Embed Size (px)
Citation preview
Unit 6: Diagnosing TBUnit 6: Diagnosing TB
Botswana National Tuberculosis Programme Manual Training for Medical Officers
Slide 6-2Unit 6: Diagnosing TB
ObjectivesObjectives
At the end of this unit, participants will be able to:
• Diagnose pulmonary tuberculosis disease using sputum smears
• Diagnose smear negative pulmonary TB disease
• Diagnose extra-pulmonary TB disease
Slide 6-3Unit 6: Diagnosing TB
Diagnosis of TuberculosisDiagnosis of Tuberculosis
• Priority is in diagnosing and curing infectious cases
• ALL persons with TB symptoms should also be tested for HIV• Routine HIV testing in Botswana• Rapid HIV testing available in all public health
facilities
Slide 6-4Unit 6: Diagnosing TB
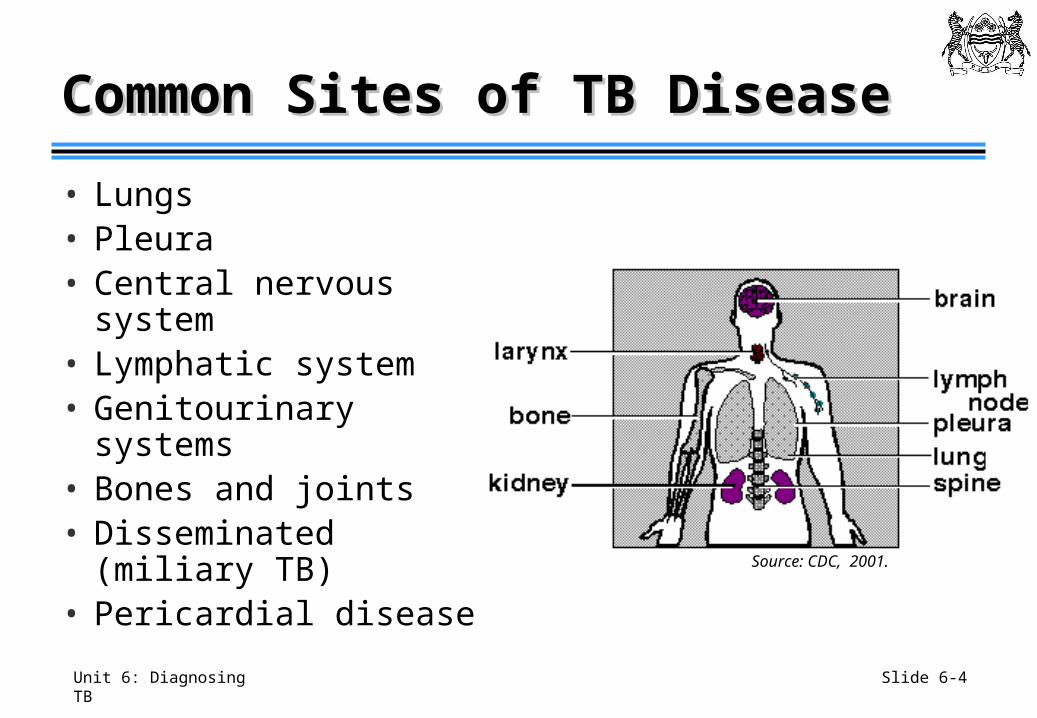
Common Sites of TB DiseaseCommon Sites of TB Disease
• Lungs• Pleura• Central nervous system• Lymphatic system• Genitourinary systems• Bones and joints• Disseminated (miliary
TB)• Pericardial disease Source: CDC, 2001.
Slide 6-5Unit 6: Diagnosing TB
The Effect of HIV Infection on The Effect of HIV Infection on Symptoms and Signs of TBSymptoms and Signs of TB
• TB is more common in HIV infected persons, systemic symptoms are very common
• HIV-related immunosuppression doesn’t always allow the body to contain TB disease to a single organ system
• Must be looking for signs and symptoms of both pulmonary and extrapulmonary TB
Slide 6-6Unit 6: Diagnosing TB
Case Finding (1)Case Finding (1)
• Highest priority to find and cure infectious cases: people with smear-positive PTB
• Two ways of identifying TB cases:• Passive case finding: illness diagnosed
when patient presents for medical care at health facility
• Active case finding: health workers actively search for patients with TB in the community
Slide 6-7Unit 6: Diagnosing TB
Who is a TB Suspect?Who is a TB Suspect?
“Any person who presents with symptoms or signs suggestive of TB, in particular cough of long duration (more than 2 weeks).”
Source: WHO, 2003
Slide 6-8Unit 6: Diagnosing TB
Case Finding (2)Case Finding (2)
Most common tools for case finding include:
• History taking
• Physical examination
• Sputum examination
• X-ray examination
• Tuberculin skin testing
Slide 6-9Unit 6: Diagnosing TB
Active Case FindingActive Case Finding
• Contact investigation most common method in Botswana
• Other methods include special surveys based on:
• Geography
• Targeted testing of defined populations
(e.g., schools, prisons)
Slide 6-10Unit 6: Diagnosing TB
Clinical PresentationClinical Presentation
• Take a thorough history for each patient• Determine if signs and symptoms point to
pulmonary or extrapulmonary TB
• Also obtain medical and social history
• Do a general physical examination with additional care to detect signs of tuberculosis
Slide 6-11Unit 6: Diagnosing TB
Medical HistoryMedical History
• Have you had close contact with someone with TB?• Do you have a cough? How long, dry, productive, colour?• Is blood present in your sputum?• Do you have chest pain? When & where?• Do you have shortness of breath? How long?• Do you sweat profusely at night?• Have you lost weight?• When did you start losing weight?• When did you lose your appetite?• How long have you been feeling weak and tired?• Do you smoke?• Have you previously been tested for TB?• Do you know your HIV status?
Source: Chiang C-V et al., 2007.
Slide 6-12Unit 6: Diagnosing TB
Common Symptoms of Common Symptoms of Adult Pulmonary TB (1)Adult Pulmonary TB (1)
• Cough (prolonged) for two to three weeks• Any person with this symptom is classified as TB suspect
• Sputum
• Fever/ night sweats
• Weight loss, wasting in advanced cases
• Shortness of breath • Malaise
Slide 6-13Unit 6: Diagnosing TB
Common Symptoms of Common Symptoms of Adult Pulmonary TB (2)Adult Pulmonary TB (2)
• Haemoptysis
• Chest pain
• Tachypnoea (abnormally fast breathing)
• Anaemia
• Abnormal breath sounds
• Loss of appetite
Slide 6-14Unit 6: Diagnosing TB
Pulmonary TB DiagnosisPulmonary TB Diagnosis
How do you currently diagnose pulmonary tuberculosis disease?
Slide 6-15Unit 6: Diagnosing TB
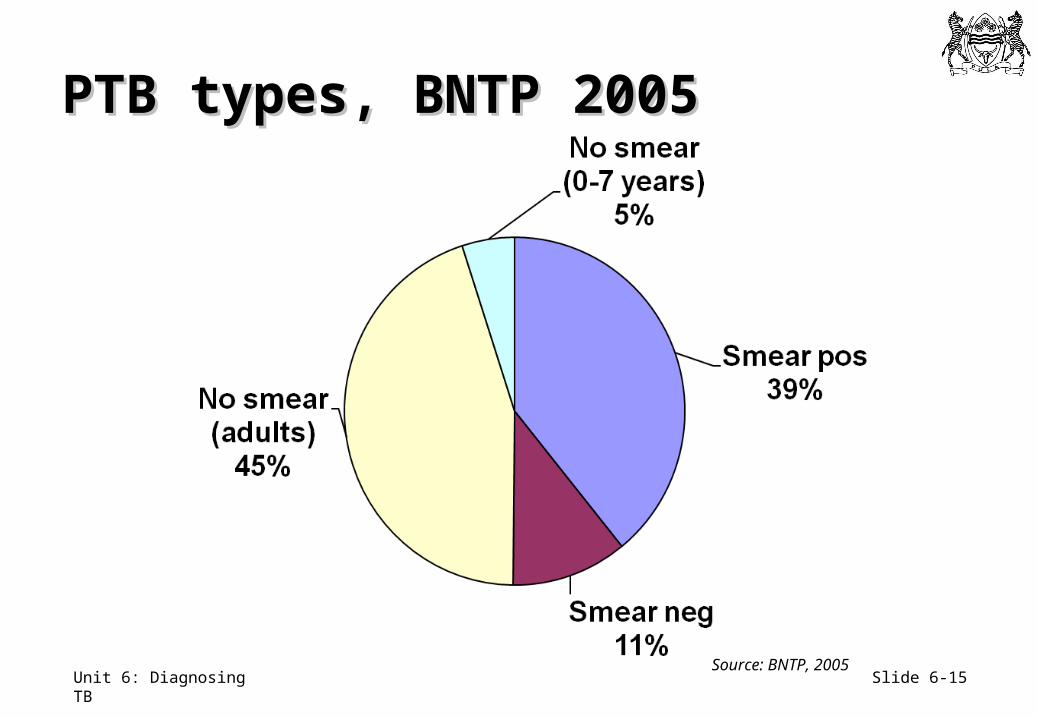
PTB types, BNTP 2005PTB types, BNTP 2005
Source: BNTP, 2005
Slide 6-16Unit 6: Diagnosing TB
Sputum SmearsSputum Smears
• Smear microscopy is widely available and accessible for diagnosis in Botswana
• When pulmonary TB is suspected, three sputum specimens must be collected for examination
• Outpatient: “spot-early morning-spot”
• Inpatient: three early morning specimens over three consecutive days
Slide 6-17Unit 6: Diagnosing TB
Sputum Collection Techniques (1)Sputum Collection Techniques (1)
• Sputum collection should be done outside or in an empty room with very good ventilation
• If above not possible, try for best possible ventilation
• Use sterile glass or plastic containers, 5-6 cm deep, with screw cap
Slide 6-18Unit 6: Diagnosing TB
Sputum Collection Techniques (2)Sputum Collection Techniques (2)
• The health worker should explain and demonstrate procedure
• The health worker should supervise, but should NOT stand in front of the patient• Collect away from other people
• Only sputum (2-5 ml) should be accepted as a good specimen
• Saliva (white, watery, frothy) should not be accepted because it will yield useless and misleading results
Slide 6-19Unit 6: Diagnosing TB
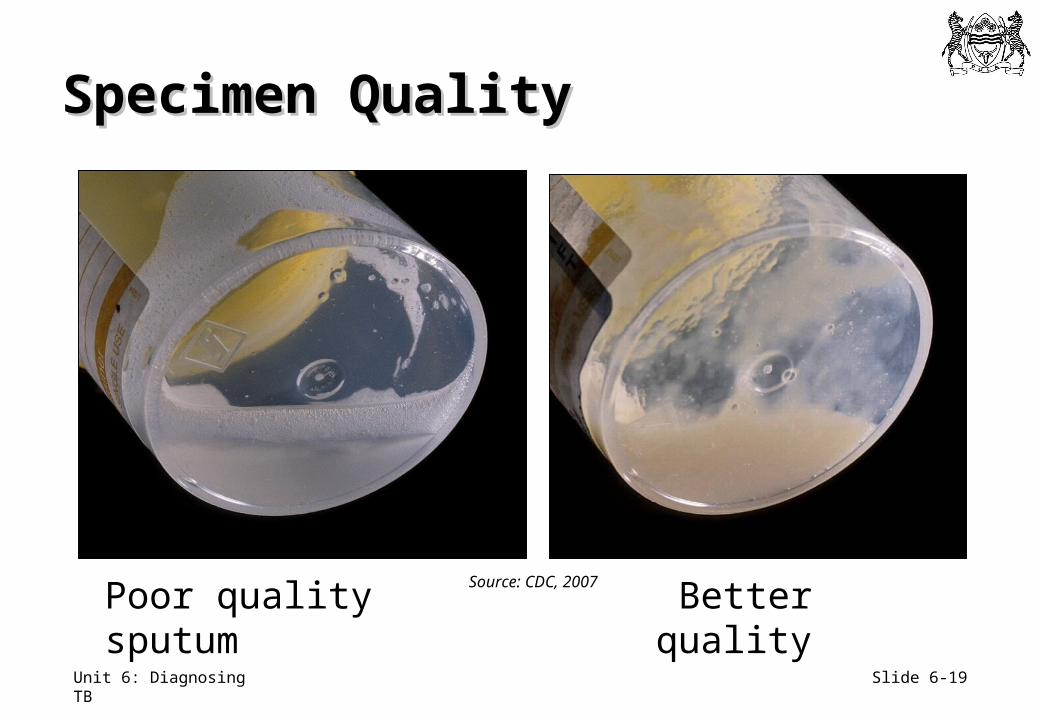
Specimen QualitySpecimen Quality
Poor quality sputum Better quality Source: CDC, 2007
Slide 6-20Unit 6: Diagnosing TB
Patient Instructions: Patient Instructions: Sputum Collection (1)Sputum Collection (1)
Explain clearly to patient:• Why sputum is needed
• Three samples required
• Spot–morning-spot
• What a “good” sample is and how to obtain it
• Opening and tight closing of containers
• Not to soil the exterior of the container
• Not to expose the sample to sunlight
• Transport of sputum containers
• The need to return to the clinic
Slide 6-21Unit 6: Diagnosing TB
Patient Instructions: Patient Instructions: Sputum Collection (2)Sputum Collection (2)
• Rinse mouth and throat with water two to three times, and drink some water to wet throat (for easy spitting of viscid sputum)
• Inhale deeply 2-3 times, breathe out hard each time• Keep the body inclined to front• Cough deeply from the chest• Open the container and keep it near mouth and spit
sputum in• Close lid securely• Wash hands after handling sputum container• Bring container to HCW
Slide 6-22Unit 6: Diagnosing TB
Sputum Smear ExaminationSputum Smear Examination
• Specimens should be sent to lab as soon as possible
• Complete Mycobacteriology Request and Report Form
• Always aim for three specimens from each suspect
• Spot-early morning-spot specimen collection will detect 90% of smear-positive cases
Slide 6-23Unit 6: Diagnosing TB
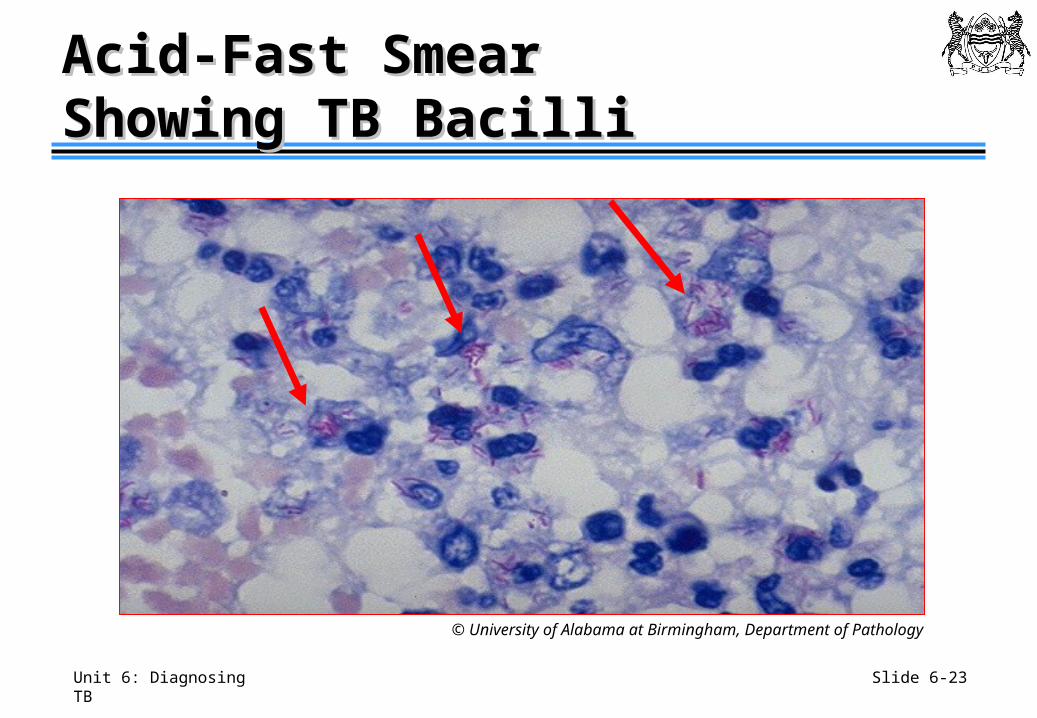
Acid-Fast Smear Acid-Fast Smear Showing TB BacilliShowing TB Bacilli
© University of Alabama at Birmingham, Department of Pathology
Slide 6-24Unit 6: Diagnosing TB
Mycobacteriology Mycobacteriology Request and Report FormRequest and Report Form• Must be completed by HCW for each specimen
submitted to lab, and must accompany it to the lab• Smear microscopy
• TB culture
• Drug sensitivity testing
• Completed suspect register
• Lab will:• Process specimen
• Complete “REPORT” section on form’s lower half
• Return to requesting HCW or treatment unit
Slide 6-25Unit 6: Diagnosing TB
Sputum ResultsSputum Results
• Once Mycobacteriology Request and Report form is received back in the clinic, the receiving HCW should record the results in:• TB Treatment card
• The Suspect and Sputum Dispatch Register • Facility TB Register as appropriate
Slide 6-26Unit 6: Diagnosing TB
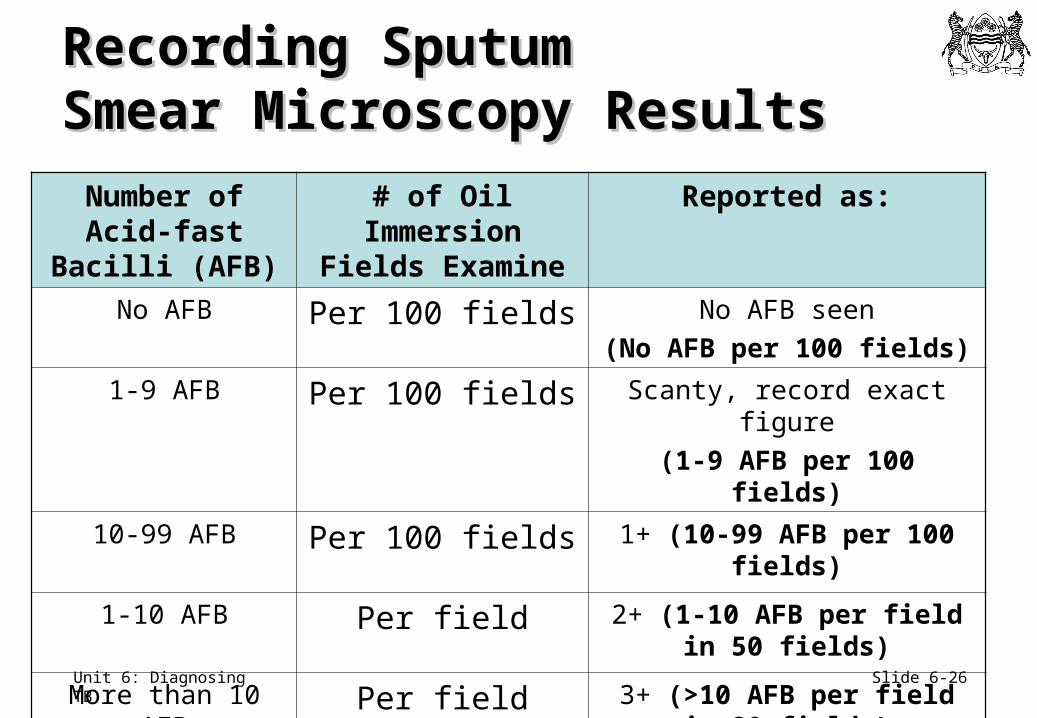
Recording Sputum Recording Sputum Smear Microscopy ResultsSmear Microscopy Results
Number of Acid-fast Bacilli (AFB)
# of Oil Immersion Fields Examine
Reported as:
No AFB Per 100 fields No AFB seen
(No AFB per 100 fields)
1-9 AFB Per 100 fields Scanty, record exact figure
(1-9 AFB per 100 fields)
10-99 AFB Per 100 fields 1+ (10-99 AFB per 100 fields)
1-10 AFB Per field 2+ (1-10 AFB per field in 50 fields)
More than 10 AFB Per field 3+ (>10 AFB per field in 20 fields)
Slide 6-27Unit 6: Diagnosing TB
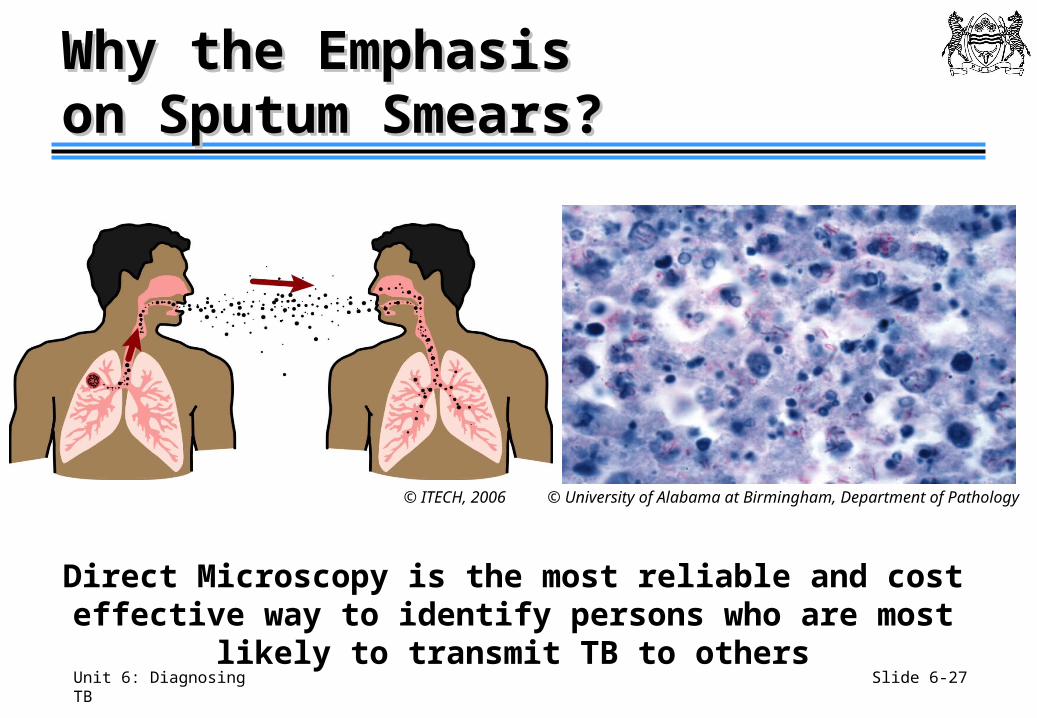
Why the Emphasis Why the Emphasis on Sputum Smears?on Sputum Smears?
Direct Microscopy is the most reliable and cost effective way to identify persons who are most likely to transmit TB to others
© ITECH, 2006 © University of Alabama at Birmingham, Department of Pathology
Slide 6-28Unit 6: Diagnosing TB
What does a Positive What does a Positive Sputum Smear Mean?Sputum Smear Mean?
• Positive smear predicts higher contagiousness to others
• Smears may be positive and not mean TB• Due to laboratory error or MOTT
• Sensitivity and specificity of a positive smear depends on prevalence of MOTT and HIV in a population
Slide 6-29Unit 6: Diagnosing TB
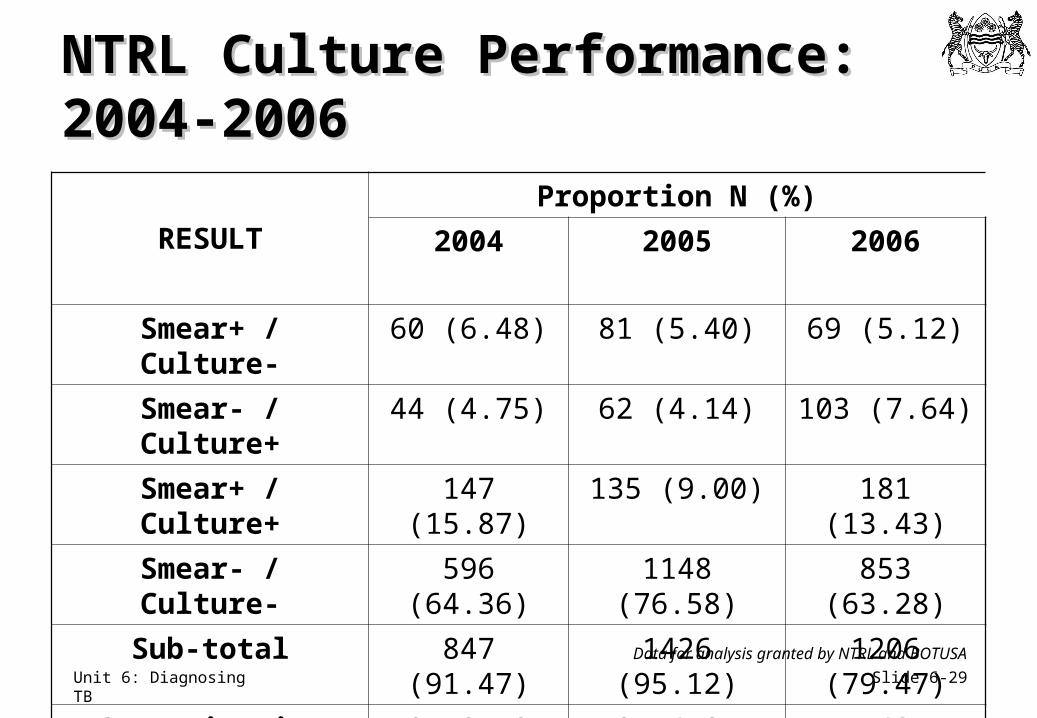
NTRL Culture Performance: NTRL Culture Performance: 2004-20062004-2006
RESULT
Proportion N (%)
2004 2005 2006
Smear+ / Culture- 60 (6.48) 81 (5.40) 69 (5.12)
Smear- / Culture+ 44 (4.75) 62 (4.14) 103 (7.64)
Smear+ / Culture+ 147 (15.87) 135 (9.00) 181 (13.43)
Smear- / Culture- 596 (64.36) 1148 (76.58) 853 (63.28)
Sub-total 847 (91.47) 1426 (95.12) 1206 (79.47)
Contamination 79 (8.53) 73 (4.87) 142 (10.53)
Total 926 1499 1348
Data for analysis granted by NTRL and BOTUSA
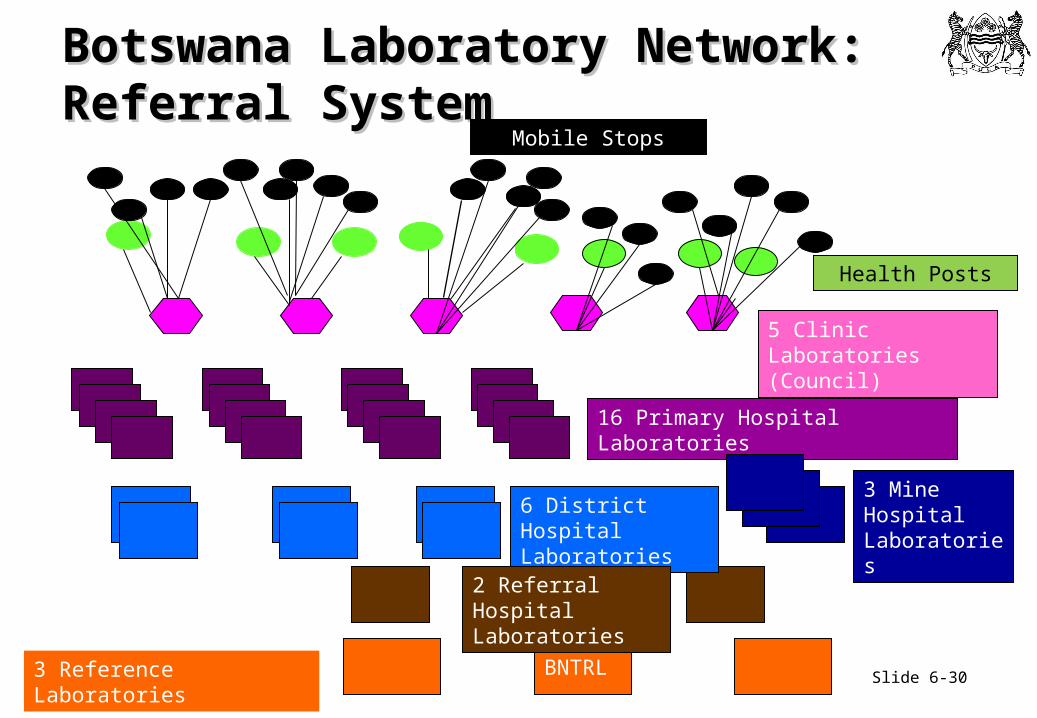
Slide 6-30Unit 6: Diagnosing TB3 Reference Laboratories BNTRL
Botswana Laboratory Network: Botswana Laboratory Network: Referral SystemReferral System
Mobile Stops
Health Posts
5 Clinic Laboratories (Council)
16 Primary Hospital Laboratories
6 District Hospital Laboratories
3 Mine Hospital Laboratories
2 Referral Hospital Laboratories
Slide 6-31Unit 6: Diagnosing TB
• Receipt of specimens: from clinics • Preparation and staining of smears• ZN microscopy /recording• Reporting of results• Maintenance of lab register• Management of reagents and supplies• Internal Quality Control (QC)• Collect specimen for culture and DST, send to NTRL • Participation in EQA
Primary and District LabPrimary and District LabServices in TB control (Level 1)Services in TB control (Level 1)
Slide 6-32Unit 6: Diagnosing TB
Nyangagbwe Referral lab (Level 2) Nyangagbwe Referral lab (Level 2) • Activities: receive specimen for AFB and
culture
• Services to clinics: FM/ZN smear microscopy (smear microscopy and send results)
• Support activities: (supply of reagents/ materials, training; EQA for smear microscopy including supervision)
• Inoculate specimen and refer to NTRL for incubation and DST
Slide 6-33Unit 6: Diagnosing TB
Role of Role of NTRL NTRL in TB Controlin TB Control
• Identify mycobacterium other than MTB • DST of M. Tuberculosis• TB laboratory equipment services and maintenance• Develop TB Lab manuals and guidelines• Primary link with NTP• Supervision of intermediate QA of culture and
microscopy• Operational and applied research• Provide EQA and monitor peripheral labs
Slide 6-34Unit 6: Diagnosing TB
Diagnosing Smear-Negative PTB Diagnosing Smear-Negative PTB
• Some seriously ill patients may have sputum AFB smear results and may die of TB if untreated
• High index of suspicion if there are:• Miliary changes on chest x-ray (CXR)• Compatible CXR and no response to Rx for bacterial
infection • Pleural effusion• Inthrathoracic adenopathy• Pericardial effusion
Source: Lockman S et al., 2003.
Slide 6-35Unit 6: Diagnosing TB
Algorithms for Diagnosis of PTB Algorithms for Diagnosis of PTB
• Algorithm for diagnosis of PTB in ambulatory patients
• Algorithm for diagnosis of PTB in seriously ill patients
Slide 6-36Unit 6: Diagnosing TB
Mycobacterial Culture (1)Mycobacterial Culture (1)
• “Gold Standard” of TB diagnosis• More expensive and more time
consuming than microscopy• Requires specialised training and
media to perform• Not recommended for routine
case detection in Botswana
Courtesy of: Kubica G, 2007.
Slide 6-37Unit 6: Diagnosing TB
Mycobacterial Culture (2)Mycobacterial Culture (2)
Reasons to request mycobacterial culture:• Patient previously on anti-TB treatment• Still smear-positive after intensive phase of treatment
or after finishing treatment• Symptomatic and at high-risk of MDR-TB• To test fluids potentially infected with M. tuberculosis• Investigation of patients who develop active PTB
during or after IPT• TB in health workers
Slide 6-38Unit 6: Diagnosing TB
• DST performed on all cultures• Tests for isoniazid, rifampicin, ethambutol, and
streptomycin
• If found to be multi-drug resistant, then send for additional testing for susceptibility to second-line medicines
TB Drug Susceptibility Testing (DST)TB Drug Susceptibility Testing (DST)
Slide 6-39Unit 6: Diagnosing TB
Role of RadiographyRole of Radiography
• Chest X-Ray (CXR) can support a diagnosis of PTB• Not used routinely for follow-up• PTB can exist with normal CXR• Must be interpreted with other information
• History and exam• Sputum smear results
• Also useful in diagnosing other types of TB, especially in bones, joints, and spine
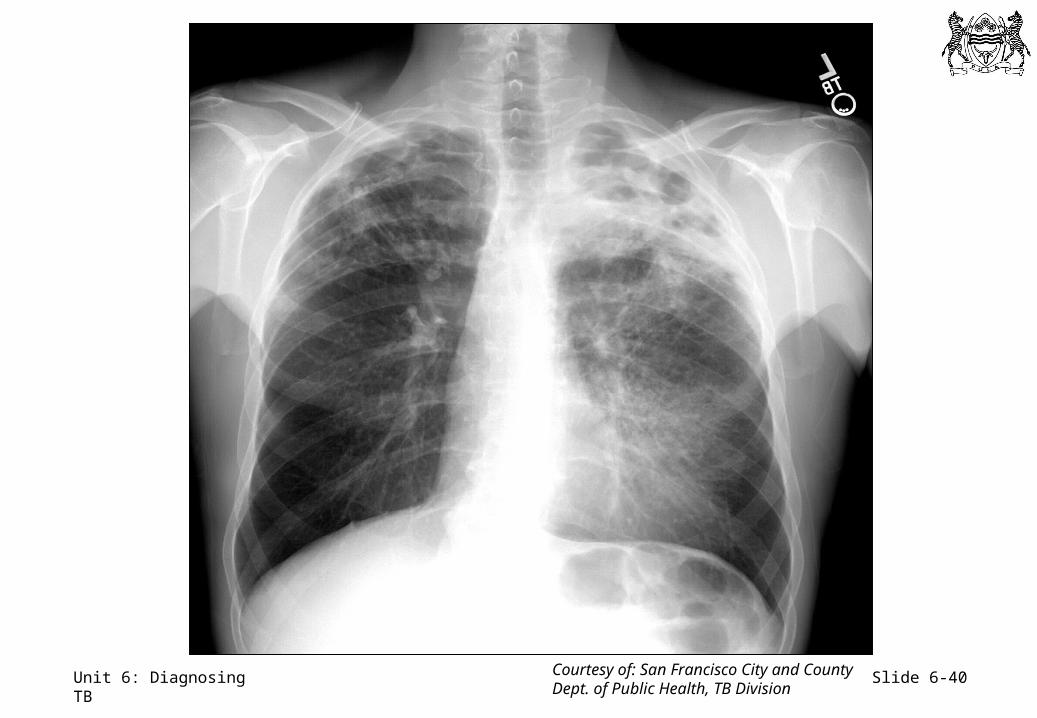
Slide 6-40Unit 6: Diagnosing TB Courtesy of: San Francisco City and County Dept. of Public Health, TB Division
Slide 6-41Unit 6: Diagnosing TB
Pulmonary TB DiagnosisPulmonary TB Diagnosis
Are there any special challenges in diagnosing pulmonary TB among
persons with HIV?
Slide 6-42Unit 6: Diagnosing TB
Sputum Smear and HIV StatusSputum Smear and HIV Status
• HIV positive patients with pulmonary TB often have negative sputum smears
• Important to recognise the clinical and chest radiographic characteristics of HIV-TB, so patients who are smear-negative can be recognised and treated appropriately
Slide 6-43Unit 6: Diagnosing TB
Early HIV disease• Cavity or upper lobe pulmonary disease• Positive sputum smear microscopy• Pleural disease
Advanced HIV disease • Sputum smear negative pulmonary disease• Disseminated TB• Pleural or pericardial effusion with or without intrathoracic
adenopathy• Lower and middle lobe infiltrates
Effect of HIV Stage on Effect of HIV Stage on Manifestations of TBManifestations of TB
Slide 6-44Unit 6: Diagnosing TB
• Severe immunodeficiency can have a dramatic effect on the CXR manifestations of TB• Not classic TB picture on CXR • Reticulonodular infiltrates (disseminated TB)
seen, but often without the classic miliary pattern• Intrathoracic adenopathy (mediastinal or hilar
adenopathy) relatively common among patients with advanced HIV-TB
• It is critical to understand this relationship so that patients with HIV-TB will be recognized and treated
Source: Post FA et al. Tuber Lung Dis. 1995.
Effect of Immunosuppression Effect of Immunosuppression on CXR in HIV-Related TBon CXR in HIV-Related TB
Slide 6-45Unit 6: Diagnosing TB
Chest X-Ray Chest X-Ray Patterns and CD4 CountsPatterns and CD4 Counts
Radiographic features associated with the degree of HIV-related immunosuppression in patients with HIV-related pulmonary TB:• Intrathoracic adenopathy associated with low
CD4 count• Cavitation and infiltrates more common in
patients with CD4 > 200 and those with less- advanced HIV
Source: Perlman DC, et al. Clin Infect Dis, 1997.
Slide 6-46Unit 6: Diagnosing TB
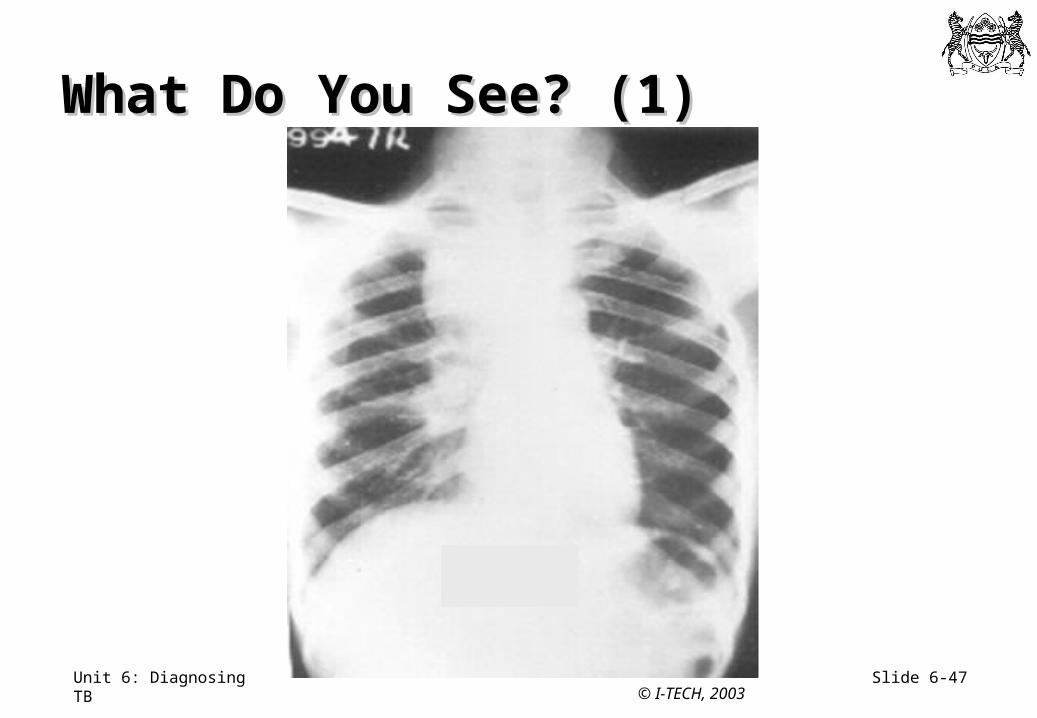
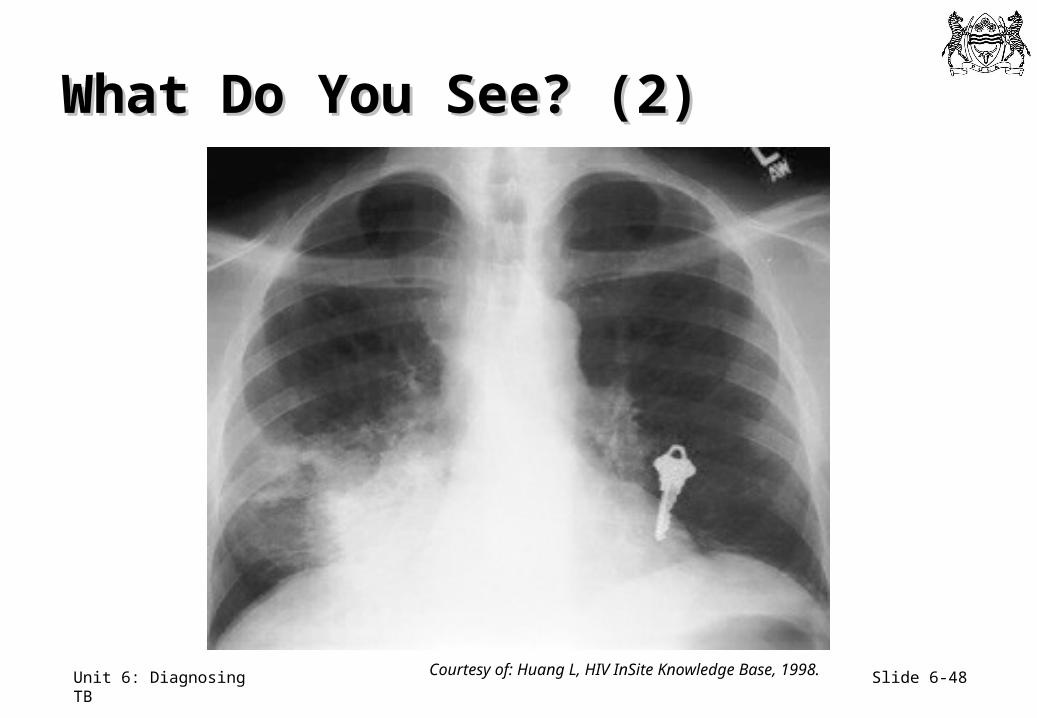
Example of Example of Immunosuppressed TB SuspectImmunosuppressed TB Suspect
• 23 year old male, HIV infected, recent CD4 count was 35
• He has cough, loss of appetite and weight loss for 3 weeks
• His sputum smear for AFB was negative, therefore a CXR was done
Slide 6-47Unit 6: Diagnosing TB
What Do You See? (1)What Do You See? (1)
© I-TECH, 2003
Slide 6-48Unit 6: Diagnosing TB
What Do You See? (2)What Do You See? (2)
Courtesy of: Huang L, HIV InSite Knowledge Base, 1998.
Slide 6-49Unit 6: Diagnosing TB
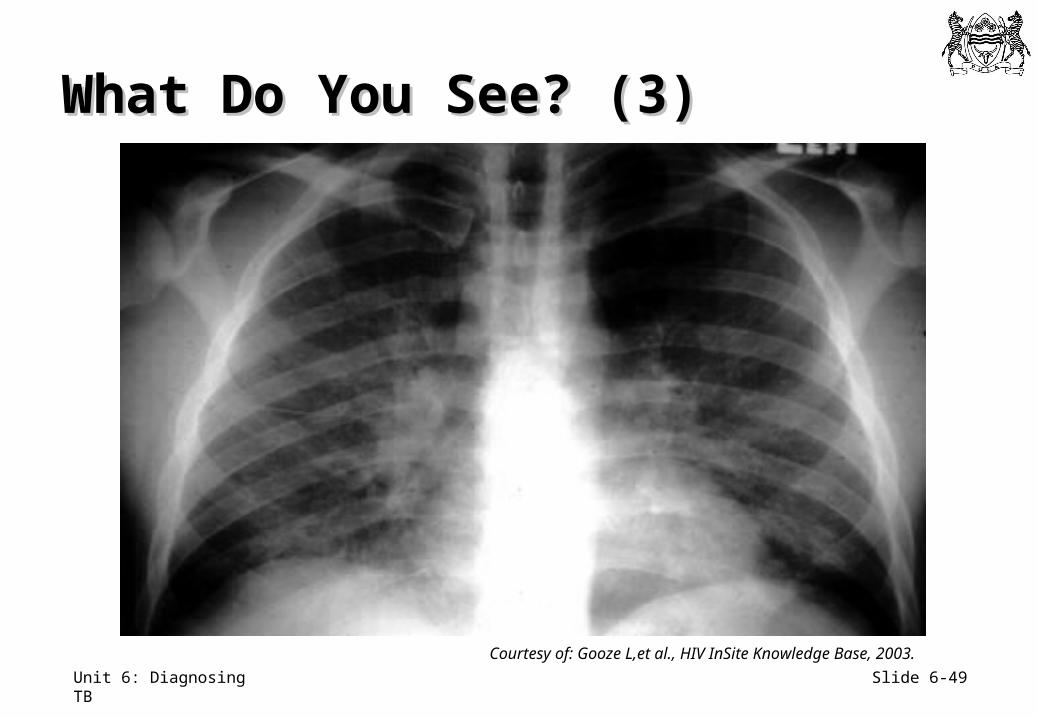
What Do You See? (3)What Do You See? (3)
Courtesy of: Gooze L,et al., HIV InSite Knowledge Base, 2003.
Slide 6-50Unit 6: Diagnosing TB
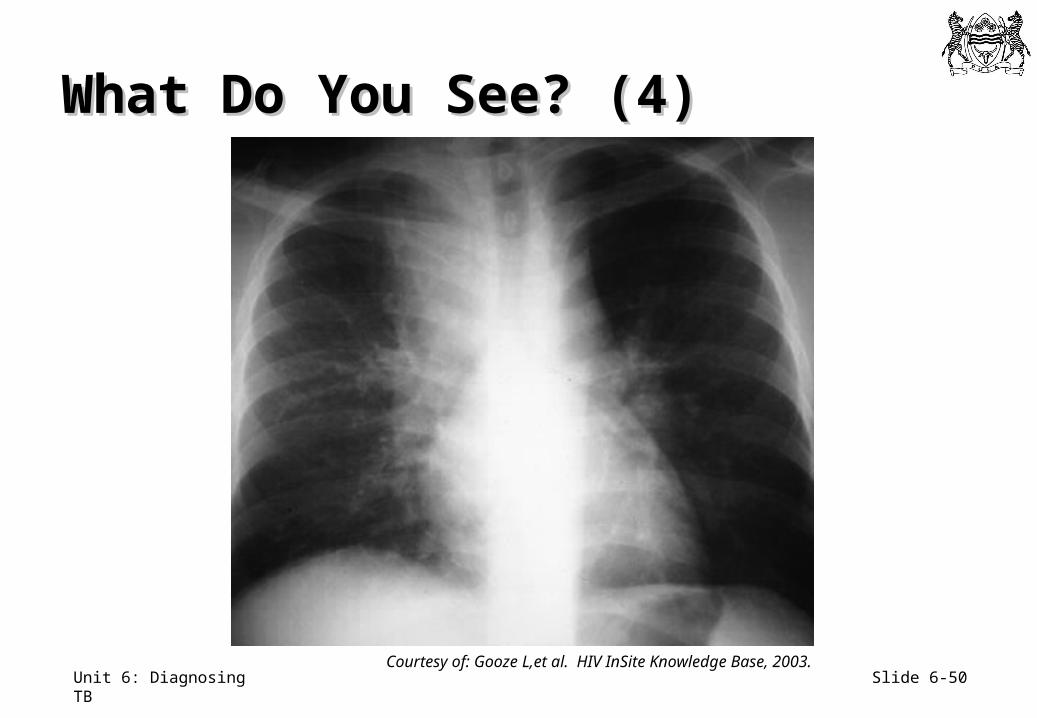
What Do You See? (4)What Do You See? (4)
Courtesy of: Gooze L,et al. HIV InSite Knowledge Base, 2003.
Slide 6-51Unit 6: Diagnosing TB
Differential Diagnoses Differential Diagnoses for TB Suspects (1)for TB Suspects (1)
• Bacterial pneumonia• Lung abscess or bronchiectasis• Asthma or chronic obstructive airways disease• Occupational lung disease, i.e., silicosis• Lung cancer other than Kaposi’s Sarcoma• Congestive cardiac failure
Slide 6-52Unit 6: Diagnosing TB
Differential Diagnoses for Differential Diagnoses for TB Suspects (2)TB Suspects (2)
• Empyema• Pneumocystis carinii (Jirovecii) pneumonia • Chronic fungal pneumonia• CMV pneumonia• Kaposi’s Sarcoma• Lymphoma• Mycobacteria Other Than Tuberculosis (MOTT)• Lymphocytic interstitial pneumonitis (LIP) in children
Slide 6-53Unit 6: Diagnosing TB
Classic Sites of Classic Sites of Extrapulmonary TBExtrapulmonary TB
• Pleura • Lymph nodes• Disseminated or miliary• Meninges• Pericardium• Abdominal (peritoneal)• Intestinal
• Spine• Other bones• Liver• Kidney• Adrenal glands• Genitourinary tract• Upper airway• Skin
Source: Caminero Luna JA, 2003.
Slide 6-54Unit 6: Diagnosing TB
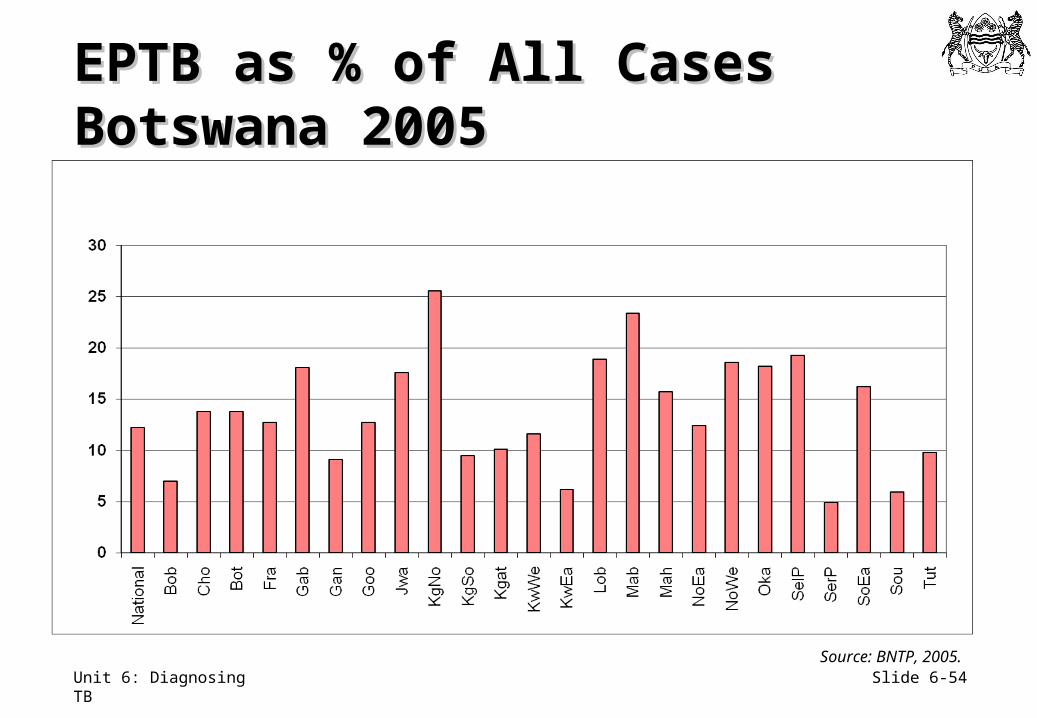
EPTB as % of All CasesEPTB as % of All CasesBotswana 2005Botswana 2005
Source: BNTP, 2005.
Slide 6-55Unit 6: Diagnosing TB
• Nodal • Peripheral nodes - cervical > axillary > inguinal• Central nodes - mediastinal > hilar, intra-abdominal
• Disseminated disease• Serosal - pleural, pericardial > ascites
• Central nervous system - meningitis, tuberculoma
• Soft tissue abscesses
Common Forms of EPTB Common Forms of EPTB Among HIV-Infected PersonsAmong HIV-Infected Persons
Slide 6-56Unit 6: Diagnosing TB
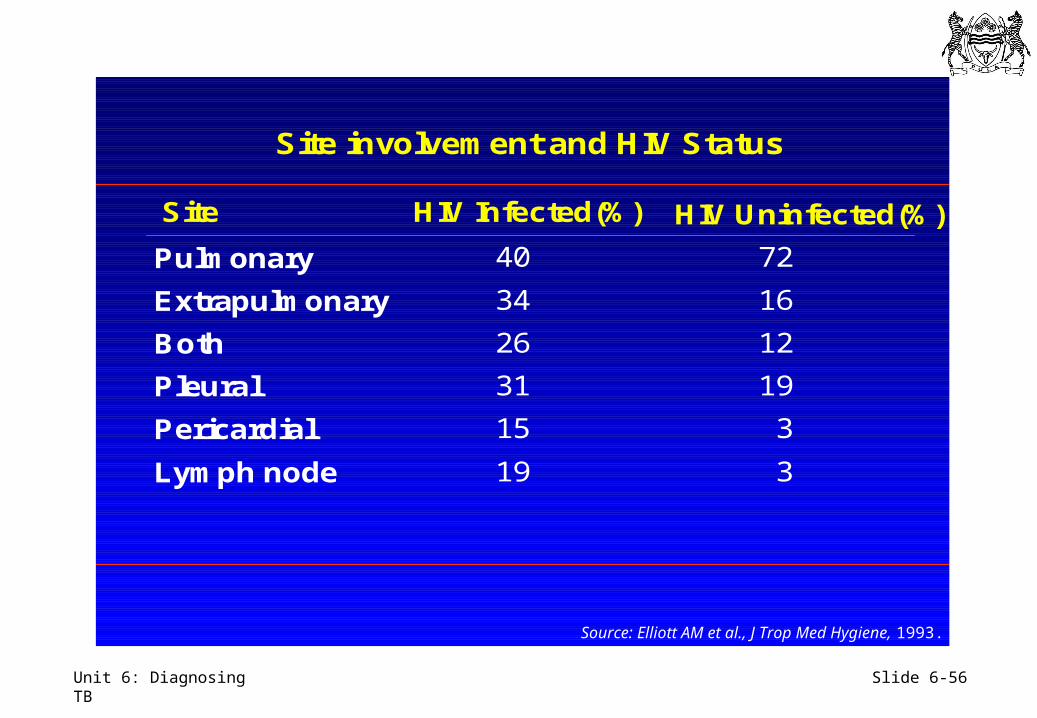
Site involvement and HIV Status
Site HIV Infected(%) HIV Uninfected(%)
Pulmonary
Extrapulmonary
Both
Pleural
Pericardial
Lymph node
40
34
26
31
15
19
72
16
12
19
3
3
Source: Elliott AM et al., J Trop Med Hygiene, 1993.
Slide 6-57Unit 6: Diagnosing TB
Tuberculosis in Tuberculosis in HIV-Positive Persons (1)HIV-Positive Persons (1)
Persons with clinically significant immunosuppression from HIV can have• Primary progressive pulmonary and
extrapulmonary TB• Reactivation pulmonary and extrapulmonary TB• A high risk of disseminated (miliary) and
meningeal TB like young (immunologically immature) children
Slide 6-58Unit 6: Diagnosing TB
Tuberculosis in Tuberculosis in HIV-Positive Persons (2)HIV-Positive Persons (2)
• HIV-positive persons have higher rates of extrapulmonary tuberculosis than HIV-negative persons
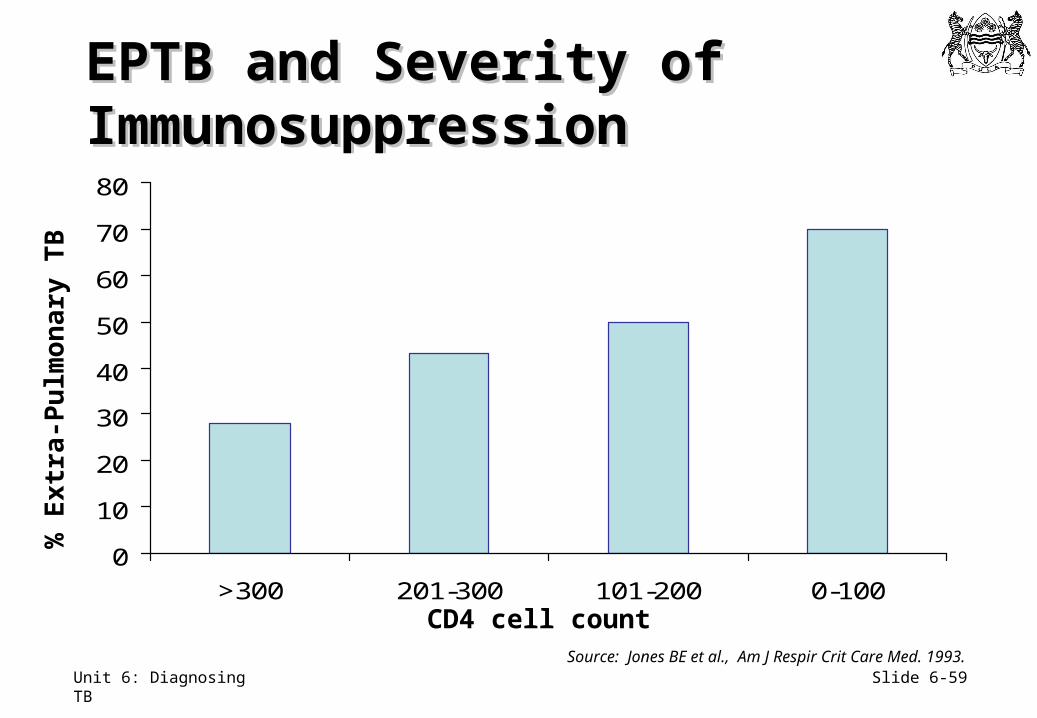
• The lower the CD4 count, the more likely an HIV-positive person is to develop extrapulmonary TB
• TB becomes a systemic multi-organ disease, rather than primarily a pulmonary disease, with progressive immunodeficiency
Slide 6-59Unit 6: Diagnosing TB
EPTB and Severity of EPTB and Severity of ImmunosuppressionImmunosuppression
0
10
20
30
40
50
60
70
80
>300 201-300 101-200 0-100CD4 cell count
% E
xtr
a-P
ulm
on
ary
TB
Source: Jones BE et al., Am J Respir Crit Care Med. 1993.
Slide 6-60Unit 6: Diagnosing TB
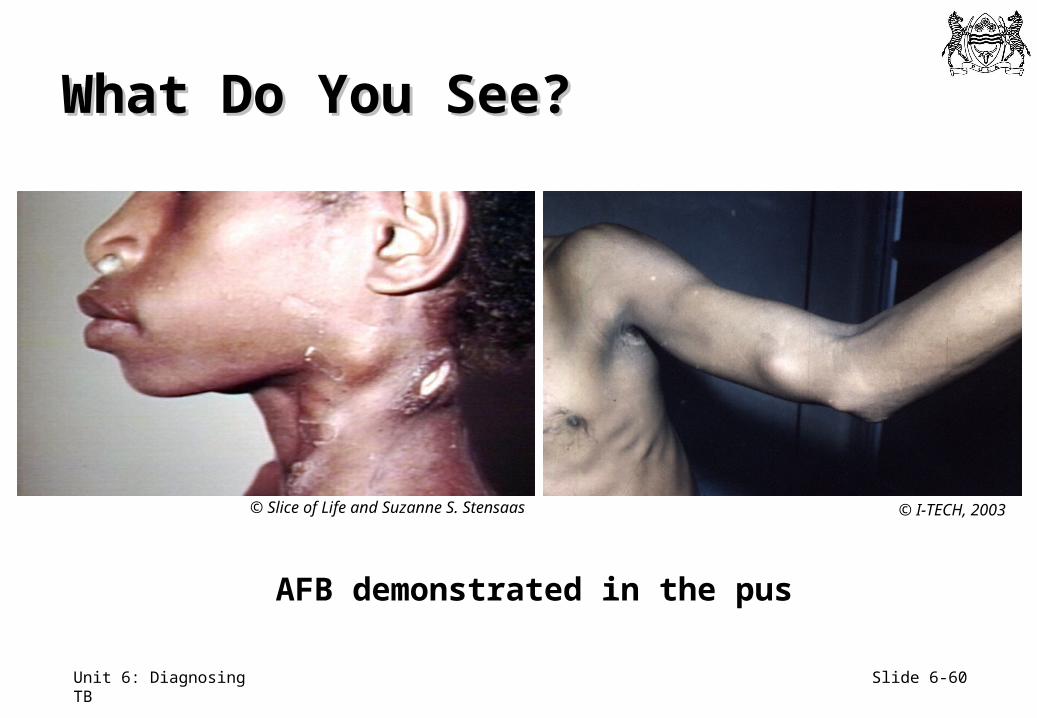
AFB demonstrated in the pus
What Do You See?What Do You See?
© I-TECH, 2003© Slice of Life and Suzanne S. Stensaas
Slide 6-61Unit 6: Diagnosing TB
Diagnosing TB LymphadenitisDiagnosing TB Lymphadenitis
Needle aspiration is a good test for TB adenitis in HIV-infected persons
• Can be done the same day in the health facility
• Has a low rate of adverse effects
• Has a high yield for diagnosing TB
Slide 6-62Unit 6: Diagnosing TB
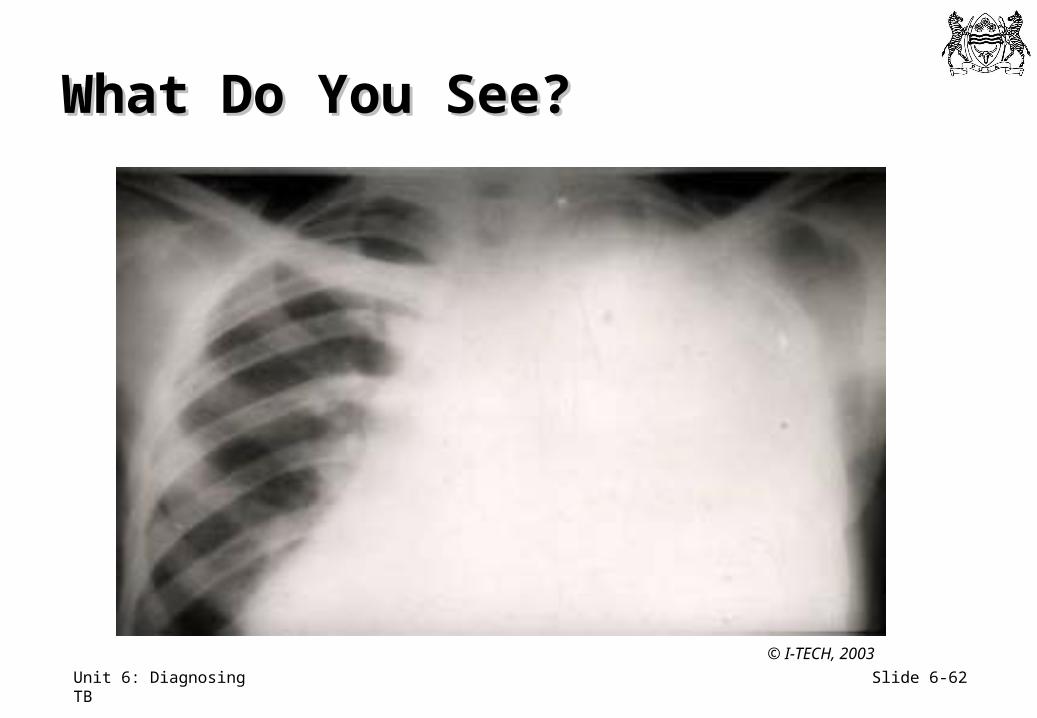
What Do You See?What Do You See?
© I-TECH, 2003
Slide 6-63Unit 6: Diagnosing TB
Diagnosing Pleural TBDiagnosing Pleural TB
• 97-99% of all pleural effusions in high HIV prevalence areas caused by TB
• A diagnostic pleural aspiration and CXR are done to confirm pleural effusion• The pleural fluid is normally an exudate
• Pleural biopsy, although invasive, also gives high diagnostic yield
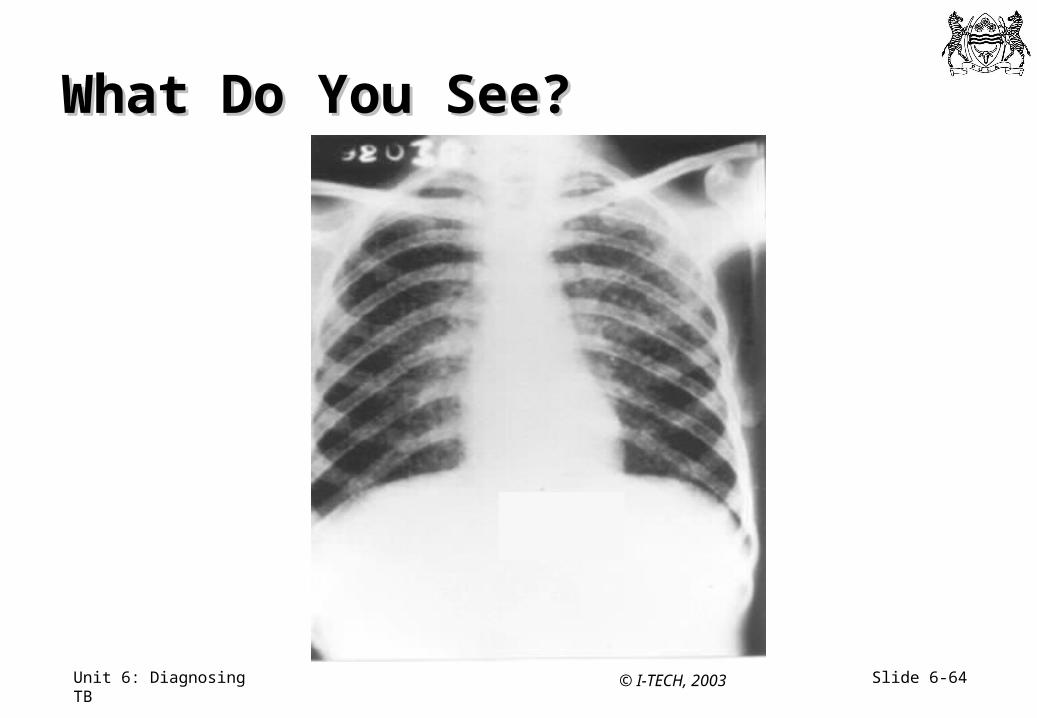
Slide 6-64Unit 6: Diagnosing TB
What Do You See?What Do You See?
© I-TECH, 2003
Slide 6-65Unit 6: Diagnosing TB
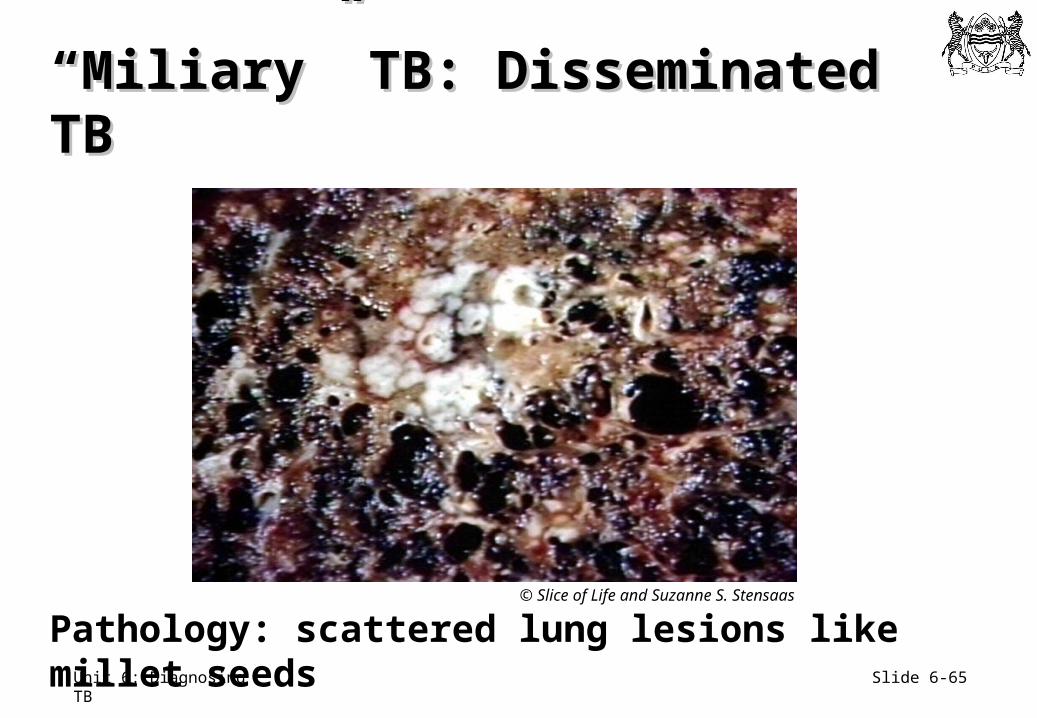
Pathology: scattered lung lesions like millet seeds
““Miliary” TB: Disseminated TBMiliary” TB: Disseminated TB
© Slice of Life and Suzanne S. Stensaas
Slide 6-66Unit 6: Diagnosing TB
TB Meningitis (1)TB Meningitis (1)
• Subacute or chronic• Headache, fever, neck stiffness, decreasing mental
status• Lumbar puncture essential for diagnosis• CSF usually shows raised white cell count
(predominantly lymphocytes) with elevated protein, reduced glucose, and negative AFBs.
• Most important differential diagnosis in Botswana is cryptococcal meningitis
Slide 6-67Unit 6: Diagnosing TB
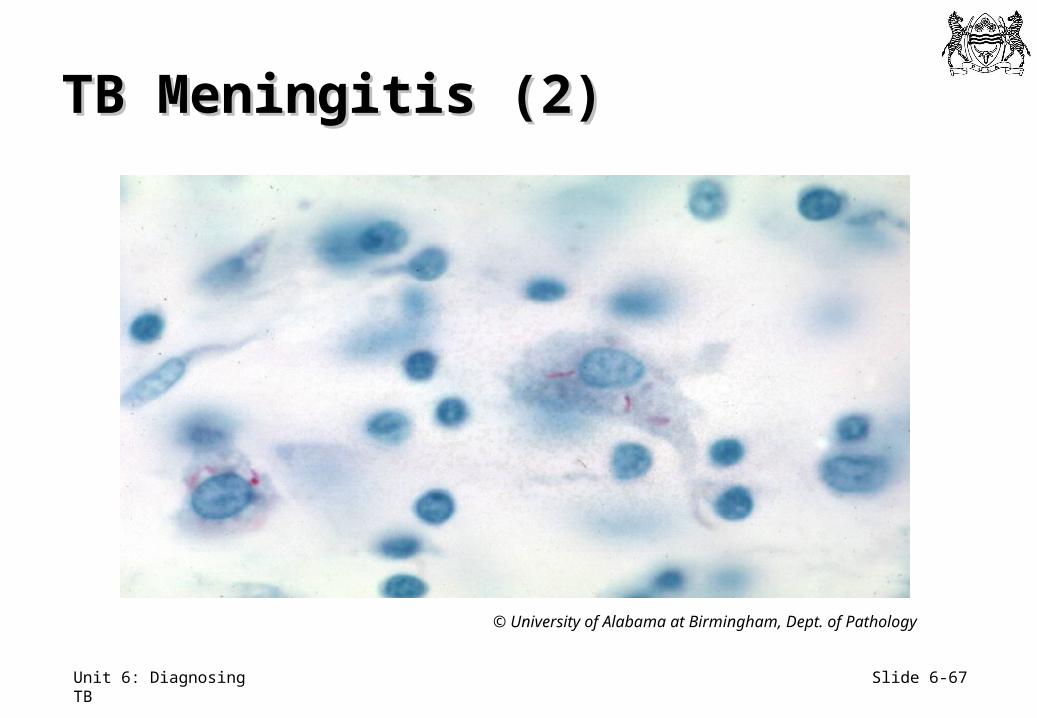
TB Meningitis (2)TB Meningitis (2)
© University of Alabama at Birmingham, Dept. of Pathology
Slide 6-68Unit 6: Diagnosing TB
Spinal TB Spinal TB
• Thoracic, lumbar, and sacral vertebrae are primarily affected by TB infection
• Most spinal TB occurs in the lower thoracic and lumbar spine • Always request x-rays of thoracic and lumbar
spine when vertebral TB is suspected
• Hip and knee are most common joints infected by TB
Slide 6-69Unit 6: Diagnosing TB
What Do You See?What Do You See?
© Slice of Life and Suzanne S. Stensaas
Slide 6-70Unit 6: Diagnosing TB
What Do You See?What Do You See?
© Slice of Life and Suzanne S. Stensaas
Slide 6-71Unit 6: Diagnosing TB
Renal TBRenal TB
• Typically see dilated calyces
• Urine smears can be falsely + due to acid fast staining of environmental bacteria
• Diagnosis confirmed with mycobacterial urine culture• Three early morning urine specimens
Slide 6-72Unit 6: Diagnosing TB
Case DefinitionCase Definition
• Standardised way to identify type of TB case in both adults and children
• Determined by:• Site of TB disease• Results of bacteriology tests (sputum smear)• History of previous TB treatment• Severity of TB disease
Slide 6-73Unit 6: Diagnosing TB
Activity 6.1: Matching (1)Activity 6.1: Matching (1)
Using Worksheet 6.1, match the terms at the top of the page with the definitions below
Slide 6-74Unit 6: Diagnosing TB
Now, apply one of the following determinants to each term:
I. Site of Disease
II. Results of Bacteriology Tests
III. History of Previous TB Treatment
IV. Severity of Previous TB Treatment
Activity 6.1: Matching (2)Activity 6.1: Matching (2)
Slide 6-75Unit 6: Diagnosing TB
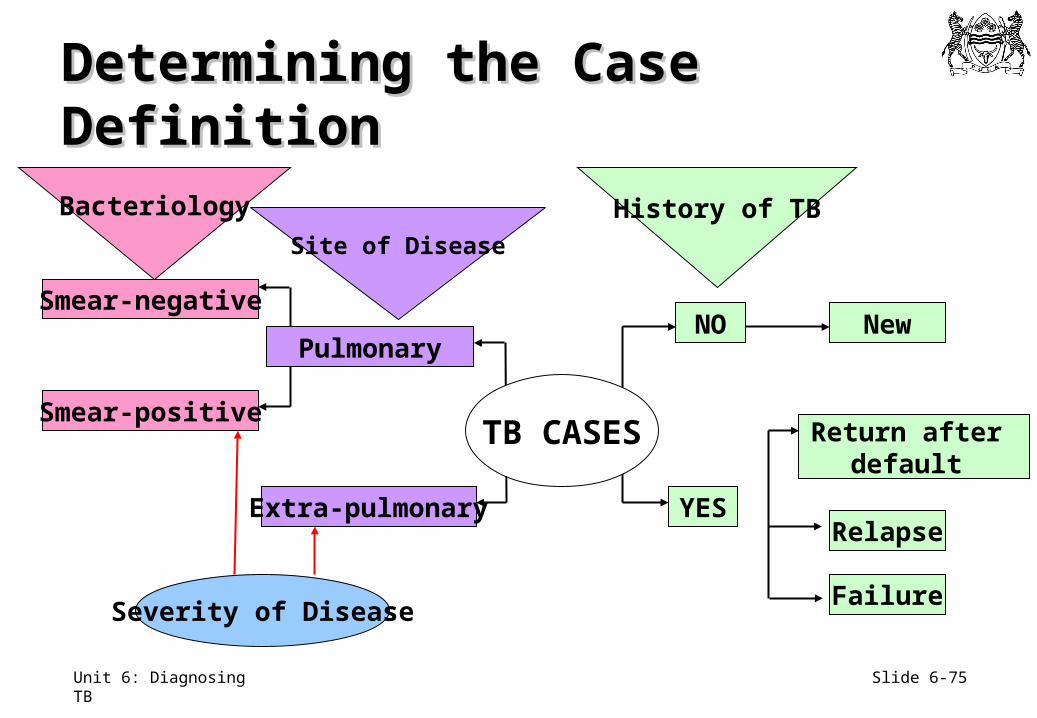
Determining the Case DefinitionDetermining the Case Definition
TB CASES
Severity of Disease
Extra-pulmonary
Smear-negative
Pulmonary
Smear-positive
NO
YES
New
Return after default
Relapse
Failure
Bacteriology
Site of Disease
History of TB
Slide 6-76Unit 6: Diagnosing TB
Site of TB DiseaseSite of TB Disease
• May be pulmonary (PTB), extrapulmonary (EPTB) or both
• Pulmonary: involving lung parenchyma
• Extrapulmonary: involving any organ beside the lung parenchyma
• Patient with BOTH PTB and EPTB is classified as having pulmonary TB
Slide 6-77Unit 6: Diagnosing TB
Results of Bacteriology Tests (1)Results of Bacteriology Tests (1)
• In PTB—determine presence of acid-fast bacilli (AFB) in sputum• Sputum smear is positive or negative dependent
on presence of AFB• “Smear-positive”: at least one smear with AFB• “Smear-negative”: any PTB case which does not
meet smear-positive criteria
Slide 6-78Unit 6: Diagnosing TB
Results of Bacteriology Tests (2)Results of Bacteriology Tests (2)
EPTB cases include:• Patients with one positive culture or positive AFB
smear from extrapulmonary site• Patients with extrapulmonary histology, lab/clinical
evidence, and doctor’s decision to start TB treatment
Slide 6-79Unit 6: Diagnosing TB
Categories of Categories of TB Treatment HistoryTB Treatment History
New Never had treatment for TB, or has taken anti-tuberculosis drugs for less than one month
Retreatment after Relapse
Previously treated for TB and declared cured, or treatment completed, and is diagnosed with bacteriologically positive (smear or culture) TB
Retreatment after Failure
Is started on a re-treatment regimen after having failed previous treatment
Retreatment after Default
Returns to treatment, positive bacteriologically, following interruption of treatment for two months or more
Source: WHO, 2003.
Slide 6-80Unit 6: Diagnosing TB
Severity of TB DiseaseSeverity of TB Disease
• Based on quantity of bacteria and disease site
• More severe:• Meningeal, spinal, pericardial, pulmonary cavitary
and miliary
• Less severe:• Lymph nodes, bones (except spine), and skin
Slide 6-81Unit 6: Diagnosing TB
Key Points (1)Key Points (1)
• Confirmed diagnosis of PTB depends on positive sputum smears• Order culture only in specific circumstances
• Smear negative PTB diagnosed on supportive clinical and CXR evidence
• Persons with low immunity likely to have atypical PTB, primary progressive TB, and extrapulmonary TB
Slide 6-82Unit 6: Diagnosing TB
Key Points (2)Key Points (2)
• Extrapulmonary TB usually diagnosed on supportive clinical and X-ray evidence• Biopsy is helpful• Culture provides proof (but still will only be positive
in about 50% of EPTB cases overall)