Embed Size (px)
Citation preview
Unit 7
Hepatic & Pancreatic ConditionsGordons Functional Health Pattern
Activity and ExercisePart 1
OBJECTIVES: Identify the metabolic functions of the liver and the alterations in these functions that occur with
liver disease.
Explain liver function tests and the clinical manifestations of liver dysfunction in relation to pathophysiologic alterations of the liver.
Relate jaundice, portal hypertension, ascites, varices, nutritional deficiencies, and hepatic coma to pathophysiologic alterations of the liver.
Describe the medical, surgical, and nursing management of patients with esophageal varices.
Compare the various types of hepatitis and their causes, prevention, clinical manifestations, management, prognosis, and home health care needs.
Use the nursing process as a framework for care of the patient with cirrhosis of the liver.
Compare the nonsurgical and surgical management of patients with cancer of the liver.
Hepatic & Pancreatic Conditions• Review of A & P Liver
• Functions: – CHO metabolism-
• Glycogenesis = the formation of glycogen from glucose• Glycogenolysis = conversion of glycogen into glucose in
the liver & muscles• Storage of glycogen• Converts galactose & fructose to glucose• Converts ammonia into urea by deamination of AA
Hepatic & Pancreatic Conditions– Protein metabolism
• Synthesizes plasma proteins• Detoxifies & biotransforms hormones, drugs & other
chemicals• Vitamin (ADEK) & iron, copper storage
– Lipid metabolism• Oxidation of fatty acids to ketones for energy sources• Formation of most lipoprotein• Synthesis of cholesterol & phospholipids
– Bile formation
Hepatic & Pancreatic Conditions• Pancreas
• Functions:– Endocrine
• Secretes insulin• Secretes glucogon• Secretes somatostatin = a peptide that regulates the
release of hormones of different neuroendocrine cells found in brain, pancreas & GI tract; blocks the exocrine & endocrine functions of the pancreas; used to treat variceal hemorrhage in pts w cirrhosis & to treat pancreatitis.
– Octreotide is synthetic version
Hepatic & Pancreatic Conditions• Function
• Pancreas– Exocrine:
• Amylase - carbohydrate• Trypsin – protein• Lipase – fat
• Effects of aging: increase fibrosis, decrease secretions & enzyme effects glucose metabolism potential for diabetes mellitus nursing implications – periodic blood glucose test
Hepatic & Pancreatic Conditions• Assessment of client
– General appearance– Hx– Assess all systems: head to toe– Diagnostic tests:
• Liver Bx:• Paracentesis – the puncture of the peritoneal cavity for
removal of fluid– Nsg responsibility: consent, pre-procedure VS, amt of fluid
removed is recorded, specimens sent to lab; puncture site will ooze for several days – change dsg frequently, documentation of procedure & pt’s response; freq. post-procedure VS, may have to start IV, may have to give plasma expander

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Hepatic & Pancreatic Conditions
• Jaundice = “yellow” skin, results of excessive levels of bilirubin; total bilirubin > 3 mg/dl – visible
The following is a review of the normal pathway for bilirubin production and excretion and its relationship to laboratory assessment of liver function:
• Step 1: Red blood cells are broken down by the reticuloendothelial system and unconjugated bilirubin in the bloodstream is carried by albumin to the liver. This is known as "pre-hepatic," "free," "unconjugated," or" indirect bilirubin" (normal value = 0.1 - 1.0 mg/dl)
Hepatic & Pancreatic Conditions• Step 2: The liver converts or conjugates bilirubin
and makes it water-soluble - an enzyme, glucuronyl transferase, is necessary for the conjugation of bilirubin (either a lack of this enzyme, or the presence of drugs that interfere with glucuronyl transferase, impairs the liver's ability to conjugate bilirubin) - This is known as "posthepatic", "conjugated" or "direct" bilirubin (normal value = 0.0 - 0.4 mg/dl)
• Step 3: Conjugated bilirubin is excreted via bile salts to intestine. Bacteria in the intestine break down bilirubin to urobilinogen for excretion in the feces (normal value for fecal urobilinogen = 40 - 280 mg/day)
Hepatic & Pancreatic Conditions– Symptom of illness:
• Obstructive jaundice of biliary tracts [produces conjugated bilirubin due to bile regurgitation]
– gallstones, mass or tumor
• Alteration of bile metabolism at cellular level( hereditary ds)• Hepatocellular jaundice results from injury or ds of the parenchymal
cells of liver – Liver cell toxic injury ( acetaminophen overdoses)– Viral infections – Cirrhosis– Infectious mononucleosis– Reactions of certain drugs ( chlorpromazine)
• Hemolytic jaundice: due to overproduction of bilirubin resulting from hemolytic processes that produce levels of unconjugated bilirubin
– Pernicious anemia, sickle cell anemia, after blood transfusions. Transfusion reactions (abo or Rh incompatibility )
Hepatic & Pancreatic Conditions• Bilirubin – lab values
– Adult total: 0.2 – 1.3mg/dl• Panic value: > 12 mg/dl
– conjugated [direct]: water soluble 0.0 – 0.2 mg/dl• Elevated in conditions: cancer at head of pancreas,
choledocholithiasis
– unconjugated [indirect]: fat soluble• hemolytic anemias due to large hematoma• Trauma in presence of large hematoma
Hepatic & Pancreatic Conditions• Hepatitis – widespread inflammation of the liver
resulting in degeneration & necrosis of liver cells– 50,000 - 70,000 cases / yr in USA– Caused by viruses, toxins, chemicals (drugs)– Often asymptomatic– S&S: jaundice, pain upon palpation, subclinical –
anicteric (w/o jaundice), mild flu-like resp symptoms, mild temp, anorexia
• Hepatitis A G– They differ in incubation, mode of transmission &
severity
Viral Hepatitis• HAV --- Hepatitis A –aka infectious hepatitis;
– Occurrence: endemic in poor areas of world, poor sanitation; common in fall & winter
– Transmission: infected feces, fecal – oral route; may be airborne if copious secretions, Infected client contains the virus before symptoms appear infection spreads, day care centers, prisons
• Infected water, milk & food, raw shellfish from c water• No carrier state
– Caused by an RNA virus of the enterovirus family– Incubation period (2-7weeks) often 4 weeks– Severity: mortality low; rarely causes fulminating hepatic
failure.– Diagnostic tests: Antibodies (anti-HAV) appear early in
course of illness [IgM,- positive in acute hepatitis; IgG – positive after infection]
– Prophylaxis: hygiene; immune globuline [passive]; inactivated hepatitis A vaccine (active)
Viral Hepatitis• HBV --- Hepatitis B;
– Occurrence: worldwide, even in remote areas; incidence in dense populations and poor hygiene; drug addicts, homosexuals; HCW are at great risk, because of close contact w blood of carriers; occurs all year
– Is a DNA virus w inner core & a surface envelope• Body forms antibodies to viral antigens HBc Ag & HBsAg • HBsAg presence in blood: a past / resolving infection; a continuous
chronic; or immunization w immunoglobin or Hep B vaccine– Transmission: parenterally, sexually, in HIV infections,
found in saliva, accounts for 5-10% of post transfusion hepatitis
– Incubation: 2-5 months– Severity: more serious, mortality rate – 10 -20%– Diagnostic tests: HBsAg, HBc IgM– Prophylaxis: hygiene, avoidance of risk factors; HBIG
[Hepatitis B immune globulin] – passive; Recombinant hepatitis B vaccine (active) - (killed virus) x 3 doses,
Viral Hepatitis• Hepatitis C – HCV
– Route of transmission: blood, blood products, parenterally, IV drug users; possible fecal-oral route; can be spread by carriers; occurs all year
– Transmission: contact w blood & body fluids, carrier state
– Incubation period: 15 – 160 days– Severity: can lead to chronic hepatitis, cancer of
liver– Diagnostic tests: anti-HCV– Prophylaxis: hygiene; no vaccine for active
immunization; interferon (Intron-A) & ribavirin (Rebetol) helps improve clinical situation
Viral hepatitis• HEV -- Hepatitis E
– Occurrence: parts of Asia, Africa, & Mexico where there is poor sanitation.
– Transmission: fecal-oral route, food or water-borne, no carrier state, resembles Hep A
– Incubation: 14 – 60 days– Severity: illness self-limiting; jaundice is present,
mortality rate in pregnant women 10-20%– Diagnostic: Anti-HEV– Prophylaxis: hygiene, sanitation; no immunity
Viral hepatitis• HDV -- Hepatitis D - delta hepatitis
– occurrence: virus causes hepatitis only in association w hepatits B virus & only in presence of HBsAg; endemic in Mediterranean.
– Transmission: co-infects w hepatitis, close personal contact
– Incubation: 30 -180 day (same as Hep B)– Severity: similar to Hep B; more severe if occurs w
chronic active hep B, may develop cirrhosis– Diagnostic: HDAg- positive; RDA RNA in serum– Prophylaxis: hygiene, Hep B vaccine (active)
Viral Hepatitis• HGV -- Hepatits G
– Occurrence: associated w chronic viremia lasting 10 days
– Transmission: percutaneous, HCW in hemodialysis, IV drug users, hemodialysis clients, chronic B or C clients.
– Incubation period: --– Severity: does not appear to cause liver ds– Diagnostic: Anti-HGV– Prophylaxis: hygiene
Hepatitis Complications• Recovery usually 3-16 weeks
• Fulminant hepatitis acute liver necrosis, jaundice, hepatic encephalopathy, and ascites, labs: coagulation defects, elevated BUN & Cr– Mortality: 90-100% in > 60 yrs
• Tx: plasmapheresis, liver transplantation
Non viral hepatitis• Toxic / drug induced hepatitis
– Chemicals when inhaled, ingested or injected acute liver cell necrosis
• Carbon tetrachloride, phosphorus, chloroform & gold, benzene, Vit A (dose related)
• Medications: isoniazid, halothane, acetaminophen, some antibiotics, antimetabolites
– Liver necrosis occurs w/I 2-3 days after acute exposure to dose-related hepatoxin; minimal exposure over time chronic hepatitis or cirrhosis
– Nsg interventions: detailed drug hx, remove causative agent, rest, relieve SE –itching; diet: restrict protien if impending hepatic encephalopathy
Alcoholic hepatitis• May be acute or chronic
• Caused by parenchymal necrosis r/t heavy drinking; sometimes reversible cirrhosis,
• S&S occur after heavy drinking bouts: anorexia, nausea, abd pain, splenomegaly, hepatomegaly, jaundice, ascites, & encephalopathy– Labs: anemia, leukocytosis, & bilirubin
• Poor prognosis – if continues to drink
• Nsg interventions - vitamin, CHO diet, folic acid, thiamine & IV fluids
CirrhosisA. Types of Cirrhosis1. Biliary2. Postnecrotic3. Alcoholic (Laennec’s)Clinical Manisfestations:1.Early signs – weakness, fatigue, transient bouts of
jaundice, enlarged liver, RUQ tenderness, indigestions2. Later Signs – liver decreases in sizeLabs – increased SGOT,SGPT, serum bilirubin, PT, serum
globulin level. Decreased serum albumin, serum cholinesterase. Leukopenia and thrombocytopenia.
Acities, portal hypertension, and varices
CirrhosisManagement:Baloon temponade – sengstaken-Blakemore tubeEndoscopic sclerotherapyEsophageal Banding therapySurgery – direct ligation, portacavl shunt – decrease danger of
esophageal and gastric varices and decrease portal hypertensionNursing Care:• Rest• Improve nutritious status – high protein diet if no ascities or
edema. Low protein diet if in hepatic coma. Moderate protein diet – if no signs of hepatic encephalopathy. Maintain caloric intake
• Skin care for puritus and jaundice• Reduce risk of injury/bleeding• Medication – lactulose
Complications:Fluid retention, ascities, encephalopathy, esophageal varices
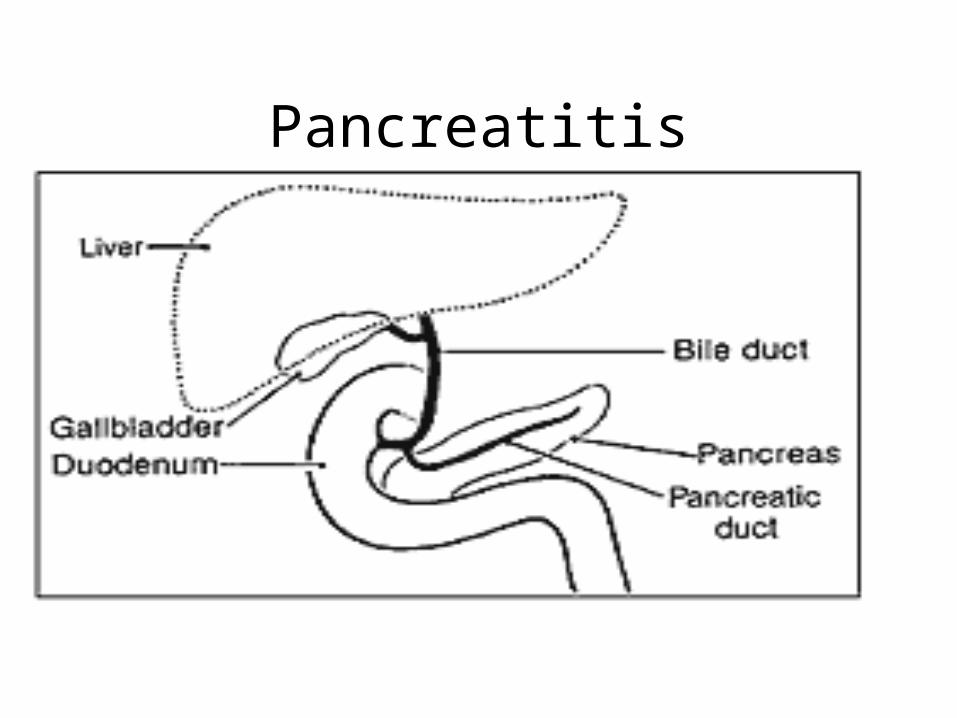
Pancreatitis• Pancreatitis begins when the digestive enzymes
become active inside the pancreas and start "digesting" it. The pancreas secretes digestive enzymes into the small intestine through a tube called the pancreatic duct. These enzymes help digest fats, proteins, and carbohydrates in food. The pancreas also releases the hormones insulin and glucagon into the bloodstream. These hormones help the body use the glucose it takes from food for energy.
Normally, digestive enzymes do not become active until they reach the small intestine, where they begin digesting food. But if these enzymes become active inside the pancreas, they start "digesting" the pancreas itself.
• Pancreatitis has two forms: acute and chronic
Pancreatitis
PancreatitisAcute pancreatitis occurs suddenly and lasts for a
short period of time and usually resolves. Chronic pancreatitis does not resolve itself and
results in a slow destruction of the pancreas. Either form can cause serious complications. In
severe cases, bleeding, tissue damage, and infection may occur. Pseudocysts, accumulations of fluid and tissue debris, may also develop. And enzymes and toxins may enter the bloodstream, injuring the heart, lungs, and kidneys, or other organs.
Common causes of pancreatitis are gallstones or alcohol abuse.
Sometimes no cause for pancreatitis can be found.
PancreatitisAcute Pancreatitis -Symptoms of acute pancreatitis include: Upper abd or mid epigastic pain that may radiate to the
back. Pain may last a few days and can become severe or get worse with eating, abdominal distention, N/V, fever, tachycardia, in a severe case - respiratory distress, hypotension, renal failure, shock.
DX: 3x more amylase and lipase (digestive enzymes formed in the pancrease), change in blood glucose levels, Ca, Mg, Na, K, and HCO3.US abd (look for gallstones, CT (look for inflammation or destruction of the pancrease, or pseudocyts)
Treatment for acute pancreatitis include:Depending on severity, TPN, intravenous fluids, NPO, oxygen, pain meds, antibiotics, or surgery.
Acute pancreatitis becomes chronic when pancreatic tissue is destroyed and scarring develops.
PancreatitisChronic PancreatitisChronic pancreatitis occurs when digestive
enzymes attack and destroy the pancreas and nearby tissues, causing scarring and pain.
The usual cause of chronic pancreatitis is many years of alcohol abuse, but the chronic form may also be triggered by only one acute attack, especially if the pancreatic ducts are damaged.
The damaged ducts cause the pancreas to become inflamed, tissue to be destroyed, and scar tissue to develop.
PancreatitisChronic PancreatitisWhile common, alcoholism is not the only cause of chronic
pancreatitis. The main causes of chronic pancreatitis are• alcoholism • blocked or narrowed pancreatic duct because of trauma
or pseudocysts have formed • heredity • unknown cause (idiopathic) • Damage from alcohol abuse may not appear for many
years, and then a person may have a sudden attack of pancreatitis. In up to 70 percent of adult patients, chronic pancreatitis appears to be caused by alcoholism. This form is more common in men than in women and often develops between the ages of 30 and 40.
PancreatitisChronic Pancreatitis• Hereditary pancreatitis usually begins in childhood but
may not be diagnosed for several years. A person with hereditary pancreatitis usually has the typical symptoms that come and go over time.
• Episodes last from 2 days to 2 weeks. • A determining factor in the diagnosis of hereditary
pancreatitis is two or more family members with pancreatitis in more than one generation.
• Treatment for individual attacks is usually the same as it is for acute pancreatitis.
• Any pain or nutrition problems are treated just as they are for acute pancreatitis. Surgery can often ease pain and help manage complications.
PancreatitisChronic Pancreatitis• Other causes of chronic pancreatitis are• congenital conditions such as pancreas
divisum • cystic fibrosis • high levels of calcium in the blood
(hypercalcemia) • high levels of blood fats (hyperlipidemia or
hypertriglyceridemia) • some drugs • certain autoimmune conditions
Chronic Pancreatitis - Symptoms• Most people with chronic pancreatitis have abdominal
pain, although some people have no pain at all. • The pain may get worse when eating or drinking, spread to
the back, or become constant and disabling.• In certain cases, abdominal pain goes away as the
condition advances, probably because the pancreas is no longer making digestive enzymes.
• Other symptoms include nausea, vomiting, weight loss, and fatty stools.
• People with chronic disease often lose weight, even when their appetite and eating habits are normal.
• The weight loss occurs because the body does not secrete enough pancreatic enzymes to break down food, so nutrients are not absorbed normally. Poor digestion leads to excretion of fat, protein, and sugar into the stool.
• If the insulin-producing cells of the pancreas (islet cells) have been damaged, diabetes may also develop at this stage.
PancreatitisChronic Pancreatitis
Diagnosis• Diagnosis may be difficult, but new techniques
can help. Pancreatic function tests help decide whether the pancreas is still making enough digestive enzymes.
• Ultrasonic imaging, endoscopic retrograde cholangiopancreatography (ERCP), and CAT scans, helps DX chronic pancreatitis (can show calcification of the pancreas, in which tissue hardens from deposits of insoluble calcium salts).
PancreatitisChronic PancreatitisTreatment• Relieving pain is the first step in treating chronic pancreatitis.
The next step is to plan a diet that is high in carbohydrates and low in fat.
• Patient may require pancreatic enzymes to take with meals if the pancreas does not secrete enough of its own. The enzymes should be taken with every meal to help the body digest food and regain some weight.
• Sometimes insulin is needed to control blood glucose.• In some cases, surgery is needed to relieve pain. The surgery
may involve draining an enlarged pancreatic duct or removing part of the pancreas.
• For fewer and milder attacks, people with pancreatitis must stop drinking alcohol, stick to their prescribed diet, and take the proper medications.
Treatment for chronic pancreatitis includes easing the pain; eating a high-carbohydrate, low-fat diet; and taking enzyme supplements. Surgery is sometimes needed as well