Embed Size (px)
Citation preview
Unit 4 Person-centered approaches to end of life care
About this unit
This unit will inform learners of the person-centred approach to end of life care and how it ensures that the individual’s physical, emotional, social and cultural needs are met.
Learning outcome 1
The learner will:
Understand the effects of symptoms in relation to end of life care. The
learner can:
1.1 Identify a range of health conditions for which end of life care may be provided
1.2 Identify symptoms that may be related to the individual’s condition and/or treatment
1.3 Outline the underlying causes of a range of symptoms
1.4 Describe how symptoms can cause the individual pain and discomfort
1.5 Outline how different factors can alleviate or exacerbate symptoms
1.1 The health conditions for which end of life care may be provided
There is a commonly held belief that end of life care is only for those with cancer. However, even though the palliative care approach developed within cancer care, anyone with an illness or condition that limits life and for which there is no chance of recovery should be offered palliative care.
The following degenerative conditions may benefit from palliative care approach:
Advanced heart, respiratory and kidney disease (all of which may or not be related to the ageing process)
Dementia
Aids
Multiple sclerosis and other neurological conditions such as Parkinson’s disease and motor neuron disease.
This list is not exhaustive.
A person who is old and frail and may be nearing the end of their life can also benefit from the provision of palliative care.
Palliative care recognises that although the person has a life limiting or life threatening illness they still have a life to live.
2
Consider the example of the late Jane Tomlinson who, although she was diagnosed with ‘terminal’ cancer several years ago, raised millions of pounds for charity by undertaking enormous physical challenges, such as running marathons.
Therefore, it is vital that a positive proactive approach to death and dying is adopted so that a good death can be experienced by the individual.
1.2 Symptoms that may be related to the individual’s condition and/or
treatment
The nature of a dying person’s illness can understandably cause people to focus on pain relief, and even though in palliative care pain is a major consideration, other distressing symptoms must not be overlooked. Some examples of these symptoms include:
Anorexia
Weakness and fatigue
Thirst
Fever
Jaundice
Nausea and vomiting
Constipation
Insomnia
Hiccups - are very distressing and if persistent can exhaust a person and affect all their activities and hamper communication
Skin irritations – A person in the end stages of a life limiting illness will be more at risk of skin problems which may range from itching, rashes, dry or broken skin or pressure sores
Incontinence
Delirium
Shortness of breath
Oedema (swelling) and ascites (fluid in the abdomen)
The common cancer treatments within cancer care and their side effects

3
Chemotherapy - Side effects
Hair loss
Dry sensitive skin
Nails may grow very slowly and develop irregular pigmentation
Sore mouth and mouth ulcers
Nausea, vomiting and diarrhoea – can be a very distressing and debilitating side effect and may last from hours to a few days
Anaemia and low white cell count
Infertility – sperm production and ovulation may be affected which can be permanent
Radiotherapy
Radiation in the form of X-rays are used to destroy cancerous cells, concentrating on the affected area of the body. It can be used to cure, or in palliative care to relieve symptoms.
Side effects
Reddening of the skin – rarely people can have mild radiation burns
Hair loss
Diarrhoea, nausea, vomiting and anorexia
Fatigue
Infertility
Cystitis
Swallowing difficulties due to sore mouth and throat.
These are usually temporary and ease once treatment is complete.
4
1.3 The underlying causes of a range of symptoms The
causes of pain
People who are dying face a number of possible causes of pain such as:
Primary disease – diseases such as cancer where tumours press on surrounding structures and nerves
Treatment – the treatment of disease may cause pain – e.g. radiotherapy, surgery, therapies (e.g. physiotherapy)
Debilitating nature of their disease – effects such as immobility, poor diet and fluid intake can lead to constipation and breakdown of pressure areas
Other factors – age, lifestyle and general state of health can lead to heart and lung disease and degeneration of bones resulting in osteoporosis and arthritis. Conditions such as diabetes can lead to kidney disease.
All of these conditions will cause some degree of pain and discomfort and may make treating the pain of a dying person more complicated as their needs are complex.
Age
Age is not in itself a cause of pain, but many conditions associated with the process of ageing (e.g. osteoarthritis) are. In addition, the incidence of disease and ill health increases with age. It is important that those caring for the elderly take this into consideration, especially when assisting with personal care needs and moving and handling people.
Do not be tempted to put people’s aches and pains down to ‘old age’ as this may result in a person’s discomfort and pain not being recognised, investigated or treated.
Anorexia
Anorexia means loss of appetite and can be a significant symptom in people who are dying, and, is indeed, very common. Health care workers can do a lot to alleviate this symptom and encourage the person to eat.
Chronic fatigue
Chronic fatigue can be very debilitating for a person with a life limiting illness. Along with all the other symptoms they have and treatments they are receiving they are feeling exhausted, drained and weak continuously. This will, inevitably, affect every aspect of their daily lives, as even the most limited of physical activity uses up all their energy reserves.
5
Nausea and vomiting
Most people have, at some time in their lives, experienced nausea and or vomiting and understand how extremely unpleasant it is. These symptoms in a person who is dying may occur for a variety of reasons, such as:
The illness itself – especially digestive tract disease
Medication side effects – some analgesia cause this
Constipation
Chemotherapy
Strong odours
Breathlessness (Dyspnoea)
Being short of breath can be a very frightening experience for the person themselves and those around them. It can cause the person to panic and terrify relatives who feel helpless.
Providing relief and reassurance is vital. People with life limiting illness, especially as they near the end of their life frequently experience breathlessness.
This may be due to many causes including the illness itself (e.g. lung cancer, emphysema, anaemia), the progress of the illness resulting in build-up of fluid in the abdomen (ascites) pressing on the lungs or triggered or worsened by anxiety, or a sign that a condition is worsening or death is near.
The care worker must observe any changes, such as very shallow or deep ‘gulping’ breaths, quickening or slowing rate or irregularity of the breathing rate. The person may be cyanosed (blue tongue or lips and nails) or the sound of breathing may be come wet/gurgling and they may cough up thick secretions or be unable to remove these themselves.
Anxiety
Anxiety is probably very common in people with life limiting illness, as they are fearful and worried about their diagnoses, prognosis, family, finances, etc. This anxiety will be further compounded by the experience, effect of the illness, treatment and medication.
Anxiety may present itself in a number of ways, including:
Excessive worrying
Poor sleep and restlessness
Agitation and ‘bad temper’
Breathing difficulties, e.g. breathlessness, hyperventilating
Panic attacks
Withdrawal – looking preoccupied – not socialising
6
Other distressing symptoms Thirst
This can be due to:
The disease process
Vomiting or diarrhea causing dehydration
The inability to drink sufficient fluids
Fever
Fever can be caused by infection or the side effects of certain medications.
Jaundice
This may be associated with disease of the liver (e.g. cirrhosis), gall bladder or other parts of the digestive tract. Infections, such as hepatitis can also be a cause.
Constipation
Causes may include:
Disease of the digestive tract
Poor nutrition and/or low fibre diet
Poor mobility
Side effects of certain medications
Diarrhoea
Can be caused by:
Infection
Disease of the digestive tract
Side effects of certain medications and/or treatments
Incontinence
Certain individuals may already be incontinent, however, others may become incontinent as a result of the disease process, immobility and frailty associated with their condition.
7
Insomnia
Causes may include:
Pain
Fear and anxiety
Breathlessness
Side effects of certain medications
Excessive day time sleeping
Response to distressing symptoms
Hiccups
Certain diseases including those of the digestive tract and the effects of medication can lead to hiccups.
Delirium
Delirium is defined as a state of acute mental confusion. This condition is usually brought on by a physical illness, or as a result of surgery, an infection or an adverse reaction to drugs. Acute withdrawal from alcohol in a person who is alcohol dependant can also cause an acute confusional state called delirium tremens.
Signs and symptoms
Disorientation to time, place and person
Impaired memory and communication – slurred or incomprehensible speech
Lack of understanding
Agitation, restlessness and ‘wandering’ behaviour
Hallucinations (usually visual or tactile – feeling of things crawling on their skin)
Showing fear, panic and extreme anxiety
Pyrexia (high temperature)
Disruption of sleep pattern, nightmares and night terrors.
Other signs and symptoms of infection, e.g. respiratory or urinary symptoms.
It is very important to diagnose delirium correctly. Do not assume it is a normal part of the disease process or in the case of an elderly person, a sign of dementia.
Delirium is an acute reversible condition with rapid onset, whereas dementia is usually a slower onset, is progressive and irreversible.
8
Skin irritations
Rashes and itching may be due to medications, reactions to heat and other irritants. Pressure sores and skin breakdown may be caused by a number of intrinsic and extrinsic factors.
Factors in the development of pressure sores
The term ‘pressure sore’ is used to describe damage to the skin or underlying tissue caused by shearing forces and/or direct pressure. The damage can range from skin redness to deep ulcers which involve fat, muscle and bone.
Causes of a pressure sore
A pressure sore develops when the blood supply to the skin is interrupted or cut off. This will cause the underlying tissue to die. Causes can be extrinsic (environmental/external) or intrinsic (within).
Pressure (Extrinsic)
A major cause of pressure sores is unrelieved pressure. This occurs when skin and underlying tissue are directly compressed between bone and a hard surface (e.g. a bed, chair or footrest). People may also be lying on creased or bulky bed linen. Never sit or lay a person along a fold.
The time scale within which damage occurs will vary enormously from person to person. It is recognised that long periods of constant pressure are dangerous. This becomes critical after two hours. However, for very poorly, frail individuals one hour or even less could be dangerous.
Shearing (Extrinsic)
When a person is ‘drag lifted’ up a bed shearing may occur. This means that the circulation is interrupted when the skin moves over underlying bone. This can cause these tissues to die due to a lack of oxygen when the blood supply is interrupted. If muscles are torn, this can result in a deep pressure sore.
9
Friction (Extrinsic)
This occurs when, as a part of shearing the top layer of skin is stripped. This may lead to the development of a superficial pressure sore. Drag lifting is again a significant cause, as is a person rubbing his/her heels against the bed. Rough, starched bed linen will aggravate the problem and should be avoided. Trauma and rough or unsafe moving and handling techniques also increase the risk of damaging the skin and underlying tissues.
Assessment must be carried out within two hours of admission. This is a maximum time scale. Assessment must be holistic and include physical examination of the skin. Findings must be recorded.
It is important that the risk of a person developing pressure sores is accurately assessed and reviewed frequently. Identifying those at risk is essential so that care can be planned to reduce the risk.
Risk assessment is the responsibility of a trained nurse who is accountable for any nursing care prescribed following assessment. The advice of a trained nurse should be sought if there are concerns that a person’s risk is high or their skin is becoming red.
You, as a care worker, can assist by reporting immediately to either a trained nurse or your manager, who will arrange for a trained nurse to assess the person.
10
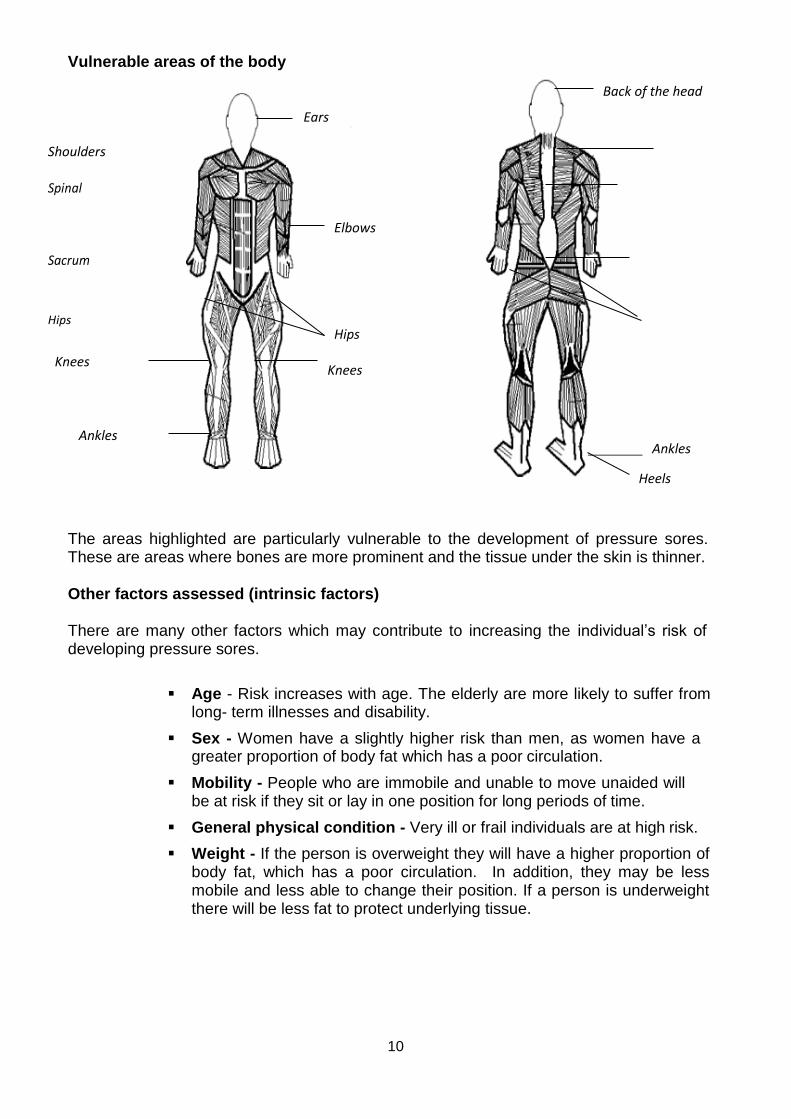
Vulnerable areas of the body
Back of the head
Shoulders
Spinal
Sacrum
Hips
Knees
Ankles
Ankles
Heels
The areas highlighted are particularly vulnerable to the development of pressure sores. These are areas where bones are more prominent and the tissue under the skin is thinner.
Other factors assessed (intrinsic factors)
There are many other factors which may contribute to increasing the individual’s risk of developing pressure sores.
Age - Risk increases with age. The elderly are more likely to suffer from long- term illnesses and disability.
Sex - Women have a slightly higher risk than men, as women have a greater proportion of body fat which has a poor circulation.
Mobility - People who are immobile and unable to move unaided will be at risk if they sit or lay in one position for long periods of time.
General physical condition - Very ill or frail individuals are at high risk.
Weight - If the person is overweight they will have a higher proportion of body fat, which has a poor circulation. In addition, they may be less mobile and less able to change their position. If a person is underweight there will be less fat to protect underlying tissue.
Ears
Elbows
Hips Knees
11
The texture and appearance of the skin - If the skin is already in poor condition, discoloured or broken, this will, inevitably, increase the risk of the skin becoming damaged further. Poor skin condition can result in pressure sores taking longer to heal once they have developed.
Mental health - A person who is depressed may lack the motivation to mobilise or communicate any discomfort to staff. People with dementia may also lack motivation and communication skills. They may also be unable to recognise how to react to pain and discomfort.
Continence status - Incontinence in itself does not cause pressure sores but can cause damage due to faeces and urine burning the skin. This will make the skin fragile.
Circulation - People with poor circulation will be more at risk and healing of an existing pressure sore will be slower.
Diabetes - Side effects of diabetes (especially in those who are dependent on insulin) cause circulation problems and loss of feeling in the hands and lower legs. This results in sores developing more quickly. These are often not felt by the person. Complications of diabetes and other effects of the condition slow down the healing process.
Strokes - Weakness and paralysis of limbs can reduce mobility. Feeling in the affected limbs may be lost or impaired and injuries may go unnoticed. The risk of injury is increased in people who have loss of awareness or sight impairment.
Medication - People who take long term steroid medication develop fragile, papery skin, which tears with the slightest knock or lightest touch. Certain sedation can cause drowsiness and reduce activity. Pain killers may mask symptoms of pressure damage.
Appetite and nutrition - A poor appetite may lead to malnutrition. This will affect the condition of the skin and reduce its ability to heal. Overeating can result in weight gain. Under eating causes weight loss.
As you can see a person who is dying may have many of the factors described both extrinsic and intrinsic factors and be at high risk of developing a pressure sore.
Oedema (swelling) and ascites (fluid in the abdomen)
A build-up of fluid can occur anywhere in the body especially the limbs and the lungs. Ascites is a build-up of fluid in the abdomen and is usually a sign of very advanced disease – particularly cancer – it is extremely uncomfortable and can cause pressure on internal organs, especially the lungs resulting in breathlessness.
Chemotherapy
Cytotoxic drugs are used to treat cancer. They work by destroying cells and may be given orally, by intravenous infusion, or a portable pump. These drugs may be given individually or as a combination. They are particularly useful as they travel through the bloodstream and can treat cancerous cells in any part of the body.
12
These drugs, however, are toxic to all cells including healthy non-cancerous cells. This effect is usually temporary but can lead to unpleasant side effects.
As discussed in Learning Outcome 1.2, all cells in the body can be affected. Anaemia and low white cell count are caused when the bone marrow is affected causing cell production to slow down.
A low white cell count can compromise the immune system and make the person more susceptible to infection. A low red cell count can result in anaemia.
1.4 How symptoms can cause the individual pain and discomfort
All of the symptoms described in Learning Outcome 1.3 can cause the individual pain and discomfort. The disease process itself and damage to and pressure on internal organs and structures can, in itself, cause pain and discomfort. Additionally, the symptoms and side effects associated with treatments, such as chemotherapy and radiotherapy, can result in pain and discomfort.
Anorexia
o This can cause abdominal pain or discomfort and may lead to weight loss and its associated problems.
Chronic fatigue
o Fatigue can lead to aches and pains particularly of the joints and tightness of the chest.
Nausea and vomiting o Abdominal pain, sore throats, and dry mouth can occur, causing distress
and discomfort.
Breathlessness o Chest pain and tightness can result when breathing becomes difficult and laboured.
Anxiety
o Many physical effects can result from anxiety including joint pains, chest pain and tightness and digestive discomfort.
Constipation and diarrhoea
o These can cause abdominal and rectal pain and discomfort.
Incontinence
o Discomfort can result due to overflow incontinence, the use of aids and appliances such as catheters, associated urinary tract infections and moisture affecting the integrity of the skin.
Fever
o This can lead to discomfort caused by sweating, shivering and feeling excessively hot.
13
Jaundice o The disease or infection process involved in development of jaundice can cause
pain and discomfort.
Insomnia o Lack of sleep may result in headaches, general aches and pains and the discomfort
associated with fatigue.
Hiccups o These may lead to abdominal pain and discomfort and symptoms relating to fatigue.
Delirium
o Symptoms associated with delirium, such as anxiety, fear, pyrexia (fever), sleep disturbances, or respiratory or urinary symptoms can lead to pain and discomfort.
Effects of pressure sores on the individual Pain
The pain which results from a pressure sore is a major problem in itself. However, pain can cause other related effects, such as:
Unable to rest or sleep properly
Reduced mobility as the fear of pain causes the person to be reluctant to move
Long-term use of certain analgesia (pain relief) may cause constipation.
Infected pressure sores
Cause an unpleasant odour
A high temperature which may cause the person to feel very unwell
Anorexia (loss of appetite) causing malnutrition
Septicemia (blood poisoning). This is an extremely serious condition from which death may result
Other effects Physical
Discomfort when sores are dressed
Formation of scars
May need surgical intervention or other unpleasant treatments (e.g. maggots)
Side effects from the use of medication, such as antibiotics and analgesia
14
Psychological
Including anxiety, depression and loss of confidence, may result in loss of independence.
Social
Social isolation may result in a person’s movements are restricted due to the effects of the sore. Also visitors may restrict contact time if the person is reluctant to communicate or if odour from the wound is unpleasant.
1.5 Different factors that can alleviate or exacerbate symptoms
There are a wide range of factors including:
Anxiety
Fear
Boredom
Effectiveness of symptom control strategies
Inactivity or excessive activity
Environmental factors including suitability and availability of facilities, amenities aids and equipment
Positioning/repositioning
Attitudes of others
Emotional/psychological aspects

15
Learning outcome 2
The learner will:
Understand a range of therapeutic options used to support effective symptom relief. The
learner can:
2.1 Identify a range of interventions that can be used to provide symptom relief
2.2 Clarify how an individual’s culture and beliefs might influence their approach to symptom management
2.1 Interventions to provide symptom relief
In order to provide person-centred, holistic care all the client’s needs must be identified and addressed. This will include other distressing symptoms as well as pain. Although symptoms may not be a source of discomfort or distress, as a result, they can have a negative effect upon a person’s quality of life, causing unnecessary suffering and unmet needs.
Quality of life
When an individual is diagnosed with a life threatening or life limiting illness, it becomes the responsibility of those who care for them to ensure that they are helped to live the remainder of their life as comfortably and as fully as possible.
It is essential that the person who is dying is in control of what happens to them. Other people may think that they know what is best for the individual, but the only person who truly knows is the individual themselves. People will have different expectations of what quality of life means to them. Consideration should be always be given to:
Appropriate support and nursing care, especially with regard to pain relief and other distressing symptoms.
Cultural, religious and spiritual beliefs and practices. Sensitivity to ethnic and religious beliefs should be observed and time should be offered to listen to and support the individual and their relatives with the complexities of the experience that they are going through.
Emotional and personal aspects of care. The wishes of the individual should always be taken into consideration. Discussion about the dying process allows individuals the opportunity to make decisions. They may want to decide what arrangements should be made to manage the final stages of their illness and may wish to attend to personal and other concerns that they consider important towards the end of their life.
Privacy and dignity. Individuals who are dying should be given the same respect and standard of care as anyone else. They and their loved ones should be treated with understanding and compassion. It is essential that the individual’s care needs are identified and met appropriately.
16
Managing pain and the use of medication
The types of drugs used to relieve pain are called analgesics. The purpose of palliative medicine is the use of pain relief and symptom control as part of end of life care. The management of pain must be part of a dying person’s care plan. It is essential that all care workers are aware of methods and issues associated with pain and symptom control and they are familiar with the care organisation’s policies and procedures. They will then be able to support the individual and the doctors and nurses trained in pain management.
Measures to alleviate pain and discomfort
Pain and discomfort can be alleviated using a variety of measures involving various members of the care team and other care professionals:
Care professionals and care workers within the care team
Nurses – specialist nurses such as MacMillan nurses
Doctors (GPs, physicians, surgeons, pain control specialists)
Managers
Physiotherapists will treat people following an operation, injury or stroke, using a combination of exercise and aids and equipment
Chiropodist – will treat foot and nail problems which will relieve pain and discomfort for individuals, especially when walking or standing
Dentist – to treat toothache, gum disease, neuralgia and infections (abscesses, etc.)
Occupational therapists – can provide aids and equipment to increase independence and maximise the individual’s comfort
Counsellors.
Medication
Medication can be obtained in a number of ways:
Over the Prescribed by medical Homeopathic counter practitioner and herbal chemist/shops remedies
Over the counter medication does not require a prescription, and can be purchased from a variety of shops or local pharmacies. Paracetamol, Aspirin or Ibuprofen can be purchased under a number of trade names for pain relief. Items such as cod-liver oil capsules (to help individuals suffering from arthritis), laxatives (for constipation) or antihistamines (for hay fever) can also be purchased.
Although a pharmacist will give individuals advice on safe use, generally we read the instructions and recommendations on the packet or bottle and use our own judgement for use.
17
Allopathic medication
This is orthodox medical treatment using drugs that treat and alleviate specific symptoms and disease. The medication, prescribed by a GP or other qualified practitioner, such as a dentist or nurse, is obtained from the pharmacy and administered at times and in doses specified by the prescriber. Medication would include:
Analgesia – painkillers, e.g. Morphine
Laxatives – to relieve constipation
Antihistamines – to relieve symptoms of allergies
Anti-inflammatory – to treat arthritis and joint pain
Antacids – to relieve symptoms caused by digestive problems
Antibiotics – to treat infections
Antidepressants and anxiolytics – to relieve anxiety and depression.
Medication and the care worker
It is important that you recognise your role in the administration, monitoring and storage of medication. It is vital that medication is handled, stored and administered safely. It is suggested that you, as a care worker, undertake a recognised educational course to ensure you understand how to deal with medication safely. This is particularly relevant to care workers who are involved in the administration of medication within their care environment.
Types of pain and symptoms relief
Analgesics are a type of medication which provides relief from pain. There are two groups of analgesics, opiates and non-opiates.
The Misuse of Drugs regulations classify Controlled Drugs into five Schedules:
Schedule 1 – Drugs in Schedule 1 are the most stringently controlled. Schedule 1 drugs are not authorised for medical use and can only be supplied, possessed or administered by a person authorised by a licence issued by the Home Office. Such licences are granted for research or special purposes.
These drugs cannot be prescribed by doctors or dispensed by pharmacists. This is the closest that the British Law comes to total prohibition. Drugs in Schedule 1 include LSD, Cannabis and raw Opium.
Schedule 2 – Opiates such as: Diamorphine, Morphine, Methadone and Fentanyl patches, major stimulants such as Amphetamines and Quinalbarbitone (severe insomnia).
Requirements as to the safe custody apply to all Schedule 2 Controlled Drugs, except Quinalbarbitone.
18
Schedule 3 – Minor stimulant drugs such as: Benzfetamine (appetite suppressant) and Temazepam (sleeping tablet).
Schedule 4 – Contains most of the benzodiazepines, e.g. Diazepam
Schedule 5 – Contains the drugs that are considered to pose minimal risk of abuse. These non-injectable, small dose preparations can be purchased over the counter at a pharmacy without a prescription but once obtained it is illegal for them to be supplied to another person. Many of these preparations include well-known cough mixtures and painkillers.
There are lots of controlled drugs, some of which will be more common than others. The pharmacist will inform you as to whether the drug is controlled or not.
Controlled drugs
Standard 9.7 of National Minimum Standards states: “In Care Homes with personal care only, all medicines, including Controlled Drugs (except those for self-administration) are administered by designated and appropriately trained staff. The administration of Controlled Drugs is witnessed by another designated appropriately trained member of staff”.
Storage of controlled drugs
Unless individuals are self-medicating, controlled drugs must be stored in cupboards which meet the requirements set out in the Misuse of Drugs (Safe Custody) Regulations 1973. These regulations specify the quality, construction, method of fixing and the lockage of controlled drugs’ cupboards.
It is usual within care homes, where controlled drug cupboards are locked, metal cupboards within a locked metal cupboard, which are securely wall mounted. You may also find controlled drug cupboards which are single wall mounted cupboards made from metal, which exclusively store controlled drugs.
Only staff with authorised access are permitted to hold the controlled drug cupboard keys, which means you should never give the keys to a member of staff who is not permitted access to controlled drugs.
You must only store controlled drugs in the controlled drug cupboard; items of value such as money/jewellery or other non-controlled drugs should not be stored in the controlled drug cupboard.
For people who self-administer their own controlled drugs, they should be stored in their own individual lockable cupboard, to which the person has his/her own key. Controlled drugs should only be taken out of the controlled drug cupboard whilst they are being dispensed or counted for stock control purposes.
19
Opiates
Opiates can be divided into two groups:
Strong opiates – e.g. Diamorphine - used for moderate to severe pain
Weak opiates – e.g. Codeine.
Opiates should be prescribed regularly, either approximately four hourly or on a more long acting basis, e.g. 12/24 hourly. Opiates can be given orally unless the person suffers side effects, or has digestive tract problems or swallowing difficulties. Fentanyl patches last for three days over which they continually release medication through the skin (trans-dermal). A syringe driver is a method by which a needle is placed under the skin and is attached to a syringe where a small battery operated pump delivers a continuous dosage of an opiate, such as Diamorphine. The syringe is renewed usually every 24 hours. Other medication, such as an anti-emetic can be given this way. The equipment is very small and can be carried in a holster or pouch, hidden under a person’s clothing.
Non-opiates
These are likely to be the most commonly used pain relief medication. They include Paracetamol, and non-steroidal anti-inflammatory drugs such as Ibuprofen and aspirin. These medications are used to treat mild to moderate pain, to lower fever, and, in the case of NSAIDS, to relieve bone and joint pain.
Co-analgesics/adjuvant
This is medication that may be used along with analgesic to treat other symptoms. These drugs may include anti-emetics (for nausea and vomiting) and anti- depressants.
Complementary, alternative and integrative medicine
Complementary therapies
These are therapies that are used alongside more traditional treatments, such as analgesics and other prescribed medication.
Following assessment, it may be considered that people who are dying may benefit from other therapies.
Complementary therapies to treat pain and distress are much more popular today and many are gaining acceptance within the National Health Service. These methods should only be carried out by a trained practitioner.
20
Alternative therapies
These are therapies that are used instead of conventional treatment, and may involve the use of herbal medicines or homeopathy.
Homeopathic preparations use minute quantities of natural substances, which in large doses produce effects similar to those of the disease being treated, the same method used to vaccinate against some diseases as a preventative measure.
A homeopath aims to treat the client holistically. After discussing the person’s problems in detail they will recommend substances derived from vegetable, animal or mineral sources.
Alternatively some of these remedies can be obtained at the pharmacy or health food shops as well as herbal remedies from flower essences and oils that can be heated in an oil burner.
Many of these are based on previous herbal remedies used when the majority of the population did not have access to trained physicians (pre NHS).
Examples of such remedies are:
St John’s Wort for mild depression
Lavender oil has a calming effect
Cranberry juice for urine infections
When an individual is considering using an alternative medicine instead of an orthodox medicine they should always discuss this with their doctor or specialist. Discontinuing or declining orthodox medicine could have implications for the well- being of the dying person and should not be undertaken without the person being aware of any possible consequence.
Integrative medicine
This involves a combination of orthodox treatment with complementary therapy or an alternative medicine.
21
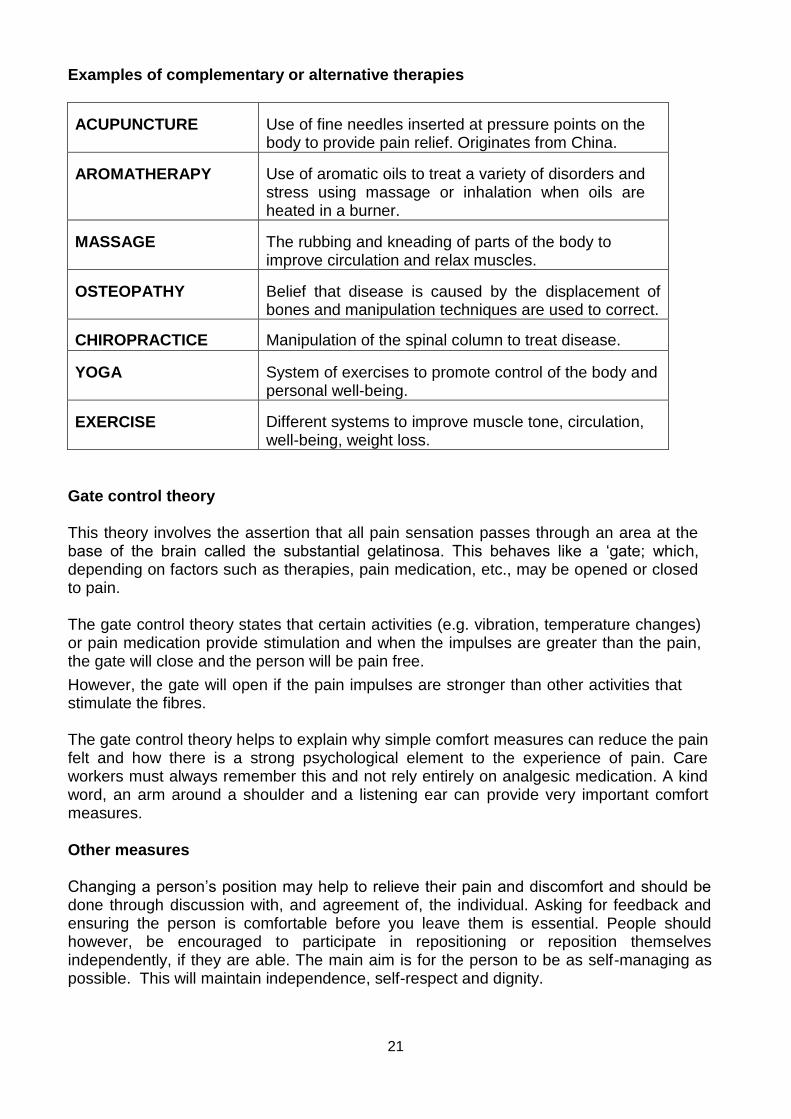
Examples of complementary or alternative therapies
ACUPUNCTURE Use of fine needles inserted at pressure points on the body to provide pain relief. Originates from China.
AROMATHERAPY Use of aromatic oils to treat a variety of disorders and stress using massage or inhalation when oils are heated in a burner.
MASSAGE The rubbing and kneading of parts of the body to improve circulation and relax muscles.
OSTEOPATHY Belief that disease is caused by the displacement of bones and manipulation techniques are used to correct.
CHIROPRACTICE Manipulation of the spinal column to treat disease.
YOGA System of exercises to promote control of the body and personal well-being.
EXERCISE Different systems to improve muscle tone, circulation, well-being, weight loss.
Gate control theory
This theory involves the assertion that all pain sensation passes through an area at the base of the brain called the substantial gelatinosa. This behaves like a ‘gate; which, depending on factors such as therapies, pain medication, etc., may be opened or closed to pain.
The gate control theory states that certain activities (e.g. vibration, temperature changes) or pain medication provide stimulation and when the impulses are greater than the pain, the gate will close and the person will be pain free.
However, the gate will open if the pain impulses are stronger than other activities that stimulate the fibres.
The gate control theory helps to explain why simple comfort measures can reduce the pain felt and how there is a strong psychological element to the experience of pain. Care workers must always remember this and not rely entirely on analgesic medication. A kind word, an arm around a shoulder and a listening ear can provide very important comfort measures.
Other measures
Changing a person’s position may help to relieve their pain and discomfort and should be done through discussion with, and agreement of, the individual. Asking for feedback and ensuring the person is comfortable before you leave them is essential. People should however, be encouraged to participate in repositioning or reposition themselves independently, if they are able. The main aim is for the person to be as self-managing as possible. This will maintain independence, self-respect and dignity.
22
Counselling
People may benefit from being able to talk over their problems with a trained counsellor. The aim of counselling is for the person to be able, with the support of the counsellor, to make decisions and deal with their problems.
Relaxation therapies
People are shown relaxation techniques to enable them to reduce their stress and anxiety levels. Those techniques can be particularly useful when pain is caused (i.e. migraine-tension headaches) or worsened by stress and anxiety.
Supporting people with distressing symptoms - the role of the health care worker
The health care worker has a vital role to play in the management and control of distressing symptoms. Care workers should:
Observe the person for any changes in condition or unusual
signs or symptoms
Provide support
Give reassurance and whatever forms of therapy staff are trained to offer
Report and document findings
23
Supporting a person with anorexia
There are a number of strategies that care staff can employ to improve the person’s dietary intake, such as:
Identify possible causes and plan appropriate treatment. Problems such as nausea and vomiting and constipation can be alleviated and this may improve the person’s appetite. Depressive illness can cause loss of appetite and loss of motivation to prepare food. Treating depression can be beneficial to the person’s dietary intake.
Assess, identify needs and formulate a plan. This must involve the person themselves, family and friends.
Menus and eating routine should be put into place that meet the person’s needs and preferences.
Offer small portions of food at regular intervals
Be flexible with meal times, don’t expect people to eat according to the clock
Find out the person’s likes and dislikes with regard to food
Ensure that food is attractively presented
Ensure the eating environment is comfortable and provide companionship during mealtimes. However, be aware that communal eating does not suit everyone and some people may find watching other people eat off-putting.
Refer to a doctor who may be able to prescribe appetite stimulating medications
Consider the smells of food – if the person dislikes a particular food or food odour this may discourage them from eating.
Seek the advice of a dietician who can compile a diet high in nutrition and prescribe nutritional supplements that can be offered to the person.
Reassure family members who will obviously be concerned and may focus on trying to persuade and put pressure on the person to eat. Ensure they are given plenty of information and are involved and assist the person to eat where this is appropriate. However, try to dissuade them from making anorexia an issue as this may discourage the person further. They may feel they are helping if they are asked to bring in special treats and favourite foods, drinks and snacks. Although they must agree that staff and the dietician are aware of any foods they are bringing in.
24
Supporting a person with chronic fatigue
A care worker can support the individual in a number of ways, including:
Offering lighter meals and smaller more frequent portions whilst maintaining nutritional content. Eating can exhaust a person with chronic fatigue.
Encourage light physical activity when appropriate - a physiotherapist may be able to advise.
Plan activities that require concentration when a person is rested Enable and encourage the person to have rest periods Discuss with the person and their family appropriate visiting
arrangements and routines for those who live at home, so as not to overtire the person.
Ensure fluid intake is sufficient Identify any other symptoms, conditions or treatments that may
aggravate or cause fatigue (e.g. anaemia) and provide relief or treatment where possible.
Provide quiet times during the day, to allow people to rest without being disturbed
Identify ways a person may conserve their energy – limiting or avoiding strenuous or taxing activities.
Supporting a person with vomiting and nausea
It is vital that these symptoms are controlled as soon as possible. This can be achieved in a variety of ways:
Identify cause – it may occasionally be possible to remove the cause, e.g. a strong smell
Formulate a plan. Involve the client and their family.
Use of anti-emeties – these can be used in conjunction with analgesia and can be administered orally, by injection, via a syringe driver.
Reassure and support the client and their family. Remember you can offer practical help as well as information and emotional support.
Clean up the vomit and the client – ensure privacy and dignity. Do this promptly.
Ensure that the client has access to a vomit bowl, tissues and water and has a means of calling for assistance.
Help the client to clean their mouth and brush their teeth
Dispose of all contaminated waste and linen appropriately
Clear away promptly
Ventilate and deodorise the room
Use recommended cleaning fluids
Use PPE (e.g. apron and gloves)
Always offer reassurance and support. The client may be very embarrassed, and family may find the smell distressing and clearing up difficult and unpleasant.

25
Supporting a person with breathlessness (Dyspnoea)
There are a number of strategies you can use to alleviate symptoms and provide support and reassurance, such as:
Be there for the client. Speak calmly and encourage them to reduce their anxiety and to breathe more regularly. If the client is known to suffer severe anxiety and panic attacks encourage them to breathe in and out into a paper bag. Check that this is the problem and that this method is within the care plan. Holding the client’s hand or gently rubbing their back can provide great comfort.
Use oxygen, as prescribed, via a nasal cannulae or a face mask
Administer any medication prescribed to dry up secretions, suppress or relieve anxiety and distress. Monitor and report effects.
Ensure the client has a means of summoning assistance – e.g. a call bell (a small hand bell can be used in a person’s home).
Make sure the client does not over-exert themselves. Spread out activities with periods of rest in between. For example, showering/bathing immediately before a mealtime, receiving visitors, attending a doctor’s appointment may exhaust the client and lead to breathlessness.
Ensure the room is not too warm and is well ventilated. An electric fan may help. The use of a humidifier to moisten the air can help loosen secretions.
Encourage the client to wear loose clothing (a shirt and tie may aggravate the feeling of being out of breath), loosen bed clothes.
People with breathing difficulties may obtain relief from sitting upright and leaning slightly forward, possibly against a bed table (sometimes called orthopnoeic position). Check with the client as they may have a particular preference with regard to positioning. Elevate the head of the bed if they are unable to sit up.
Night time can cause anxiety – ensure that clients can summon assistance quickly and that there is somebody available to sit with the client to offer comfort and support. A night light may be beneficial.
Listen to the client’s worries and concerns – make efforts to help the client to resolve any difficulties or problems they have. This can reduce stress and prevent anxiety.
Use and encourage relaxation, complementary and alternative therapies within the plan of care.
Frequent mouth care. This will clear and clean excess secretions and moisten a dry mouth.
Physiotherapy – may help to remove excess secretions and encourage cough reflex.
All of those interventions may provide relief and reassurance. However, if they do not you will need to report this and ask for advice and assistance as more specialist support and treatment may be required from doctors, nurses or other health care professionals.
26
Precautions when using oxygen therapy
Oxygen must always be prescribed and administered as the person who prescribed it instructs
Always ensure that there are adequate supplies of oxygen available – clients being cared for at home will need to be informed of when, how and where to order replacement oxygen supplies and report faults 24 hours a day.
Ensure that oxygen masks and nasal cannulae are positioned correctly, comfortably and securely
Keep nasal passages and mouth moist
Ensure the tubing does not rub and cause friction to the skin – padding may be used between the skin and tubing
Oxygen is flammable – ensure that there is no ignition source – e.g. lighting cigarettes or matches
Store oxygen safely
Ensure oxygen is switched off when not in use. This is particularly important in those people who self-medicate oxygen. This applies to piped oxygen and cylinders.
Supporting a person with anxiety
It is important that you recognise these signs and symptoms as a client may not always voice their concerns and worries and may not tell you they feel anxious. The client with anxiety can be supported in many ways:
Actively listening – talking about how you feel and having the presence of another person who is offering comfort and reassurance can reduce anxiety.
Discuss with the client, their family and friends and the care team so that strategies are planned as a team to reduce anxiety by establishing the causes and adopting a problem solving approach.
Certain medication, alcohol and excess caffeine may cause increased anxiety levels and may be withdrawn or reduced to relieve symptoms.
A client may benefit from counselling, access to a minister of religion, social worker or other professionals, such as a solicitor.
Medication to reduce anxiety.
27
Supporting other distressing symptoms
Thirst – prevent and treat dehydration. Careful mouth care.
Fever – treat infection. Tepid sponging, a cool room and an electric fan. Use of antipyretic medication such as Paracetamol.
Jaundice – Yellowing of skin and whites of eyes usually caused by liver disease/condition – jaundice although it looks frightening to the family and the client is not a physically distressing symptom unless there is itching. Care staff should provide support and reassurance. Medical intervention may be required to treat any troublesome itching.
Constipation – Ensure fluid and fibre intake is adequate. An aperient (laxative) may need to be prescribed. Bowel habits should be monitored and medication reviewed as some may cause constipation – doctor may prescribe an alternative.
Diarrhea – can be a very distressing symptom and can lead to dehydration, weakness and skin breakdown. Any infection must be treated and medication used to manage diarrhea. Look at the client’s diet – avoid highly spiced food and milk products. Certain medication may cause diarrhea; this should be reviewed and if possible as alternative prescribed.
Incontinence – can have many causes, e.g. physical disease, neurological disorder or immobility causing the client not to be able to access toilet facilities. Full assistance should be given for clients to access toilet facilities (or commode, bedpan or urine bottle) wash, dry and change soiled clothing and bedding. A client should be able to call for assistance and be attended to promptly. The use of continence aids, such as pads and mattress protectors should be employed. Family and carers should be given practical and emotional support and the client’s dignity and privacy should be maintained at all times.
Insomnia - can add to a client’s distress and can worsen fatigue and anxiety. Ensure the client undertakes a relaxing activity before bed, offer a milky drink. Discuss any concerns a client has which may cause greater anxiety during the quiet of the night.
28
Care workers can do many things to help clients to sleep and rest. For example:
The individual’s personal routines and preferences are identified and accommodated as long as these do not interfere with, or upset others.
Do not overlook the needs and interests of the more dependent individuals. They may not be able to make their wishes known.
Sleep requirement declines with age. Avoid putting people to bed very early (unless this is what they wish) as it is unrealistic to expect a person who goes to bed at 7pm to settle immediately and sleep, uninterrupted, until 7am.
Ensure that individuals are offered the toilet before they go to bed
Provide all individuals with a call bell to summon assistance
Clients with heart and lung disease often have breathing difficulties, especially during the night. If they are receiving oxygen therapy and they cannot see staff they may be concerned that the supply may fail, especially if the supply is from a cylinder which will eventually empty. Clients with cardiac failure can also be frightened due to shortness of breath, often due to their ‘sliding down’ in their bed. These individuals need to sleep and rest in a sitting position and see their care workers as well as the care workers seeing them. Consider how you would feel if you were unable to breathe without the aid of added oxygen.
Carry out positional changes with the minimum disturbance to the client
Encourage rest periods during the day, but try to keep clients occupied with activities, socialising, etc. A client who sleeps all day will not sleep at night. Activity also prevents boredom and frustration.
Regularly check on individuals in your care – quietly and discreetly, throughout the night, ideally without disturbing them. Observe for wakefulness, restlessness and agitation. It is often wrongly assumed that the client’s inability to settle is that their noisiness and agitation are preventing them from sleeping. Often the cause of agitation is the reason a client can’t sleep. Remove the cause = remove the agitation = increased likelihood of sleep and rest.
Offer a hot or cold drink before bed. Avoid caffeine. If the client requests a small ‘tot’ of alcohol, a doctor must prescribe this. Some clients may like to have a cold drink beside the bed overnight.
A client may wish to watch TV or listen to the radio – ensure this does not disturb others.
Deal with incontinence and requests for the toilet promptly – use pads advised by continence advisor. Do not wake individuals unless this is advised or they themselves ask you.
Ensure there is a quiet period during the day
Care workers should wear shoes with quiet soles and be careful to behave in a quiet manner whilst clients rest and sleep.
Report and remove (if possible) any problems with noise from equipment, the client themselves or others.
Encourage others to be quiet
29
Routines may need to be changed to accommodate a client’s need for rest and sleep.
Noisy maintenance work and the cleaners’ and cooks’ routines may need to be altered to allow clients to rest. There is little point in having a quiet period, if this is the time the fire alarms are tested, the cleaner does the vacuuming or the cook tidies the pan cupboard!
Ensure that visitors and workers, as well as other clients, respect the individuals’ need to have a rest period during the day.
If possible, shut bedroom doors. This must be considered safe by your manager. A closed door will reduce noise from both within and outside the room.
Adjust lighting to suit individual preference – providing this does not affect others. The client may need the light subdued by use of a dimmer switch, closing curtains and blinds, or the position changed to reduce glare. Other clients may find the night sky soothing and prefer curtains to be left open once the sky is dark. It is up to you to communicate with the client to discover what suits them.
Ensure heating is adequate. Problems may be caused by the ambient temperature of the room - a client with circulation problems requires the background temperature to be warm or their hands and feet will be cold and affect their ability to sleep or rest. How do you sleep if your feet are cold when going to bed? Bed socks may be helpful or they may prefer the room temperature to be increased.
Provide comfortable bedding – sheets and blankets may be easier to add or remove, than a quilt. Bed cradles, etc., can increase the client’s comfort.
Ensure any music chosen is of the individual’s preference
The position of TVs and radios may need to be changed. Ear-phones may be a solution to reduce noise levels.
Space should be sufficient to ensure adequate sleep and rest. Trying to relax and rest in a cramped area may be impossible. Lack of space can restrict access to rest and sleep areas and compromise safety.
Furniture must be arranged in a way that allows adequate space to move around safely and does not cause an obstruction which may injure others.
Hiccups
Repositioning and elevating the head of the bed can help. However, medication may be required.
Skin irritations
Establish the cause and if possible remove irritant or treat with local creams and ointments and oral medications. Measures to prevent pressure sores are essential. Any pressure sores that have already developed should be treated.
Oedema and ascites
Medication such as diuretics can relieve symptoms. A doctor may periodically drain the fluid (paracentesis) to relieve symptoms and make the client more comfortable.
30
Delirium
Supporting a client with delirium
A calm, reassuring approach
Make the client feel safe. Having familiar people and objects around them can provide reassurance and reduce confusion.
Minimise stimulation by reducing noise levels and lighting, placing the client in a quiet environment away from the main activity.
Re-orientate to time, place and person being careful to do this quietly, patiently whilst preserving the client’s dignity and self-esteem.
Investigate the cause – review medication and screen for infection, monitor fluid intake and output as delirium can be worsened by dehydration.
Assist nursing and medical staff in treating the cause.
Activities to prevent and minimise the effect of pressure
It is good practice to assess risk using an up to date assessment scale, such as The Waterlow Pressure Sore Prevention/Treatment Policy (1985). Other risk assessment scales have also been developed, for example:
Norton (1962)
Medley (1991)
You may have considered a number of practical care interventions. The development of a pressure sore should never be considered an unavoidable consequence of immobility, illness, disease or old age.
Pressure sores are preventable; therefore care should be focussed on measures to stop their development.
However, pressure sores do occur and care planned to prevent their development can be applied to minimise their effects and prevent further deterioration.
Keeping people mobile is an extremely important aspect of preventing the development of pressure sores. It must always be remembered that it is not only people who are bedridden (bed bound) who are at risk. Bed sores can be a misleading term. People who spend long periods sitting motionless in a chair, maybe with their heels on a foot stool, unable to change position independently, are also at risk.
Practical care interventions
It is vital that the individual’s level of mobility and independence is identified, in order that realistic goals can be set within the plan of care.
31
Exercise, mobility and recreation
Keeping active is an important part of preventing pressure sores. You can encourage clients to take short walks, take part in recreational activities and help with tasks, such as laying tables. You can help, whenever possible, by walking clients to the toilet or lounge instead of using a wheelchair. Clients can exercise limbs and gently change their position whilst they are sitting.
Passive exercise
This is exercise, performed by the care worker, for clients who are immobile. This involves taking the limbs through their full range of movement for at least five minutes in every hour.
Relieving pressure
Individuals must change their position at least every two hours. Ill and frail clients may need to be repositioned hourly or even more frequently.
For those clients who are unable to do this themselves you must do this for them. This will range from reminding them to move and giving minimal assistance to changing the position of an immobile client.
It is important that you are aware of the clients’ level of risk and the care planned to deal with this. You must know how frequently the client’s position is to be changed, the condition of the client’s skin, what position they need to be in, how the positional change is to be carried out and any equipment required to do this.
Positional change must be recorded, along with the condition of the skin. The client should be involved and fully understand the reasons for positional changes, including the benefits to them and the adverse effects of long periods of unrelieved pressure, shearing and friction. The clients can then make informed choices and participate actively in the positional change (if they are able).
Your care establishment should have documentation recording the level of risk of the development of a pressure sore, the strategies planned to assist in preventing and minimising the adverse effects of pressure, including changes of position.
Promoting self-management
To maintain independence it is important that a client is encouraged to be as self- managing as possible. A pleasant, patient attitude and gentle encouragement should build the client’s confidence. Goals set should be realistic and achievable. Freedom of choice should be respected, even if the client does not wish to cooperate. Problems should be discussed with the manager, so care can be reviewed and alternatives explored.
32
Maintaining respect for clients who are dying
It is very important that you show respect for clients who are dying. This can be achieved in a number of ways. Together these will help to maintain a client’s self- esteem, build confidence and encourage independence.
Comfort
It is vital that you ensure that comfort is assured for the client who is dying. The care team should be aware of client’s needs and strive to meet these whilst ensuring that pain and discomfort are relieved. Creating a relaxing and harmonious atmosphere is as important as having pleasant and comfortable physical surroundings.
Preparation
Prior to assisting an individual with personal hygiene it is important that they and the environment are carefully prepared.
Establishing the support the client will require, and the method of hygiene appropriate
It is important that you know how much support the individual needs. Giving too much or too little support can have physical, psychological and health and safety consequences.
You must find out what support is needed before you attend to personal hygiene. To do this you will need to find information from:
Your manager/senior or trained staff
The client’s care notes
The client themselves.
Meeting an individual’s needs All
methods
Spectacles and hearing aids should be replaced
The client should be returned to an area of their choice
The client should be made comfortable
A call bell placed within reach
The area should be left clean and tidy.
33
Hair washing and styling
It is important that a client’s hair is kept clean. How often the hair is washed will vary between individuals and be due to many factors.
When helping a client to wash their hair, their own choice of a suitable shampoo should be available. Some care homes have a hairdresser who visits, but you do not have to be a hairdresser to wash and style a client’s hair.
Let the individual choose their style and method, e.g. blow drying, using rollers.
Care of the nails
Nail care is an important part of personal hygiene. You must take care when cutting, or filing them to prevent injury. Nails should be cut straight across.
A chiropodist should always cut the nails of a diabetic or of a client who has thickened nails. You must ensure that nails are clean. Do not use sharp objects to clean under the nails. Care workers’ nails should be kept short and clean to prevent injury and infection.
Shaving and removal of unwanted hair
Removal of surplus hair
Shaving is mainly a male activity, however, women may need to remove unwanted hair on their body or face. Shaving may be done with an electric shaver, a razor and blades or a disposable razor (using foam, soap or gel). Hair removing creams can also be used. You must take care not to cut the client if you are shaving them. Razors must never be shared.
Accessing toilet facilities - including alternatives to toilets
You may need to assist individuals to access and use toilet facilities. Clients may require assistance to access toilet facilities, as they are not able to do this independently. Alternatively a client may not be aware of the need to use the toilet and the care worker may need to remind and encourage the client to use the toilet at regular intervals.
Level of assistance
It is vital that you establish the level of assistance the client needs before you begin.
Assisting the client to use toilet facilities - including alternatives to the toilet
Your assistance may be required to help a client to use the toilet facility. Being aware of the amount of help the client requires, will ensure that you give only the help needed. This may include help with getting on and off the toilet and assistance with cleaning, wiping and adjusting clothing.
34
Mouth care
Keeping the mouth clean
Care of the mouth is very important. The teeth should be cleaned using a toothbrush, a soft brush can be used for the gums and palate and tongue. Mouth washes freshen the mouth, however, all individuals should be given the opportunity to brush their teeth twice a day, or helped to do this. Very many elderly people have dentures. These should be soaked and brushed.
Clients who are very ill may need help to maintain mouth care.
Oral hygiene may need to be carried out as frequently as two-hourly, dependant on need.
Measures to keep the mouth moist and pain free
A dry mouth can be very uncomfortable, make the client feel thirsty and lead to ulcers and cracking of the lips and tongue.
Ensure that the client does not become dehydrated by encouraging oral fluids where this is possible or give ice to suck and artificial saliva products where this is prescribed. Rinsing the mouth frequently and keeping the lips moist will relieve discomfort.
Antiseptic mouth washes, used frequently, will help prevent infections and ulcers. Where there is an infection, such as thrush, a doctor can prescribe a local medicine and analgesic.
2.2 How an individual’s culture and beliefs might influence their preferred
approach to symptom management
There are a variety of reasons why an individual’s culture and beliefs may influence their approach to symptom management. These may include:
Gender – believing that is it not manly to accept certain treatments or to admit to symptoms such as pain and discomfort.
Religious beliefs may influence choice of symptom management. Some people may believe that God guides medical and nursing staff, whilst others may believe that pain and suffering are sent for them to endure.
Personal beliefs may affect choices such as complementary therapies and analgesia. Some people may believe these will help improve their quality of life. Others may distrust complementary therapies or fear becoming addicted to opiate analgesics.
Certain cultures may distrust anyone outside their family or cultural group, therefore become reluctant to consider any approaches to symptom management suggested or advised by health care professionals.
35
Learning outcome 3
The learner will:
Understand the principles of pain management. The
learner can:
3.1 Describe common types of pain
3.2 Identify signs that might indicate that an individual is experiencing pain
3.3 Suggest different ways to monitor pain
3.4 Describe factors that can influence an individual’s perception of pain
3.5 Explain the World Health Organisation’s analgesic ladder
3.6 Explain the importance of maintaining regular pain relief
3.7 Outline the reasons for planning activities after pain relief has taken effect
3.1 Common types of pain The
sensation of pain
Pain is defined as a physical sensation relayed to the brain through the nervous system.
It must be remembered, however, that any definition is a clinical explanation and does not describe how each individual experiences pain. Every person will have a different pain experience even if the illness or disease process is the same. What is bearable for one person may be completely unbearable for another. Never assume that certain illnesses or conditions are always associated with a specific type and level of pain. Everyone will experience pain in different ways, as unique as the individual themselves.
Always understand and accept that a person’s pain is what they say it is, not what you think it should be. Do not be judgemental or make assumptions – observe and listen to the person themselves.
Common types of pain
It is important that, as a care worker, you understand that there are different types of pain that require different responses. This is vital to enable the type of pain to be identified and the appropriate treatment response given.
Acute pain
This is usually a sign that the body is responding to the symptoms of a sudden illness or disease process (e.g. heart attack, appendicitis) or that an injury has occurred (e.g. a fracture, burn, cut).
36
The resulting pain is severe and lasts until the cause is treated, healing takes place, pain relief is given or, at worst, the person dies (e.g. heart pain or a ruptured appendix) acute pain lasts a relatively short time. It is the body’s way of warning us there is something very wrong and it is so incapacitating it cannot be ignored or tolerated.
Chronic pain
This type of pain is ‘persistent’, although not necessarily present all the time. It may come in bouts with hours, days or even weeks in between. Chronic pain can range from mild to severe. However, for many people the pain does not go away and is present to some degree all the time. Some people may find the pain so severe that it affects all their activities of daily living, which can lead to immobility and dependence.
Appropriate and effective treatment can significantly improve a person’s life as the pain is controlled and they are able to continue to have a more fulfilling and independent life.
Break through pain
People may experience this when they have periods where pain breaks through. This is usually an indication that certain activities (e.g. walking, being moved in bed, etc.) are aggravating their symptoms or that, if they are receiving pain medication, it is inadequate.
3.2 The signs of pain
Pain and discomfort has many causes and it can manifest itself as a physical, psychological or emotional problem.
Signs and symptoms of pain and discomfort can be many and varied, including:
General body tension
Verbalising the need for analgesia (pain killers)
Complaining of pain
Restricted movement/reluctance to move
Pointing to/holding the affected part
Swelling/deformity/inflammation
Crying or other signs of distress
Non-verbal signs, e.g. facial expressions, posture, etc.
Agitation/confusion/irritability/fidgeting/nervous habits
Sleeplessness (insomnia), disturbed sleep, restlessness
Depression and/or anxiety
Changes in behaviour – withdrawal or aggression
Signs of fear or reluctance to seek medical advice – verbalising worries about ill health
Light headedness, fainting, nausea or vomiting
37
3.3 Ways to monitor pain
In order to effectively treat pain you must first assess the pain. This is vital, as an inaccurate assessment may lead to inadequate pain management.
Assessment will be done initially when you first encounter the individual, but this must be an on-going process. Observe for changes and take action. Pain may be intensified by other symptoms, such as anxiety, fear, social pain, nausea and vomiting and other physical symptoms (e.g. pyrexia (high temperature/fever)). Distortion of the experience may be due to confusion and/or a toxic state.
Most people will tell you pain occurs in a particular place – location. However, some people may have a generalised feeling of pain or ill-being.
The most accurate and important way of assessing pain is to take a detailed history of the location, intensity, pattern and duration of the pain from the individual themselves.
This can be done by discussion with the client, their loved ones, any professionals involved and by your observation. Remember the best source of information is the client themselves and this must always be the primary source wherever possible.
Location
Talk to the client and carefully ask them where the pain is and whether it is generalised or localised.
Intensity
Establish what the pain feels like to the client. They may describe it as a sharp pain, a nagging pain. You may be able to suggest some words such as throbbing, burning, etc. Discuss the severity and how much it limits the client’s activities of daily living.
Pattern
It is important to find out if the pain has a pattern and if so what form this takes. This will be particularly useful when planning pain control measures.
Ask the client specific questions, such as how long they have had the pain and how often it occurs.
Some people may complain that pain is worse at certain times of the day or they experience pain during or following certain activities, e.g. mobilising, eating, etc.
38
Try and find out if there is anything the client says relieves or reduces the pain and if there are any other troubling symptoms that they are experiencing.
Duration
The length of time the pain lasts and whether it is constant or intermittent will provide important information when planning pain control measures.
Assessing pain and discomfort
Observe the client and identify any changes in their verbal and non-verbal communication. Non-verbal signs are particularly important in people with communication difficulties, e.g. speech, hearing, understanding or insight problems. This may mean they are unable to communicate their pain, discomfort and related stress by speech. Care workers must be aware that some people may not have the ability to communicate their pain or discomfort due to brain injury, disease or mental health problems. This is a particular problem in those people with dementia – who may become agitated, noisy and aggressive, as care professionals fail to recognise pain as the cause. The use of gestures, facial expression and the written word can aid communication.
Discussion with individuals as to their perception of the cause of their pain or discomfort. For those people with communication difficulties discussion may take place with family and friends, and others who know the individual well. This, however, must not be the only assessment but must be taken into consideration with information gathered from other sources.
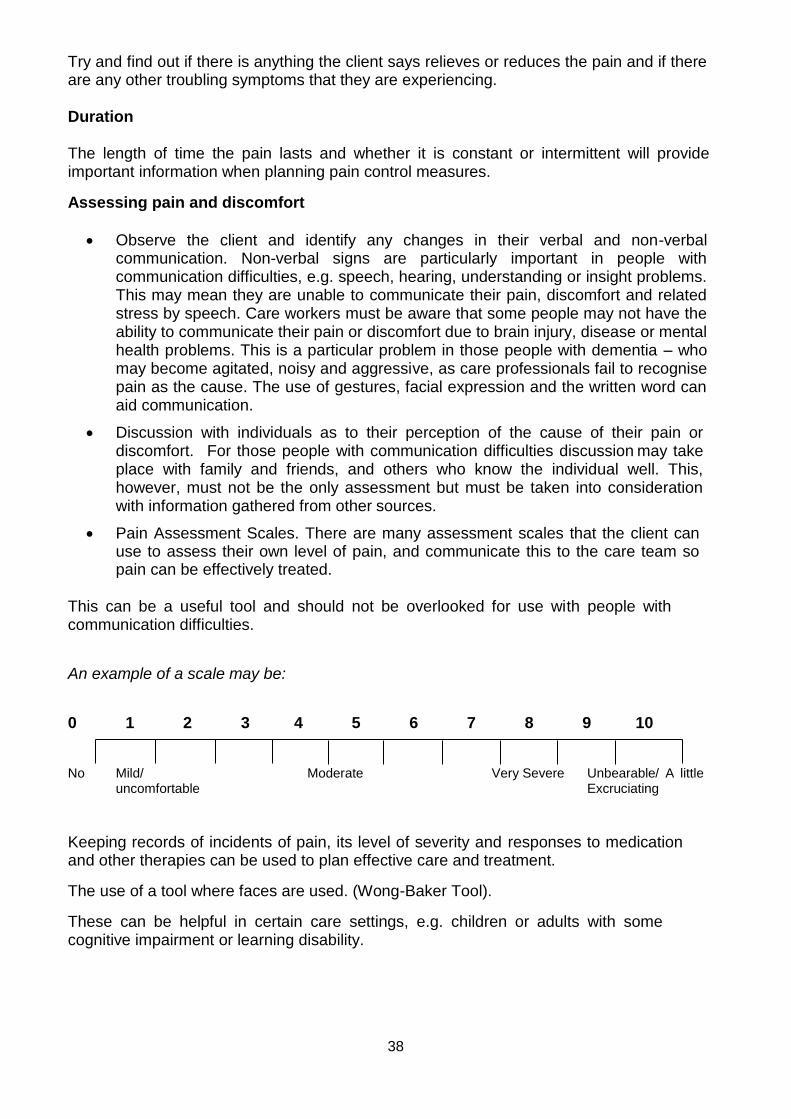
Pain Assessment Scales. There are many assessment scales that the client can use to assess their own level of pain, and communicate this to the care team so pain can be effectively treated.
This can be a useful tool and should not be overlooked for use with people with communication difficulties.
An example of a scale may be:
0 1 2 3 4 5 6 7 8 9 10
No Mild/ Moderate Very Severe Unbearable/ A little uncomfortable Excruciating
Keeping records of incidents of pain, its level of severity and responses to medication and other therapies can be used to plan effective care and treatment.
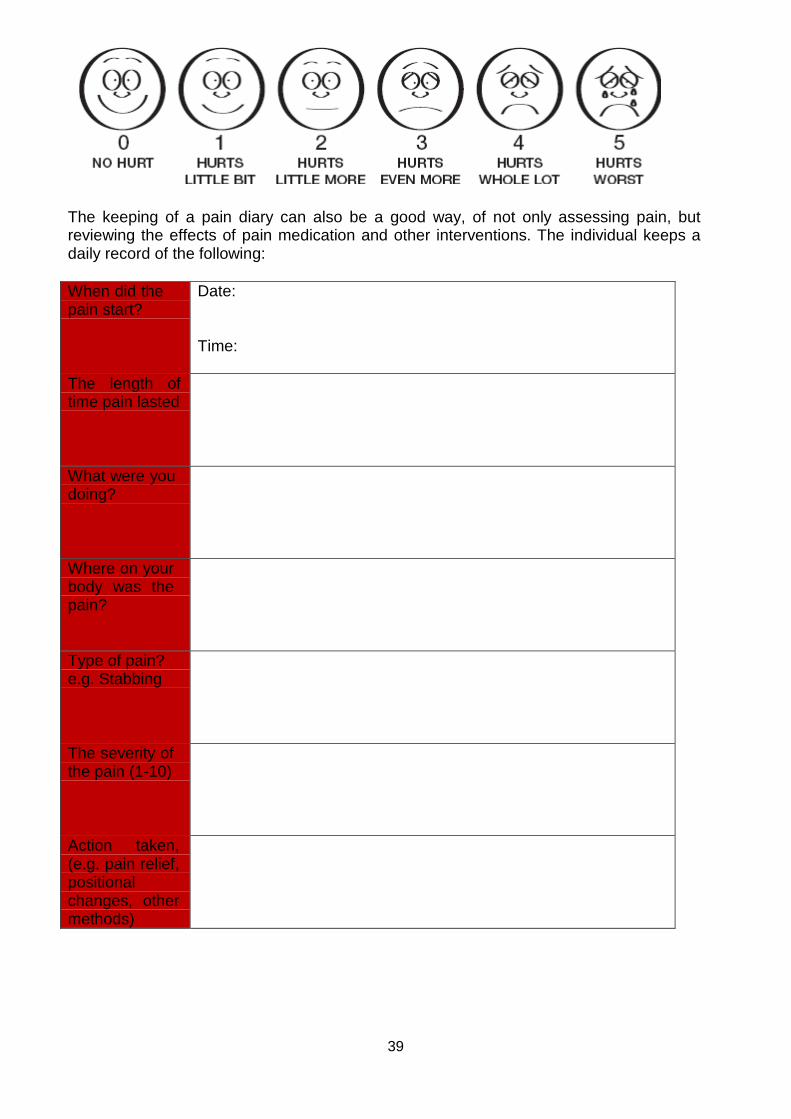
The use of a tool where faces are used. (Wong-Baker Tool).
These can be helpful in certain care settings, e.g. children or adults with some cognitive impairment or learning disability.
39
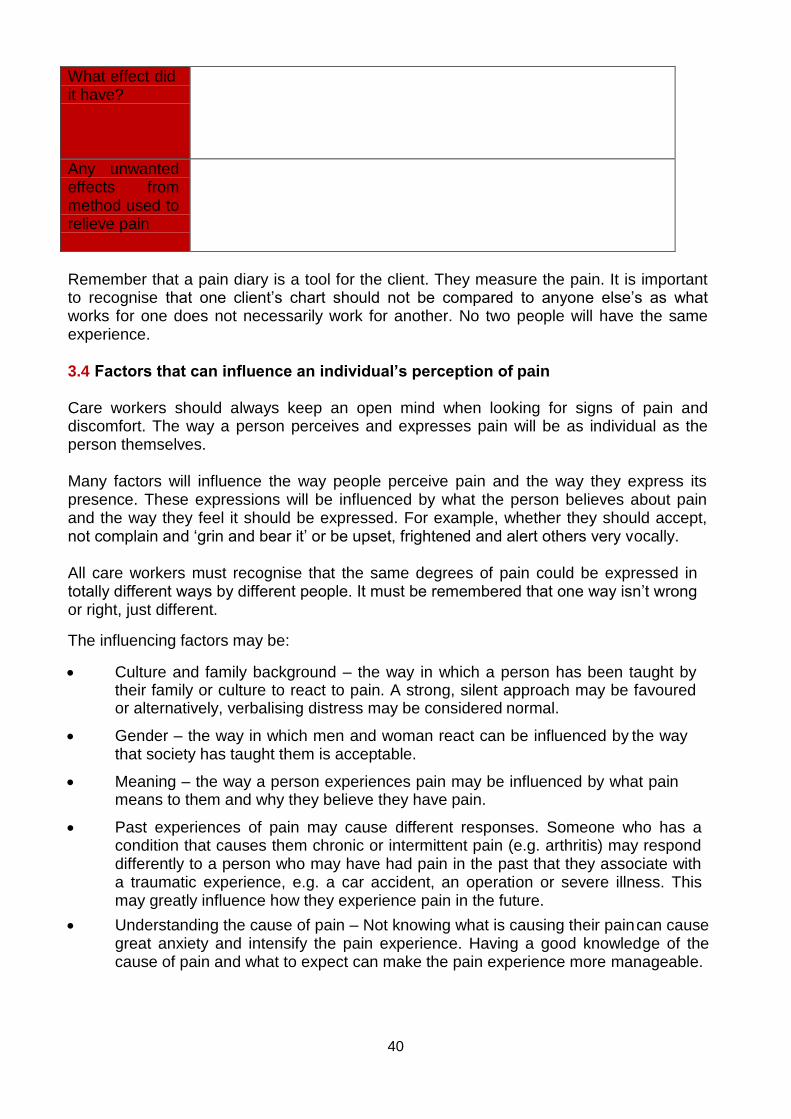
The keeping of a pain diary can also be a good way, of not only assessing pain, but reviewing the effects of pain medication and other interventions. The individual keeps a daily record of the following:
When did the pain start?
Date:
Time:
The length of time pain lasted
What were you doing?
Where on your body was the pain?
Type of pain? e.g. Stabbing
The severity of the pain (1-10)
Action taken, (e.g. pain relief, positional changes, other methods)
40
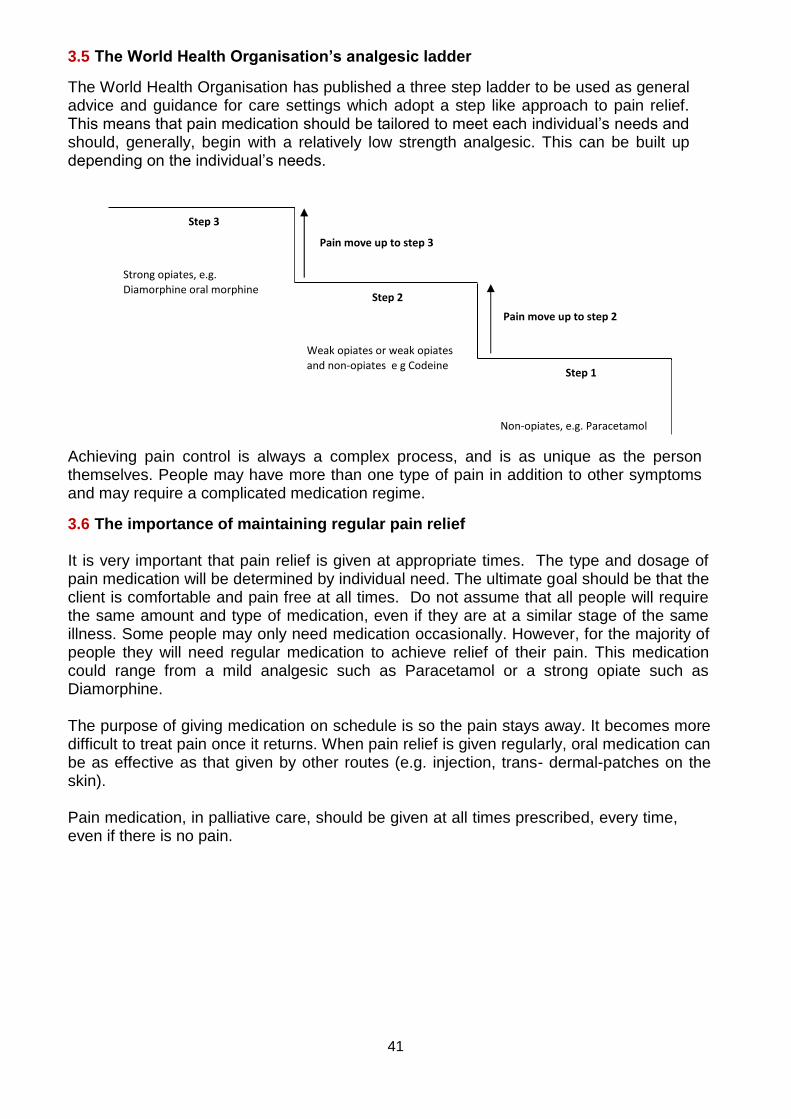
What effect did it have?
Any unwanted effects from method used to relieve pain
Remember that a pain diary is a tool for the client. They measure the pain. It is important to recognise that one client’s chart should not be compared to anyone else’s as what works for one does not necessarily work for another. No two people will have the same experience.
3.4 Factors that can influence an individual’s perception of pain
Care workers should always keep an open mind when looking for signs of pain and discomfort. The way a person perceives and expresses pain will be as individual as the person themselves.
Many factors will influence the way people perceive pain and the way they express its presence. These expressions will be influenced by what the person believes about pain and the way they feel it should be expressed. For example, whether they should accept, not complain and ‘grin and bear it’ or be upset, frightened and alert others very vocally.
All care workers must recognise that the same degrees of pain could be expressed in totally different ways by different people. It must be remembered that one way isn’t wrong or right, just different.
The influencing factors may be:
Culture and family background – the way in which a person has been taught by their family or culture to react to pain. A strong, silent approach may be favoured or alternatively, verbalising distress may be considered normal.
Gender – the way in which men and woman react can be influenced by the way that society has taught them is acceptable.
Meaning – the way a person experiences pain may be influenced by what pain means to them and why they believe they have pain.
Past experiences of pain may cause different responses. Someone who has a condition that causes them chronic or intermittent pain (e.g. arthritis) may respond differently to a person who may have had pain in the past that they associate with a traumatic experience, e.g. a car accident, an operation or severe illness. This may greatly influence how they experience pain in the future.
Understanding the cause of pain – Not knowing what is causing their pain can cause great anxiety and intensify the pain experience. Having a good knowledge of the cause of pain and what to expect can make the pain experience more manageable.
41
3.5 The World Health Organisation’s analgesic ladder
The World Health Organisation has published a three step ladder to be used as general advice and guidance for care settings which adopt a step like approach to pain relief. This means that pain medication should be tailored to meet each individual’s needs and should, generally, begin with a relatively low strength analgesic. This can be built up depending on the individual’s needs.
Achieving pain control is always a complex process, and is as unique as the person themselves. People may have more than one type of pain in addition to other symptoms and may require a complicated medication regime.
3.6 The importance of maintaining regular pain relief
It is very important that pain relief is given at appropriate times. The type and dosage of pain medication will be determined by individual need. The ultimate goal should be that the client is comfortable and pain free at all times. Do not assume that all people will require the same amount and type of medication, even if they are at a similar stage of the same illness. Some people may only need medication occasionally. However, for the majority of people they will need regular medication to achieve relief of their pain. This medication could range from a mild analgesic such as Paracetamol or a strong opiate such as Diamorphine.
The purpose of giving medication on schedule is so the pain stays away. It becomes more difficult to treat pain once it returns. When pain relief is given regularly, oral medication can be as effective as that given by other routes (e.g. injection, trans- dermal-patches on the skin).
Pain medication, in palliative care, should be given at all times prescribed, every time, even if there is no pain.
Step 3
Pain move up to step 3
Strong opiates, e.g.
Diamorphine oral morphine Step 2
Pain move up to step 2
Weak opiates or weak opiates
and non‐opiates e g Codeine Step 1
Non‐opiates, e.g. Paracetamol
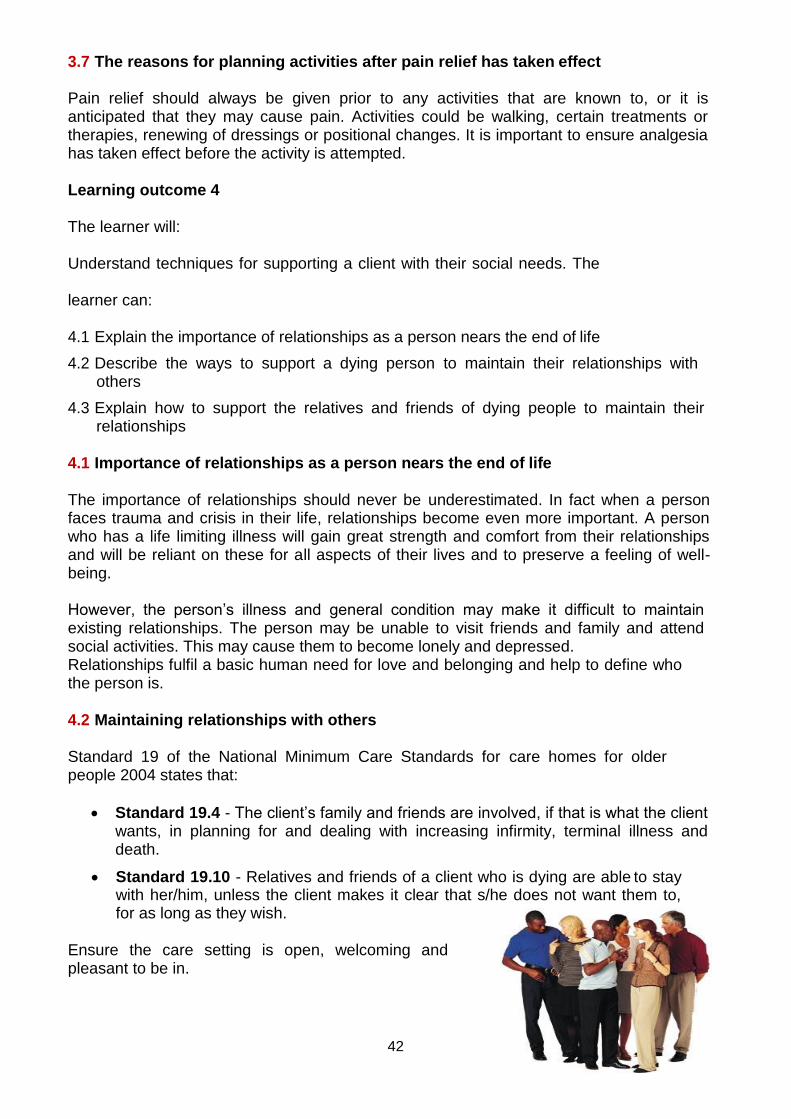
42
3.7 The reasons for planning activities after pain relief has taken effect
Pain relief should always be given prior to any activities that are known to, or it is anticipated that they may cause pain. Activities could be walking, certain treatments or therapies, renewing of dressings or positional changes. It is important to ensure analgesia has taken effect before the activity is attempted.
Learning outcome 4
The learner will:
Understand techniques for supporting a client with their social needs. The
learner can:
4.1 Explain the importance of relationships as a person nears the end of life
4.2 Describe the ways to support a dying person to maintain their relationships with others
4.3 Explain how to support the relatives and friends of dying people to maintain their relationships
4.1 Importance of relationships as a person nears the end of life
The importance of relationships should never be underestimated. In fact when a person faces trauma and crisis in their life, relationships become even more important. A person who has a life limiting illness will gain great strength and comfort from their relationships and will be reliant on these for all aspects of their lives and to preserve a feeling of well-being.
However, the person’s illness and general condition may make it difficult to maintain existing relationships. The person may be unable to visit friends and family and attend social activities. This may cause them to become lonely and depressed. Relationships fulfil a basic human need for love and belonging and help to define who the person is.
4.2 Maintaining relationships with others
Standard 19 of the National Minimum Care Standards for care homes for older people 2004 states that:
Standard 19.4 - The client’s family and friends are involved, if that is what the client wants, in planning for and dealing with increasing infirmity, terminal illness and death.
Standard 19.10 - Relatives and friends of a client who is dying are able to stay with her/him, unless the client makes it clear that s/he does not want them to, for as long as they wish.
Ensure the care setting is open, welcoming and pleasant to be in.
43
This will apply even if the care setting is the client’s home. Although it is recognised that the client may have more power and control in their home it must be acknowledged that they may still need help to maintain relationships, especially if care professionals are spending a great deal of the time in that person’s home.
Special consideration must be given to the importance of giving time and space to the individual. This should meet with the needs and wishes of that individual. Visits by relatives and friends should be a beneficial experience for the client and measures to avoid exhausting or distressing the individual are essential.
Care workers should observe how long the client can concentrate and how many visitors they can tolerate.
Social networks and support
The importance of key people and social networks should never be underestimated. The support available will have a great influence on the experience of the individual and those who care for them.
Visitors and visiting arrangements
Visiting times and arrangements should be very flexible. Private areas need to be provided and visitors made to feel welcome and valued. The client’s wishes must be respected. This may involve requests for special arrangements, including increasing or limiting visitors and visiting times or refusing visitors altogether.
Maintaining contact
For those clients whose family and friends are unable to visit frequently, due to ill health, disability or distance, maintaining contact is equally important. Assisting a client to make or receive a telephone call, write or read a letter or card or send and receive e-mails (if this is available) is a very important part of your role.
Making journeys and visits
Arrangements may be made for people to visit friends and relatives who are in care homes or hospitals. This will apply whether the client lives in their own home or in a residential setting. You may be asked to accompany a client and it is important that you understand your responsibilities before and during the journey and visit.
Many people in a residential setting (e.g. hospice, hospital or care home) have partners. Privacy should be provided without interruption. Respect should be given for intimacy and confidentiality maintained. Partners should be involved in the life of the care setting, as should members of the community and other relatives and friends.
44
Forming new relationships
It is very important that people who are dying form new relationships. They need to trust the health care professionals who treat them so they can benefit most from their support.
When a person is admitted to a hospice or care home it will be helpful to them to form relationships with other residents.
This will give the client an interest, company and support, as they realise they are not alone and others may have similar difficulties and problems. In some instances they may find it easier to talk to someone else who has first-hand experience of what they are going through and can understand.
As a care worker you can facilitate this by creating opportunities for people to meet and socialise. Find out whether people have similar interests and background and introduce them; maybe arranging social events, having coffee together, etc. It must be taken into consideration that close friendships will create emotional attachment and a person may be very affected by a friend leaving the care setting or dying. They may need as much support as that person’s family, and this should not be overlooked.
4.3 Supporting relatives and friends to maintain relationships
All aspects of the care sector should ensure they support families to maintain relationships with individuals. This is particularly important in the area of palliative care, where families will need increased support and reassurance for their mixture of emotions.
When an individual is dying, his or her family and friends will also need support and guidance. Communicating with relatives may help them to anticipate the individual’s death. Communicating is not just about talking it is also about listening and showing your understanding to those you are communicating with. Individuals, key people and others must be reassured that you are able to respond openly and honestly to their questions and concerns. People have a right to ask questions and receive honest responses. You must, however, ensure that confidentiality is maintained.
Draw on the knowledge of relatives. They know the client better than anyone and in many cases the relatives have provided care over a period of time. They will understand the needs and wishes of the individual and know that a non-judgemental approach is vital. Remember they are experiencing an emotional roller coaster and may behave in a way that presents challenges to care staff. Do not pass judgement on people’s relationships, treat everyone with respect and do not discriminate.
It is essential that you know where and how to access any information and support you require for yourself, the person who is dying, key people and others. Senior staff, management and other care professionals are excellent sources of information, advice and support. Information should be available within your care organisation.
45
You may need to ask if you are unsure of where and how to access information or if you need advice on the most appropriate information and ways of communicating this to people. Other useful sources may be the local library, nursing/medical publications and the internet. Find out correct details of local support networks. There are many services that support individuals with particular diseases and their families. They may have support groups. Within your care setting you can form a support group amongst relatives and carers. This must be done with the support and input of the care team.
The family and friends should be supported, as far as is possible, in order that they may stay with the dying individual.
There should be facilities for relatives to make hot drinks and obtain a hot meal. Overnight accommodation may need to be arranged and consideration should be given to enable relatives to sleep and rest.
It is important that relatives are not left for long periods on their own with a dying person without regular contact from care staff. They should be shown how to contact staff whenever they need reassurance or assistance.
If appropriate, relatives or carers should be allowed to participate in the care of the individual if they wish. However, if they do not, this should be respected. As discussed previously, if the individual is unresponsive or unconscious, it should be explained to relatives that the individual may still be able to hear them and should be encouraged to talk to the individual.
Family and friends may be anxious about recognising the moment of death, and should be encouraged to call the staff for support if they are worried about any changes in the individual’s condition.
Some relatives may be reluctant to leave the individual’s bedside as they may be afraid of not being there when the individual dies. It is essential that they are fully supported to make their own decisions. They should also be reassured that the individual will not be left alone. It may be useful to offer to sit with the individual whilst relatives or friends go for something to eat or have a rest.
Relatives who are encouraged to leave the bedside against their own wishes could, if the individual dies during their absence, suffer a deep sense of guilt and find this even more difficult to come to terms with. The family and friends of the individual who is dying should be given as much privacy as possible and, if a single room is available, the individual and their relatives should be given the choice as to whether they would like to use it. It must be remembered that the individual at the centre of all this will need rest too, and it must be acknowledged that visitors around the clock could be extremely tiring.
46
Learning outcome 5
The learner will:
Understand how to support a person’s spiritual, religious and cultural needs. The
learner can:
5.1 Distinguish between spirituality and religion
5.2 Identify the things that a person may classify as being spiritually important to them
5.3 Give examples of how to support an individual to meet their religious and/or spiritual needs
5.1 The difference between spirituality and religion
Spirituality is whatever gives a person meaning, value and worth in their life. This may not necessarily be organised religion or God. It is the strength and solace people gain from things that are important to them that give a person a purpose to living. It may be the love of their family, the peace of the countryside or enjoying creating a piece of art.
Even though many people consider spirituality the same as religion they do differ. Religion is a system of faith and worship with a reverence to a power commonly described as ‘god’. Spirituality is much less formal and constitutes anything which provides an individual with some meaning and understanding of life.
5.2 Spiritual importance
The meaning of spirituality will differ for each person and may include:
Religion – the person’s religious faith may be very important and they may gain great strength and comfort from their beliefs. However, some individuals may question their beliefs and this may cause great emotional pain.
The meaning and purpose of one’s life. A person with a life limiting illness may question the meaning of their life, what was their purpose in life and what will happen after they die.
Relationships with other people – The focus of a person’s spirituality may be their relationships, e.g. with their children, parents, partner, etc. They may grieve for the special relationships they leave behind.
Key events – As people near the end of their life they may ‘take stock’ and think about key events in their life. They may obtain great comfort from thinking of what they have achieved and periods of their life that were happy and rewarding. However, they may also dwell on unhappy periods or events and feel guilt, shame, sadness or regret. Some people may have regrets about what they didn’t do, didn’t achieve or opportunities they missed.
47
Cultural, family and religious tradition
The traditions that a person hold dear will have great spiritual significance. They will make the person feel they belong and that they can rely on these. Some people may find it more difficult to be involved in traditions as they become more ill and feel a sense of loss and fear that they will become isolated from their culture, family or religion.
Music and arts
Music and the arts can be an important part of a person’s spirituality, something from which they gain great comfort and peace.
5.3 Meeting religious and/or spiritual needs
Meeting religious needs
The care setting can demonstrate they are meeting a person’s religious needs in a number of ways, such as:
Assessing a person’s religious needs on an individual basis – even though people share a faith they may have very different religious beliefs; there are many Christian denominations, e.g. Catholic, Methodist, Anglican, etc.
Consulting with a person and their family about religious matters, including prayer, diet and routines of personal hygiene.
Respecting and, where necessary, making arrangements for sacred practises
Making arrangements for priests and other religious figures to visit the person if they wish
Reassuring the person that the rites of their religion and culture will be fully respected after their death.
Supporting spiritual and cultural needs
A person’s identity is inextricably tied to their spiritual and cultural beliefs. So it is just as important to meet these needs as it is to meet physical and psychological needs. Recognising each person’s unique individuality is vital. Health care staff have a responsibility to meet the whole care needs of the individual including spiritual and cultural aspects.
This can be achieved in a number of ways including:
Appreciating that everyone has a spiritual dimension – including people who appear to have no religious beliefs and those who don’t openly discuss their spirituality or what gives their lives meaning and purpose. Almost everyone has something that makes life worth living.
Recognising that some people will have a religious and or cultural element to their spirituality

48
Practising active listening
Being mindful of one’s non-verbal messages
Appreciating that people will express their spirituality and possible spiritual pain in different ways
Acknowledging that there may be conflicts within families around spiritual issues.
Cultural needs:
Treat each person as an individual
Learn from the person – ask the person and their families about their culture and specific rituals, beliefs and traditions. Listen to what people say and act on what you learn.
Research the different cultural groups within the health care setting – find out what information is available within your care setting. Speak with managers and colleagues who may be excellent sources of information. Research what local or national associations exist that may supply you with information and give support.
Be sensitive to a person’s past – as this may have an effect on the way the person behaves and reacts to your support. Past experiences of discrimination will affect the way people relate to others and it may be harder to gain that person’s trust.
Understand what values different cultures hold with regard to illness and the administering of care and treatment - the way in which a culture views health professionals’ role and their own responsibilities will determine how willing they are to accept help and treatment from others. Everyone’s culture and society has its own views and attitudes towards illness, death and dying including prejudices and taboos.
The family needs to be reassured that professionals will support not replace their role
Provide clear, understandable information in a form that is user friendly.
Discrimination and equality
It is vital that all individuals are treated equally and are not discriminated against. There may be a number of ways in which a terminally ill person may be discriminated against.
Cultural, religious and personal beliefs
The care worker must show respect for, and fulfil the needs and wishes of individuals in their care, providing these are within your role and competence. It is never acceptable to dismiss someone’s beliefs, or not fulfil a person’s wishes because they are not the same as the beliefs the care worker holds.
49
Age
Great care must be taken not to make certain assumptions about how an elderly person views death and dying. They may be anxious, frightened or angry, and, assuming that they accept their approaching death calmly and peacefully, may result in support being inadequate. Alternatively, care workers may find it more difficult to support a younger person and may not give adequate support and care; they may avoid contact because the care worker feels awkward, uncomfortable and inadequate.
First class care and symptom control should be top priority whatever the age of the person.
Illness and disease
A person should never be discriminated against because of the illness or disease they are suffering from. For example, some care workers may see an alcoholic with advanced liver disease, a heavy smoker with lung cancer or an intravenous drug user suffering from AIDS, as less deserving of care, as they perceive these conditions as self-inflicted. Remember, pain and suffering are the same whatever the cause, and fulfilling your duty of care means treating all people with the same good standards of care.
Any form of discrimination or withholding of rights is completely unacceptable and should be reported immediately and a record made.
Policies and procedures
Your workplace should have policies concerning equality and diversity and cultural and ethnic issues that are applied when caring for the dying. These policies should reflect local and national policies and legislation.
Learning outcome 6 The learner will:
Understand techniques for supporting a person with their psychological and emotional needs.
The learner can:
6.1 Explain how an individual’s priorities and ability to communicate may vary over time
6.2 Describe the fears people commonly experience towards the end of life
6.3 Explain how to support an individual to address their fears
6.4 Describe how to support an individual or others who want to discuss sensitive issues
50
6.1 How an individual’s priorities and ability to communicate may vary over time
There are many factors which influence the individual’s skills, priorities and ability to communicate. These may include:
Physical health
Mental or physical disability
Social circumstances
Personal beliefs and preferences
The ability to understand
Educational experience and opportunities
Culture, race or religion
Language – the ability to speak English
Aspects such as physical and mental health, understanding and social circumstances may vary over time. Any deterioration may affect the person’s ability to communicate.
An individual’s personal beliefs and preferences may alter according to their age and life experiences. For instance, a person may choose to change their religion or abandon religious practices altogether, affecting their priorities.
The ability to speak English, if it is not the person’s first language, may improve with education or deteriorate with factors such as memory impairment.
6.2 The fears people commonly experience towards the end of life
A person who is dying may have many fears. Recognising and acknowledging these will help care workers to support the individual to alleviate these fears. Fears may include:
Fear about pain or physical illness – many people fear they will suffer agonising, untreatable pain. They also may fear what effect the illness will have on their physical well-being and what it will do to their bodies.
Fear of choking or suffocation. This may particularly affect those who have swallowing difficulties and side effects. People may have fears about the side effects, for instance of chemotherapy or controlled drugs such as Diamorphine.
Fears about psychological effects – people may fear they will ‘lose their mind’ and not be able to make decisions or choices.
Fear about losing control – This could refer to emotions, physical functions or aspects of daily living, such as control over finances.
Fear of being a burden to others
51
Fear of separation – This may be fear of being separated from loved ones during their illness or even after death – especially if they have strong religious beliefs.
Fear of dying alone. This can be a particular worry for those who live alone, have ill partners or family who live a long distance away.
Financial worries - They may fear those left behind will not be able to manage financially. People who are still working may find loss of earnings lead to financial worries.
Fears and worries about how dependent children will cope without them
6.3 Supporting an individual to express their fears
Every individual should feel that they have a right to express their feelings and communicate their needs. As a care-worker, you must respond to this in a way that shows you support their rights to this expression. It can be very easy for care workers to take people’s comments personally, feeling they are being criticised, instead of viewing comments as helpful and constructive.
Empathy is the ability to understand the world as it appears to another person, by putting yourself in their position. This is a skill that will help you to understand why people behave in certain ways. It will also enable the person to feel that you can see things from their point of view. This will develop a relationship based on trust and understanding.
Empathy with individuals involves actively listening to what they are saying (both verbally and non-verbally) and reflecting their feelings and what they have said back to them. It will enhance the relationship you have with the person, and the quality of care you deliver.
Due to the nature of palliative care there may be many sensitive issues discussed and fears expressed, not least the issue of death and dying. It is recognised that these can be very difficult issues for care workers and the client themselves to deal with.
People may at times ask difficult questions, e.g. ‘Am I dying?’ The following should be considered:
You can employ the communication techniques already discussed in this unit to make the person feel comfortable and ready to ‘open up’. With questions such as, ‘Am I dying?’ you need to respond with a question such as, ‘What makes you feel this way?’ This will enable you to establish what the person knows and understands about their illness and prognosis and what is happening to them. It is vital that communication between the care team is good. This will enable you to have prior knowledge of the individual.
However do not assume that the person understands or accepts the information they have received.
Use empathy – even though you cannot know exactly what it feels like to be in the position of a dying person you can imagine how you may feel.
52
Do not confuse empathy with sympathy – when a person makes statements about the end of their life do not tell them ‘don’t talk like that’ or ‘you can’t think that way’ this is ‘blocking’ - a way for us to handle emotions we are uncomfortable with. Strong emotions can be difficult to handle, but do not shy away from them. If a person cries or becomes angry allow them to vent their feelings, acknowledge the strong emotions, whilst showing empathy and support.
Be aware of ‘blocking’, as previously discussed – do not block emotions as this will prevent the person from saying what they feel and makes them feel they shouldn’t have said anything. Death and dying should definitely not be a taboo subject in palliative care!
Be honest about your own feelings. Be polite and sensitive, say you don’t feel comfortable discussing a particular issue. You may be able to give a reason for this, e.g. if a person is unable to understand their prognosis and is pressing you for information, or that it is beyond your experience and expertise. You may be able to explain that you need to get a suitably qualified and experienced person to speak to them. Discuss any issues with your care team as a person absorbs information.
Avoid offering misleading reassurances. This can be very tempting, and in some instances, almost automatic. Statements like, ‘Don’t worry, everything will all right’ or ‘You’re going to be fine’ may prevent the person from having the opportunity to talk.
Be prepared to repeat yourself. A person may not take in what they have been told, be shocked, scared and in denial.
Give information consistent with the level of understanding
Always tell the truth. It is very important that you establish your responsibilities with senior colleagues, if a person asks a question such as, ‘Am I going to die?’ The response you give will impact greatly on the person so being prepared and sure of how you should react is essential.
Check what they know about their illness first
Avoid medical jargon. Information should be given in plain English.
Reinforce information by repeating or writing down
Always allow time for individuals to ask questions, and give them the chance to ask more questions when the information has sunk in and they have had time to reflect on exactly what they need to know.
A quiet and private space is important to any significant conversation
If a conversation has to be carried out at the bedside, then closing screens or sitting close to the client can help to create privacy.
It is important that a health care worker accompany any person who is imparting bad news. They are often the person to whom the individual will turn to following the discussion and it is important that they know exactly what has been discussed.
It should always be the decision of the individual as to whether they want relatives or friends to be present.
53
6.4 Supporting individuals or others who want to discuss sensitive issues What
constitutes complex and sensitive information?
Within the context of this unit difficult, complex and sensitive communication refers to information that is likely to be distressing, traumatic, frightening or threatening. It may include information that may pose a risk to the individual or it may have serious implications for the individual and their family and friends, for example the breaking of bad news. It is, however important to keep an open mind as to what bad news constitutes.
When hearing these words many people tend to think of the worst-case scenario, for example informing an individual that he/she has cancer or informing an individual that his or her loved one has died or is going to die. Working in the field of health care we do not always recognise the information that we convey as being bad news, for example, for some a simple blood test may be a terrifying prospect, for others the thought having to use a hoist to be lifted may be extremely daunting.
It is vitally important to understand that although you may not perceive something as being serious or sensitive this does not mean that clients for who you provide care will think the same. To them the issue may be extremely sensitive and this could be even more so if the individual has communication difficulties and does not fully understand what you are trying to convey to them.
Factors that need to be taken into account when communicating complex and sensitive issues
Communicating complex and sensitive issues can be extremely difficult for health care professionals and there are many factors that you should be aware of and many things that you can do to make the communication process as uncomplicated as possible. Communicating and handling sensitive issues requires an appropriate environment, where information is discussed at an appropriate time It requires the care worker to show empathy, through active listening, and honesty is essential in order to gain and maintain trust.
Reaction during and after communication of sensitive issues
Every person is different in the way that they will react to the disclosure of difficult or sensitive information, and to a large extent the individual’s reactions will depend upon the nature of the information that is being communicated. Having an understanding of the types of reactions that individuals may display will help you to understand and support the feelings that a person may go through.
54
The person’s feelings may not be initially apparent, but it is important to observe the individual’s body language in order to gauge their feelings and provide the support that they may need. A person may demonstrate any number of the following reactions:
Fear
Tearfulness
Hyperventilation
Nausea
Bewilderment, confusion, inability to concentrate
Shock
Disbelief
Anger with others and themselves
Guilt
Relief
Distress
It is important that you detect these reactions as they present themselves, to prevent stress becoming distress. By observing a person’s body language, you will be able to gauge how best to support that person. Support may take many forms, from physical presence, the appropriate use of touch and verbal support, to practical interventions and enlisting the support of other professionals and outside agencies.
55
Learning outcome 7
The learner will:
Understand people’s responses to dying. The
learner can:
7.1 Explain the term ‘anticipatory loss’
7.2 Describe the stages of ‘anticipatory grief’ commonly experienced by individuals with a life limiting illness
7.3 Describe how to support the individual throughout each phase of anticipatory grief
7.4 Explain why people with a life limiting illness may become depressed
7.5 Identify the signs and symptoms that might indicate depression
7.1 Anticipatory loss
Anticipatory loss refers to the sense of loss and grief that begins before the actual death of a person.
It is understandable to think that grief only begins after a person dies. This may be so if death is unexpected, but when death is expected the grieving process can begin as soon as a prognosis is given. The word cancer can cause some people to grieve long before any life limiting prognosis is given.
Losses a dying person may experience
A dying person may experience many losses due to advancing illness and physical and psychological effects. These may include:
Loss of control over own life, bodily functions, etc.
Loss of independence
Loss of productivity
Loss of employment
Loss of security
Loss of family role
Loss of work and social role
Loss of community
Loss of future
Loss of hope
Loss of physical, psychological, functional and cognitive abilities
Loss of ability to complete plans
Loss of loved ones
Loss of consistency and predictability
56
Loss of freedom
Loss of home environment
Loss of routine
Loss of hobbies and interests.
7.2 The stages of anticipatory grief
STAGE 1 - Denial and isolation – Disbelief; being unable to accept the prognosis; denying what is happening. Feeling alone and that nobody else feels the way you do.
STAGE 2 - Anger - At the diagnosis, ‘Why me?’ Angry with other people who are not ill; angry with the doctors, nurses, family.
STAGE 3 - Bargaining – People set themselves goals that they hope to live long enough to achieve, e.g. going on a special holiday, seeing their child’s graduation, the birth of a grandchild.
STAGE 4 - Depression – Sadness, misery and grief
STAGE 5 - Acceptance – Accepting the prognosis and making the most of the time left
7.3 Supporting each phase of anticipatory grief
Sometimes individuals know that there is something wrong long before they are told. They may have been in hospital for some time or may have been having extensive tests and examinations. The breaking of the news then confirms what they have suspected all along.
Many people learn that they have an incurable illness from a doctor, in surroundings that are unfamiliar to them. Depending upon your role within your care setting you may be the person who accompanies the doctor as they speak to the person and their loved ones. Having some understanding of the issues surrounding the breaking of bad news may help you in fulfilling this role.
Breaking bad news is one of the most difficult tasks faced by health care professionals.
Supporting those in denial
Remember denial is a normal response. No one wants to believe they are dying. It is a way of protecting themselves, a defence mechanism.
Accept the feelings and do not try to force the individual to face facts – they are simply not ready.
Do not judge the person. They may have extreme ideas and beliefs about failure of care or even mis-diagnosis but this is part of the grieving process and should not be taken personally.
Let the person discuss the same things over and over. This may help them come to terms with their situation. Expect and be prepared for changes in mood and outlook.
57
Ask for the advice of other care professionals if there are difficulties communicating with and between yourself and the person
Allow the person to take their own time and be there to listen, answer questions and comfort in times of distress.
Anger
A person may feel anger for a number of reasons, which may include the losses they have suffered or anticipate. They feel resentment and jealousy – ‘Why me?’ ‘I’m too young.’ ‘Why not the old lady in the bed next to me?’ Anger may stem from feelings that the prognosis would be better if professionals had diagnosed the illness sooner, provided better or more prompt treatment, etc. The following should be considered:
Instead you may feel at times the anger is directed at you. However difficult it is do not take this personally. Look beyond the behaviour and see the distress. Remain calm and caring.
Allow the person to say why they are angry and if you can offer a solution. Make efforts to do so. Tell the person you can accept their angry feelings.
Encourage the person to talk about their feelings. This can be easier said than done, especially if the person is particularly hostile to your approaches and offers of support. Ensure you listen. Ask the person to tell you how they feel and then let them talk, cry or shout.
Do not be tempted to avoid a person in this stage of grief. This will only make them feel lonely and isolated and will fuel their anger as they become resentful of the lack of attention and contact.
Try to diffuse anger by giving the person your time even if initially they simply direct their anger at you.
They will eventually trust and form a bond with you, talk more and diffuse their anger.
Be patient – a ‘demanding’ person may be a distressed, lonely, frightened person.
Show the person empathy and try to find out if the anger is triggered by anything in particular.
Ask people to think of times when they had to face difficult situations and reflect on how they dealt with these. They may remember what strategies they used to help them through these difficulties. Always ensure the person is given choice and they are encouraged to maintain their independence. People may become angry if they are not allowed to do things themselves and are not in control. Once they feel they are able to be independent and are able to choose and are in control they may feel calmer and their anger will reduce.
Supporting those in the bargaining phase
Providing the person’s hope and goals are realistic and achievable they should be encouraged. Even though the person is dying they can still hope. This will give the person something positive to focus on and aim for. Bear this in mind that these hopes and goals may change as the person’s illness progresses. Spend time discussing with the person how they plan to achieve these goals and offer help and support where this is required.
58
For example, arranging for a lady to choose a knitting pattern and yarn for a garment for an expected grandchild will help her achieve her goal and give her purpose and hope in her life.
Always ensure that you report and make accurate records of your discussions so the rest of the care team is aware of the individual’s goals.
7.4 Why people with a life limiting illness may become depressed
It is understandable why depression occurs amongst people who are dying. Depression can also affect their loved ones. There may be reasons why a person may become depressed.
In addition to the loss of life itself, the reasons may include a sense of helplessness and dependency, regret over ‘missed opportunities’, physical pain and discomfort, the side-effects of treatment, disfigurement and so on.
Supporting depression
Depression may at times be overlooked or treated as something inevitable. Even if the latter is so, depression is an illness that will add to the person’s ‘total pain’ and therefore requires treatment.
Remember depression is more than just feeling fed up or miserable.
Spend time listening to the person, empathise with them and encourage them to open up to you. Try to discover what fears and anxieties they have. The person may wish to discuss ways in which they can manage their depression.
Setting small goals suggested by the individual may bring back some hope and sense of purpose.
Always report and document these conversations as it is important that a definite diagnosis of depression is reached so the person can receive appropriate treatment. This may include counselling and medication. Careful monitoring should take place and any voiced suicidal thoughts should be taken very seriously and advice sought immediately.
Acceptance
Although the person has reached this stage they still need support. They may need help to make visits or carry out final wishes. Although it is a time of peace it may take place late in the illness when the person feels very weak and tired. They may appear detached and isolated to loved ones who may feel they are being rejected.
Care workers should support relatives and help them to understand the person’s behaviour. It will be a great comfort to know that their loved one has found peace. The stages of anticipatory grief are the same for loved ones.
However, it must be recognised that they may not reach each stage at the same time as the person who is dying. In fact they may not move to acceptance in the person’s life time and be unable to move from one of the earlier stages, e.g. denial or anger.
59
Care workers must be aware of this as it may affect the loved one’s behaviours both before and after the person’s death.
7.5 Signs and symptoms of depression
Low mood Reduced energy
Loss of interest Disturbed sleep
Reduction in concentration Alteration in appetite
Indecisiveness Weight change
Feelings of worthlessness and guilt Reduced sex drive
Hopelessness and pessimism Loss of interest in their Appearance
Suicidal thoughts and acts Lack of motivation





























