Embed Size (px)
Citation preview
Berghold, IMI, MUG
Biostatistics
Univ.-Prof. DI Dr. Andrea Berghold
Institute for Medical Informatics, Statisticsand Documentation
Medical University of Graz
Berghold, IMI, MUG
Content
• Introduction to Medical Statistics
• Study designs in medical research with emphasis on clinical trials
• Exploring and summarizing data
• Populations and samples
• Statements of probability and confidence intervals
• Drawing inferences from data - Hypothesis testing
• Estimating and comparing means
• Proportions and chi-square tests
• Correlation and regression
• Diagnostic tools
• Methods for analysing survival data
Berghold, IMI, MUG
Literature
• Martin Bland: An Introduction to Medical Statistics. 3rd ed. Oxford University Press, 2000.
• Douglas Altman: Practical Statistics for Medical Research. Chapman & Hall.
• Aviva Petrie and Caroline Sabin: Medical Statistics at a Glance.Blackwell Science, 2000
• …
Berghold, IMI, MUG
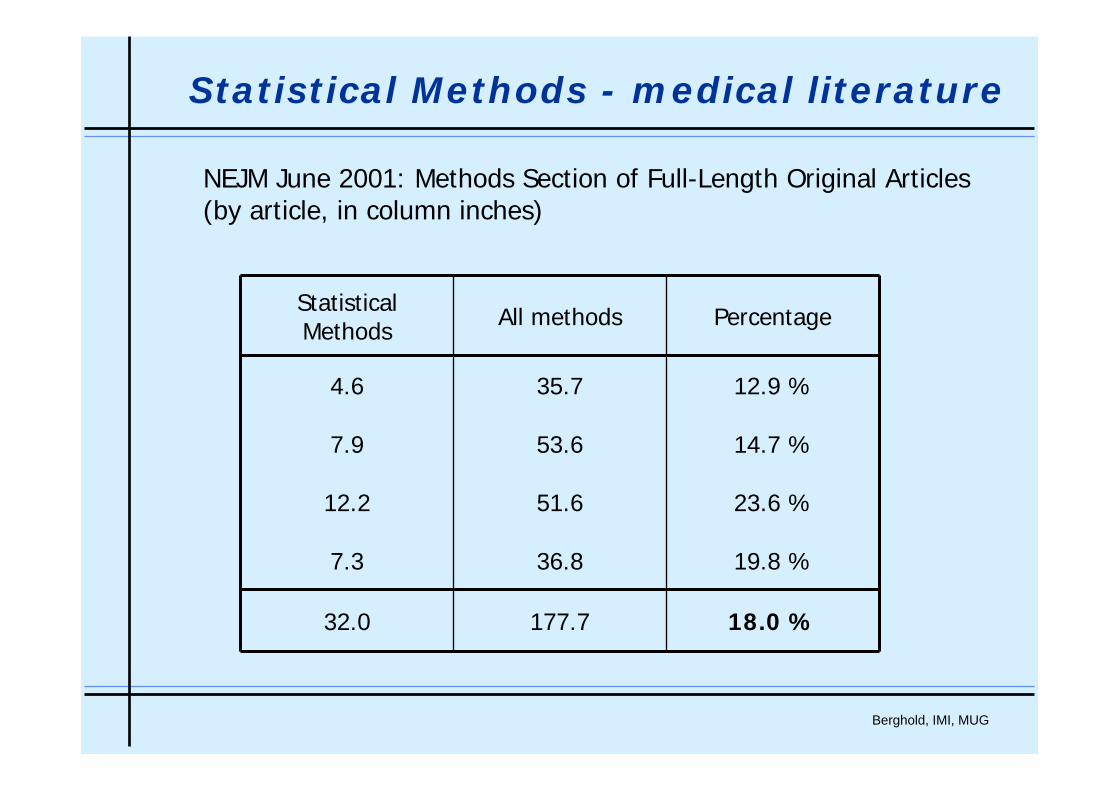
NEJM June 2001: Methods Section of Full-Length Original Articles(by article, in column inches)
Statistical Methods - medical literature
PercentageAll methodsStatisticalMethods
12.9 %35.74.6
14.7 %53.67.9
23.6 %51.612.2
19.8 %36.87.3
18.0 %177.732.0
Berghold, IMI, MUG
In the same issue the following statistical methods were mentioned:
Statistical Methods - medical literature
• Bonferroni method
• Chi-square test for independence
• Chi-square test for goodness-of-fit
• Confidence intervals
• Cox proportional hazards models
• Cumulative mortality
• Fisher's exact test
• Intention-to-treat analysis
• Interim analysis
• Kaplan-Meier survival curves
• Logistic regression
• Logrank test
• Mantel-Haenszel adjusted relative risks
• Noninferiority testing
• Odds ratio
• Power Analysis
• P-values
• Randomization
• Relative risk reduction
• Repeated measures ANOVA
• Sample size estimation
• Spearman correlation
• t-tests
• Wilcoxon test
Berghold, IMI, MUG
Is it worth to struggle with statistics?
Bad statistics leads to bad research,
and bad research is unethical
Altman (1982)
Statistics
Berghold, IMI, MUG
• Design of studies- How do I get adequate data?
• Data analysis using statistical methods- What do I do with the data?
• Critical appraisal- How do I interpret study results?
Biostatistics - Medical Statistics
Berghold, IMI, MUG
Study
interpret
analyse data
collect data
plan study
Berghold, IMI, MUG
1. Stating the problem
• Major objective of the study -determine relevant variables und factors
• Search the literature, discussion with experts
Study
2. Designing the study
• Study design, sample size calculation etc.
• Statistical analysis plan
• Study protocol
Berghold, IMI, MUG
A Study
3. Collecting data
• Collecting data and plausibility checks
4. Data analysis
• Graphs and summary statistics
• Statistical inference
5. Interpretation of results and conclusions
• Discussion of new information
Berghold, IMI, MUG
Some questions which should be answered in advance:
Stating the problem
• What is the major objective of the study?
• Is the question clearly defined?
• Is it also relevant?
Berghold, IMI, MUG
1. Are there differences in the one-year rate of restenosis usingstents or PTA with stenosis of arteria iliaca?
2. Does a betablocker decrease all-cause mortality in patientswith chronic heart failure?
3. Have cancer patients who have anemia a worse prognosisthan patients without anemia?
4. Which method should be used for training of laparascopicsurgery?
5. …
Examples
Berghold, IMI, MUG
• Primary variable, endpoint1. rate of restenosis;2. all-cause mortality;3. 5 year disease-specific survival;4. number of stitches per minute; …
• Factors1. none2. stage (NYHA); 3. anemia, size of tumour, lymph nodes;4. method, playing an instrument; ...
• Other factorsAge, sex, smoking ....
Variables
Berghold, IMI, MUG
• Random error
• inter- and intraindividual variability
• Systematic error - Bias
• Selection bias
• Assessment bias
• Information bias
• …
Try to avoid bias and reduce random error as much as possible.
Errors
Berghold, IMI, MUG
Types of studies
• Observational studies
• Experimental studies
Berghold, IMI, MUG
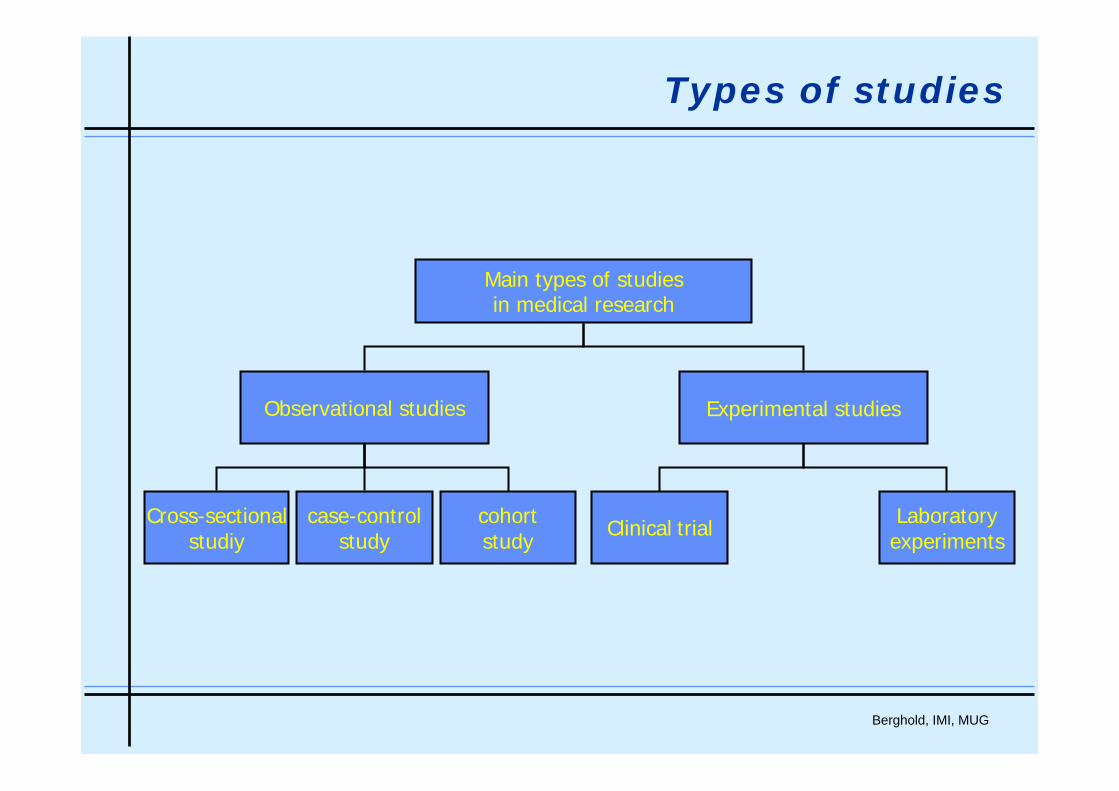
Types of studies
Main types of studiesin medical research
Observational studies Experimental studies
Cross-sectionalstudiy
case-controlstudy
cohortstudy Clinical trial Laboratory
experiments
Berghold, IMI, MUG
Observational Studies
Berghold, IMI, MUG
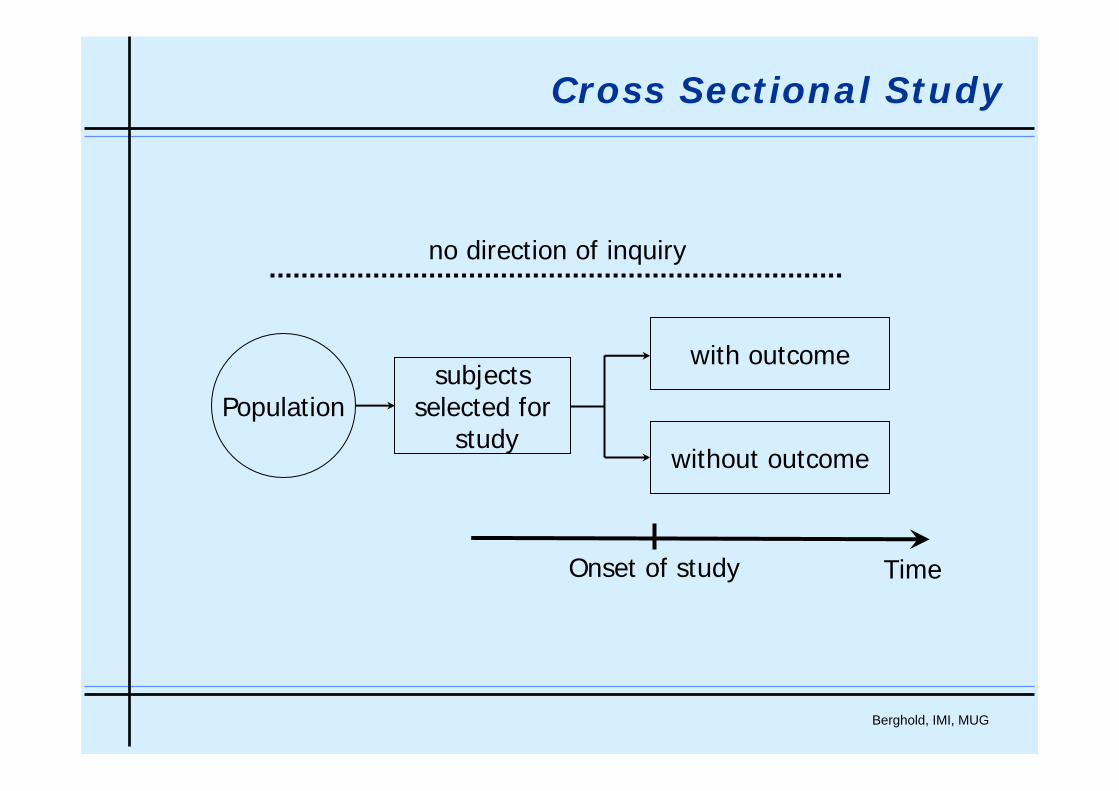
Cross Sectional Study
Populationsubjects
selected forstudy
with outcome
without outcome
Onset of study Time
no direction of inquiry
Berghold, IMI, MUG
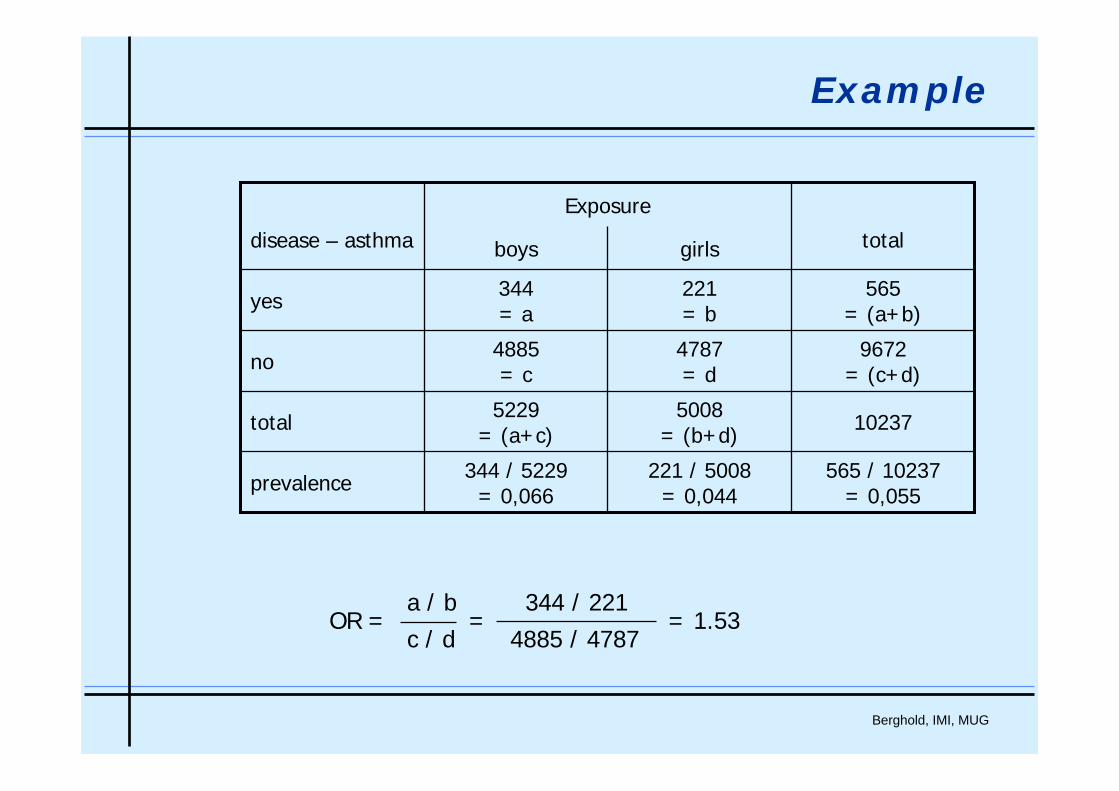
Example
565 / 10237= 0,055
221 / 5008= 0,044
344 / 5229= 0,066prevalence
102375008= (b+d)
5229= (a+c)total
9672= (c+d)
4787= d
4885= cno
565= (a+b)
221= b
344= ayes
totalgirlsboysdisease – asthma
Exposure
OR = = = 1.53a / b 344 / 221c / d 4885 / 4787
Berghold, IMI, MUG
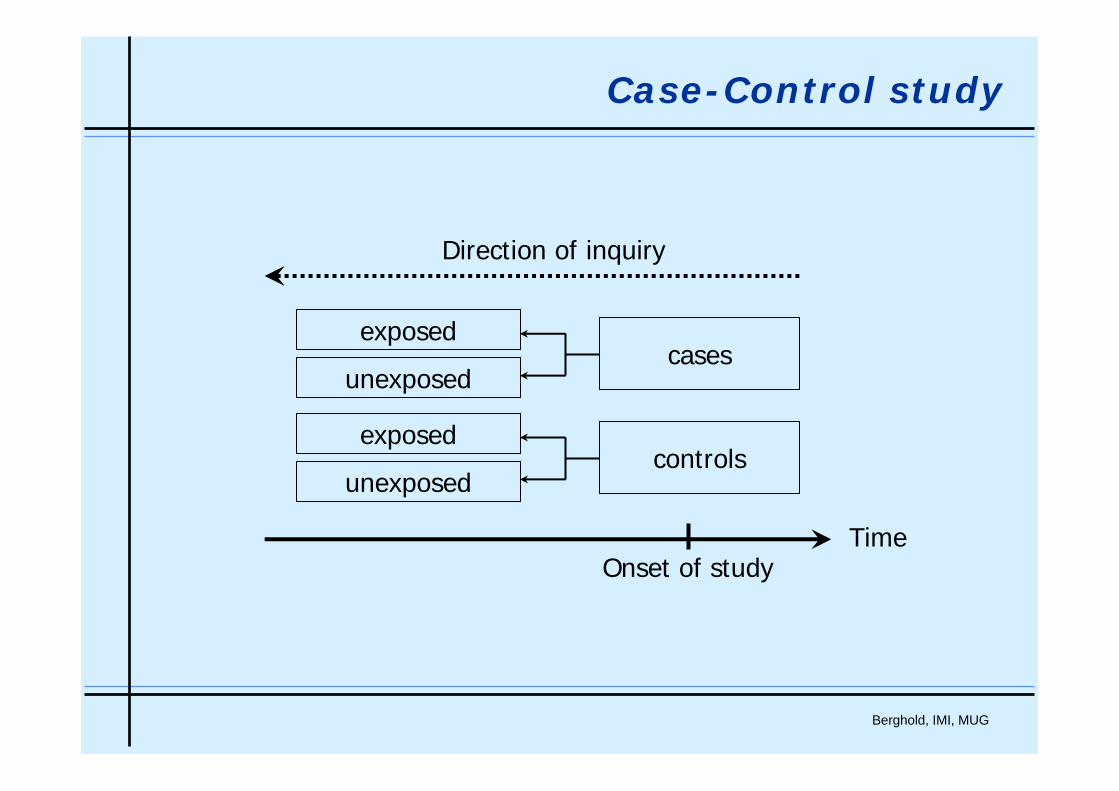
Case-Control study
cases
controls
exposed
unexposed
exposed
unexposed
Onset of studyTime
Direction of inquiry
Berghold, IMI, MUG
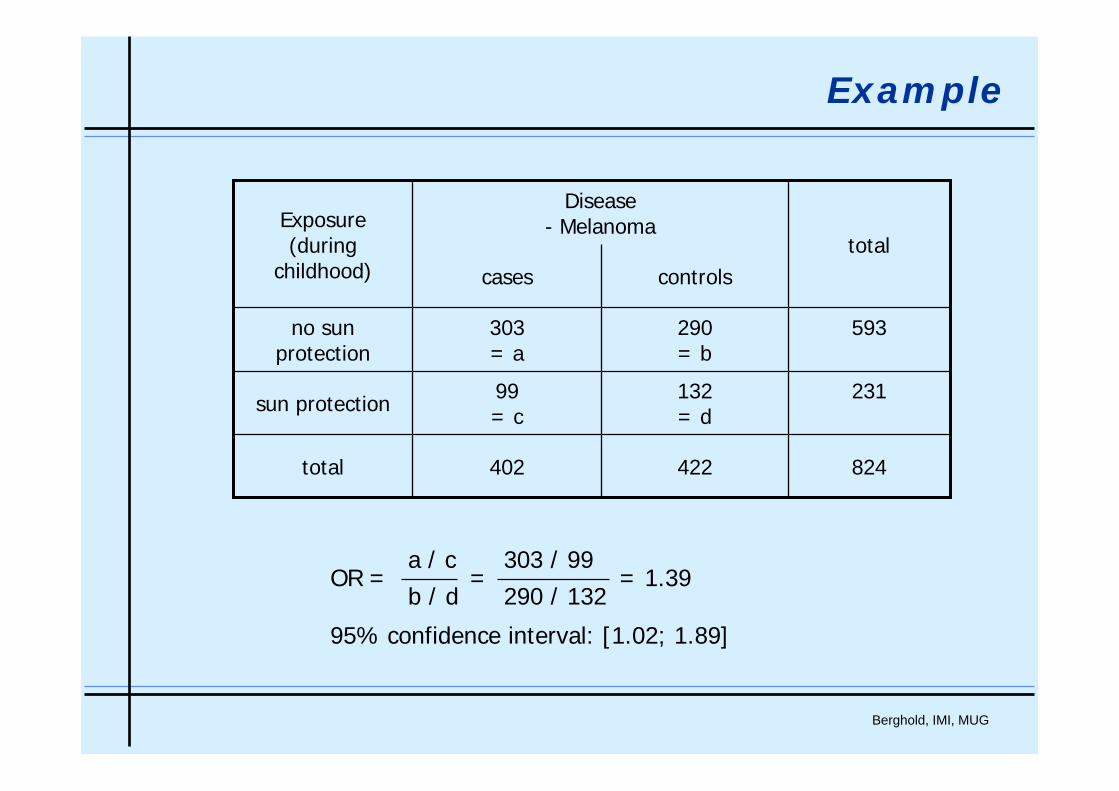
Example
824422402total
231132= d
99= csun protection
593290= b
303= a
no sunprotection
totalcontrolscases
Exposure(during
childhood)
Disease- Melanoma
OR = = = 1.39
95% confidence interval: [1.02; 1.89]
a / c 303 / 99b / d 290 / 132
Berghold, IMI, MUG
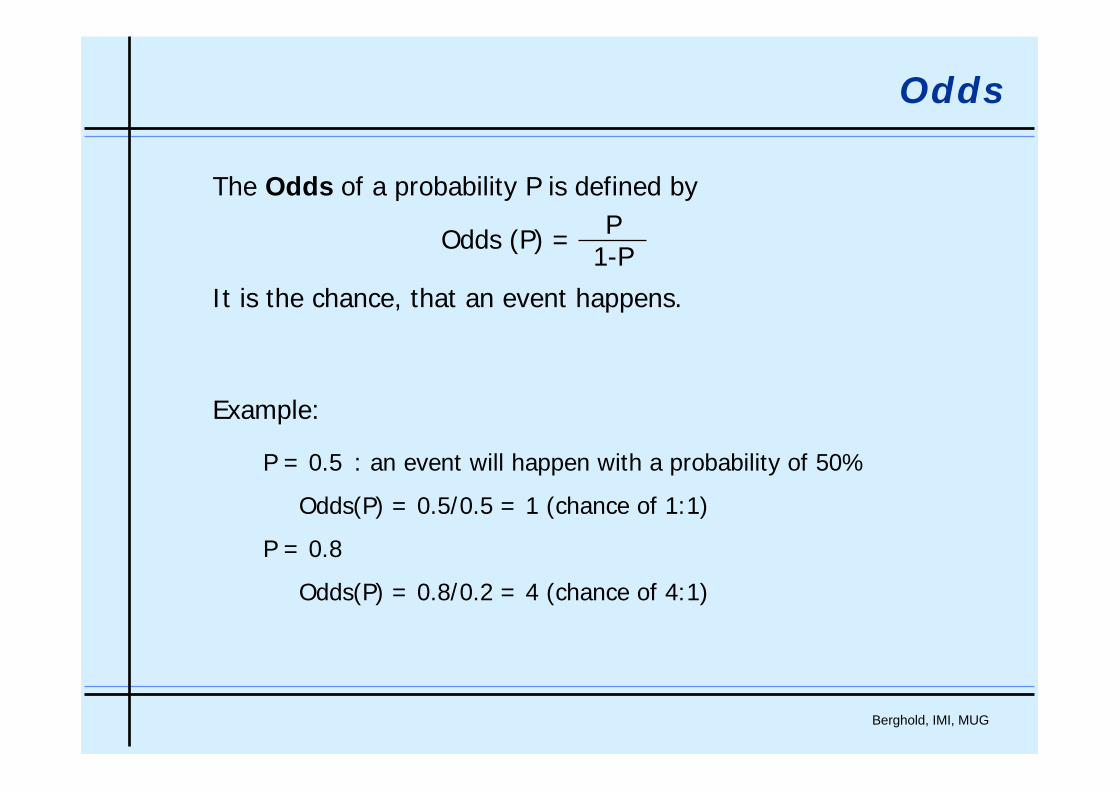
Odds
The Odds of a probability P is defined by
It is the chance, that an event happens.
Example:
P = 0.5 : an event will happen with a probability of 50%
Odds(P) = 0.5/0.5 = 1 (chance of 1:1)
P = 0.8
Odds(P) = 0.8/0.2 = 4 (chance of 4:1)
Odds (P) = P1-P
Berghold, IMI, MUG
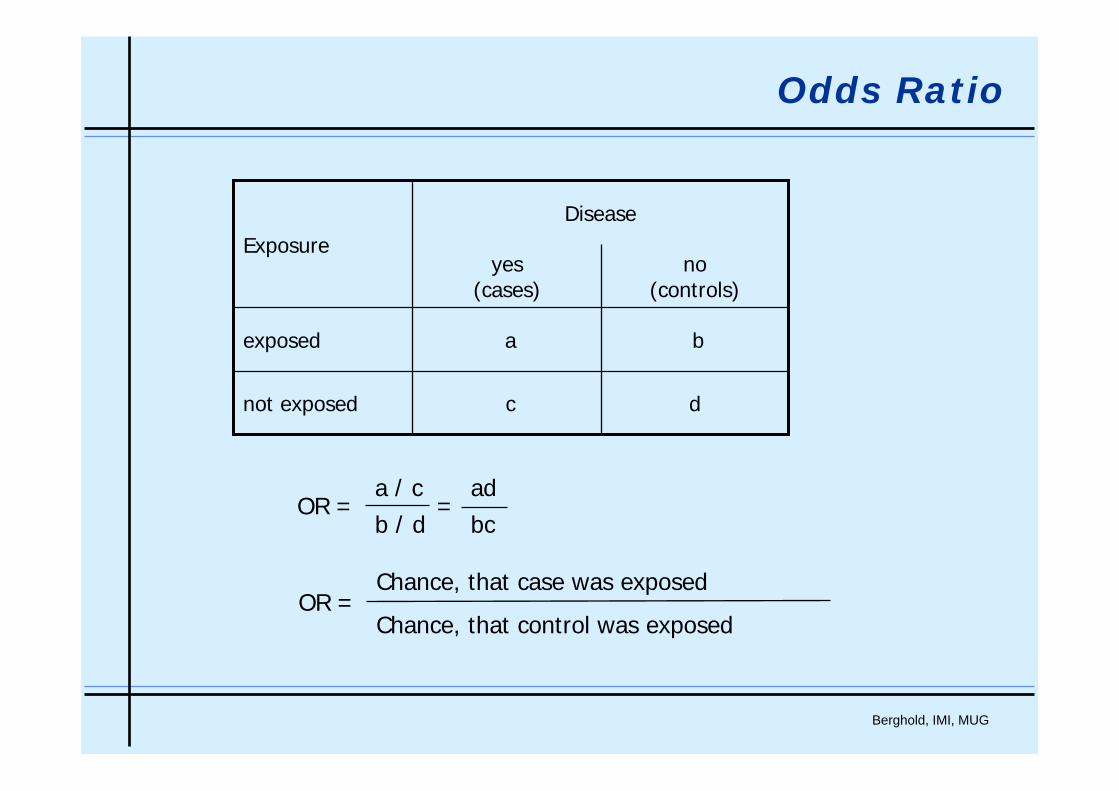
Odds Ratio
dcnot exposed
baexposed
no(controls)
yes(cases)
ExposureDisease
OR = =a / c adb / d bc
OR =Chance, that case was exposed
Chance, that control was exposed
Berghold, IMI, MUG
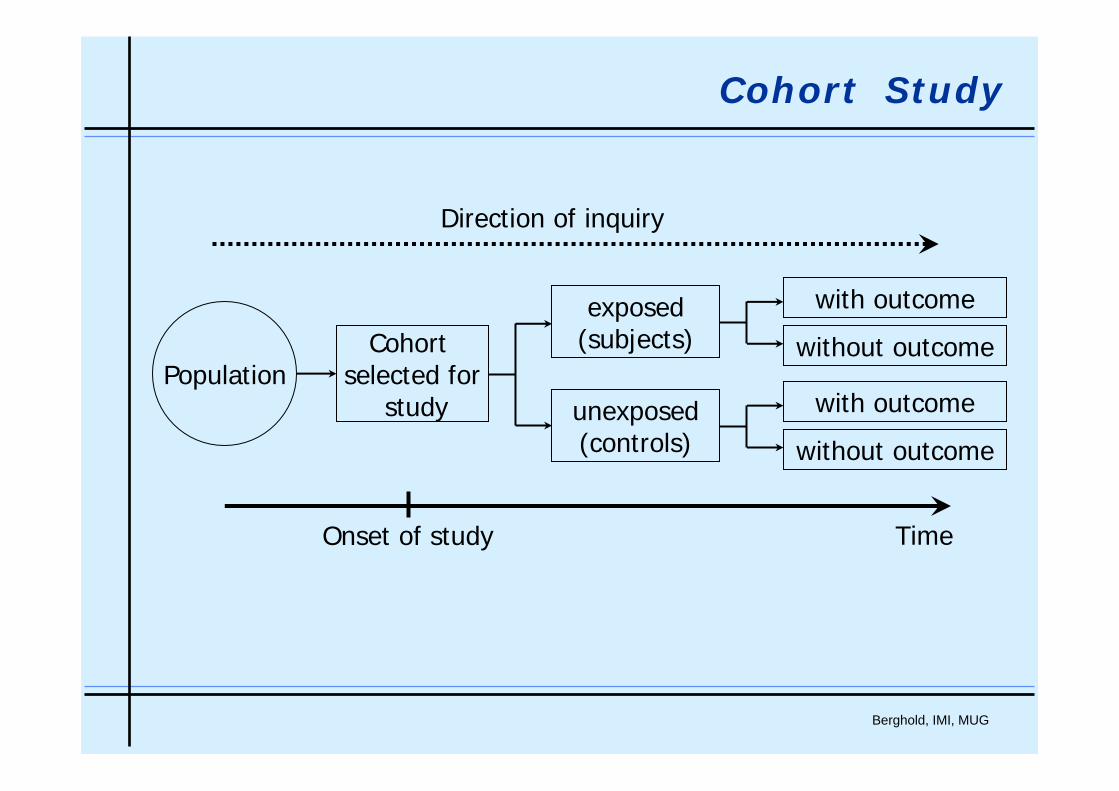
Cohort Study
PopulationCohort
selected forstudy
exposed(subjects)
unexposed(controls)
with outcome
without outcome
with outcome
without outcome
Onset of study Time
Direction of inquiry
Berghold, IMI, MUG
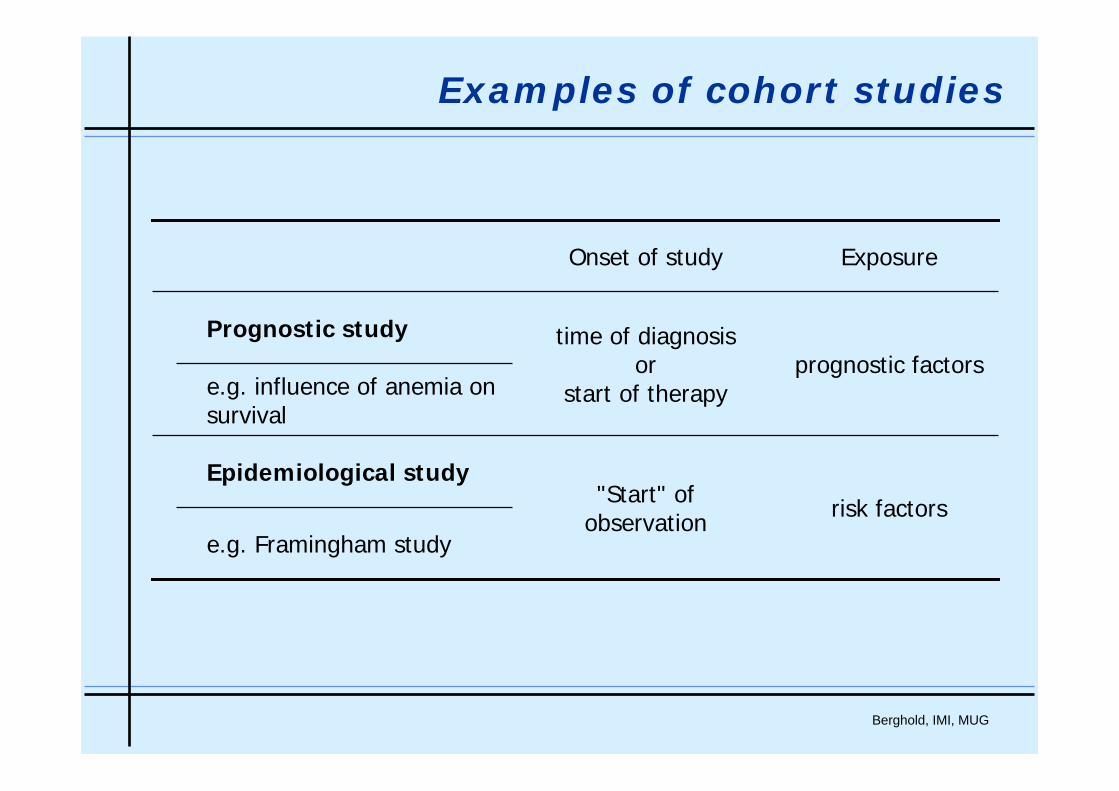
Examples of cohort studies
e.g. Framingham study
Prognostic study
risk factors"Start" of observation
Epidemiological study
prognostic factorstime of diagnosis
orstart of therapye.g. influence of anemia on
survival
ExposureOnset of study
Berghold, IMI, MUG
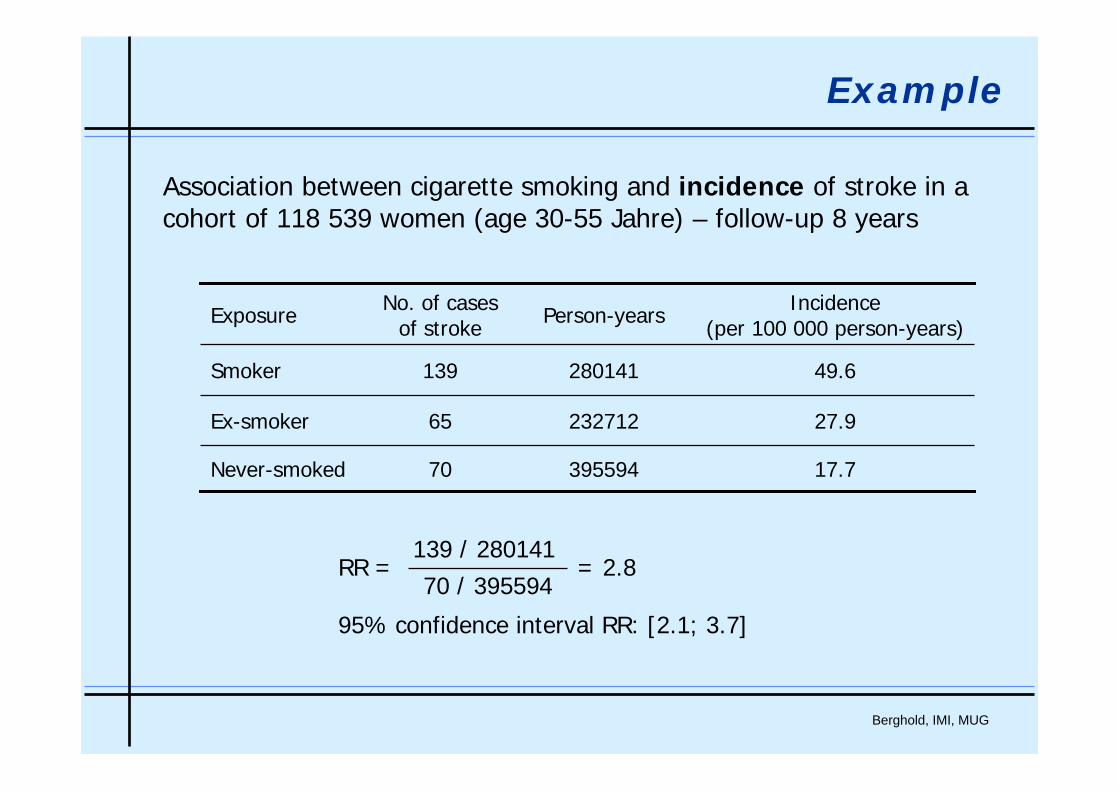
Example
Association between cigarette smoking and incidence of stroke in a cohort of 118 539 women (age 30-55 Jahre) – follow-up 8 years
27.923271265Ex-smoker
17.7
49.6
Incidence(per 100 000 person-years)
39559470Never-smoked
280141139Smoker
Person-yearsNo. of casesof strokeExposure
RR = = 2.8
95% confidence interval RR: [2.1; 3.7]
139 / 28014170 / 395594
Berghold, IMI, MUG
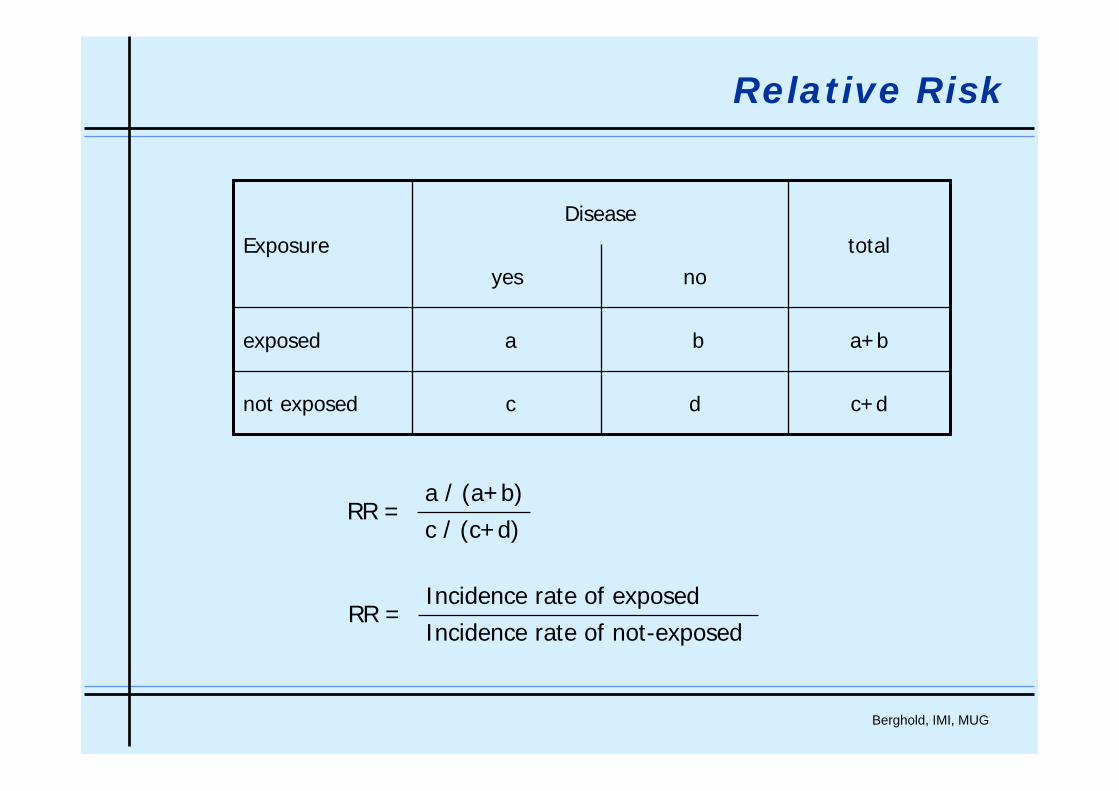
Relative Risk
c+ddcnot exposed
a+bbaexposed
totalnoyes
ExposureDisease
RR =a / (a+b)c / (c+d)
RR =Incidence rate of exposedIncidence rate of not-exposed
Berghold, IMI, MUG
Experimental Studies
Berghold, IMI, MUG
Comparison of the efficacy of different drugs, therapies, vaccinesetc. after controlling for confounders (e.g. age, sex, stage of disease).
Clinical trial
Aim:
Observed differences in success rates betweentreatment groups can exclusively be put down to thefact that differences are caused by the efficacy of the
different treatments.
Berghold, IMI, MUG
Statistical issues
• The efficacy and safety of treatments have to be judgedagainst a background of biological variability
• In designing studies, two main points have to be kept in mind:
• the effect of bias
• the effect of chance
Berghold, IMI, MUG
Focus
• Comparative trials:
• Interested in treatment effect and treatment comparisons
• Concurrent control group• Investigate a new experimental intervention versus placebo or a
“standard” intervention• compare two alternative commonly-used interventions with each
other• Study the result of adding an additional agent to a standard regimen• Compare different doses or intensities of an intervention
• Pre-defined study objective
Berghold, IMI, MUG
Design techniques to avoid bias
• Randomization
• Blinding
„The most important design techniques for avoiding bias in clinical trials are blinding and randomisation.“ (ICH E9: Statistical Principles in Clinical Trials)
Berghold, IMI, MUG
Randomization
• To allocate treatments to subjects in a trial at random (usingcoins, dice, random number tables or generators)
• Allocation concealment
• Neither the subject nor the investigator knows ahead of time what treatment the subject will receive
• Benefits:
• Eliminates assignment basis – avoids selection bias
• Tends to produce comparable groups
• Statistical basis for a valid treatment comparison
Berghold, IMI, MUG
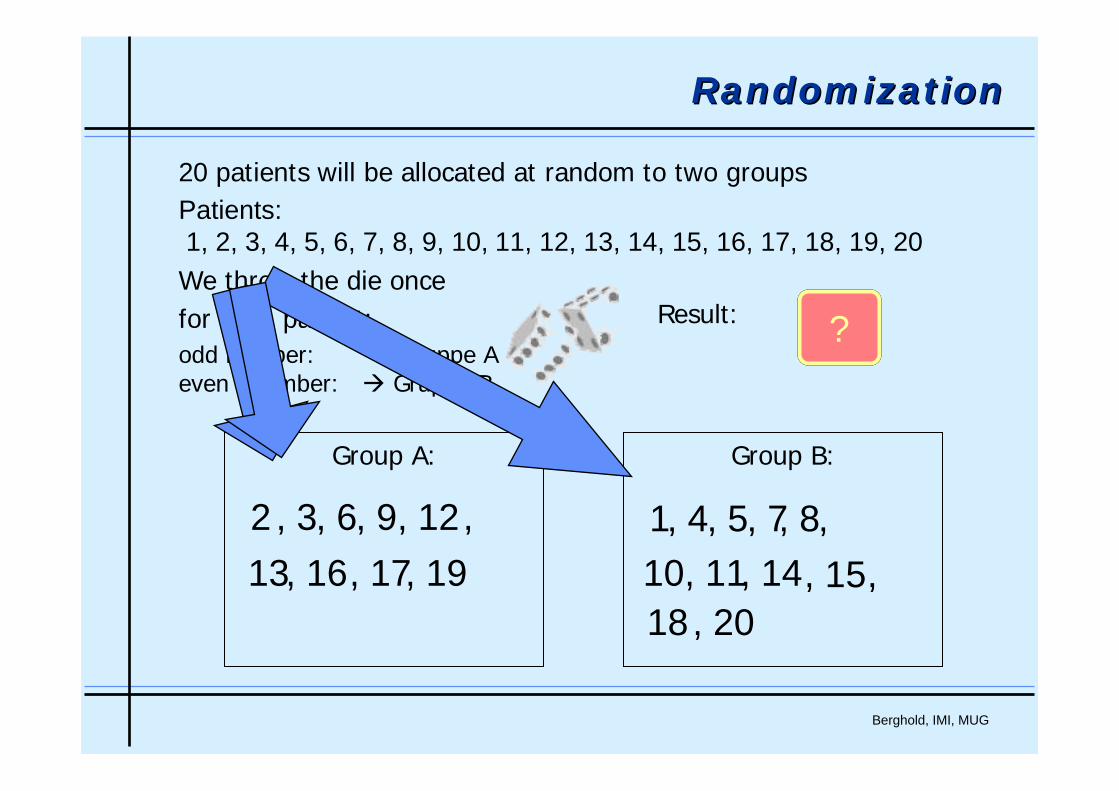
20 patients will be allocated at random to two groupsPatients:1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20We throw the die oncefor each patient:odd number: Gruppe Aeven nuumber: Gruppe B
Group A: Group B:
Result: ?2
1
?5
2
?3
, 3
?
, 4, 5, 6 , 7, 8, 910
,, 11
, 1213
,, 14, 15, 16, 17
18,, 19
, 20
RandomizationRandomization
Berghold, IMI, MUG
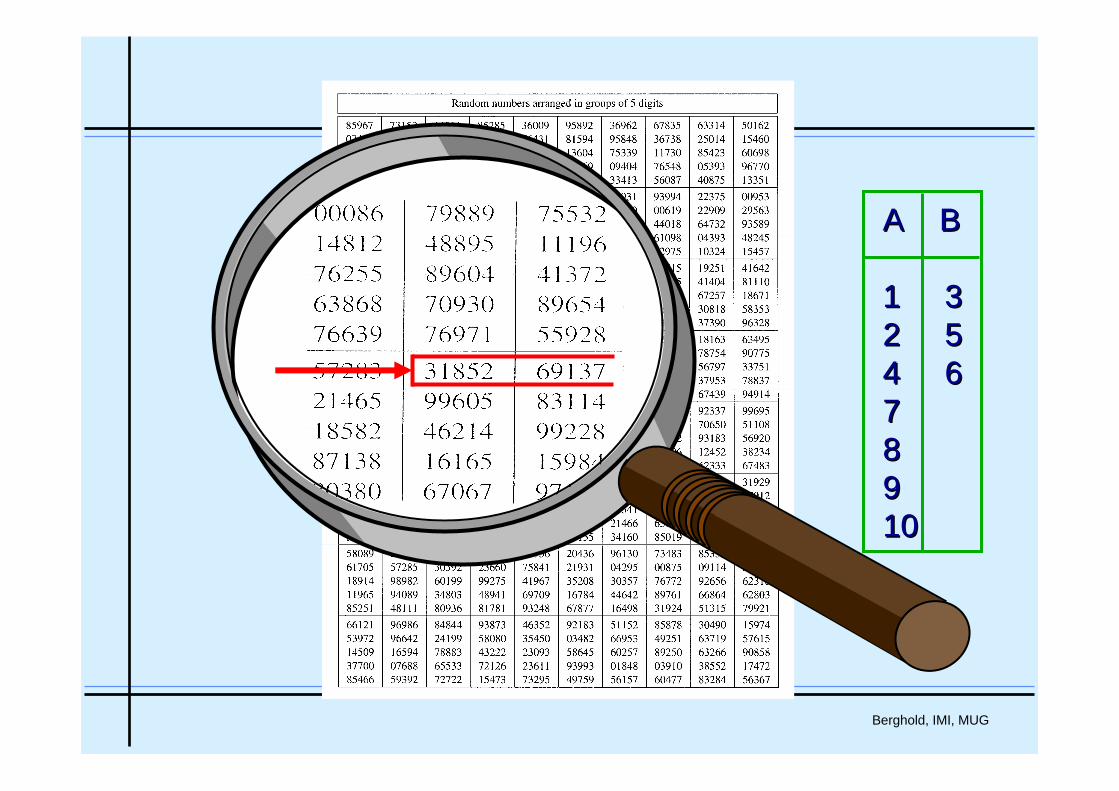
A BA B
1 31 32 52 54 64 677889910 10
Berghold, IMI, MUG
Restricted randomization
• Disadvantages of simple randomization:
• No guarantee of equal or approximately equal sample size in eachtreatment group at any stage of the trial
• With n = 20 on two treatments A and B, the chance of a 12:8 split or worse is approximately 0.19
• No protection against long runs of one treatment• Subject characteristics may change over time
• Restricted randomization:
Permuted blocks (Matts & Lachin)Biased coin (Efron)Urn design (Wei)Big Stick (Soares & Wu)…
Berghold, IMI, MUG
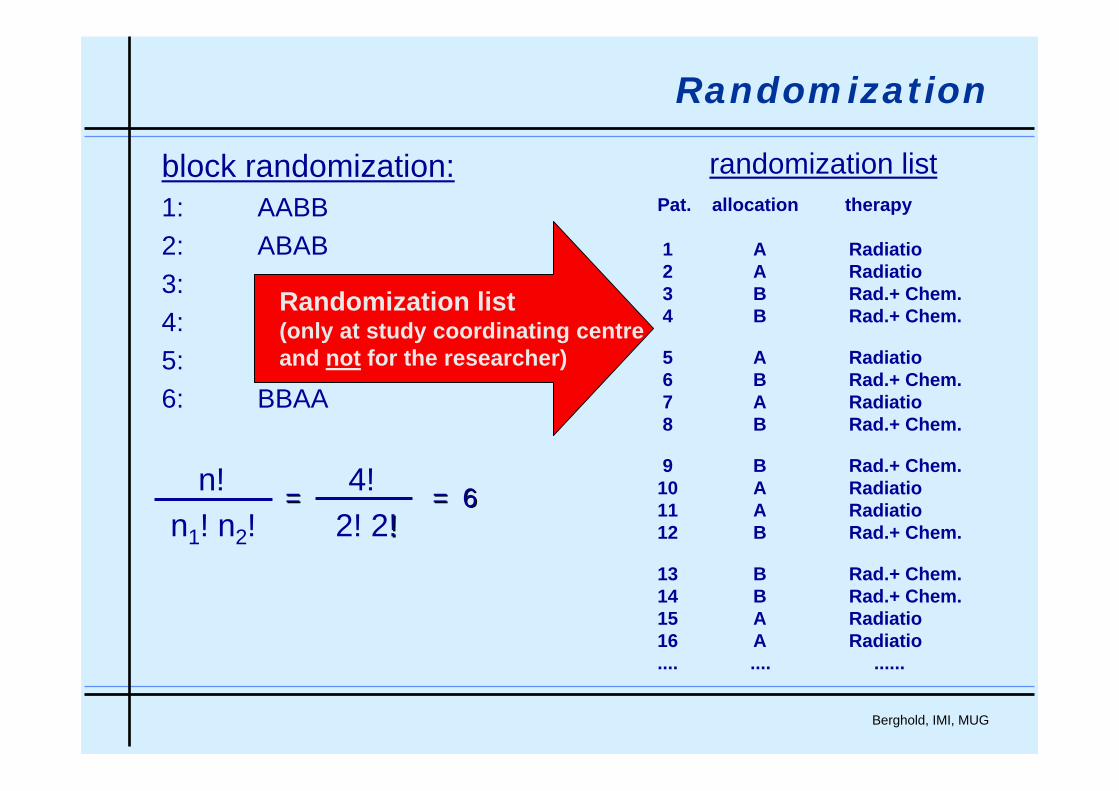
Pat. allocation therapy
1 A Radiatio2 A Radiatio3 B Rad.+ Chem.4 B Rad.+ Chem.
5 A Radiatio6 B Rad.+ Chem.7 A Radiatio8 B Rad.+ Chem.
9 B Rad.+ Chem.10 A Radiatio11 A Radiatio12 B Rad.+ Chem.
13 B Rad.+ Chem.14 B Rad.+ Chem.15 A Radiatio16 A Radiatio.... .... ......
randomization listblock randomization:1: AABB2: ABAB3: ABBA4: BABA5: BAAB6: BBAA
n! 4!n1! n2! 2! 2!!
= = 6= = 6
Randomization list(only at study coordinating centreand not for the researcher)
Randomization
Berghold, IMI, MUG
Stratified randomization
• Balance treatment groups with respect to prognostic factors
• For large studies, randomization “tends” to give balance
• For smaller studies a better guarantee may be needed
• Common factors used for stratification - e.g. clinical centre, age, sex, disease severity
• Define strata – e.g. Age: < 40, 40-60, > 60;Sex: M, F (3 x 2 strata)
• Randomization is performed within each stratum and is usually blocked
• Rule of thumb – use as few stratification factors as possible
Berghold, IMI, MUG
Randomized controlled trials
The trial carried out by the Medical Research Council (MRC, 1948) to test the efficacy of streptomycin for the treatment of pulmonarytuberculosis is generally considered to be the first randomizedexperiment in medicine.
target population: patients with progressive bilateral pulmonarytuberculosis (bacterially proven), aged 15-30 years
107 patients in 3 centers were allocated by a series of randomnumbers drawn up for each sex at each centre.
Berghold, IMI, MUG
Implementation
• Sequenced sealed envelopes
• Phone call / fax to trial coordination centre
• Interactive Voice Response Systems
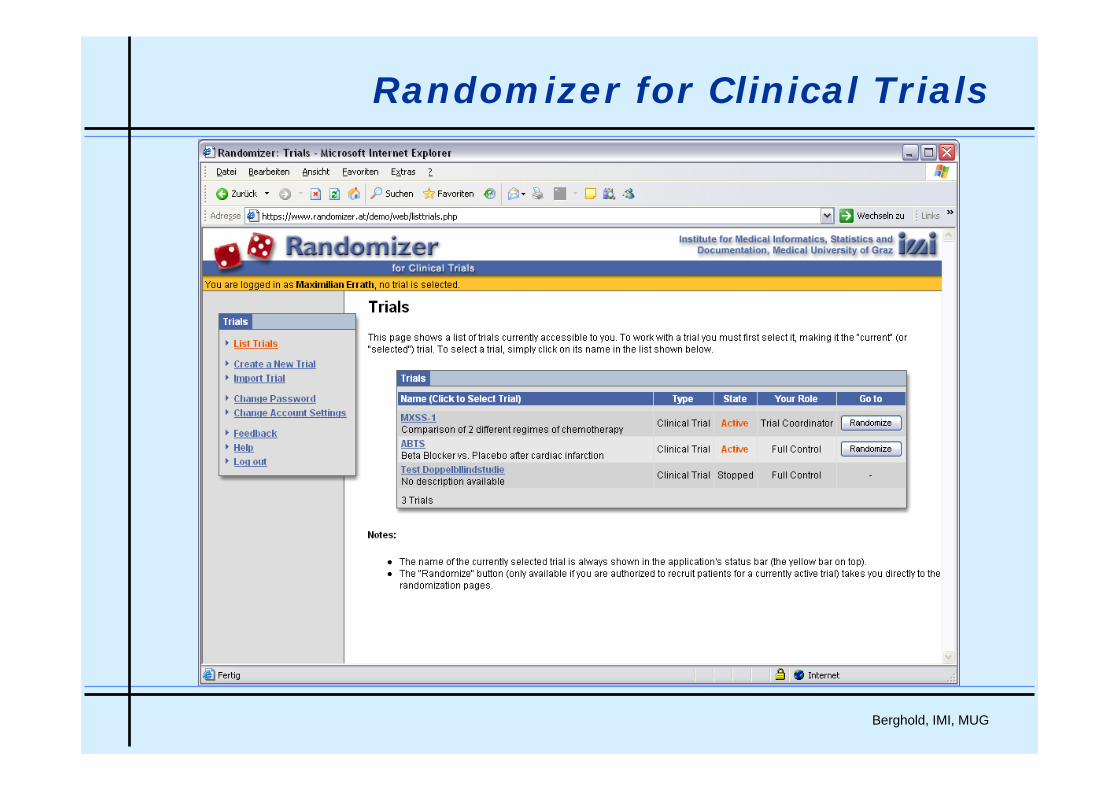
• Internet-based Systems (e.g. Randomizer for Clinical Trials)
Berghold, IMI, MUG
Randomizer for Clinical Trials

Berghold, IMI, MUG
Online Randomization
www.randomizer.at
Berghold, IMI, MUG
Blinding - Masking
• To limit the occurrence of bias in the conduct and interpretation of the trial (in the care, the assessment of endpoints, the attitude of subjects to treatments etc.)
• Double-blind: neither subject nor investigator/staff are awareof the treatment received
• placebo, “double dummy”, masked vials
• blinding may not be possible• surgical versus medical intervention• one intervention has obvious side-effect
• Outcome assessed by masked observer
• Single-blind
• Open-label trial
Berghold, IMI, MUG
Randomized controlled trials
• Choice of target population
Selection of patients: Definition of target population usinginclusion and exclusion criteria
• Trial Design
• Parallel – Design
• Cross-Over – Design
Berghold, IMI, MUG
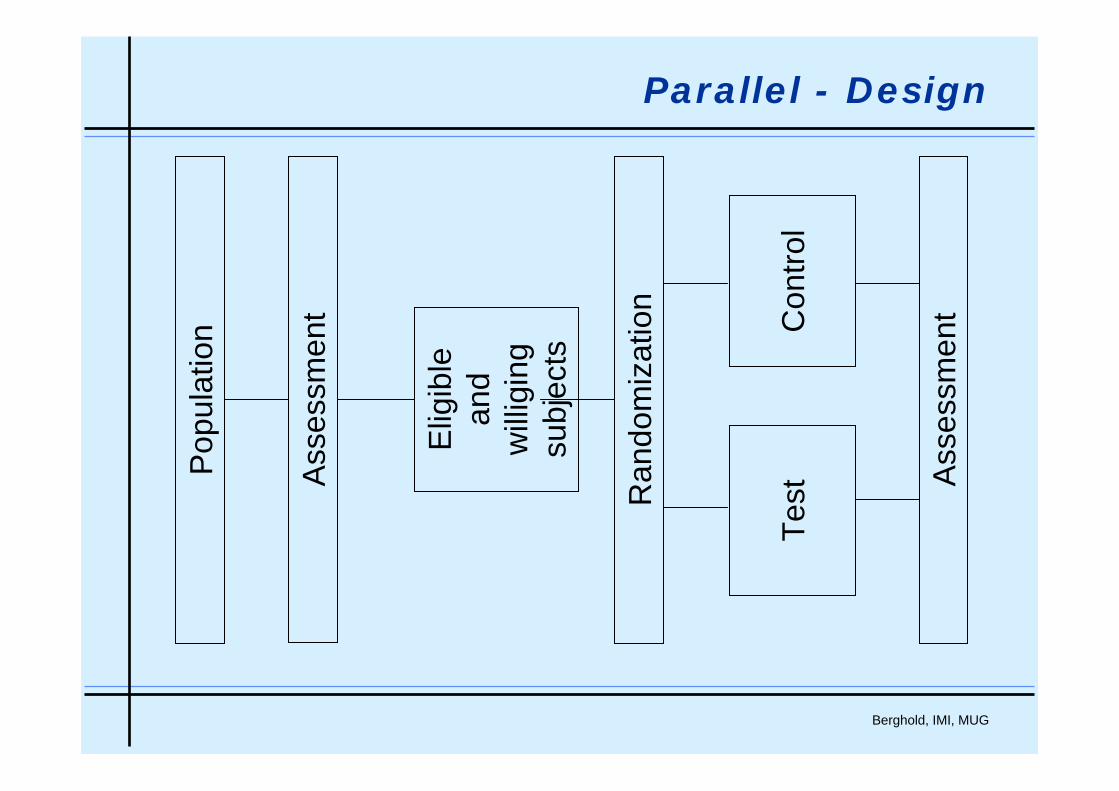
Parallel - Design
Elig
ible
and
will
igin
gsu
bjec
ts
Con
trol
Ran
dom
izat
ion
Ass
essm
ent
TestA
sses
smen
t
Pop
ulat
ion
Berghold, IMI, MUG
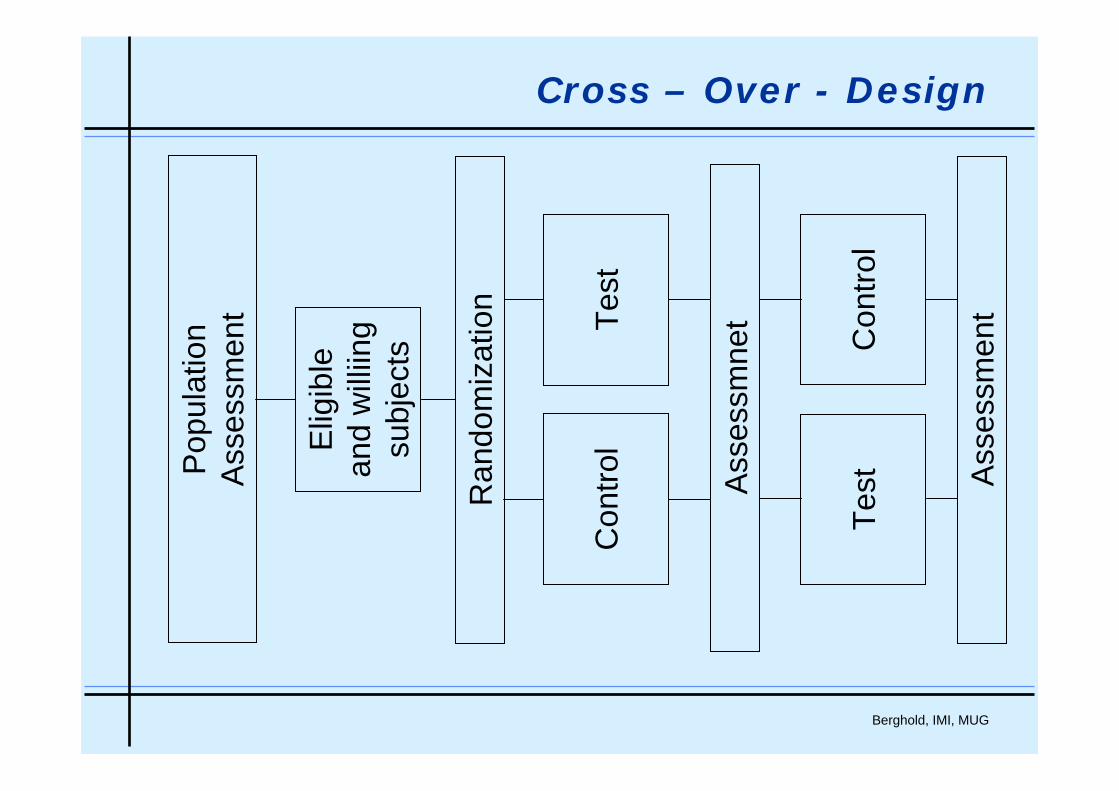
Cross – Over - Design
Ran
dom
izat
ion
Ass
essm
ent
Pop
ulat
ion
Ass
essm
ent
Ass
essm
net
Con
trol
Con
trol
Elig
ible
and
will
iing
subj
ects
Test
Test
Berghold, IMI, MUG
• The statistical analysis has to be defined before the study iscarried out
• Statistical analysis plan (SAP)
• Population used for analysis:
• All-Randomized patients
• Per-Protocol patients
• Safety population
Statistical analysis
Berghold, IMI, MUG
Intention-to-Treat
all randomized patients must be included in the analysis -
they have to be included in the group they were randomised to, independent of what happened after randomization.
Berghold, IMI, MUG
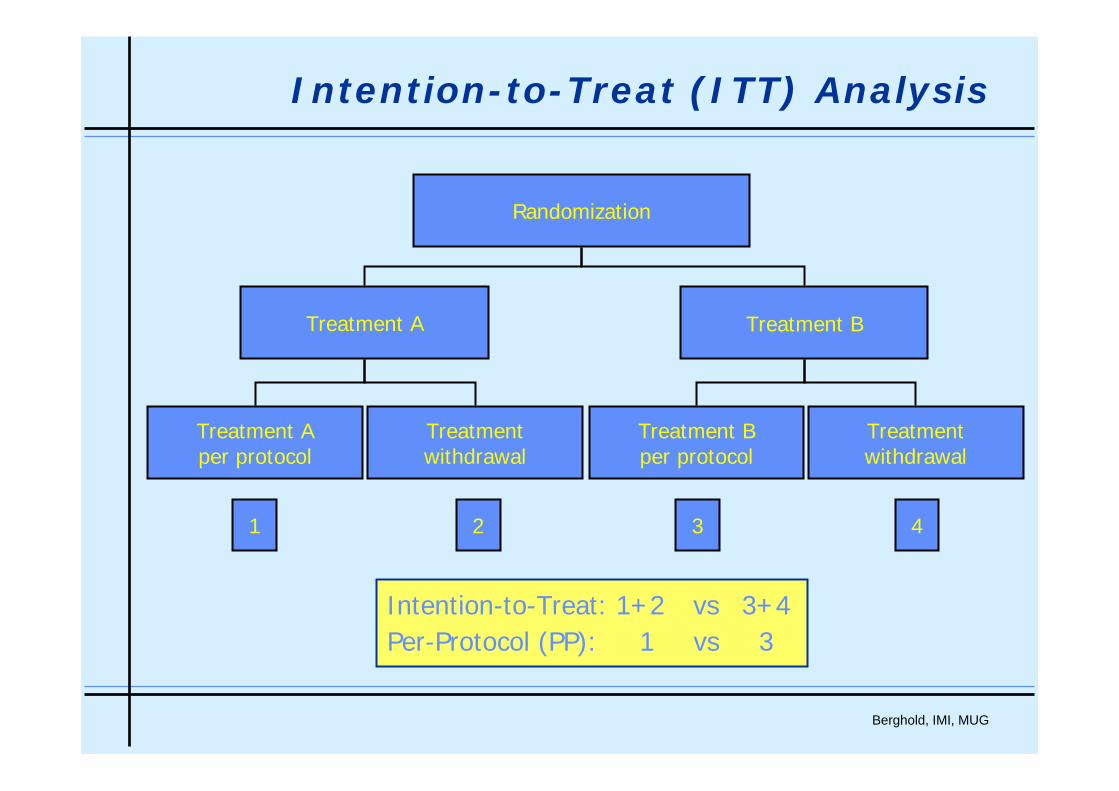
Intention-to-Treat (ITT) Analysis
Randomization
Treatment A Treatment B
Treatment Aper protocol
Treatmentwithdrawal
Treatment Bper protocol
Treatmentwithdrawal
Intention-to-Treat: 1+2 vs 3+4Per-Protocol (PP): 1 vs 3
1 2 3 4
Berghold, IMI, MUG
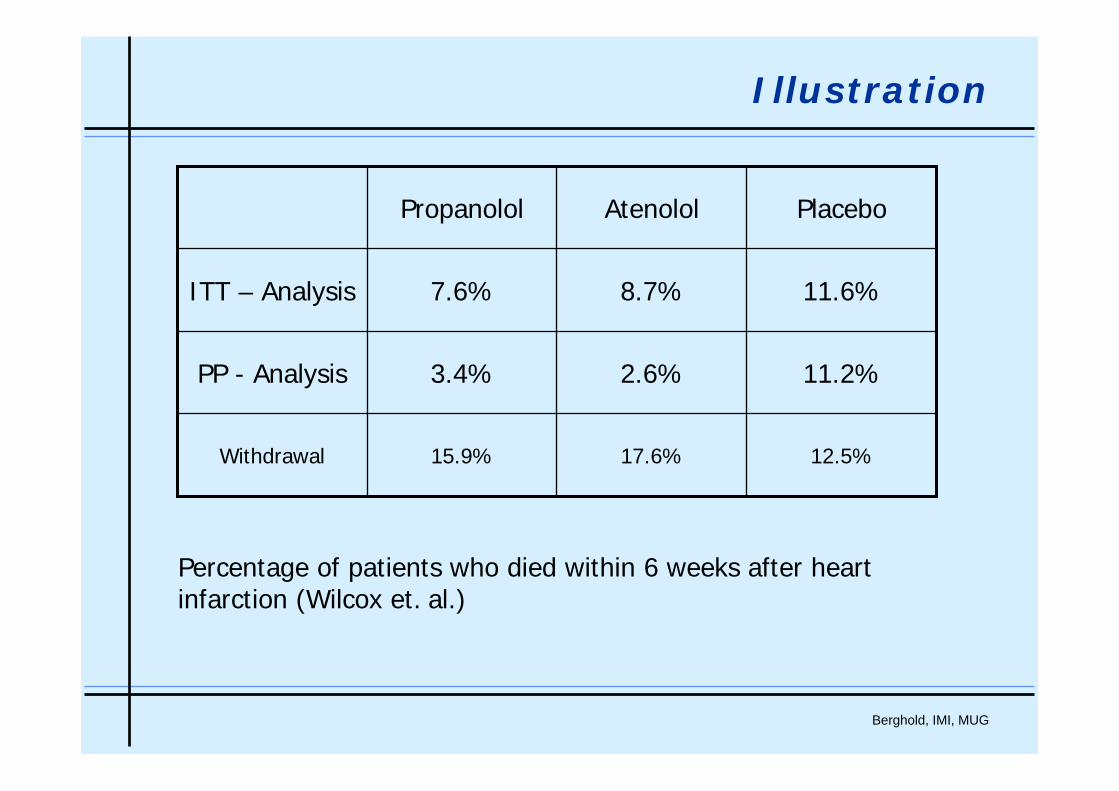
Illustration
11.6%8.7%7.6%ITT – Analysis
12.5%17.6%15.9%Withdrawal
11.2%2.6%3.4%PP - Analysis
PlaceboAtenololPropanolol
Percentage of patients who died within 6 weeks after heartinfarction (Wilcox et. al.)
Berghold, IMI, MUG
Efficacy and Effectiveness
Efficacyeffect under optimal conditions
All patients are included in the analysis, who were treated per protocol.
Per-Protocol Analysis
Effectivenesseffect under „real“ conditions.
All patients are included in the analysis, who were included in thestudy (Withdrawal, changing treatment etc.).
Intention-to-treat Analysis
Berghold, IMI, MUG
Main points RCTs
• Randomization – concealed allocation
• Blinding – double blind study
• Minimal loss in follow up
• Intention to treat Analyse
• Carry out specified analysis