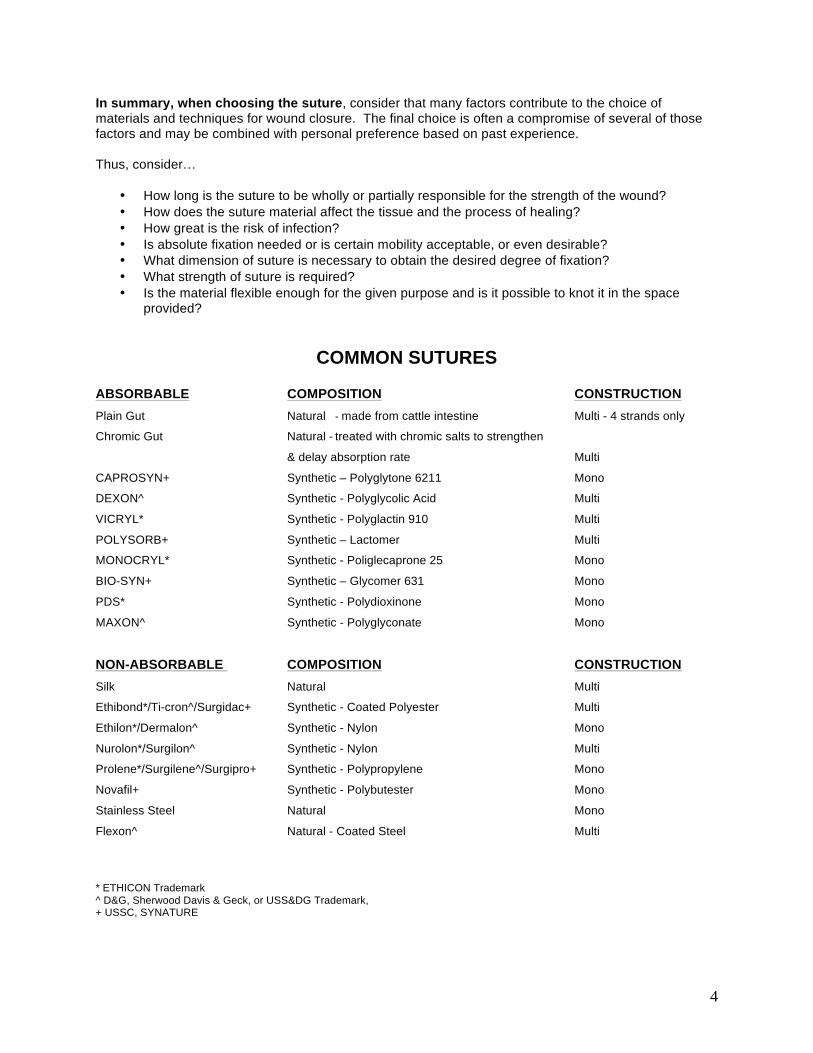
COMMON SUTURES ABSORBABLE COMPOSITION CONSTRUCTION Plain Gut Natural - made from cattle intestine Multi - 4 strands only
Chromic Gut Natural - treated with chromic salts to strengthen
& delay absorption rate Multi
CAPROSYN+ Synthetic – Polyglytone 6211 Mono
DEXON^ Synthetic - Polyglycolic Acid Multi
VICRYL* Synthetic - Polyglactin 910 Multi
POLYSORB+ Synthetic – Lactomer Multi
MONOCRYL* Synthetic - Poliglecaprone 25 Mono
BIO-SYN+ Synthetic – Glycomer 631 Mono
PDS* Synthetic - Polydioxinone Mono
MAXON^ Synthetic - Polyglyconate Mono
NON-ABSORBABLE COMPOSITION CONSTRUCTION Silk Natural Multi
Ethibond*/Ti-cron^/Surgidac+ Synthetic - Coated Polyester Multi
Ethilon*/Dermalon^ Synthetic - Nylon Mono
Nurolon*/Surgilon^ Synthetic - Nylon Multi
Prolene*/Surgilene^/Surgipro+ Synthetic - Polypropylene Mono
Novafil+ Synthetic - Polybutester Mono
Stainless Steel Natural Mono
Flexon^ Natural - Coated Steel Multi
* ETHICON Trademark ^ D&G, Sherwood Davis & Geck, or USS&DG Trademark, + USSC, SYNATURE
5
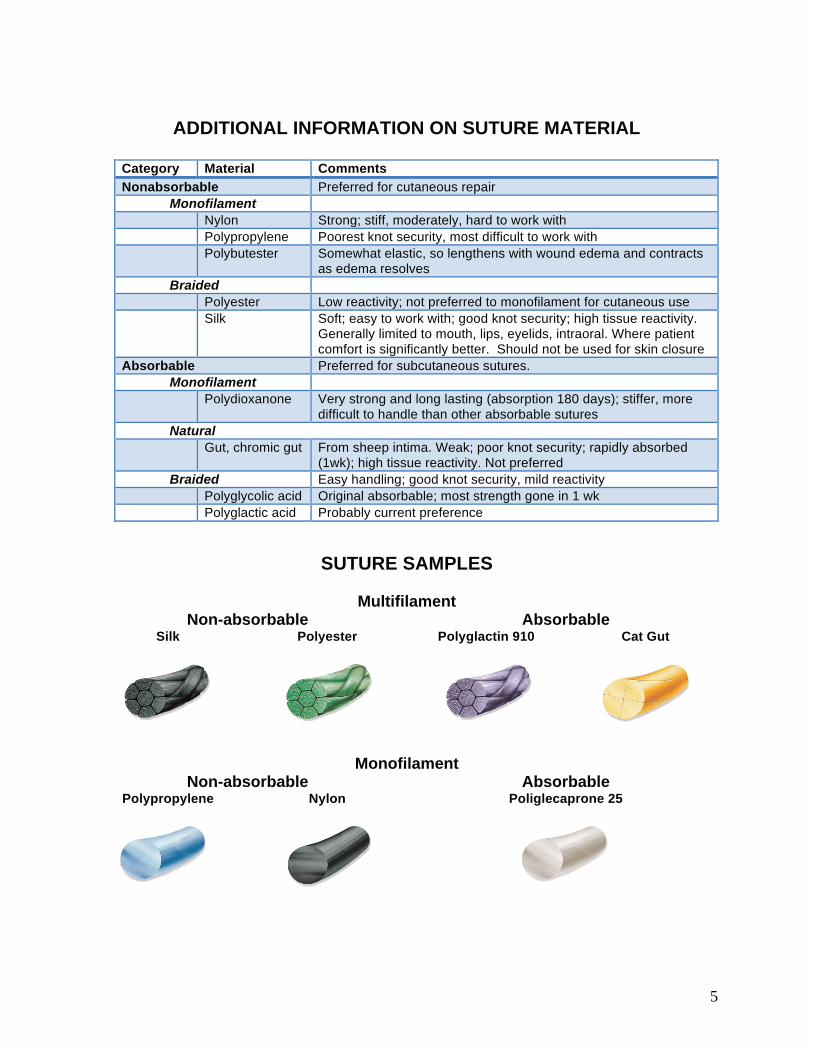
ADDITIONAL INFORMATION ON SUTURE MATERIAL
Category Material Comments Nonabsorbable Preferred for cutaneous repair
Monofilament Nylon Strong; stiff, moderately, hard to work with Polypropylene Poorest knot security, most difficult to work with Polybutester Somewhat elastic, so lengthens with wound edema and contracts
as edema resolves Braided
Polyester Low reactivity; not preferred to monofilament for cutaneous use Silk Soft; easy to work with; good knot security; high tissue reactivity.
Generally limited to mouth, lips, eyelids, intraoral. Where patient comfort is significantly better. Should not be used for skin closure
Absorbable Preferred for subcutaneous sutures. Monofilament
Polydioxanone Very strong and long lasting (absorption 180 days); stiffer, more difficult to handle than other absorbable sutures
Natural Gut, chromic gut From sheep intima. Weak; poor knot security; rapidly absorbed
(1wk); high tissue reactivity. Not preferred Braided Easy handling; good knot security, mild reactivity
Polyglycolic acid Original absorbable; most strength gone in 1 wk Polyglactic acid Probably current preference
SUTURE SAMPLES
Multifilament Non-absorbable Absorbable
Silk Polyester Polyglactin 910 Cat Gut
Monofilament Non-absorbable Absorbable
Polypropylene Nylon Poliglecaprone 25

6
SUTURE ABSORBABLE NON-ABSORBABLE
7
SUTURE SIZING
Suture is available from a "7" (Heaviest) to "11 - 0" (Finest). The important factor in deciding suture size is the relationship between the tensile strength of the suture, and the tissue to be sutured. Tensile strength of the wound need only match or slightly exceed the holding power of the tissue to be sutured. For example, you don't need a rope to tie your shoes... it might work, but its overkill. A shoelace would do. Finer diameter sutures make smaller knots, provide less tissue reaction, and result in minimal scar formation. Finer stands are very flexible, easy to handle, but do require gentle tying. Closely placed, fine sutures create a stronger suture line than widely spaced, heavy sutures. Tissue drag is also closely related to gauge; the finer the gauge, the less tissue trauma is caused by the passage of the suture.
Finest <<<<---------------------------------------------------------------------------------------->>>> Largest
11-0 10-0 9-0 8-0 7-0 6-0 5-0 4-0 3-0 2-0 0 1 2 3 4 5 6 7
Weakest <<<<--------------------------------------------------------------------------------------->>>> Strongest
SKIN SUTURE SELECTION The skin is one area where the final result, based on your selection of suture and your technical skill, will be the most evident to your patient. Make informed choices that will give the best result possible. Stitches that are tied too tight and are left in too long may leave “hatch marks” on either side of the scar. The hole made by the stitch may rip and become larger with increased tension on the wound (i.e. swelling). Sometimes, these marks are more noticeable long term than the scar itself. PERCUTANEOUS (TRANSCUTANEOUS) SUTURE (e.g. simple, interrupted pattern)
Recommendation: SYNTHETIC, NON-ABSORBABLE, MONOFILAMENT Example: NOVAFIL, PROLENE, SURGI-PRO, SURGILENE, DERMALON, STAINLES STEEL
Possible Alternative: SYNTHETIC, ABSORBABLE, MONOFILAMENT Example: MONOCRYL, MAXON, PDS, BIO-SYN
Unsuitable: Organic or synthetic, braided absorbable materials
Example: SILK, DEXON, VICRYL
SIZE: Suggest 3-0 or 4-0 for rats, 4-0 or 5-0 for mice depending on size but will vary NEEDLE: Reverse cutting, 3/8 curve Comments: Percutaneous sutures should be tied loosely to barely appose wound edges; otherwise, postoperative swelling may cause the suture to be too tight, strangle cutaneous vessels and lead to pain, infection and wound failure.
INTRACUTANEOUS (SUBCUTICULAR) SUTURE
Recommendation: Continuous (generally preferred) or interrupted pattern with SYNTHETIC, ABSORBABLE (uncoloured) MONO or MULTIFILAMENT
8
Example: MONOCRYL, MAXON, PDS (Monofilament); DEXON, VICRYL (Multifilament)
Possible Alternative: A continuous pattern with SYNTHETIC, NON-ABSORBABLE, MONOFILAMENT (to be removed)
Example: NOVAFIL, PROLENE, SURGILENE
SIZE: Suggest 3-0 or 4-0 for rats, 4-0 or 5-0 for mice depending on size but will vary NEEDLE: Reverse cutting, 3/8 curve
Comments: Intracutaneous suturing has the advantage of completely avoiding stitch marks. It can be used with advantage where cosmetic aspects are especially important. If synthetic absorbable materials are used, it is quite common that temporary nodules appear under the scar a couple of weeks after suturing. These disappear spontaneously in the course of months as the suture breaks down and absorbs.
SUBCUTANEOUS (FAT LAYER) SUTURE
Recommendation: Generally no suture but may be warranted if excess skin tension. Continuous (generally preferred) or interrupted pattern with SYNTHETIC, ABSORBABLE (uncoloured) MONO or MULTIFILAMENT
Example: MONOCRYL, MAXON, PDS (Monofilament); DEXON, VICRYL (Multifilament)
SIZE: Suggest 3-0 or 4-0 for rats, 4-0 or 5-0 for mice depending on size but will vary NEEDLE: Taper, 3/8, 1/2, 5/8 curve Comments: The subcutaneous fat is the tissue with the least resistance to infection and so, it’s best to avoid introduction of foreign materials, like suture. If the tissue is reasonably elastic, good apposition is obtained spontaneously. However, do not leave a DEAD SPACE as this can cause greater problems. This tissue must be gently approximated.
THE SURGICAL NEEDLE
9
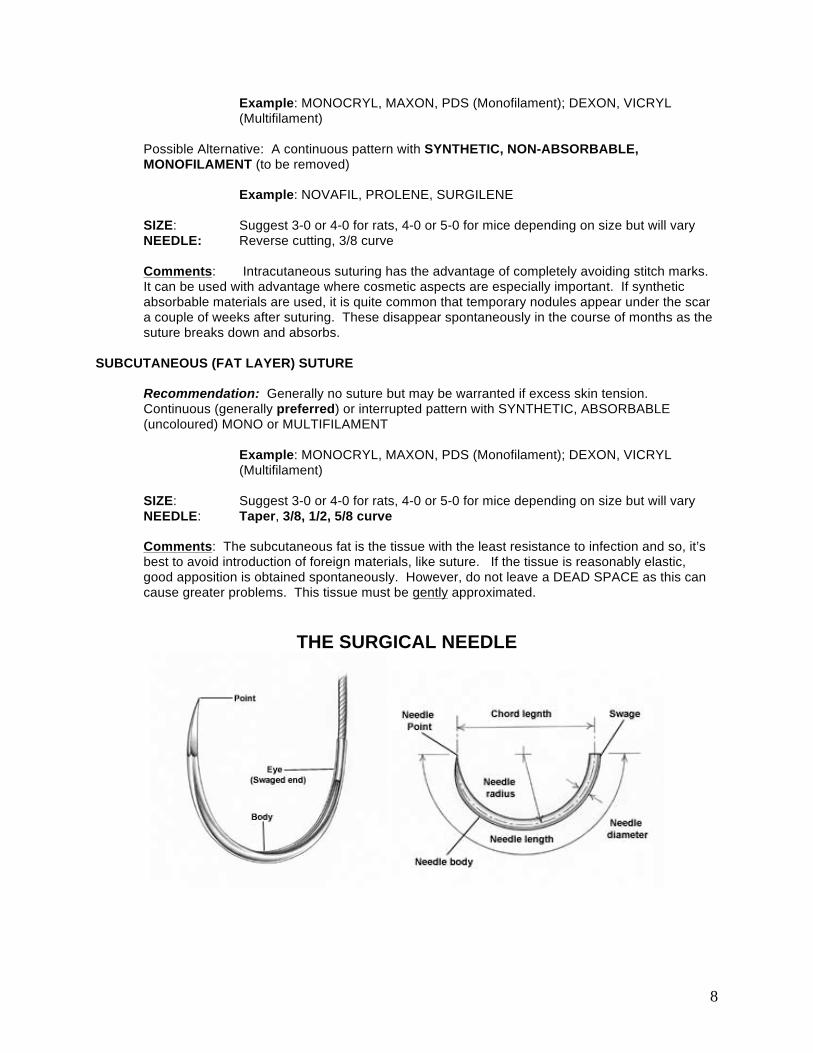
Regardless of its intended use, every surgical needle has three basic components:
a. The eye. b. The body. c. The point.
The measurements of these specific components determine, in part, how they will be used most efficiently. Needle size may be measured in inches or in metric units. The following measurements determine the size of a needle.
a. CHORD LENGTH--The straight line distance from the point of a curved needle to the swage. b. NEEDLE LENGTH--The distance measured along the needle itself from point to end. c. RADIUS--The distance from the center of the circle to the body of the needle if the curvature of
the needle were continued to make a full circle. d. DIAMETER--The gauge or thickness of the needle wire. Very small needles of fine gauge are
needed for microsurgery. Large, heavy gauge needles are used in large animals to penetrate the sternum and to place retention sutures in the abdominal wall. A broad spectrum of sizes are available between the two extremes.
10
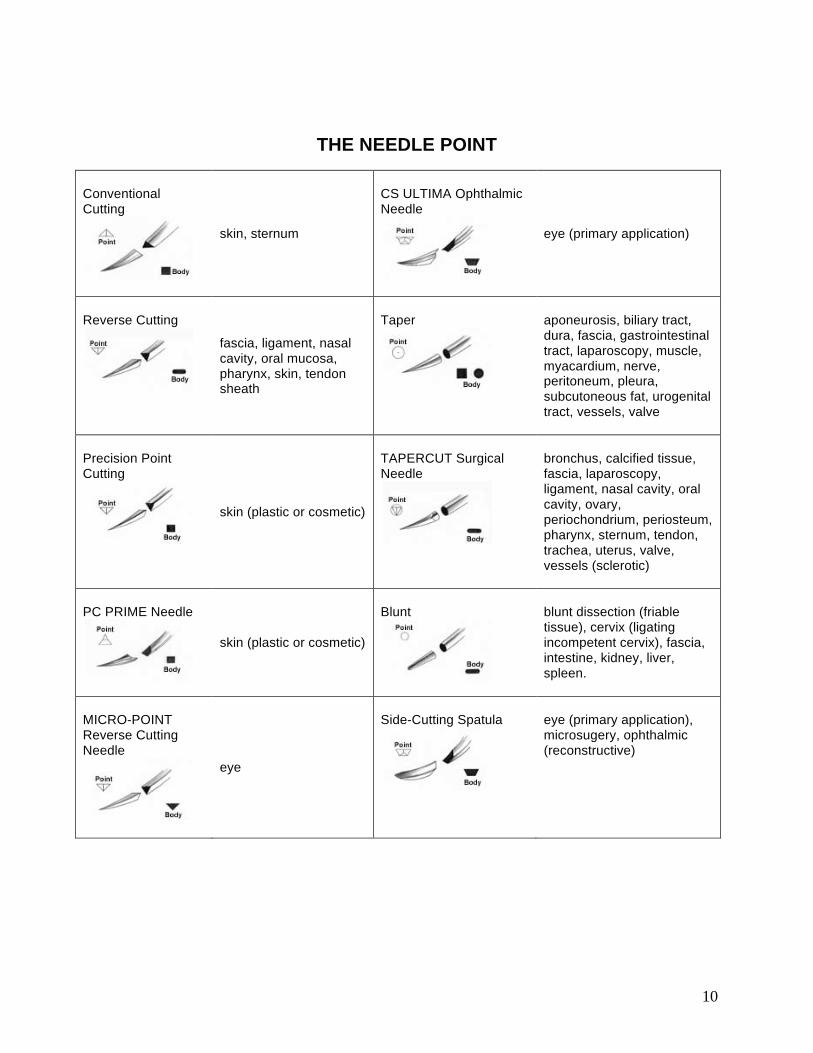
THE NEEDLE POINT
Conventional Cutting
skin, sternum
CS ULTIMA Ophthalmic Needle
eye (primary application)
Reverse Cutting
fascia, ligament, nasal cavity, oral mucosa, pharynx, skin, tendon sheath
Taper
aponeurosis, biliary tract, dura, fascia, gastrointestinal tract, laparoscopy, muscle, myacardium, nerve, peritoneum, pleura, subcutoneous fat, urogenital tract, vessels, valve
Precision Point Cutting
skin (plastic or cosmetic)
TAPERCUT Surgical Needle
bronchus, calcified tissue, fascia, laparoscopy, ligament, nasal cavity, oral cavity, ovary, periochondrium, periosteum, pharynx, sternum, tendon, trachea, uterus, valve, vessels (sclerotic)
PC PRIME Needle
skin (plastic or cosmetic)
Blunt
blunt dissection (friable tissue), cervix (ligating incompetent cervix), fascia, intestine, kidney, liver, spleen.
MICRO-POINT Reverse Cutting Needle
eye
Side-Cutting Spatula
eye (primary application), microsugery, ophthalmic (reconstructive)
11
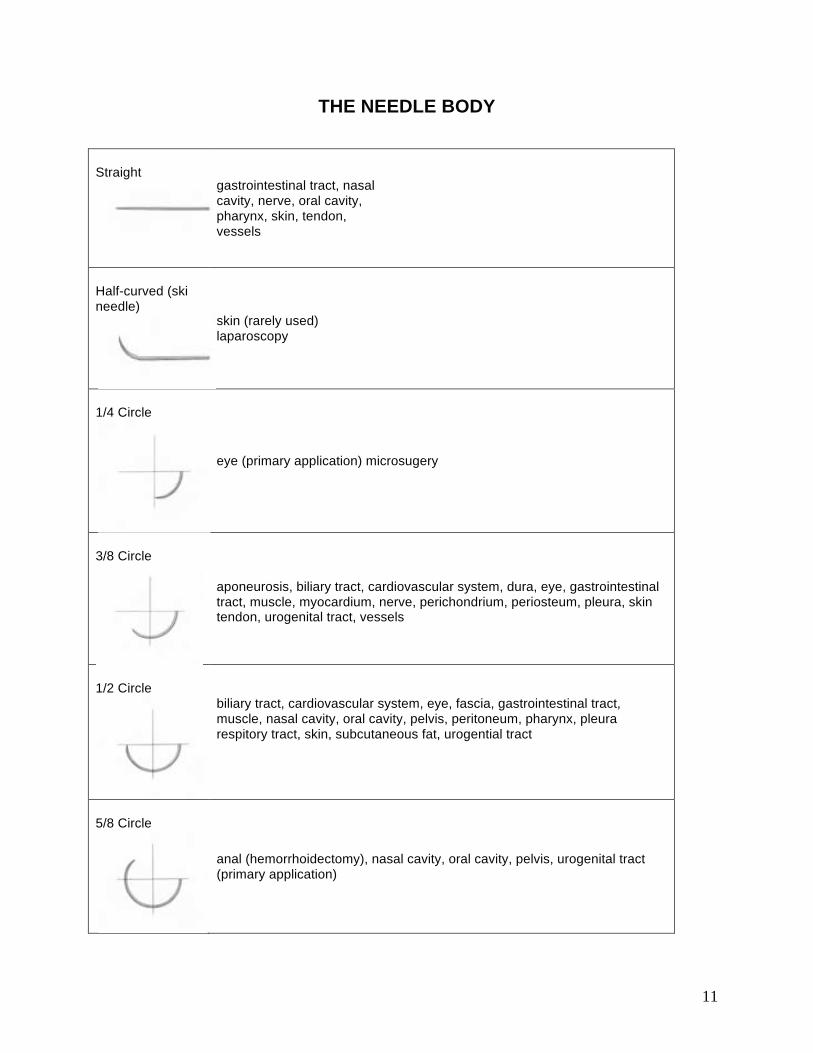
THE NEEDLE BODY
Straight
gastrointestinal tract, nasal cavity, nerve, oral cavity, pharynx, skin, tendon, vessels
Half-curved (ski needle)
skin (rarely used) laparoscopy
1/4 Circle
eye (primary application) microsugery
3/8 Circle
aponeurosis, biliary tract, cardiovascular system, dura, eye, gastrointestinal tract, muscle, myocardium, nerve, perichondrium, periosteum, pleura, skin tendon, urogenital tract, vessels
1/2 Circle
biliary tract, cardiovascular system, eye, fascia, gastrointestinal tract, muscle, nasal cavity, oral cavity, pelvis, peritoneum, pharynx, pleura respitory tract, skin, subcutaneous fat, urogential tract
5/8 Circle
anal (hemorrhoidectomy), nasal cavity, oral cavity, pelvis, urogenital tract (primary application)
12
CHOOSING THE NEEDLE
One basic assumption must be made in considering the ideal surgical needle for a given application, namely, that the tissue being sutured should be altered as little as possible by the needle since the only purpose of the needle is to introduce the suture into the tissue for apposition. While there are no hard and fast rules governing needle selection, the following principles should be kept in mind:
a. Consider the tissue in which the surgeon will introduce the needle. Generally speaking, taper point needles are most often used to suture tissues that are easy to penetrate. Cutting or TAPERCUT needles are more often used in tough, hard-to-penetrate tissues. When in doubt about whether to choose a taper point or cutting needle, choose the taper point for everything except skin sutures.
b. Select the length, diameter, and curvature of the needle according to the desired placement of the suture and the space in which the surgeon is working.
c. When using eyed needles, try to match needle diameter to suture size. Swaged needles, where the needle is already attached to the suture strand, eliminate this concern.
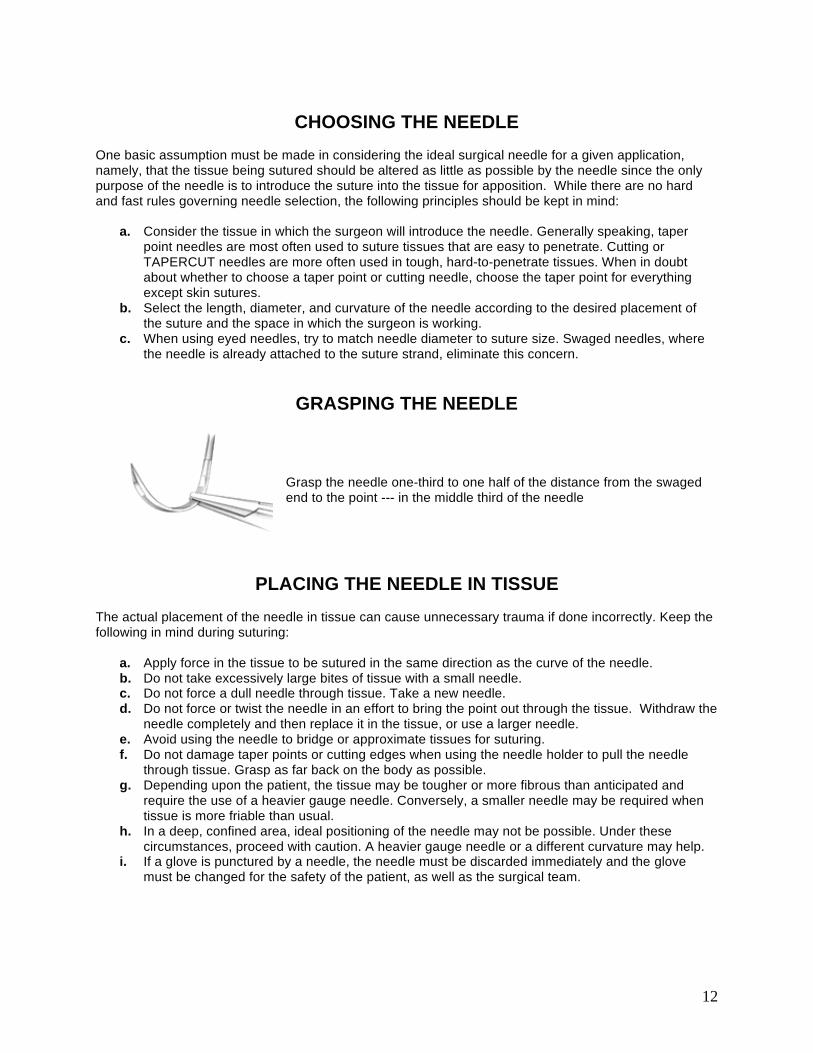
GRASPING THE NEEDLE
Grasp the needle one-third to one half of the distance from the swaged end to the point --- in the middle third of the needle
PLACING THE NEEDLE IN TISSUE
The actual placement of the needle in tissue can cause unnecessary trauma if done incorrectly. Keep the following in mind during suturing:
a. Apply force in the tissue to be sutured in the same direction as the curve of the needle. b. Do not take excessively large bites of tissue with a small needle. c. Do not force a dull needle through tissue. Take a new needle. d. Do not force or twist the needle in an effort to bring the point out through the tissue. Withdraw the
needle completely and then replace it in the tissue, or use a larger needle. e. Avoid using the needle to bridge or approximate tissues for suturing. f. Do not damage taper points or cutting edges when using the needle holder to pull the needle
through tissue. Grasp as far back on the body as possible. g. Depending upon the patient, the tissue may be tougher or more fibrous than anticipated and
require the use of a heavier gauge needle. Conversely, a smaller needle may be required when tissue is more friable than usual.
h. In a deep, confined area, ideal positioning of the needle may not be possible. Under these circumstances, proceed with caution. A heavier gauge needle or a different curvature may help.
i. If a glove is punctured by a needle, the needle must be discarded immediately and the glove must be changed for the safety of the patient, as well as the surgical team.
13
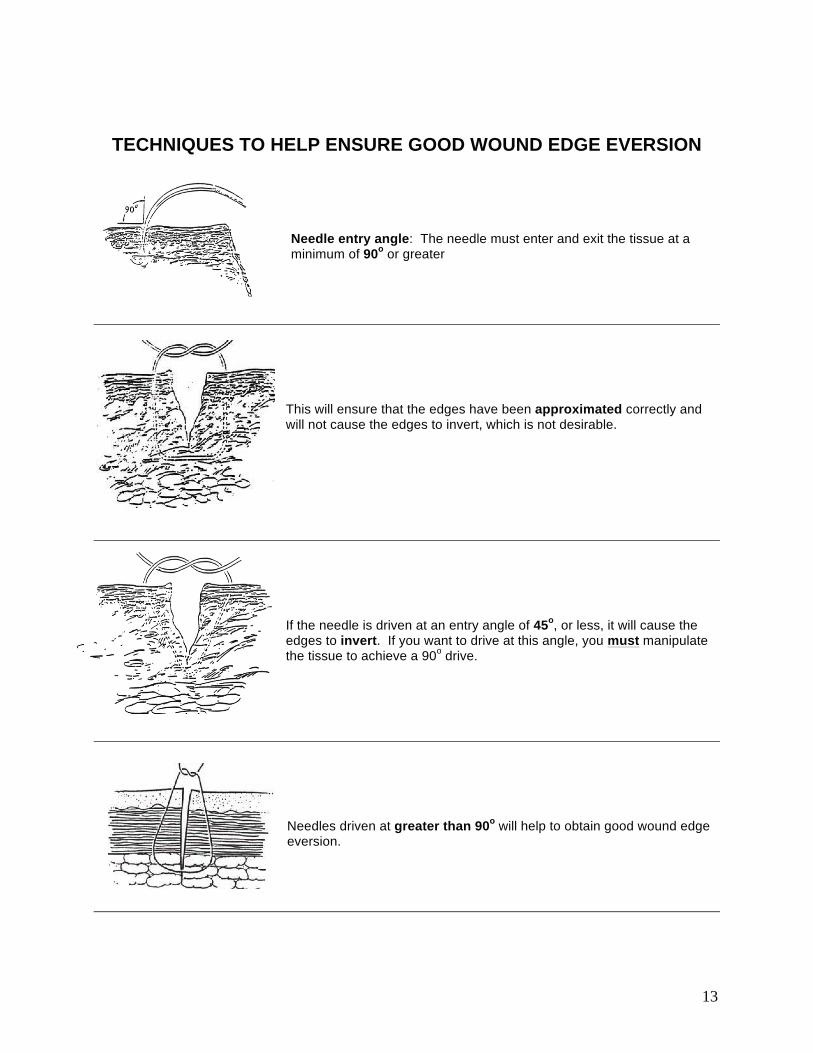
TECHNIQUES TO HELP ENSURE GOOD WOUND EDGE EVERSION Needle entry angle: The needle must enter and exit the tissue at a minimum of 90o or greater
This will ensure that the edges have been approximated correctly and will not cause the edges to invert, which is not desirable.
If the needle is driven at an entry angle of 45o, or less, it will cause the edges to invert. If you want to drive at this angle, you must manipulate the tissue to achieve a 90o drive.
Needles driven at greater than 90o will help to obtain good wound edge eversion.
14
TISSUE HANDLING Minimal trauma to tissues is fundamentally important for optimal wound healing. This requires that:
Tissues are handled carefully using delicate instruments Tissues are not strangulated and made ischemic by sutures Wound edges are loosely coapted since there is always some postoperative swelling Dead space is avoided
KNOT TYING The general principles of knot tying which apply to all suture materials are:
a. The completed knot must be firm to virtually eliminate slippage. The simplest knot for the material used is the most desirable.
b. Tie the knot as small as possible and cut the ends as short as possible. This helps to prevent excessive tissue reaction toward absorbable sutures and to minimize foreign body reaction to nonabsorbable sutures.
c. Avoid friction. "Sawing" between strands may weaken suture integrity. d. Avoid damage to the suture material during handling, especially when using surgical instruments
in instrument ties. e. Avoid excessive tension, which may break sutures and cut tissue. Practice will lead to successful
use of finer gauge materials. f. Do not tie sutures used for tissue approximation too tightly, as this may contribute to tissue
strangulation. Approximate-- do not strangulate. g. Maintain traction at one end of the strand after the first loop is tied to avoid loosening of the throw. h. Make the final throw as nearly horizontal as possible. i. Do not hesitate to change stance or position in relation to the patient in order to place a knot
securely and flat. j. Extra throws do not add to the strength of a properly tied knot, only to its bulk. Some procedures
involve tying knots with the fingers, using one or two hands; others involve tying with the help of instruments. Perhaps the most complex method of knot tying is done during endoscopic procedures, when the surgeon must manipulate instruments from well outside the body cavity.
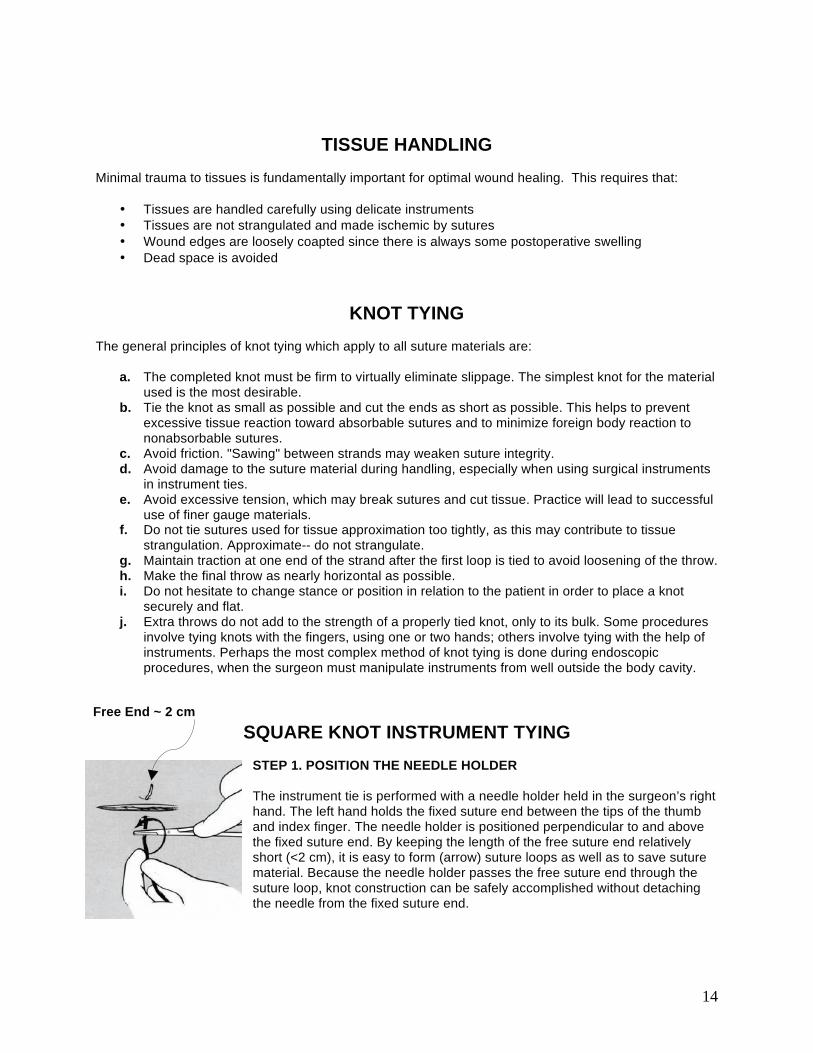
SQUARE KNOT INSTRUMENT TYING
STEP 1. POSITION THE NEEDLE HOLDER The instrument tie is performed with a needle holder held in the surgeon’s right hand. The left hand holds the fixed suture end between the tips of the thumb and index finger. The needle holder is positioned perpendicular to and above the fixed suture end. By keeping the length of the free suture end relatively short (<2 cm), it is easy to form (arrow) suture loops as well as to save suture material. Because the needle holder passes the free suture end through the suture loop, knot construction can be safely accomplished without detaching the needle from the fixed suture end.
Free End ~ 2 cm
15
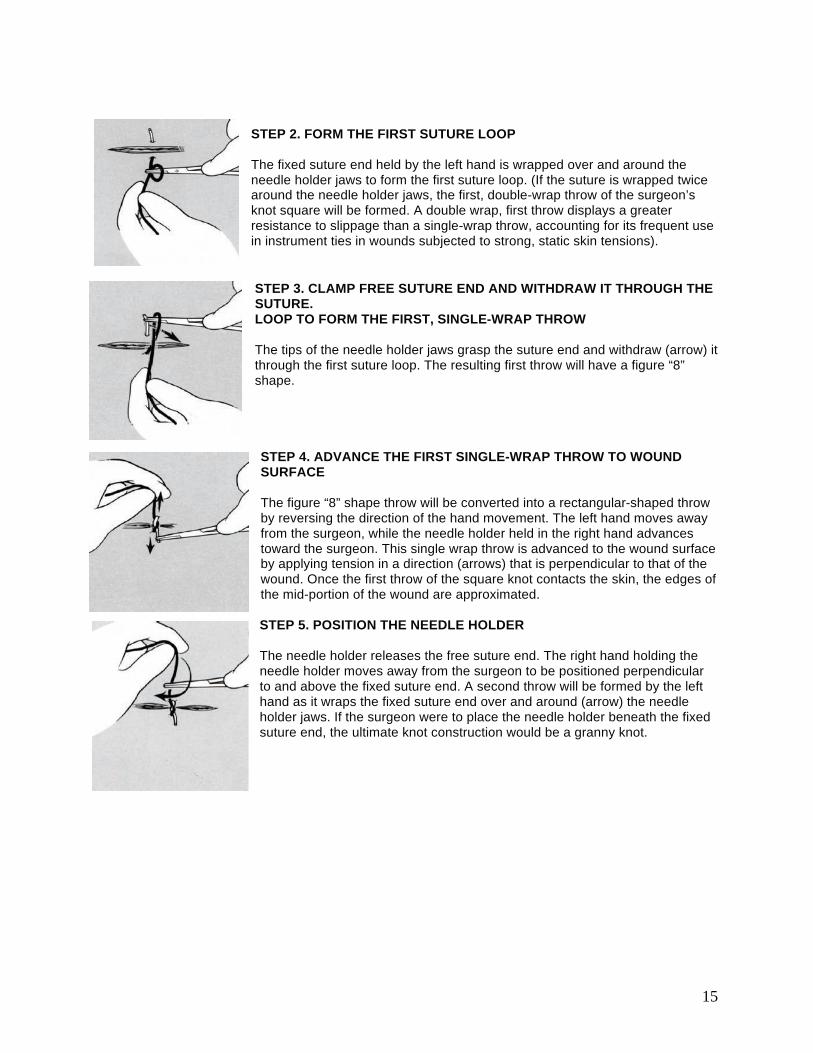
STEP 2. FORM THE FIRST SUTURE LOOP The fixed suture end held by the left hand is wrapped over and around the needle holder jaws to form the first suture loop. (If the suture is wrapped twice around the needle holder jaws, the first, double-wrap throw of the surgeon’s knot square will be formed. A double wrap, first throw displays a greater resistance to slippage than a single-wrap throw, accounting for its frequent use in instrument ties in wounds subjected to strong, static skin tensions). STEP 3. CLAMP FREE SUTURE END AND WITHDRAW IT THROUGH THE SUTURE. LOOP TO FORM THE FIRST, SINGLE-WRAP THROW The tips of the needle holder jaws grasp the suture end and withdraw (arrow) it through the first suture loop. The resulting first throw will have a figure “8” shape. STEP 4. ADVANCE THE FIRST SINGLE-WRAP THROW TO WOUND SURFACE The figure “8” shape throw will be converted into a rectangular-shaped throw by reversing the direction of the hand movement. The left hand moves away from the surgeon, while the needle holder held in the right hand advances toward the surgeon. This single wrap throw is advanced to the wound surface by applying tension in a direction (arrows) that is perpendicular to that of the wound. Once the first throw of the square knot contacts the skin, the edges of the mid-portion of the wound are approximated. STEP 5. POSITION THE NEEDLE HOLDER The needle holder releases the free suture end. The right hand holding the needle holder moves away from the surgeon to be positioned perpendicular to and above the fixed suture end. A second throw will be formed by the left hand as it wraps the fixed suture end over and around (arrow) the needle holder jaws. If the surgeon were to place the needle holder beneath the fixed suture end, the ultimate knot construction would be a granny knot.
16
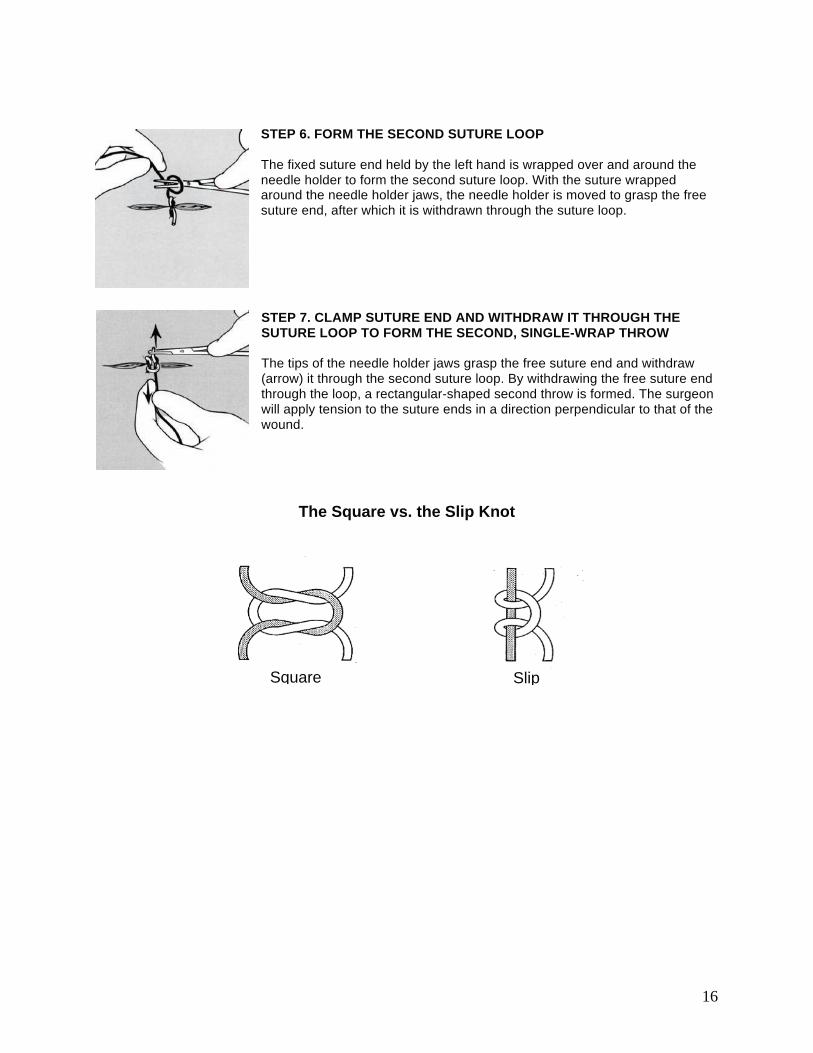
STEP 6. FORM THE SECOND SUTURE LOOP The fixed suture end held by the left hand is wrapped over and around the needle holder to form the second suture loop. With the suture wrapped around the needle holder jaws, the needle holder is moved to grasp the free suture end, after which it is withdrawn through the suture loop. STEP 7. CLAMP SUTURE END AND WITHDRAW IT THROUGH THE SUTURE LOOP TO FORM THE SECOND, SINGLE-WRAP THROW The tips of the needle holder jaws grasp the free suture end and withdraw (arrow) it through the second suture loop. By withdrawing the free suture end through the loop, a rectangular-shaped second throw is formed. The surgeon will apply tension to the suture ends in a direction perpendicular to that of the wound.
The Square vs. the Slip Knot
Square Slip
17
When suturing…DO
a. Pass the surgical needle swaged to a suture through the wound edges in a direction toward you.
b. Construct a two-throw square knot that can be advanced to the wound edge, providing a preview
of the ultimate apposition of the wound edges.
c. Approximate the edges of the divided tissue without strangulating the tissue encircled by the
suture loop.
d. Once meticulous apposition of the wound edges is achieved, construct a knot that has sufficient
number of throws that allow it to fail by breakage rather than by slippage.
e. Position your hands on each side and parallel to the suture loop.
f. Apply opposing forces to the knot “ears” that are equal in magnitude and in a plane parallel to that
of the wound surface.
g. After each throw, reverse the position of your hands that apply tension to the suture ends.
h. Apply constant force slowly to the “ears” of each throw of the knot.
i. Use the two-hand tie technique to maintain continuous tension on suture ends.
j. During an instrument tie, position the needle holder parallel to the wound.
k. Position the needle holder above the fixed suture end to form the first and second suture throws
of a square (1=1) knot.
l. Clamp only the free end of the suture during the instrument tie.
When suturing…DON’T
a. Pass the surgical needle swaged to a suture through the wound edge in a direction away from
you.
b. Construct a secure knot that cannot be advanced to the wound edges.
c. Apply frictional forces (sawing) between the suture “ears” during knot construction that damage
the suture and reduce its strength.
d. Add further throws to a knot that has the required number of throws for knot security.
e. Position your hands perpendicular to the suture loop.
f. Exert unequal levels of tension to the suture ends that convert the knot into a slip knot.
g. Maintain the same position of your hands after each additional throw.
h. Apply a constant force rapidly to the “ears” of each throw of the knot.
i. Use the one-hand tie technique to maintain continuous tension of the suture ends.
j. During an instrument tie, position the needle holder perpendicular to the wound.
k. Position the needle holder above the fixed suture end to form the first throw, and then below the
fixed suture end to form the second throw of the square knot (1=1).
l. Clamp the suture loop with an instrument because it will crush the suture, reducing its strength.
18
SUTURE SPACING
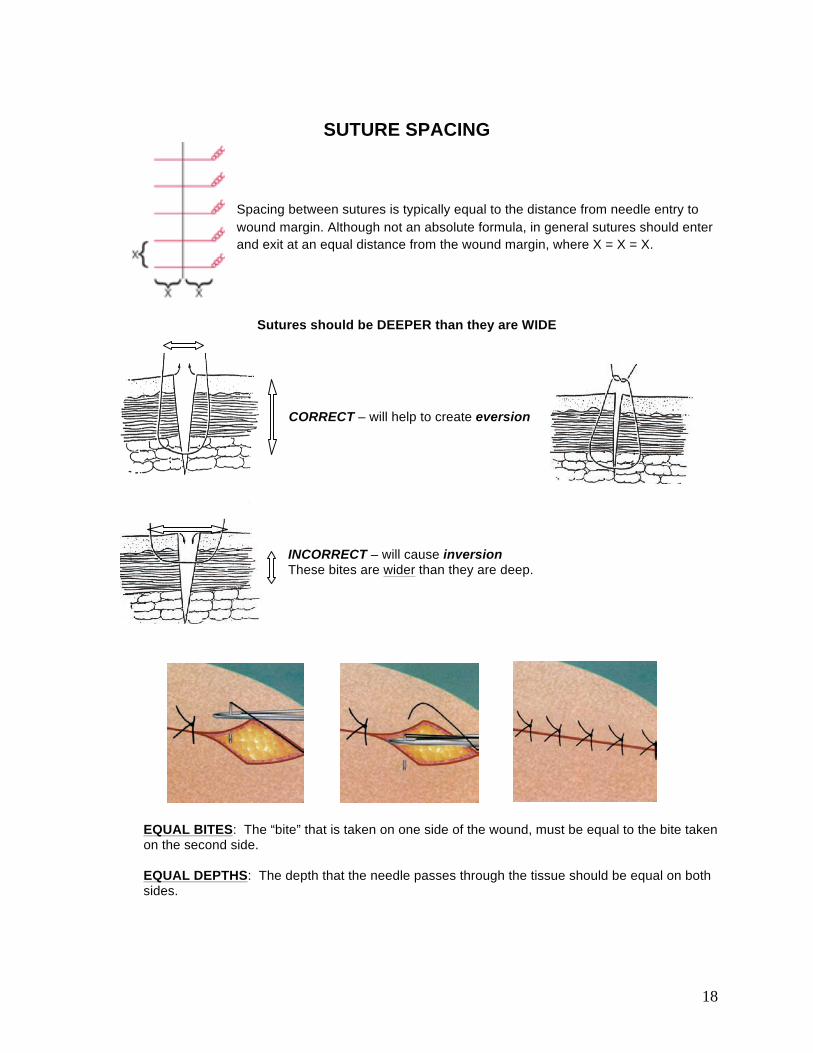
Spacing between sutures is typically equal to the distance from needle entry to wound margin. Although not an absolute formula, in general sutures should enter and exit at an equal distance from the wound margin, where X = X = X.
Sutures should be DEEPER than they are WIDE
CORRECT – will help to create eversion
INCORRECT – will cause inversion These bites are wider than they are deep.
EQUAL BITES: The “bite” that is taken on one side of the wound, must be equal to the bite taken on the second side. EQUAL DEPTHS: The depth that the needle passes through the tissue should be equal on both sides.
19
PERPENDICULAR: The needle should pass through the tissue perpendicular to the incision. This will help to restore the anatomy correctly. Oblique stitches will result in uneven closing and may result in a “dog ear” effect at the end of the incision. Remember…
EQUAL BITES
EQUAL DEPTHS
PERPENDICULAR
SQUARE KNOTS!
THE PRIMARY SUTURE LINE The primary suture line is the line of sutures that holds the wound edges in approximation during healing by first intention. It may consist of a continuous strand of material or a series of interrupted suture strands. Other types of primary sutures, such as deep sutures, buried sutures, purse-string sutures, and subcuticular sutures, are used for specific indications. Regardless of technique, a surgical needle is attached to the suture strand to permit repeated passes through tissue.
THE SECONDARY SUTURE LINE
A secondary line of sutures may be used:
a. To reinforce and support the primary suture line, eliminate dead space, and prevent fluid accumulation in an abdominal wound during healing by first intention. When used for this purpose, they may also be called retention, stay, or tension sutures.
b. To support wounds for healing by second intention.
c. For secondary closure following wound disruption when healing by third intention.
NOTE: If secondary sutures are used in cases of non-healing, they should be placed in opposite fashion from the primary sutures (i.e., interrupted if the primary sutures were continuous, continuous if the primary sutures were interrupted).
20
RETENTION SUTURES Retention sutures are rarely used in rodents and is more commonly used in large animals. When used, they are placed further away from each edge of the wound (~ 2 cm in large animals). The tension exerted lateral to the primary suture line contributes to the tensile strength of the wound. Through-and-through sutures are placed from inside the peritoneal cavity through all layers of the abdominal wall, including the peritoneum. They should be inserted before the peritoneum is closed using a simple interrupted stitch. The wound may be closed in layers for a distance of approximately three-fourths its length. Then the retention sutures in this area may be drawn together and tied. It is important that a finger be placed within the abdominal cavity to prevent strangulation of the viscera in the closure. The remainder of the wound may then be closed. Prior to tightening and tying the final retention sutures, it is important to explore the abdomen again with a finger to prevent strangulation of viscera in the closure. The remainder of the wound may then be closed. Retention sutures utilize nonabsorbable suture material. They should therefore be removed as soon as the danger of sudden increases in intra-abdominal pressure is over-- usually 2 to 6 weeks, with an average of 3 weeks.
CUTTING SUTURES
Once the knot has been securely tied, the ends must be cut. Before cutting, make sure both tips of the scissors are visible to avoid inadvertently cutting tissue beyond the suture. Cutting sutures entails running the tip of the scissors lightly down the suture strand to the knot. The ends of surgical gut are left relatively long, approximately 1/4" (6mm) from the knot. Other materials are cut closer to the knot, approximately 1/8" (3mm), to decrease tissue reaction and minimize the amount of foreign material left in the wound. To ensure that the actual knot is not cut, twist or angle the blades of the scissors prior to cutting. Make certain to remove the cut ends of the suture from the operative site.
SUTURE REMOVAL When the wound has healed so that it no longer needs the support of non-absorbable suture material, skin sutures must be removed. The length of time the sutures remain in place depends upon the rate of healing and the nature of the wound. Sutures should be removed before the epithelium has migrated into deeper parts of the dermis, generally between days 10-14 post-op, but this may vary. Sutures should be removed using clean or aseptic technique. The following steps are recommended:
STEP 1--Cleanse the area with an antiseptic. Hydrogen peroxide can be used to remove dried serum encrusted around the sutures. STEP 2--Pick up one end of the suture with thumb forceps or thumb and index finger, and cut as close to the skin as possible where the suture enters the skin. STEP 3--Gently pull the suture strand out through the side opposite the knot with the forceps. To prevent risk of infection, the suture should be removed without pulling any portion that has been outside the skin back through the skin.
21
COMMON SUTURE PATTERNS
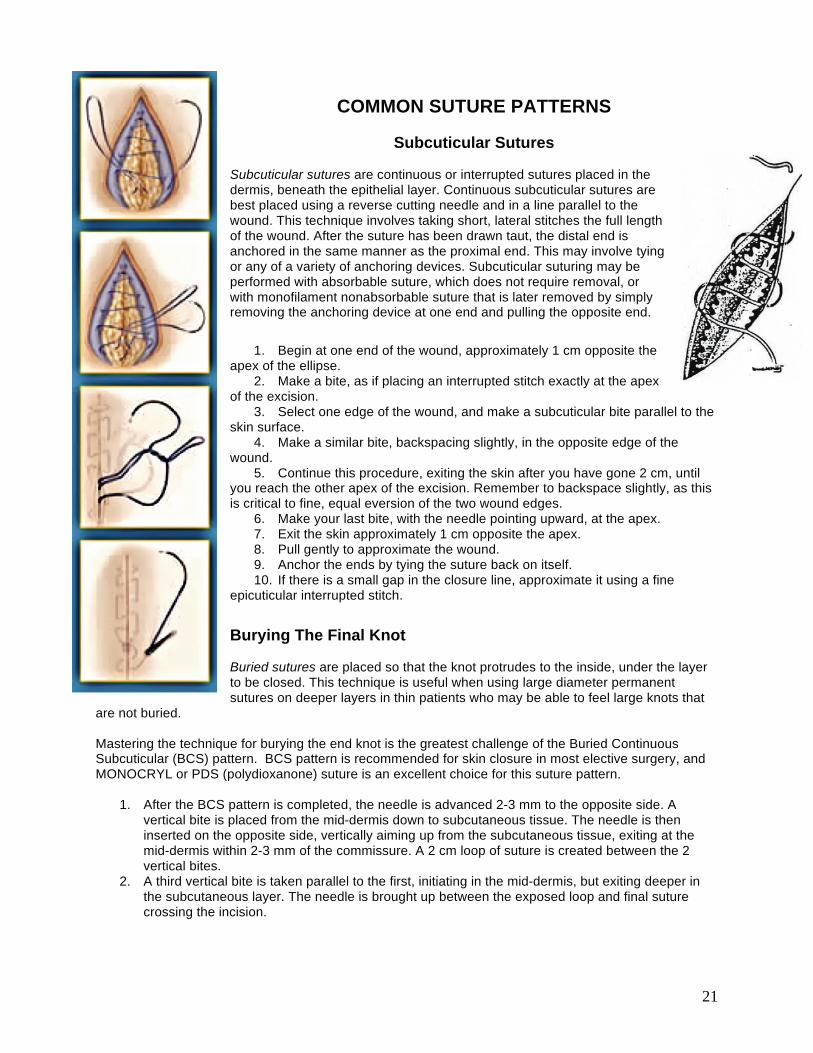
Subcuticular Sutures Subcuticular sutures are continuous or interrupted sutures placed in the dermis, beneath the epithelial layer. Continuous subcuticular sutures are best placed using a reverse cutting needle and in a line parallel to the wound. This technique involves taking short, lateral stitches the full length of the wound. After the suture has been drawn taut, the distal end is anchored in the same manner as the proximal end. This may involve tying or any of a variety of anchoring devices. Subcuticular suturing may be performed with absorbable suture, which does not require removal, or with monofilament nonabsorbable suture that is later removed by simply removing the anchoring device at one end and pulling the opposite end.
1. Begin at one end of the wound, approximately 1 cm opposite the apex of the ellipse.
2. Make a bite, as if placing an interrupted stitch exactly at the apex of the excision.
3. Select one edge of the wound, and make a subcuticular bite parallel to the skin surface.
4. Make a similar bite, backspacing slightly, in the opposite edge of the wound.
5. Continue this procedure, exiting the skin after you have gone 2 cm, until you reach the other apex of the excision. Remember to backspace slightly, as this is critical to fine, equal eversion of the two wound edges.
6. Make your last bite, with the needle pointing upward, at the apex. 7. Exit the skin approximately 1 cm opposite the apex. 8. Pull gently to approximate the wound. 9. Anchor the ends by tying the suture back on itself. 10. If there is a small gap in the closure line, approximate it using a fine
epicuticular interrupted stitch.
Burying The Final Knot
Buried sutures are placed so that the knot protrudes to the inside, under the layer to be closed. This technique is useful when using large diameter permanent sutures on deeper layers in thin patients who may be able to feel large knots that
are not buried. Mastering the technique for burying the end knot is the greatest challenge of the Buried Continuous Subcuticular (BCS) pattern. BCS pattern is recommended for skin closure in most elective surgery, and MONOCRYL or PDS (polydioxanone) suture is an excellent choice for this suture pattern.
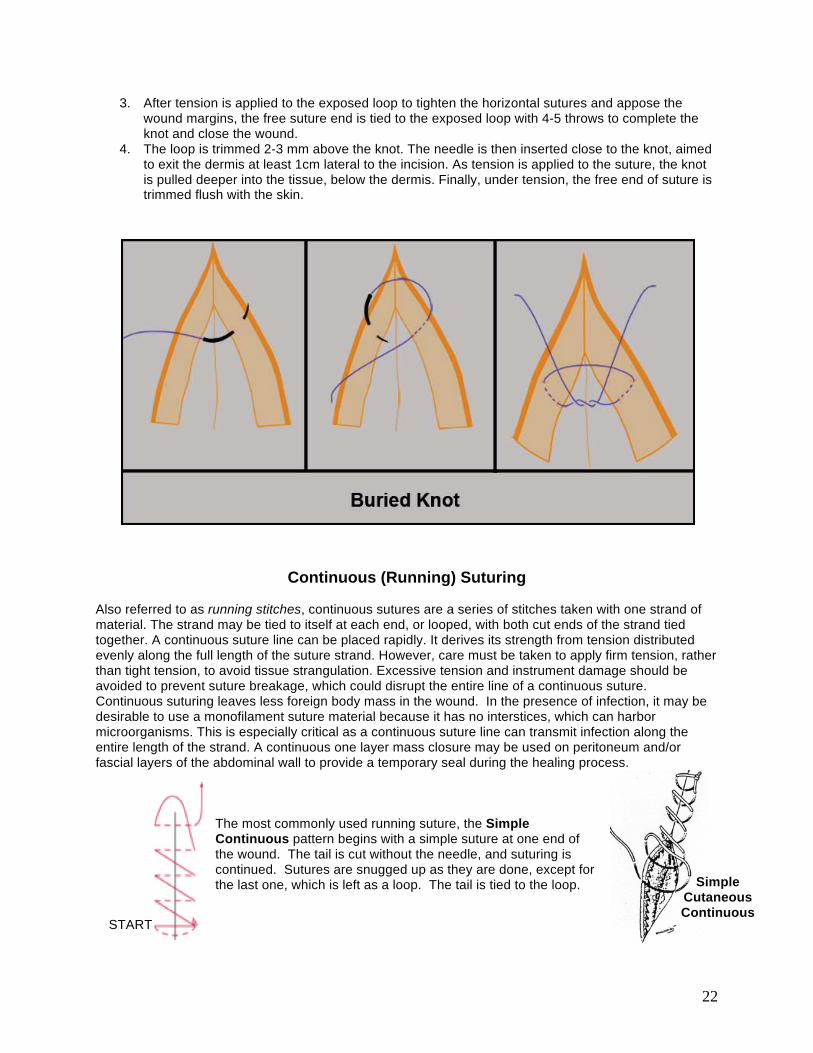
1. After the BCS pattern is completed, the needle is advanced 2-3 mm to the opposite side. A vertical bite is placed from the mid-dermis down to subcutaneous tissue. The needle is then inserted on the opposite side, vertically aiming up from the subcutaneous tissue, exiting at the mid-dermis within 2-3 mm of the commissure. A 2 cm loop of suture is created between the 2 vertical bites.
2. A third vertical bite is taken parallel to the first, initiating in the mid-dermis, but exiting deeper in the subcutaneous layer. The needle is brought up between the exposed loop and final suture crossing the incision.
22
3. After tension is applied to the exposed loop to tighten the horizontal sutures and appose the wound margins, the free suture end is tied to the exposed loop with 4-5 throws to complete the knot and close the wound.
4. The loop is trimmed 2-3 mm above the knot. The needle is then inserted close to the knot, aimed to exit the dermis at least 1cm lateral to the incision. As tension is applied to the suture, the knot is pulled deeper into the tissue, below the dermis. Finally, under tension, the free end of suture is trimmed flush with the skin.
Continuous (Running) Suturing
Also referred to as running stitches, continuous sutures are a series of stitches taken with one strand of material. The strand may be tied to itself at each end, or looped, with both cut ends of the strand tied together. A continuous suture line can be placed rapidly. It derives its strength from tension distributed evenly along the full length of the suture strand. However, care must be taken to apply firm tension, rather than tight tension, to avoid tissue strangulation. Excessive tension and instrument damage should be avoided to prevent suture breakage, which could disrupt the entire line of a continuous suture. Continuous suturing leaves less foreign body mass in the wound. In the presence of infection, it may be desirable to use a monofilament suture material because it has no interstices, which can harbor microorganisms. This is especially critical as a continuous suture line can transmit infection along the entire length of the strand. A continuous one layer mass closure may be used on peritoneum and/or fascial layers of the abdominal wall to provide a temporary seal during the healing process.
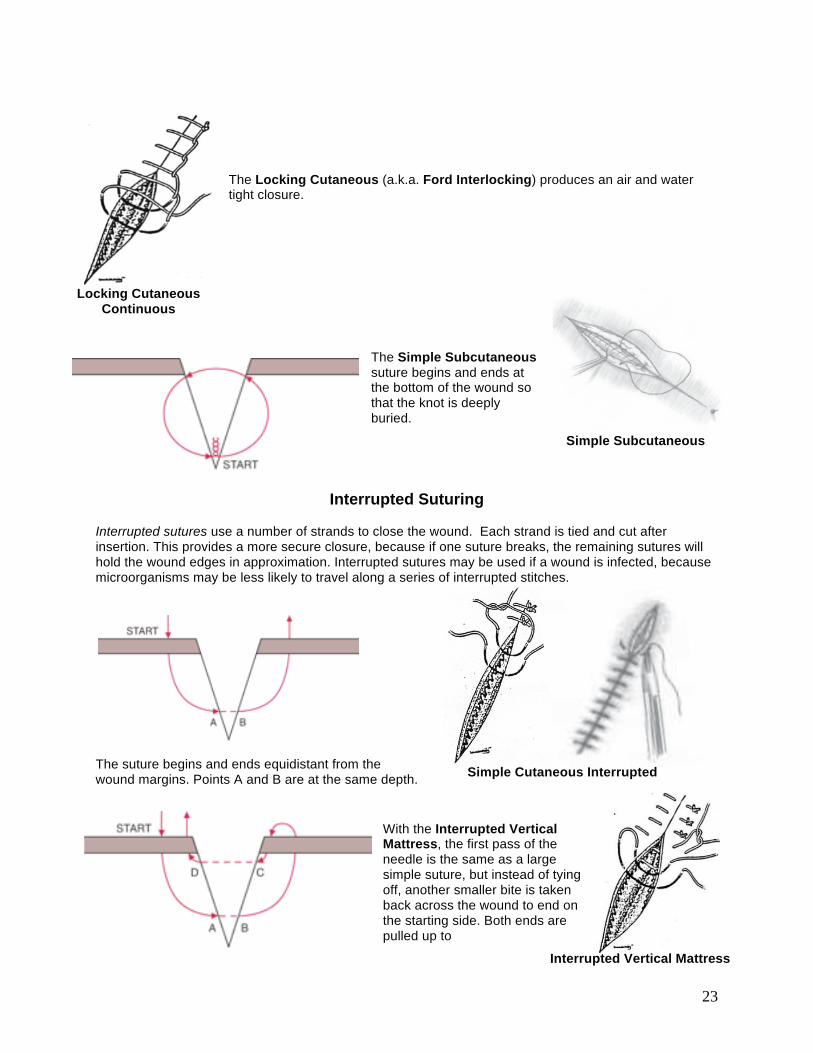
The most commonly used running suture, the Simple Continuous pattern begins with a simple suture at one end of the wound. The tail is cut without the needle, and suturing is continued. Sutures are snugged up as they are done, except for the last one, which is left as a loop. The tail is tied to the loop.
Simple Cutaneous Continuous
START
23
The Locking Cutaneous (a.k.a. Ford Interlocking) produces an air and water tight closure.
The Simple Subcutaneous suture begins and ends at the bottom of the wound so that the knot is deeply buried.
Interrupted Suturing
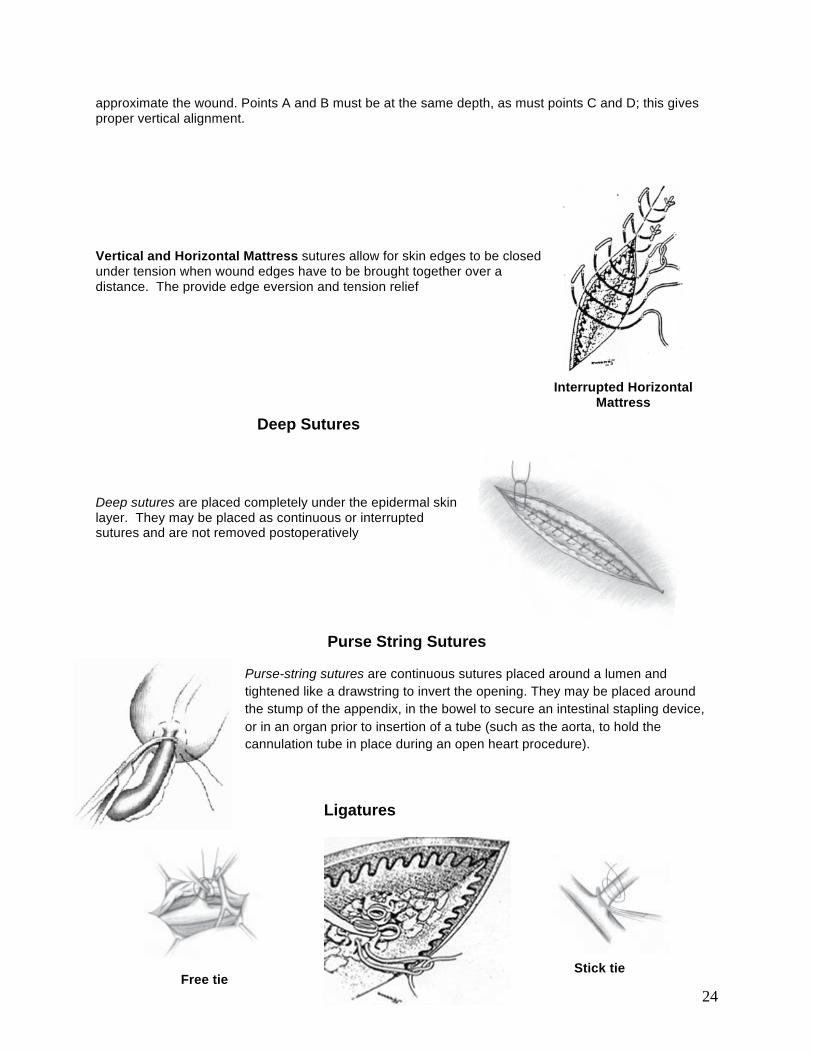
Interrupted sutures use a number of strands to close the wound. Each strand is tied and cut after insertion. This provides a more secure closure, because if one suture breaks, the remaining sutures will hold the wound edges in approximation. Interrupted sutures may be used if a wound is infected, because microorganisms may be less likely to travel along a series of interrupted stitches.
The suture begins and ends equidistant from the wound margins. Points A and B are at the same depth.
With the Interrupted Vertical Mattress, the first pass of the needle is the same as a large simple suture, but instead of tying off, another smaller bite is taken back across the wound to end on the starting side. Both ends are pulled up to
Simple Subcutaneous
Simple Cutaneous Interrupted
Interrupted Vertical Mattress
Locking Cutaneous Continuous
24
approximate the wound. Points A and B must be at the same depth, as must points C and D; this gives proper vertical alignment. Vertical and Horizontal Mattress sutures allow for skin edges to be closed under tension when wound edges have to be brought together over a distance. The provide edge eversion and tension relief
Deep Sutures Deep sutures are placed completely under the epidermal skin layer. They may be placed as continuous or interrupted sutures and are not removed postoperatively
Purse String Sutures Purse-string sutures are continuous sutures placed around a lumen and tightened like a drawstring to invert the opening. They may be placed around the stump of the appendix, in the bowel to secure an intestinal stapling device, or in an organ prior to insertion of a tube (such as the aorta, to hold the cannulation tube in place during an open heart procedure).
Ligatures
Interrupted Horizontal Mattress
Free tie Stick tie

25
Anastomotic Closure Technique
Inverted Closure Technique References (adapted from):
1. Surgical Knot Tying Manual (US Surgical Corp) 2. Knot Tying Manual (Ethicon, Inc.) 3. Wound Closure Manual (Ethicon, Inc.) 4. Merck Manual (Merck, Inc.)
Single Layer Double Layer

Vol 53, No 6November 2014
Pages 684–691
Journal of the American Association for Laboratory Animal ScienceCopyright 2014by the American Association for Laboratory Animal Science
684
The goals of achieving a surgical plane of anesthesia are to provide immobility, unconsciousness, analgesia, amnesia, and attenuation of autonomic responses to noxious stimuli5 without adversely compromising physiologic variables such as heart rate, respiratory rate, body temperature, and blood pressure.1,5 For prolonged surgical procedures, inhaled anesthetics gener-ally are recommended because of rapid onset of and recovery from anesthesia, efficacy in attaining and maintaining a surgical plane of anesthesia, and relative safety.15 In laboratory animal practice, there are situations when inhaled anesthetics cannot be used due to technical or experimental limitations.6,13,15,43 In these cases, an intraperitoneal injectable anesthetic protocol, typically including the combination of ketamine–xylazine–ace-promazine (KXA), is used in mice to achieve a surgical plane of anesthesia.3,8,22,47 If the procedure requires a duration of anesthesia beyond what a single dose of these drugs can pro-vide, repeat-bolus dosing is the default method to extend the duration of anesthesia in mice. Although previous studies have evaluated the safety and efficacy of a single bolus of injectable anesthetics in rodents, no study has evaluated these parameters in the repeated dosing of injectable anesthetics to extend the duration of anesthesia, resulting in minimal information and
guidance for researchers and veterinarians beyond anecdotal experience.3,8-11,14,16,17,22,25,30,39
When considering repeat-bolus dosing, it is essential to fac-tor in the dose as well as the timing of administration to the animal. Knowledge of pharmacokinetics of each drug, as well as of drug interactions with other combined agents, is impera-tive for deciding how much to administer and when to provide the repeat dose to avoid either overdosing or underdosing the animal. The elimination half-life of ketamine in various strains of mice is approximately 13 min when administered by the intraperitoneal route,28 making it a preferred drug for redosing, because systemic concentrations are likely to be diminished at the time of dissipation of the surgical plane of anesthesia. Poten-tial negative effects of ketamine include respiratory depression, arrhythmias, seizures, tremors, muscle hypertonicity, and erratic or prolonged anesthetic recovery.32,42 Xylazine has a half-life of 1.2 to 1.6 h in rats, and although it has not been evaluated in mice,44,45,48 the half-life of xylazine in mice is presumably longer than that of ketamine. Due to the lack of information on the half-life of xylazine in mice, caution should be taken with any redosing scenario to prevent overdosing the drug. Adverse effects of xylazine in multiple species include hypotension, bradycardia, decreased gastrointestinal motility, and respiratory and cardiovascular depression.32,42 The metabolism of xylazine is likely unaffected by concurrent ketamine administration, ac-cording to in vitro data.26 Acepromazine has a relatively long half-life in nonrodent species, for example 7.1 h in dogs and 50 to 183 min in horses,21,37 and is not routinely redosed in mice.
Dose Regimens, Variability, and Complications Associated with Using Repeat-Bolus Dosing to Extend a Surgical Plane of Anesthesia in
Laboratory Mice
Samer M Jaber,1,2 F Claire Hankenson,1,2 Kathleen Heng,4 Andrew McKinstry-Wu,3 Max B Kelz,3 and James O Marx1,2,*
Extending a surgical plane of anesthesia in mice by using injectable anesthetics typically is accomplished by repeat-bolus dosing. We compared the safety and efficacy of redosing protocols administered either during an anesthetic surgical plane (maintaining a continuous surgical plane, CSP), or immediately after leaving this plane (interrupted surgical plane, ISP) in C57BL/6J mice. Anesthesia was induced with ketamine, xylazine, and acepromazine (80, 8, and 1 mg/kg IP, respectively), and redosing protocols included 25% (0.25K), 50% (0.5K), or 100% (1.0K) of the initial ketamine dose or 25% (0.25KX) or 50% (0.5KX) of the initial ketamine–xylazine dose. In the ISP group, the surgical plane was extended by 13.8 ± 2.1 min (mean ± SEM) after redosing for the 0.25K redose with 50% returning to a surgical plane, 42.7 ± 4.5 min for the 0.5K redose with 88% returning to a surgical plane, and 44.3 ± 15.4 min for the 1.0K redose, 52.8 ± 7.2 min for the 0.25KX redose, and 45.9 ± 2.9 min for the 0.5KX redose, with 100% of mice returning to a surgical plane of anesthesia in these 3 groups. Mortality rates for ISP groups were 0%, 12%, 33%, 12%, and 18%, respectively. Mice in CSP groups had 50% mortality, independent of the repeat-dosing protocol. We recommend redosing mice with either 50% of the initial ketamine dose or 25% of the initial ketamine–xylazine dose immediately upon return of the pedal withdrawal reflex to extend the surgical plane of anesthesia in mice, optimize the extension of the surgical plane, and minimize mortality.
Abbreviations: CSP, continuous surgical plane; ISP, interrupted surgical plane; KXA, ketamine–xylazine–acepromazine; PWR, pedal withdrawal reflex; RR, righting reflex.
Received: 27 Feb 2014. Revision requested: 25 Mar 2014. Accepted: 01 May 2014.1University Laboratory Animal Resources, 2Department of Pathobiology, School of Veterinary Medicine, and 3Department of Anesthesiology and Critical Care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania; 4School of Veterinary Medicine, University of California, Davis, California.
*Corresponding author. Email: [email protected]
jaalas14000039.indd 684 11/20/2014 11:28:45 AM

685
Repeat-bolus dosing for anesthesia of B6 mice.
acepromazine (10 mg/mL, Acepromazine maleate, Phoenix Pharmaceuticals, St Joseph, MO) at doses of 80, 8, and 1 mg/kg IP, respectively. Artificial tears ointment (Akwa Tears, Akorn, Lake Forest, IL) was applied to the eyes at the beginning of each trial. The initial dose of KXA was based on published reports in rodents3,8,22,47 and a pilot experiment to test the response of C57BL/6J mice (n = 14 mice; 22 anesthetic events) to different anesthetic doses (Table 1).
Mice were monitored every 30 s from the time of injection for the loss of righting reflex (RR). The RR was defined as the abil-ity to return to sternal recumbency or normal standing posture with all 4 limbs on the ground within 60 s after being placed in dorsal recumbency on a flat surface. Once the RR was lost, the mice were placed in dorsal recumbency on a circulating-water heating pad (Gaymar Industries, Orchard Park, NY) set to maintain a surface temperature of 37 °C and instrumented for physiologic monitoring. Temperature was measured by using a temperature probe placed rectally (length of the probe; RET-3, Thermoworks, Lindon, UT) connected to a thermometer (MicroTherma TW2-193, Thermoworks). Starting temperatures and lowest temperatures during anesthesia were 36.5 ± 0.1 °C and 35.6 ± 0.1 °C, respectively. Electrocardiogram leads were placed on immobilized mice on the right forelimb and the base of the tail with coupling gel and held in place by using standard medical adhesive tape. Respiratory rate was measured visually by counting thoracic excursions. Heart rate, respiratory rate, and rectal temperature were recorded every 5 min under anesthesia. These parameters were measured prior to assessment of the pedal withdrawal reflex (PWR) to reflect resting physiologic parameters under anesthesia.
A surgical plane of anesthesia was defined by the absence of any motor response to a noxious stimulus. The PWR was assessed every 5 min immediately after evaluating the physi-ologic parameters as previously described (300-g, 6.65-gauge Touch-Test Sensory Evaluator, North Coast Medical, Gilroy, CA),.23,27 The point of compression was on the dorsal aspect of the metatarsal region and alternated between hindlimbs. A positive response was defined as any flexion of the stifle, tarsus, hip, or combination of joints in response to this stimulus or any other spontaneous motion of the mouse not associated with the stimulated limb. Once loss of the PWR was confirmed, this stimulus was reapplied every 5 min until return of the PWR or until the mouse exhibited spontaneous movement. For mice that had spontaneous motion between the 5-min intervals of PWR assessment, the time until return of the PWR was recorded, and the repeat dose was administered immediately, but the as-sessment interval was not reset and instead continued every 5 min from the previous assessment. The duration of the surgical plane of anesthesia was defined as the time between the loss of the PWR and its return.
Mice were divided randomly into 2 groups according to the tim-ing of the repeat dose. One group was dosed prior to the anticipated return of the PWR, at 30 min after the initial injection, providing a continuous surgical plane (CSP group). This administration time point was approximately 10 min prior to the anticipated return of the PWR, on the basis of the shortest duration of a surgical plane of anesthesia in the pilot study (Table 1). The mice received 25%, 50%, or 100% of their initial dose of ketamine (0.25K, 0.5K, and 1.0K, respectively) or 50% of both the initial doses of ketamine and xylazine combined (0.5KX). The second group of mice, which had an interrupted surgical plane (ISP group), was dosed immediately after return of the PWR or when any spontaneous motion was observed. These mice were redosed with either 0.25K, 0.5K, 1.0K, or 0.5KX or 25% of the initial dose of both ketamine and xylazine
The timing of drug administration is another critical factor to consider when addressing anesthetic redosing. Ideally, an effective repeat-dosing regimen achieves an uninterrupted, continuous surgical plane of anesthesia with a predictable an-esthetic recovery. The advantage of redosing prior to the animal leaving the surgical plane of anesthesia is that a continuous surgical plane of anesthesia is maintained, eliminating concerns over patient awareness and perception of pain. The main disad-vantage of this redosing approach is that adding more drug to the system while there is potentially still a considerable amount affecting the animal increases the risk of adverse side effects. Conversely, dosing at the time of emergence from a surgical plane of anesthesia decreases the risk of anesthetic overdose but may increase the possibility of a patient’s transient conscious awareness of the procedure.
The aim of the present study was to identify a safe and effec-tive dosing regimen to extend the surgical plane of anesthesia in mice by using an injectable anesthetic combination of KXA. We hypothesized that the ideal anesthetic regimen would permit the administration of a second dose of anesthetic before the mouse emerged from a surgical plane of anesthesia, thus facilitating an uninterrupted extension of that plane of anesthesia while minimizing mortality.
Materials and MethodsAnimals and facility. Male SPF C57BL/6J mice (Mus musculus,
n = 56; age, 8 to 14 wk; weight, 27.3 ± 0.2 g [range, 23 to 31 g]) were obtained from an approved vendor (Jackson Laboratories, Bar Harbor, ME). Male mice were selected to eliminate the po-tential influence of hormonal variations of the estrus cycle on anesthetic responses. To adhere to the principle of reduction, mice were used for as many as 2 separate anesthetic experi-ments, with a minimum of 10 d as a washout period between anesthetic exposures. All mice were housed in an AAALAC-accredited rodent facility at a 12:12-h light:dark cycle in static polycarbonate microisolation cages (Max 75, Alternative Design, Siloam Springs, AR) on disposable bedding (0.12-in. Bed-O-Cobs, The Andersons, Maumee, OH). Mice were fed standard pelleted laboratory rodent chow (no. 5010, LabDiet, St Louis, MO) and provided municipal water supplied by bottle. All procedures described were approved by the University of Pennsylvania’s IACUC.
A subset of mice (n = 20) was used to determine the baseline heart rate for unanesthetized, unrestrained mice. Heart rate was determined on a recording platform by ECG after a 3-min acclimation period (ECGenie, Mouse Specifics, Quincy, MA; eMouse 11 Analysis Software, Mouse Specifics, Quincy, MA). The baseline heart rate of the mice was 734 ± 8 bpm (range, 654 to 788 bpm).
Anesthetic dosing and monitoring. All procedures were performed during the last 6 h of the light cycle to reduce envi-ronmental and circadian rhythm variability. Mice were weighed individually on a digital scale (US-ACE, US Balance, Vincennes, IN) prior to dosing. The anesthetic drugs were diluted to 10% of their original concentration by using sterile 0.9% NaCl and combined at the designated doses into a single syringe imme-diately prior to injection. Doses for each drug were rounded to the nearest 0.01 mL. Each mouse was manually restrained for intraperitoneal injection in the right lower quadrant of the abdomen by using a 27-gauge needle (5/8 in. length) on a 1-mL syringe. Injection volumes ranged from 0.31 to 0.40 mL for initial doses based on weight. Mice received ketamine (100 mg/mL, Ketaset, Fort Dodge Industries, Fort Dodge, IA,) xylazine (20 mg/mL, AnaSed, Lloyd Laboratories, Shenandoah, IA), and
jaalas14000039.indd 685 11/20/2014 11:28:45 AM

686
Vol 53, No 6Journal of the American Association for Laboratory Animal ScienceNovember 2014
effect on the body temperature of the sedated mice, because thermal support of the sedated mice could not be provided on the ECGenie platform.
Statistical analysis. Means ± SE were calculated for all data. The extension of the surgical plane in surviving mice was ana-lyzed by 2-way ANOVA, with main effects of the timing of the redosing and the dose of anesthetics administered. A repeated-measures, 2-way ANOVA was performed to compare the heart and respiratory rates of survivors and nonsurvivors over time. Two-way repeated-measures ANOVA also was used to analyze the effects of ketamine or saline injection on heart rate. When significant differences were detected, Tukey post hoc analysis was performed. A t-test was performed to compare the body weights of mice that died unexpectedly with those of mice that survived. χ2 tests were performed to determine whether there was a difference in survival between the first and second anesthetic event and for the 4 different ISP and CSP redosing protocols. For all analyses, a P value less than 0.05 was consid-ered to be statistically significant. All statistical analysis was done by using SigmaPlot 12.3 (Systat Software, San Jose, CA).
ResultsInitial dose. The initial dose of KXA (80, 8, and 1 mg/kg,
respectively) was successful in inducing a surgical plane of anesthesia without excessive mortality in 88.4% (76 of 86) of the anesthetic events. The initial dose resulted in death in 3 of the 86 mice; these mice were excluded from further evaluation. In addition, 7 of the 86 mice did not reach a surgical plane of anesthesia after the initial dose. The average time to loss of the RR was 2.5 ± 0.1 min (range, 1.40 to 4.98 min). The average time to loss of the PWR was 17.0 ± 0.8 min (7.9 to 30.8 min). The average time of repeat dosing in ISP group animals was 39.7 ± 1.8 min (range, 25.0 to 90.0 min). Although some mice had mild swelling and erythema of the paw after PWR testing, these were self-resolving, and no lameness could be appreciated on inspection the day after testing.
ISP groups. The duration of surgical plane of anesthesia after redosing, the time to return of the RR, and mortality data for the ISP group are summarized in Table 2. The extension of a surgical plane of anesthesia was significantly (P < 0.05) less for the 0.25K dose than for the 0.25KX and 0.5KX doses (Table 3). Mortality in
combined (0.25KX). Two mice initially assigned to the CSP group, one each in the 0.5K and 1.0K groups, demonstrated return of the PWR at 25 min after the initial injection and therefore were included in the ISP group. Acepromazine was not redosed in light of its long duration of action.32
After redosing, physiologic parameters and PWR were moni-tored every 5 min for loss of the PWR, until return of the PWR or spontaneous motion was noted. Monitoring instrumentation then was removed, and the mice remained in dorsal recumbency until the return of the RR. The time to the return of the RR was established as the time until the mouse spontaneously righted itself from dorsal recumbency 3 consecutive times. Mice were monitored until they were ambulatory and subsequently were monitored once daily for 2 d after the experiments for any ad-verse clinical signs induced due to use of the sensory evaluator, including redness or swelling of the foot or gait abnormalities.
During the course of the experiments, several mice (n = 19) developed an agonal pattern of breathing. No mice that de-veloped agonal breathing recovered from anesthesia without intervention. The animals were considered to have reached the point of death when there was complete respiratory arrest for 1 min in conjunction with cardiac arrest noted via ECG. A subset of the mice (7 of 19) that developed agonal breathing while un-der anesthesia after their repeated dose were give atipamezole (0.1 mg IP per mouse; Antisedan, Zoetis, Florham Park, NJ) to attempt to reverse the injectable anesthesia. For these animals, the time of dosing of atipamezole was considered the time of death for purposes of analysis of response to the redosing pro-tocol. These mice were not reused in subsequent experiments.
Effect of ketamine on heart rate. To evaluate the effect of ketamine independently, heart rate was recorded (ECGenie, Mouse Specifics) both before and after mice were given either ketamine (n = 6) or saline (control, n = 4). Mice were placed on the platform and allowed to acclimate before recording the baseline ECG. Mice were injected as previously described for the anesthetic protocols. Total administration volumes were diluted with 0.9% NaCl to match drug volumes used in the KXA protocol. The ECG was recorded continuously until the mouse exhibited grooming behavior or the heart rate returned to resting heart rate. Heart rate was measured at 2.5 and 5 min after dosing and at 5-min intervals thereafter. A single mouse was dosed with ketamine to confirm that the drugs had minimal
Table 1. Results of the pilot study to determine initial injectable anesthetic dose
Dose group (mg/kg)No. of mice that reached a surgical plane of
anesthesia/ total no. of miceDuration (min) of surgical plane of anesthe-
sia (mean ± SE [range])No. of deaths/ total no.
of mice
Ketamine 50 0/4 not applicable 0/4Xylazine 5Acepromazine 1
Ketamine 80 6/7 45.1 ± 9.4 (40–73; n = 6) 0/7Xylazine 8Acepromazine 1
Ketamine 100 7/7 67.7 ± 2.9 (64–72; n = 3) 4/7Xylazine 10Acepromazine 1–2
Ketamine 100 3/4 23.3 ± 16.7 (5–50; n = 3) 0/4Xylazine 10
Methods for monitoring and support of mice in pilot study (n = 14 mice; 22 anesthetic events) were identical to those used for the experimental animals.
jaalas14000039.indd 686 11/20/2014 11:28:45 AM

687
Repeat-bolus dosing for anesthesia of B6 mice.
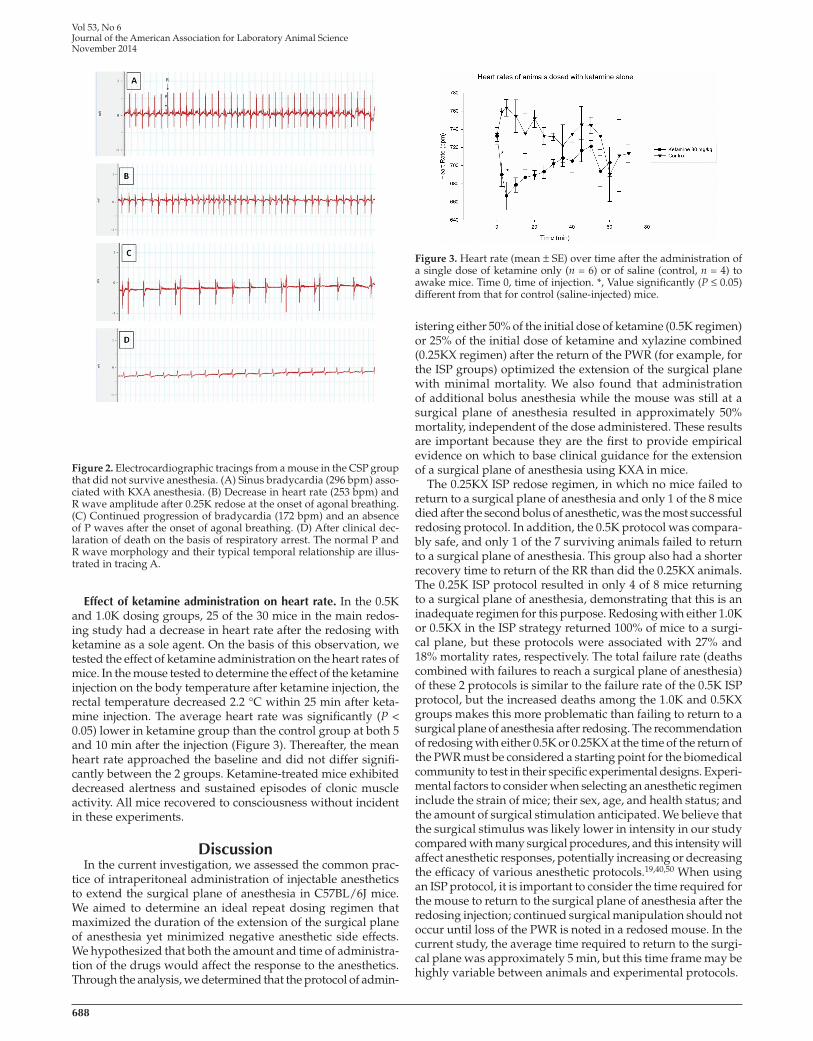
ventricular tachycardia or fibrillation, were noted in the ECG tracing of any animals prior to the onset of agonal breathing. ECG tracings at various time points for a mouse that did not survive are shown in Figure 2.
Anesthetic reversal. Of the 7 mice that received atipamezole reversal after exhibiting agonal respiration, 43% (n = 3) went on to recover from anesthesia, whereas the remaining 57% (n = 4) progressed to death. In the mice that did not recover, death occurred within 10 min after administration of the reversal agent. The mice that recovered displayed a rapid increase in heart rate (658 ± 38 bpm) compared with the animals that did not successfully recover (331 ± 23 bpm) at 5 min after reversal. The same trend was seen for respiratory rate, with survivors having higher rates (212 ± 25 breaths per minute) compared with nonsurvivors (32 ± 13 breaths per minute) at 5 min after reversal. For the 3 animals that recovered, average time to return of the RR from the time of reversal administration was 27.3 ± 9.9 min (range, 13 to 41 min). The PWR was not evaluated after the administration of atipamezole.
the ISP groups increased with increasing anesthetic dose, result-ing in 0%, 12%, 33%, 12%, and 18% mortality rates in the 0.25K, 0.5K, 1K, 0.25KX, and 0.5KX groups respectively. χ2 analysis did not reveal significant differences between the mortality rates of the 5 protocols, but this analysis lacks sensitivity at this group size. ISP mice required 5.2 ± 0.5 min (range, 1.1 to 12.1 min) to return to a surgical plane of anesthesia after redosing, and 50% of the 0.25K mice and 12.5% of the 0.5K group failed to return to a surgical plane of anesthesia after repeat dosing.
CSP groups. The duration of the surgical plane of anesthesia after redosing, the time to return of the RR, and mortality data for the CSP group are summarized in Table 3. Mortality in CSP groups was unacceptably high and ranged from 43% to 57% among the redosing protocols. All redosing paradigms extended the surgical plane of anesthesia, except for a single mouse in the 0.25K group, which displayed a positive PWR at 5 min after redosing. The high rate of mortality prevented detection of dif-ferences between doses in the CSP groups in regard to extension of the surgical plane of anesthesia. There was no significant difference in the mortality rates between the various protocols.
Heart and respiratory rates in mice with anesthetic death compared with recovery. One of the animals in the CSP 0.25K group died the day after a successful anesthetic recovery and was excluded from the analysis comparing animals that died with the surviving mice. All other deaths occurred during the anesthetic event itself. All the mice that died displayed agonal breathing. None of the mice that displayed this criti-cal sign recovered without pharmacologic intervention with atipamezole. The duration of agonal breathing prior to death was approximately 1 to 2 min in the 12 of 19 mice that did not receive atipamezole. No significant differences were detected between the weights of surviving mice and mice that died or between those that died during the first compared with second anesthetic events. Mice that survived without atipamezole reversal had a progressive increase in heart rate for several minutes prior to recovery, whereas the heart rates of mice that died remained constant during the procedure prior to arrest (Figure 1). In contrast to this pattern, the respiratory rates of the mice that died had a slowly progressive drop in frequency, whereas surviving mice had a nearly constant respiratory rate prior to recovery (Figure 1). No lethal abnormalities, such as
Table 2. Anesthetic effect, recovery, and complication rate for mice in ISP group.
Dose group
Time (min) at surgical plane of anesthesia after redose (mean ± SE [range])
Time (min) to return of the RR after redose (mean ± SE [range])
No. of deaths/ total no.
Time (min) to death after redose (mean ± SE [range])
0.25K 13.8 ± 2.1 (0-45; n = 8) 49.4 ± 5.0 (14-137; n = 8) 0/8 not applicable
0.5K 42.7 ± 4.5 (0-84; n = 7) 82.7 ± 4.2 (36-129; n = 7) 1/8 35.0 (n = 1)
1K 44.3 ± 15.4 (20-60; n = 6) 83.5 ± 2.7 (64-105; n = 6) 3/9 58.3 ± 4.4 (50-65; n = 3)0.25KX 52.8 ± 7.2a (35-85; n = 7) 140.3 ± 9.0 (114-162; n = 7) 1/8 30.0 (n = 1)
0.5KX 45.9 ± 2.9a (10-79; n = 9) 81.3 ± 2.9 (41-109; n = 9) 2/11 15.0 ± 5 (10-20; n = 2)aValue significantly (P < 0.05) different from that for the 0.25K group.
Table 3. Anesthetic effect, recovery, and complication rate for mice in CSP group
Dose group
Time (min) at surgical plane of anesthesia after redose (mean ± SE [range])
Time (min) to return of the RR after redose (mean ± SE [range])
No. of deaths/ total no.
Time (min) to death after redose (mean ± SE [range])
0.25K 21.3 ± 5.0 (0-45; n = 4) 57.3 ± 5.1 (38-82; n = 4) 3/7a 77.5 ± 32.5 (45-110; n = 2)0.5K 25.0 ± 0 (25; n = 3) 43.7 ± 0.5 (42-45; n = 3) 3/6 81.7 ± 21.7 (45-120; n = 3)1K 61.7 ± 10.5 (35-95; n = 3) 105.0 ± 11.9 (80-146; n = 3) 4/7 67.5 ± 13.6 (50-100; n = 4)0.5KX 55.0 ± 10.4 (35-70; n = 3) 61.7 ± 2.6 (55-70; n = 3) 3/6 53.3 ± 12.7 (35-70; n = 3)aOne of 3 mice died after the experiment; the data from this mouse are not included in the means and ranges in this table.
Figure 1. Heart rate and respiratory rate (mean ± SE) of mice in all redosing groups. Time 0 is the time to return of the RR for survivors or the last recordable time point (that is, 5 min) prior to the onset of agonal breathing in mice that died. *, Significant (P ≤ 0.05) difference between time points in the nonsurviving mice when compared with all time points from –60 min through –35 min. +, Significant (P ≤ 0.05) difference between time points in the surviving mice when compared with all time points from –60 min through –25 min.
jaalas14000039.indd 687 11/20/2014 11:28:45 AM
688
Vol 53, No 6Journal of the American Association for Laboratory Animal ScienceNovember 2014
istering either 50% of the initial dose of ketamine (0.5K regimen) or 25% of the initial dose of ketamine and xylazine combined (0.25KX regimen) after the return of the PWR (for example, for the ISP groups) optimized the extension of the surgical plane with minimal mortality. We also found that administration of additional bolus anesthesia while the mouse was still at a surgical plane of anesthesia resulted in approximately 50% mortality, independent of the dose administered. These results are important because they are the first to provide empirical evidence on which to base clinical guidance for the extension of a surgical plane of anesthesia using KXA in mice.
The 0.25KX ISP redose regimen, in which no mice failed to return to a surgical plane of anesthesia and only 1 of the 8 mice died after the second bolus of anesthetic, was the most successful redosing protocol. In addition, the 0.5K protocol was compara-bly safe, and only 1 of the 7 surviving animals failed to return to a surgical plane of anesthesia. This group also had a shorter recovery time to return of the RR than did the 0.25KX animals. The 0.25K ISP protocol resulted in only 4 of 8 mice returning to a surgical plane of anesthesia, demonstrating that this is an inadequate regimen for this purpose. Redosing with either 1.0K or 0.5KX in the ISP strategy returned 100% of mice to a surgi-cal plane, but these protocols were associated with 27% and 18% mortality rates, respectively. The total failure rate (deaths combined with failures to reach a surgical plane of anesthesia) of these 2 protocols is similar to the failure rate of the 0.5K ISP protocol, but the increased deaths among the 1.0K and 0.5KX groups makes this more problematic than failing to return to a surgical plane of anesthesia after redosing. The recommendation of redosing with either 0.5K or 0.25KX at the time of the return of the PWR must be considered a starting point for the biomedical community to test in their specific experimental designs. Experi-mental factors to consider when selecting an anesthetic regimen include the strain of mice; their sex, age, and health status; and the amount of surgical stimulation anticipated. We believe that the surgical stimulus was likely lower in intensity in our study compared with many surgical procedures, and this intensity will affect anesthetic responses, potentially increasing or decreasing the efficacy of various anesthetic protocols.19,40,50 When using an ISP protocol, it is important to consider the time required for the mouse to return to the surgical plane of anesthesia after the redosing injection; continued surgical manipulation should not occur until loss of the PWR is noted in a redosed mouse. In the current study, the average time required to return to the surgi-cal plane was approximately 5 min, but this time frame may be highly variable between animals and experimental protocols.
Effect of ketamine administration on heart rate. In the 0.5K and 1.0K dosing groups, 25 of the 30 mice in the main redos-ing study had a decrease in heart rate after the redosing with ketamine as a sole agent. On the basis of this observation, we tested the effect of ketamine administration on the heart rates of mice. In the mouse tested to determine the effect of the ketamine injection on the body temperature after ketamine injection, the rectal temperature decreased 2.2 °C within 25 min after keta-mine injection. The average heart rate was significantly (P < 0.05) lower in ketamine group than the control group at both 5 and 10 min after the injection (Figure 3). Thereafter, the mean heart rate approached the baseline and did not differ signifi-cantly between the 2 groups. Ketamine-treated mice exhibited decreased alertness and sustained episodes of clonic muscle activity. All mice recovered to consciousness without incident in these experiments.
DiscussionIn the current investigation, we assessed the common prac-
tice of intraperitoneal administration of injectable anesthetics to extend the surgical plane of anesthesia in C57BL/6J mice. We aimed to determine an ideal repeat dosing regimen that maximized the duration of the extension of the surgical plane of anesthesia yet minimized negative anesthetic side effects. We hypothesized that both the amount and time of administra-tion of the drugs would affect the response to the anesthetics. Through the analysis, we determined that the protocol of admin-
Figure 2. Electrocardiographic tracings from a mouse in the CSP group that did not survive anesthesia. (A) Sinus bradycardia (296 bpm) asso-ciated with KXA anesthesia. (B) Decrease in heart rate (253 bpm) and R wave amplitude after 0.25K redose at the onset of agonal breathing. (C) Continued progression of bradycardia (172 bpm) and an absence of P waves after the onset of agonal breathing. (D) After clinical dec-laration of death on the basis of respiratory arrest. The normal P and R wave morphology and their typical temporal relationship are illus-trated in tracing A.
Figure 3. Heart rate (mean ± SE) over time after the administration of a single dose of ketamine only (n = 6) or of saline (control, n = 4) to awake mice. Time 0, time of injection. *, Value significantly (P ≤ 0.05) different from that for control (saline-injected) mice.
jaalas14000039.indd 688 11/20/2014 11:28:46 AM

689
Repeat-bolus dosing for anesthesia of B6 mice.
The cause of the deaths in the current study was not defini-tively determined, but respiratory depression undoubtedly was a major contributing factor based on anesthetic monitoring prior to cardiac arrest. The mice that died had a significant drop in respiratory rate 10 to 15 min before arrest (Figure 1), whereas surviving mice maintained a constant respiratory rate before regaining consciousness. Both ketamine and xylazine are known to decrease tidal volume and respiratory rate;4,7,12,18,20,24,29,36,41 however, we cannot rule out that the respiratory changes are a secondary marker of the actual cause of death. A trend toward higher heart rates in nonsurvivors may be indicative of a com-pensatory change in response to hypotension, and although no definitive statement can be made to this end given that no blood pressure measurements were obtained from these ani-mals, these data are suggestive of a link between changes in the cardiovascular system and death.
The period of respiratory depression before cardiac arrest presents a potential window, based on an easily measured parameter, when intervention to attempt to save animals for which death is imminent may be possible. In fact, the adminis-tration of atipamezole alone, which reverses only the effects of the α-agonist xylazine, led to the recovery of 43% of the mice that displayed agonal breathing, an advanced state of respira-tory depression. Earlier and more aggressive intervention may lead to a higher success rate in avoiding mortality in these mice. Other possible pharmacologic interventions that may address the underlying cause of death can be evaluated in future stud-ies, including assessments of parasympatholytic agents such as atropine, sympathomimetic agents such as ephedrine, and the respiratory stimulant doxapram. In light of these observa-tions, monitoring respiratory rate may prove to be a valuable predictor of anesthetic complications in mice receiving inject-able anesthetics.
Work in other species has shown that ketamine administration in normal animals increases the heart rate due to the stimulation of the sympathetic nervous system.32 We were surprised to see that the heart rate frequently decreased after the administration of ketamine alone in the redosing protocol. We evaluated the effects of ketamine alone on heart rate in mice; unexpectedly, there was a significant decrease in heart rate after ketamine injection compared with a saline injection. Ketamine is known to depress myocardial function, but this effect is usually over-come by sympathetic stimulation.42 In addition, some of the cardiovascular depression seen in critically ill patients has been attributed to the depletion of catecholamine stores after release induced by ketamine.46 If mice in the current experiment had complete depletion of catecholamine stores prior to redosing with ketamine, the direct myocardial depressive effects may have contributed to anesthetic complications. Because of their intact catecholamine stores, healthy mice that received only ketamine should not have demonstrated this effect, yet a de-crease was noted. Although the decrease in heart rate in the ketamine-only group was statistically significant compared with controls, what contribution this transient decrease in heart rate has on the adverse events associated with repeat-bolus dosing is unknown.
When evaluating the surgical plane of anesthesia in animals, it is important to remember that the motor response to a noxious stimulus is mediated at the level of the spinal cord and may not necessarily reflect perception or awareness.2,33-35 The ultimate goal of anesthetic use in experimental animals is to prevent awareness and any pain perception. It is therefore important to acknowledge that even though the surgical plane may have dissipated as evidenced by return of the PWR, it does not nec-
The advantage of administering additional anesthetics prior to return of the PWR is an uninterrupted surgical plane that eliminates the likelihood of patient awareness or perception of pain during the procedure. In the current investigation, ap-proximately 50% mortality occurred when mice were redosed while under a surgical plane of anesthesia, independent of the redose of drug administered. This outcome demonstrates that the plane of anesthesia at the time of drug redosing is critical in predicting the animal’s response to the anesthetics and that a more profound effect, consistent with the narrow therapeutic index of anesthetic drugs, occurs when drugs are readministered during a surgical plane of anesthesia. It is very challenging to assess subtle differences in the depth of anesthesia in mice due to the lack of a direct way to clinically detect the fraction of the initial drug that an individual animal has metabolized, redistrib-uted, or eliminated, ultimately resulting in considerable risk of anesthetic overdose. A helpful adjunct for evaluation of depth of anesthesia may be parameters derived from the EEG. This monitoring technique allows for direct assessment of activity with the CNS. The use of EEG in anesthetic monitoring and its limitations are reviewed elsewhere.38 For EEG to be considered a true reflection of depth of anesthesia in mice, additional in-vestigation is necessary for this species with different types of anesthetic drugs, doses, and combinations. If validated, these measures could prove useful in determining effective anesthetic regimens. However, it should be noted that EEG reflects cortical evidence of anesthetic drug effects, whereas our definition of the surgical plane as loss of the PWR more closely reflects anesthetic drug effects on the spinal cord. The measures of movement may or may not be congruent with processed EEG indices.
Lack of movement in response to noxious stimuli is the vet-erinary standard for detection of a surgical plane of anesthesia, due to its ease of evaluation and confidence that it provides that the animal is not experiencing any pain or distress. The PWR measured by movement away from a consistent 300-g stimulus provided an objective measure for our studies, but this stimulus is likely less severe than is that incurred by other procedures, particularly invasive surgery. An important factor for the bio-medical community to consider when using these guidelines is that the amount of surgical stimulation is a critical factor in determining the anesthetic requirement.31,49
Consistent with previous work,3 the mice in our study dem-onstrated profound variability in response to the different drug regimens in the current investigation, despite controlling for the strain of mouse, sex, age, health status, circadian rhythm, and stimulation while under anesthesia. The mice had a wide array of responses, which ranged from mice not reaching a surgical plane of anesthesia to mice remaining at a surgical plane of anes-thesia for 25 to 90 min and further to mice dying from this initial administration. Another example of the variable response to the anesthetics is demonstrated in the 0.25K CSP group, in which 1 mouse failed to maintain a surgical plane of anesthesia and half of the group had fatal anesthetic outcomes. Demonstrating similar variability, another study3 tested 8 different anesthesia protocols. Three protocols had some percentage of mice fail to reach a surgical plane of anesthesia, whereas some mice reached a surgical plane of anesthesia and recovered, and some died.3 This documented variability, along with our findings herein, verifies that there is no specific and ideal regimen for injectable anesthetics that can be ap-plied universally to laboratory mice. Laboratory animal specialists and biomedical scientists must be flexible and, using the current recommendations as a guide, plan to adapt anesthesia protocols to specific procedures and the responses of individual animals.
jaalas14000039.indd 689 11/20/2014 11:28:46 AM
690
Vol 53, No 6Journal of the American Association for Laboratory Animal ScienceNovember 2014
(pentobarbitone, ketamine–xylazine, carfentanyl–etomidate). Res Exp Med (Berl) 184:159–169.
15. Fish RE, Clarence J; Marshall Memorial Library Fund. 2008. An-esthesia and analgesia in laboratory animals, 2nd ed. Burlington (MA): Elsevier Academic Press.
16. Green CJ. 1975. Neuroleptanalgesic drug combinations in the anaesthetic management of small laboratory animals. Lab Anim 9:161–178.
17. Green CJ, Knight J, Precious S, Simpkin S. 1981. Ketamine alone and combined with diazepam or xylazine in laboratory animals: a 10-year experience. Lab Anim 15:163–170.
18. Greene SA, Thurmon JC. 1988. Xylazine—a review of its phar-macology and use in veterinary medicine. J Vet Pharmacol Ther 11:295–313.
19. Groeben H, Meier S, Tankersley CG, Mitzner W, Brown RH. 2003. Heritable differences in respiratory drive and breathing pattern in mice during anaesthesia and emergence. Br J Anaesth 91:541–545.
20. Hamza J, Ecoffey C, Gross JB. 1989. Ventilatory response to CO2 following intravenous ketamine in children. Anesthesiology 70:422–425.
21. Hashem A, Kietzmann M, Scherkl R. 1992. [The pharmacokinetics and bioavailability of acepromazine in the plasma of dogs]. Dtsch Tierarztl Wochenschr 99:396–398. [Article in German].
22. He S, Atkinson C, Qiao F, Chen X, Tomlinson S. 2010. Ketamine–xylazine–acepromazine compared with isoflurane for anesthesia during liver transplantation in rodents. J Am Assoc Lab Anim Sci 49:45–51.
23. Hill WA, Tubbs JT, Carter CL, Czarra JA, Newkirk KM, Sparer TE, Rohrbach B, Egger CM. 2013. Repeated administration of tribromoethanol in C57BL/6NHsd mice. J Am Assoc Lab Anim Sci 52:176–179.
24. Jaspar N, Mazzarelli M, Tessier C, Milic-Emili J. 1983. Effect of ketamine on control of breathing in cats. J Appl Physiol 55:851–859.
25. Kawai S, Takagi Y, Kaneko S, Kurosawa T. 2011. Effect of 3 types of mixed anesthetic agents alternate to ketamine in mice. Exp Anim 60:481–487.
26. Lavoie DS, Pailleux F, Vachon P, Beaudry F. 2013. Characteriza-tion of xylazine metabolism in rat liver microsomes using liquid chromatography–hybrid triple quadrupole–linear ion trap–mass spectrometry. Biomed Chromatogr 27:882–888.
27. Lieggi CC, Artwohl JE, Leszczynski JK, Rodriguez NA, Fickbohm BL, Fortman JD. 2005. Efficacy and safety of stored and newly prepared tribromoethanol in ICR mice. Contemp Top Lab Anim Sci 44:17–22.
28. Maxwell CR, Ehrlichman RS, Liang Y, Trief D, Kanes SJ, Karp J, Siegel SJ. 2005. Ketamine produces lasting disruptions in encoding of sensory stimuli. J Pharmacol Exp Ther 316:315–324.
29. McCashin FB, Gabel AA. 1975. Evaluation of xylazine as a sedative and preanesthetic agent in horses. Am J Vet Res 36:1421–1429.
30. Olson ME, Renchko P. 1988. Azaperone and azaperone–ketamine as a neuroleptic sedative and anesthetic in rats and mice. Lab Anim Sci 38:299–304.
31. Otto KA, Mally P. 2003. Noxious stimulation during orthopaedic surgery results in EEG ‘arousal’ or ‘paradoxical arousal’ reaction in isoflurane-anaesthetised sheep. Res Vet Sci 75:103–112.
32. Plumb DC. 2011. Plumb’s veterinary drug handbook, 7th ed. Ames (IA): John Wiley and Sons.
33. Rampil IJ. 1994. Anesthetic potency is not altered after hypother-mic spinal cord transection in rats. Anesthesiology 80:606–610.
34. Rampil IJ, Laster MJ. 1992. No correlation between quantitative electroencephalographic measurements and movement response to noxious stimuli during isoflurane anesthesia in rats. Anesthe-siology 77:920–925.
35. Rampil IJ, Mason P, Singh H. 1993. Anesthetic potency (MAC) is independent of forebrain structures in the rat. Anesthesiology 78:707–712.
36. Sarton E, Teppema LJ, Olievier C, Nieuwenhuijs D, Matthes HW, Kieffer BL, Dahan A. 2001. The involvement of the mu-opioid receptor in ketamine-induced respiratory depression and antinociception. Anesth Analg 93:1495–1500 [table of contents.].
essarily imply that the animals actually emerged sufficiently to regain consciousness or form memories. We caution that the administration of additional anesthetics while animals are still at a surgical plane of anesthesia may lead to unacceptable mortality rates.
In summary, when repeat-bolus dosing is used to extend the surgical plane of anesthesia in mice, we recommend frequent assessment of the PWR and redosing only once the reflex has returned. We recommend providing either 50% of the initial ketamine dose or 25% of the initial combined ketamine–xylazine as an effective and relatively safe protocol to extend the surgical plane of anesthesia in C57BL/6 mice.
AcknowledgmentsWe appreciate assistance provided by Ms Kyla Yeregui during her
externship in ULAR. This work was supported in part by funding from the Office of the Vice Provost for Research at the University of Pennsyl-vania. This project was supported in part by NIH grant 8R25OD010986. The contents of this report are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
References 1. Antognini JF, Barter L, Carstens E. 2005. Overview: movement as
an index of anesthetic depth in humans and experimental animals. Comp Med 55:413–418.
2. Antognini JF, Schwartz K. 1993. Exaggerated anesthetic require-ments in the preferentially anesthetized brain. Anesthesiology 79:1244–1249.
3. Arras M, Autenried P, Rettich A, Spaeni D, Rulicke T. 2001. Optimization of intraperitoneal injection anesthesia in mice: drugs, dosages, adverse effects, and anesthesia depth. Comp Med 51:443–456.
4. Aziz MA, Carlyle SS. 1978. Cardiovascular and respira-tory effects of xylazine in sheep. Zentralbl Veterinarmed A 25:173–180.
5. Barash PG, Clarence J; Marshall Memorial Library Fund. 2009. Clinical anesthesia, 6th ed. Philadelphia (PA): Wolters Kluwer–Lip-pincott Williams and Wilkins.
6. Bickler PE, Fahlman CS. 2006. The inhaled anesthetic isoflurane enhances Ca2+-dependent survival signaling in cortical neurons and modulates MAP kinases, apoptosis proteins, and transcription factors during hypoxia. Anesth Analg 103:419–429.
7. Bourke DL, Malit LA, Smith TC. 1987. Respiratory interactions of ketamine and morphine. Anesthesiology 66:153–156.
8. Buitrago S, Martin TE, Tetens-Woodring J, Belicha-Villanueva A, Wilding GE. 2008. Safety and efficacy of various combinations of injectable anesthetics in BALB/c mice. J Am Assoc Lab Anim Sci 47:11–17.
9. Burnside WM, Flecknell PA, Cameron AI, Thomas AA. 2013. A comparison of medetomidine and its active enantiomer dexme-detomidine when administered with ketamine in mice. BMC Vet Res 9:48.
10. Cesarovic N, Jirkof P, Rettich A, Nicholls F, Arras M. 2012. Combining sevoflurane anesthesia with fentanyl–midazolam or s-ketamine in laboratory mice. J Am Assoc Lab Anim Sci 51:209–218.
11. Cruz JI, Loste JM, Burzaco OH. 1998. Observations on the use of medetomidine–ketamine and its reversal with atipamezole for chemical restraint in the mouse. Lab Anim 32:18–22.
12. Dehghani S, Sharifnia N, Yahyaei MR, Souri A. 1991. Clinical, haemotological, and biochemical effects of xylazine, ketamine, and their combination in caprine and feline. Vet Anaesth Analg 18:129–133.
13. Elena G, Amerio N, Ferrero P, Bay ML, Valenti J, Colucci D, Puig NR. 2003. Effects of repetitive sevoflurane anaesthesia on immune response, select biochemical parameters, and organ histology in mice. Lab Anim 37:193–203.
14. Erhardt W, Hebestedt A, Aschenbrenner G, Pichotka B, Blumel G. 1984. A comparative study with various anesthetics in mice
jaalas14000039.indd 690 11/20/2014 11:28:46 AM

691
Repeat-bolus dosing for anesthesia of B6 mice.
37. Schneiders FI, Noble GK, Boston RC, Dunstan AJ, Sillence MN, McKinney AR. 2012. Acepromazine pharmacokinetics: a forensic perspective. Vet J 194:48–54.
38. Silva A, Antunes L. 2012. Electroencephalogram-based anaesthetic depth monitoring in laboratory animals. Lab Anim 46:85–94.
39. Smith W. 1993. Responses of laboratory animals to some injectable anaesthetics. Lab Anim 27:30–39.
40. Sonner JM, Gong D, Eger EI 2nd. 2000. Naturally occurring vari-ability in anesthetic potency among inbred mouse strains. Anesth Analg 91:720–726.
41. Teppema LJ, Baby S. 2011. Anesthetics and control of breathing. Respir Physiol Neurobiol 177:80–92.
42. Tranquilli WJ, Thurmon JC, Grimm KA, Lumb WV. 2007. Lumb and Jones’ veterinary anesthesia and analgesia, 4th ed. Ames (IA): Blackwell Publishing.
43. Valentim AM, Alves HC, Olsson IA, Antunes LM. 2008. The effects of depth of isoflurane anesthesia on the performance of mice in a simple spatial learning task. J Am Assoc Lab Anim Sci 47:16–19.
44. Veilleux-Lemieux D, Beaudry F, Hélie P, Vachon P. 2012. Effects of endotoxemia on the pharmacodynamics and pharmacokinetics of ketamine and xylazine anesthesia in Sprague–Dawley rats. Veterinary Medicine: Research and Reports 3:99–109.
45. Veilleux-Lemieux D, Castel A, Carrier D, Beaudry F, Vachon P. 2013. Pharmacokinetics of ketamine and xylazine in young and old Sprague–Dawley rats. J Am Assoc Lab Anim Sci 52:567–570.
46. Waxman K, Shoemaker WC, Lippmann M. 1980. Cardiovascular ef-fects of anesthetic induction with ketamine. Anesth Analg 59:355–358.
47. Welberg LA, Kinkead B, Thrivikraman K, Huerkamp MJ, Ne-meroff CB, Plotsky PM. 2006. Ketamine–xylazine–acepromazine anesthesia and postoperative recovery in rats. J Am Assoc Lab Anim Sci 45:13–20.
48. Xu Q, Ming Z, Dart AM, Du XJ. 2007. Optimizing dosage of ketamine and xylazine in murine echocardiography. Clin Exp Pharmacol Physiol 34:499–507.
49. Zbinden AM, Maggiorini M, Petersen-Felix S, Lauber R, Thom-son DA, Minder CE. 1994. Anesthetic depth defined using multiple noxious stimuli during isoflurane–oxygen anesthesia. I. Motor reactions. Anesthesiology 80:253–260.
50. Zuurbier CJ, Emons VM, Ince C. 2002. Hemodynamics of anes-thetized ventilated mouse models: aspects of anesthetics, fluid support, and strain. Am J Physiol Heart Circ Physiol 282:H2099–H2105.
jaalas14000039.indd 691 11/20/2014 11:28:47 AM














![Animal in Animal Imaging'12 - University of Arizona · irritant effect on CNS (epileptiform activity seen on EEG) [Goble, E. and Ruhnke, A. Adverse Drug Reaction Bull 2009] – Use](https://img.pdfslide.us/doc/110x75/5eb7b5f8022e29278f78be7f/animal-in-animal-imaging12-university-of-arizona-irritant-effect-on-cns-epileptiform.jpg)