Embed Size (px)
Citation preview
UNIT 3
Introduction to health, development and Primary Health Care
Welcome to Unit 3!
So far we have analysed the causes of ill-health and concluded that in order to effectively and sustainably address health problems we need to not only address the physical/biological causes but also the underlying socio-economic, cultural and political root causes so as to make a lasting impact on the health of nations. In this unit we will assess the impact of colonialism, industrial capitalism, monopoly capitalism and imperialism on underdeveloped countries. Most people believe that the negative effects far outweigh the benefits. The results were underdevelopment, increased poverty, a system of dominant and dominated economies, as well as widening social inequality between groups of people based on class, race and gender.
Study sessions
There are two Study Sessions in Unit 3:
Study Session 1 The impact of colonialism, capitalism and underdevelopment on health care
Study Session 2 The Declaration of Alma Ata and the Primary Health Care Approach
Intended learning outcomes
By the end of this session, you should be able to:
Public Health Outcomes
Discuss how colonialism, capitalism and underdevelopment have impacted on Africa
Explore how development impacts on the health status of the population
Describe the origins, evolution and main features of Primary Health Care (particularly Comprehensive Primary Health Care)
Academic Learning Outcomes
Take notes Compare information in texts Interpret, compare and draw
diagrams to represent information Read critically, read for a purpose,
identify key points, classify and summarise information
Work out the meaning of terms Draw conclusions from texts
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
117
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
118
Unit 3 – Study Session 1 The impact of colonialism, capitalism and underdevelopment on health care Introduction
In the first study session of Unit 3, we focus on events that took place in Britain during the 19th century with the growth of capitalism and industrialisation. We examine the effects on the pattern of disease and death, and how Britain managed to improve the health of the people through the distribution of some of the resources created by the new capitalist system – a system based significantly on colonial exploitation. Ironically, these processes contributed to the unequal development of countries of the North and South, and a system of dominant and dominated economies. Historically, a more equitable distribution of power and resources nationally and internationally has been achieved through various forms of popular struggle.
Session contents
1 Learning outcomes of this session2 Readings and references3 Capitalism and colonialism 4 A brief history of colonialism and underdevelopment5 How colonialism impacted on health systems6 The evolution of health policies in underdeveloped nations.7 Community-based approaches and national health systems8 Session summary
Timing of this session
There are two readings for this session and five tasks. It should take you about 5 hours to complete.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
119

1 LEARNING OUTCOMES OF THIS SESSION
By the end of this session, you should be able to:
Public Health Outcomes
Discuss how colonialism and capitalism impacted on development.
Discuss how the legacy of colonialism and capitalism impacts on health care in Africa
Compare health services and expenditure in developed and underdeveloped countries
Explain the inequitable distribution of health care resources and measures taken to address this
Explain the basic needs approach
Academic outcomes
Preview texts Take notes Compare information in texts Interpret, compare and draw
diagrams to represent information Read critically, read for a purpose,
identify key points, classify and summarise information
Work out the meaning of terms Draw conclusions from texts
2 READINGS AND REFERENCES
The two readings for this Study Session are listed below. You will be directed to them in the course of the Study Session.
Author/s Reference detailsWerner, D. & Sanders, D.
(1997). Ch 2 - The Historical Failures and Accomplishments of the Western Medical Model in the Third World. In Questioning the Solution: The Politics of Primary Health Care and Child Survival. Palo Alto: HealthWrights: 13 -17.
Sanders, D & Carver R.
(1985). Ch 3 - Health, Population and Underdevelopment. In The Struggle for Health. London: Macmillan: 54-70.
3 CAPITALISM AND COLONIALISM
In preparation for the main readings in this session, clarify your understanding of the concept of capitalism.
TASK 1 – Clarify concepts
1. On a mind-map, brainstorm as many key words as you can think of to do with capitalism.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
120
FEEDBACKCapitalism is an economic system in which private owners control the means of production, including industrial, agricultural and financial resources, with the aim of making a profit.
In history, capitalism has surfaced in different forms– merchant capitalism, industrial capitalism and monopoly capitalism.
Merchant capitalismMerchant capitalism started in the 16th century when European traders travelled to the Middle East, the Far East and Africa to obtain spices, precious metal and ivory. They soon also began to trade cloth, guns, beads and other goods for slaves, who were shipped and sold in the East Coast of South America, the Caribbean Islands and the southern parts of what is now the United States of America. These slaves worked on plantations producing cotton, sugar and tobacco. These raw materials were taken back to Britain and sold at a vast profit. Some of the traders later invested their profit in industrial production and coal mining in Britain at the time of the ‘Industrial Revolution’. The growth of industry became known as Industrial capitalism.
Industrial capitalismIndustrial capitalism is based on the private ownership of machines, factories, industries and the employment of wage earners. The capitalist invests in capital, such as land, raw materials, machinery and labour, to produce goods that will be distributed and sold at a profit. In its pure form, industrial capitalism is based on the principle of ‘free competition’, whereby a large number of producers compete with each other to produce, buy and sell goods or services in the market. The market operates according to the laws of supply and demand, which regulates the supply and price of goods and services. Put very simply, when there is more produced or available than can be sold, the price falls. Conversely, when there is not enough produced to meet the demand, there is a shortage, and so the price rises.
Monopoly capitalismWhen large companies dominate national or international markets this is called monopoly capitalism. These companies are referred to as ‘conglomerates’, ‘transnationals’ (TNCs) or ‘multinationals’ – the latter two operating in and across many countries. When giant producers have no more room to expand in their own national markets, they set up production in other parts of the word, to export their capital and to conquer new markets for their finished goods. Together, TNCs control most of world trade. They have no particular commitment to the countries in which they operate, and their main commitment is to making a profit, using the available resources and labour. Although they create jobs in these countries, they strive to keep wages as low as possible. TNCs sometimes have enormous power and leverage over the governments of these countries.
monopolythe complete possession or control of something by one group or single producerconglomeratea large company that owns companies in different industrial sectors, such as mining, or manufacturingmulti-nationals/transnationalshuge companies, usually with their headquarters in a First World country, and factories, mines and offices in developing counties
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
121
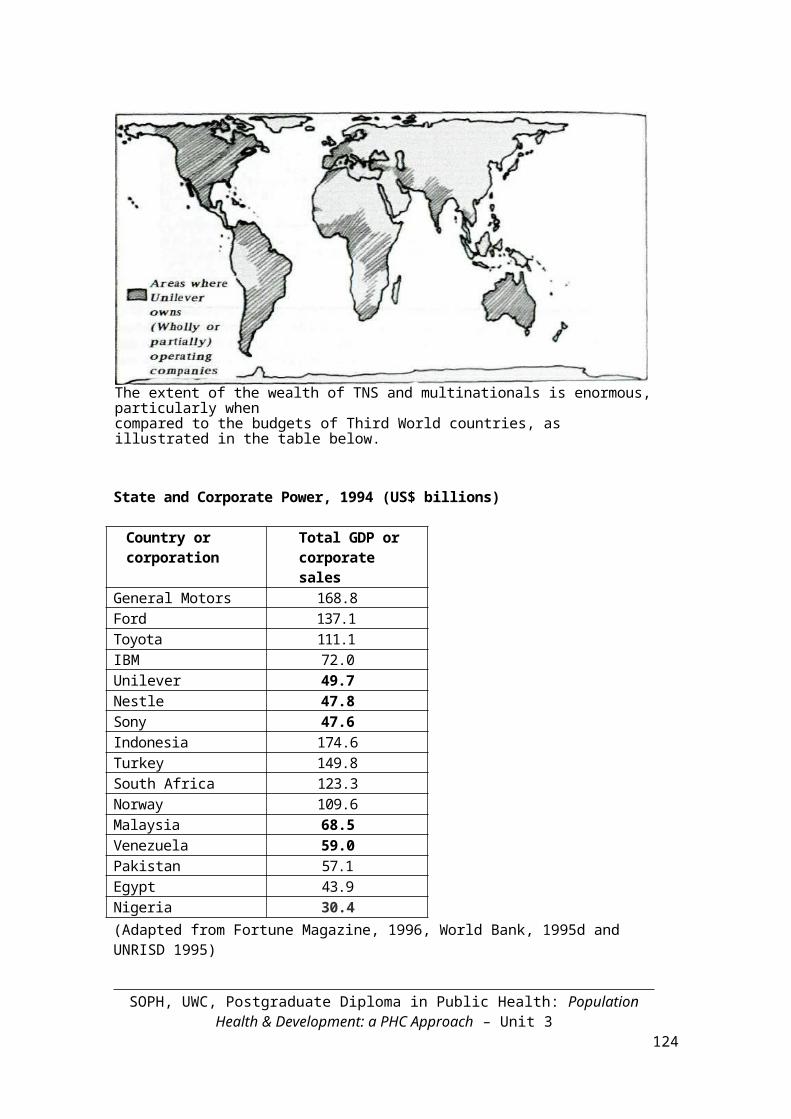
The map below shows the extent of the operations worldwide of the transnational Unilever.
The extent of the wealth of TNS and multinationals is enormous, particularly whencompared to the budgets of Third World countries, as illustrated in the table below.
State and Corporate Power, 1994 (US$ billions)
Country or corporation
Total GDP or corporate sales
General Motors 168.8Ford 137.1Toyota 111.1IBM 72.0Unilever 49.7Nestle 47.8Sony 47.6Indonesia 174.6Turkey 149.8South Africa 123.3Norway 109.6Malaysia 68.5Venezuela 59.0Pakistan 57.1Egypt 43.9Nigeria 30.4(Adapted from Fortune Magazine, 1996, World Bank, 1995d and UNRISD 1995)
Colonial domination of large parts of the world was one result of the growth of monopoly capitalism at the end of the 19th Century. During this period, countries from the North conquered territories in the South, exploited their wealth, exported capital to them, and established new industries. We now take a closer look at colonial domination and how it impacted on the social conditions, health and health care of the colonised people.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
122
4 A BRIEF HISTORY OF COLONIALISM AND UNDERDEVELOPMENT
TASK 2 – Check your knowledge of colonialism
1. What does colonialism mean? What was its purpose?
2. Who were the colonisers? Which continents and countries did they colonise? Jot down your ideas.
FEEDBACK
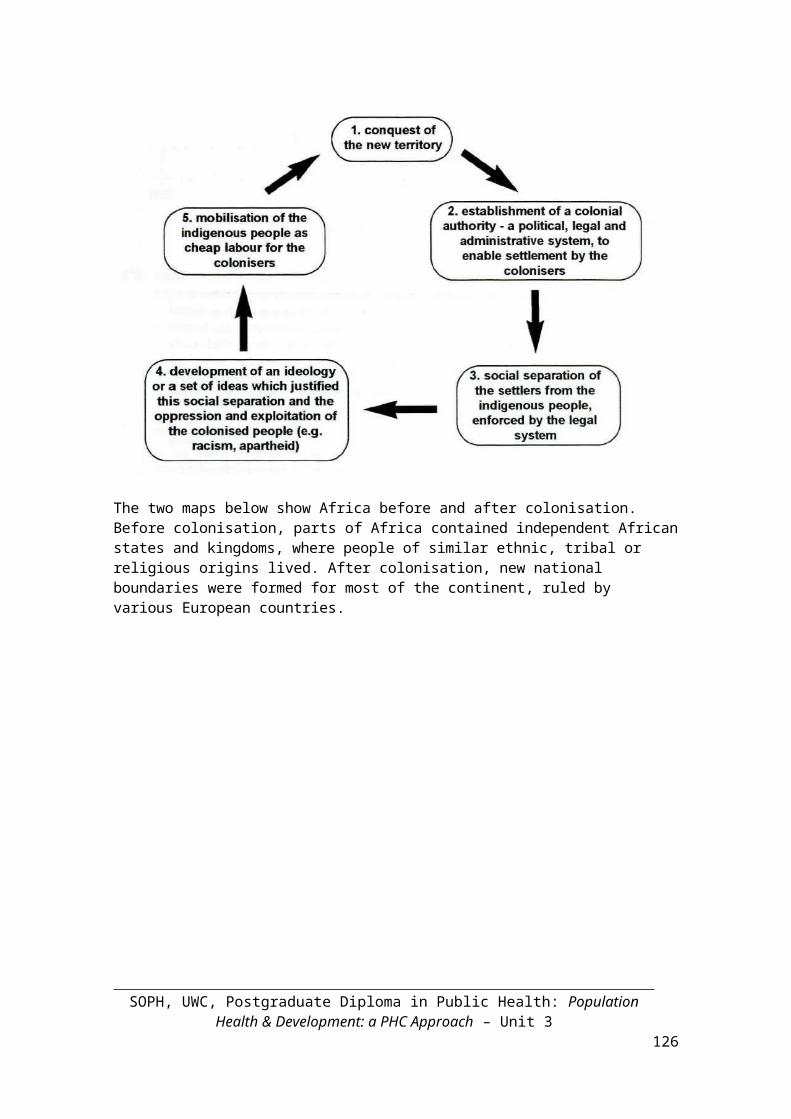
Colonialism is the imposition of the power of one state over the territories of another, (often through military conquest) for political or economic ends. Early colonialism refers to the period during the 16th century when Latin America was colonised by Spain and Portugal. However, the main period of colonial expansion was in the late 19th – 20th centuries and is known as the ‘scramble for Africa’. During this period, European missionaries, explorers and traders came to Africa. They soon realised the potential wealth in Africa and saw African countries as a source of cheap, raw materials and an outlet for the sale of manufactured goods from Europe. Thus, colonialism was geared towards serving the interests of European industrial capitalism. Although there was extensive resistance from Africans, by 1900, the whole continent was divided up and new national and political boundaries were formed, ruled by various European countries.
The process of colonisation usually happened as follows:
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
123
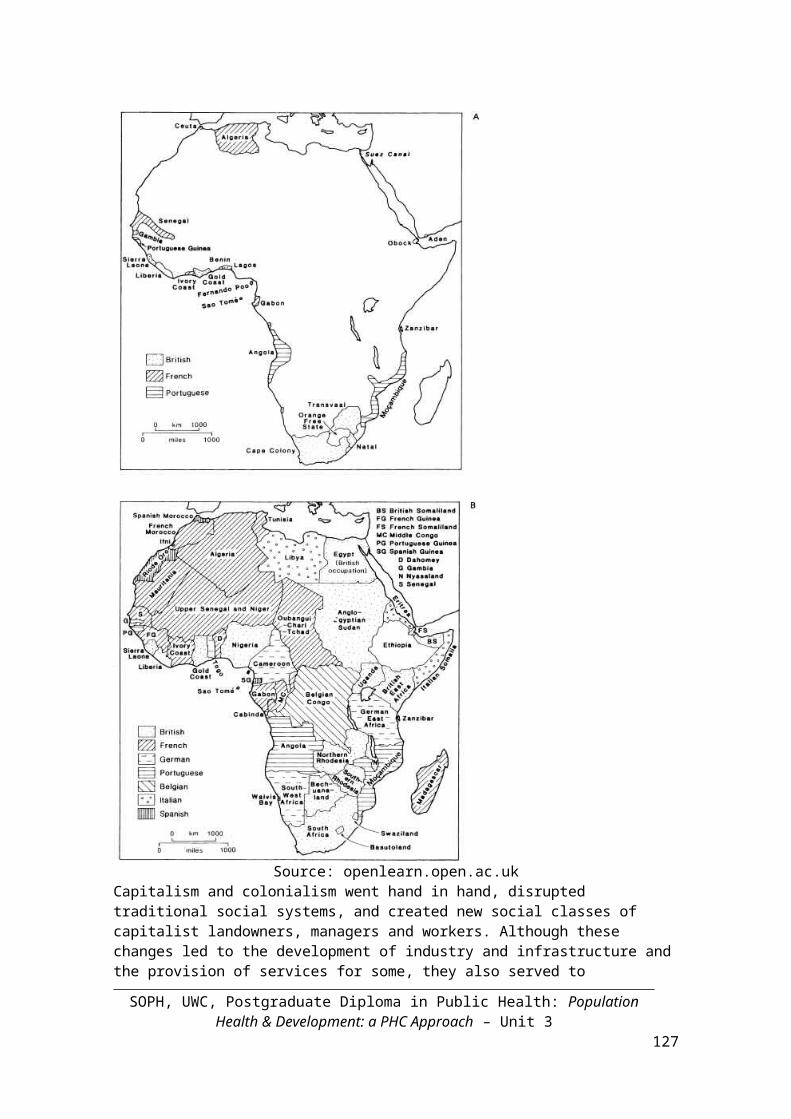
The two maps below show Africa before and after colonisation. Before colonisation, parts of Africa contained independent African states and kingdoms, where people of similar ethnic, tribal or religious origins lived. After colonisation, new national boundaries were formed for most of the continent, ruled by various European countries.
Source: openlearn.open.ac.uk
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
124
Capitalism and colonialism went hand in hand, disrupted traditional social systems, and created new social classes of capitalist landowners, managers and workers. Although these changes led to the development of industry and infrastructure and the provision of services for some, they also served to exacerbate social inequality between groups of people, based on class and race.
Read this oral history account of colonisation in Tanzania.
Tanzania: Colonialism and capitalism
My name is Shantsi and I live in Tanzania. This story was passed on to me by my grandfather. It was told to him by his father who was a young man during the 1880s when the colonists arrived.
When the whites first came to our country, they came on huge boats made of iron. We Africans had never seen this before. At first we were curious to meet these strange white people, but soon we started to hate them. The whites changed all our traditional ways of living. They forced us to grow crops which we could not eat, like cotton. They needed these crops in their own country. They turned our chiefs into overseers or supervisors and made them whip us if we didn’t plant the white man’s crops. Many families died of hunger because they weren’t allowed to use their own land to grow food.
The white missionaries told our women to cover their bodies instead of wearing traditional clothing. They changed our beliefs and forced us to become Christians. We lost our land, our cattle and our youth, who went to work on the mines and in the new towns. Many never came back.
(Adapted from ASECA, Development in Africa, Sached Trust, 1995: 3)
Colonisation in Tanzania did very little to develop the country. Traditional social, political and economic life was totally disrupted. People died resisting colonialism, some died from hunger, and others provided cheap labour for European-owned industries. With little infrastructure and an economy built upon cash crops such as cotton, Tanzania was poor and underdeveloped when independence came.
Most African countries achieved political independence during the 1950s and 1960s. The last countries to gain independence were Zimbabwe, Namibia and South Africa. Although politically independent, most African countries did not achieve economic independence. Some countries, such as Nigeria, inherited huge political problems that have crippled progress and development. Other countries, such as Tanzania, inherited weak economies and have been unable to develop themselves.
The poverty and underdevelopment experienced by post-independent countries, can be partly be explained by historical processes around their economic and political exploitation through colonialism and capitalism. However, politically independent countries remain poor and underdeveloped today and are particularly vulnerable to other forms of economic domination. Can you think of some ways in which these countries continue to be dominated economically today? Read this extract about Tanzania after independence.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
125
Tanzania – Post-independence
After independence, Tanzania chose to follow a socialist path of development and self-reliance. This was difficult. Although Tanzania restricted investment by foreign countries, the government was forced to enter into agreements with some companies, in order to develop Tanzania’s infrastructure, which in turn would support the growth of trade and industry.
Here are two examples of what happened:Britain offered to build a highway in Tanzania for US$110 million. Of this, only $10 million was spent in Tanzania. The rest of the funding was paid to British firms to plan and build the road. Only eight Tanzanians were involved in building the road.
Tanzania asked a Canadian international development agency to build a new bread factory in Tanzania. The construction cost Tanzania much more than they had estimated. Only 60 Tanzanians were employed on this project. Canadian machinery was used to build the factory, which meant that when it broke down, the Tanzanians had to pay the Canadian company to fix it.
(Adapted from ASCA, Development in Africa, Sached Trust, 1995: 46.)
You can see from this extract that Tanzania had to depend on aid from the developed world in order to build the infrastructure it needed. However, the aid really benefited the developed countries more than Tanzania. So, as during colonialism, the developed world continued to profit from the underdeveloped world, while the underdeveloped world lacked power to develop itself. Many African countries found themselves in the same position as Tanzania. For example, they depended on loans from organisation like the World Bank, in order to develop their countries. However, these loans came with conditions that had negative consequences. (For more information on the negative consequences of these loans refer to IPH, Unit 3, Study Session 3.)
Political independence had not solved the economic problems of the Third World countries. In fact, Third World countries have remained underdeveloped, and in some cases have grown even poorer as a result of ongoing exploitation and domination by more powerful First World countries. Sometimes this is termed ‘neo-colonialism’. New forms of exploitation and dominance operate in the global world context today.
5 HOW COLONIALISM IMPACTED ON HEALTH CARE
The readings that follow provide an overview of how broader social and economic developments in different periods impacted on the health of people, and the health policies and health care approaches that were adopted in the countries of the South. The first reading brings together and summarises many of the ideas discussed in this session so far. It also provides useful examples and illustrations of these ideas. The second readings provides an insight into the underdevelopment of the South, the influence of the Western medical model, and the eventual rethinking of health care
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
126
strategies with a focus on meeting the basic needs of people and addressing the social determinants of poor health.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
127
TASK 3 – Preview the text
READINGS
Sanders, D. & Carver R. (1985). (1985). Ch 3 - Health, Population and Underdevelopment. In The Struggle for Health. London: Macmillan: 54-70. Werner, D. & Sanders, D. (1997). Ch 2 - The Historical Failures and Accomplishments of the Western Medical Model in the Third World. In Questioning the Solution: The Politics of Primary Health Care and Child Survival. Palo Alto: HealthWrights: 13-17.
1. Quickly preview the whole of chapter 3 of the first reading (Sanders & Carver, 1985). Then read it carefully and make your own notes.
2. Preview the second reading (Werner & Sanders, 1997) Now read the first paragraph of the chapter. It tells us what the aim or purpose of the chapter is. Use your own words to write down the main aim of the chapter. (Why are we looking at the history of social and economic development in the Third World?)
3. Continue reading Werner & Sanders (1997). Read the first sentence of each paragraph and then answer these questions:
a. Who has directed the development of the undeveloped, less developed or developing colonies in the South since colonial times?
b. What did development planners emphasise in the late 1960s and early 1970s? Why was this trend reversed and what was the consequence?
c. By the end of the colonial period, what was the Third World’s health care approach modelled on? What was the main problem of this model?
d. In the 1970s what new health care strategy emerged? What programme emerged from this and what kind of methods were used?
e. What plan was formulated by health ministers from around the world in 1978?
4. The notes you have made should provide you with a good summary of the main ideas in this second reading. Compare these with the notes you made for the first reading? Are they more or less useful, do you think? Why is this? How can you improve your skills of making notes while reading?
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
128
FEEDBACK
Below is an example of our brief summary of the main ideas in the reading:
The main aim of the chapter is to discuss the changing approaches to health care in the Third World within the larger context of social and economic development at various times.
From colonial times the North has directed the ‘development’ of the undeveloped, less developed or developing colonies in the South.
In the late 1960s and early 1970s development planners emphasised the importance of eliminating poverty through increasing employment opportunities and more equitable income distribution. In other words, the focus was on an economic growth model.
This trend was reversed in the late 1970s due to the economic crisis. The consequence was growing unemployment and the continued inequitable distribution of income.
By the end of the colonial period, the Third World’s health care approach was modelled on that of the industrialised countries, i.e. a Western medical model. The main problem of this model was that it ignored the underlying socio-economic and political causes of health problems.
In the 1970s there was a growing move to a basic needs approach strategy. From this the concept of community-based health care emerged. The Community-Based Health Programmes that emerged used different methods to help people analyse their own health needs and take action to organise around these needs.
In 1978 health ministers from around the world met in Alma Ata to formulate a plan to make health services accessible to all people.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
129
TASK 4 – Read the text in detail
READING
Werner, D. & Sanders, D. (1997). Ch 2 - The Historical Failures and Accomplishments of the Western Medical Model in the Third World. In Questioning the Solution: The Politics of Primary Health Care and Child Survival. Palo Alto: HealthWrights: 13-17.
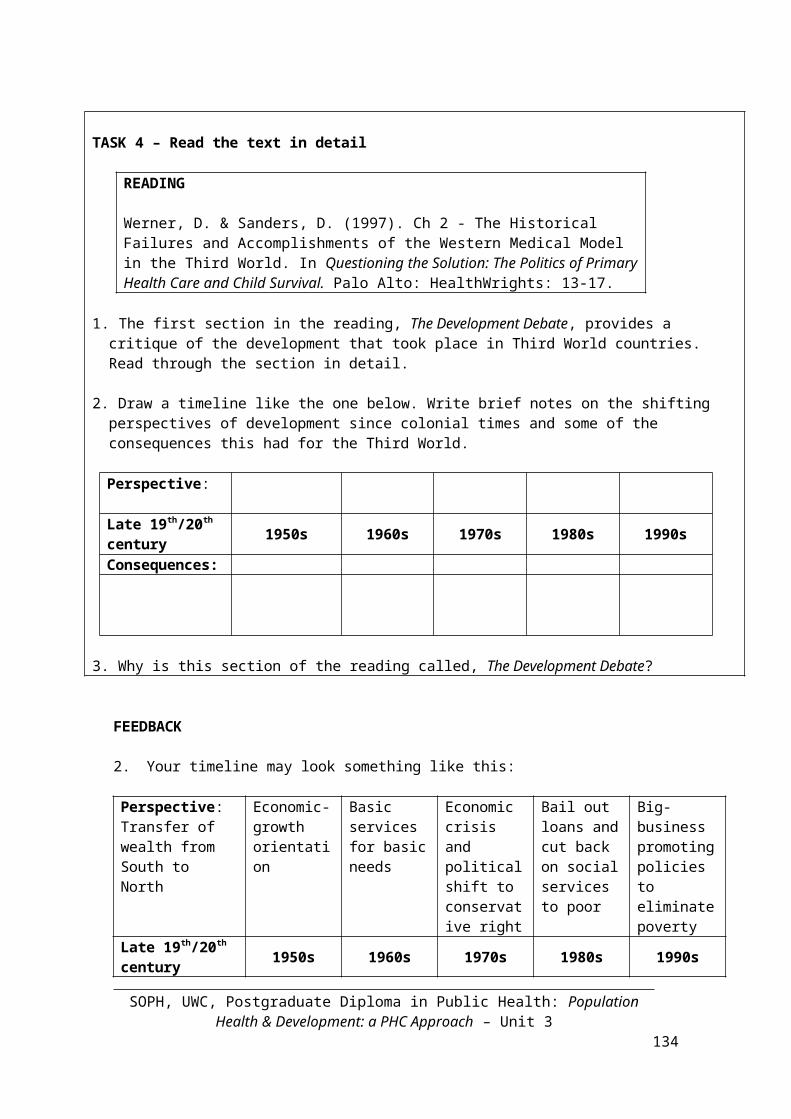
1. The first section in the reading, The Development Debate, provides a critique of the development that took place in Third World countries. Read through the section in detail.
2. Draw a timeline like the one below. Write brief notes on the shifting perspectives of development since colonial times and some of the consequences this had for the Third World.
Perspective:
Late 19th/20th century 1950s 1960s 1970s 1980s 1990sConsequences:
3. Why is this section of the reading called, The Development Debate?
FEEDBACK
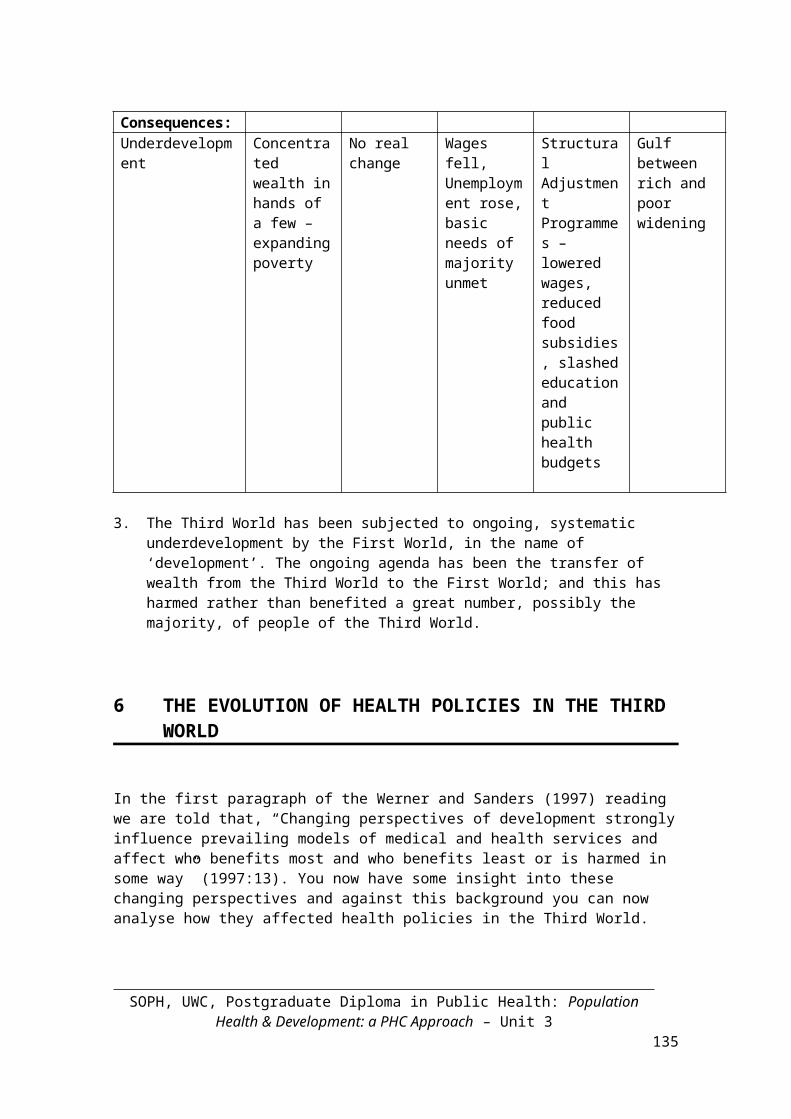
2. Your timeline may look something like this:
Perspective:Transfer of wealth from South to North
Economic-growth orientation
Basic services for basic needs
Economic crisis and political shift to conservative right
Bail out loans and cut back on social services to poor
Big-business promoting policies to eliminate poverty
Late 19th/20th century 1950s 1960s 1970s 1980s 1990s
Consequences:Underdevelopment Concentrated
wealth in hands of a few –expanding poverty
No real change Wages fell,Unemployment rose, basic needs of majority unmet
Structural Adjustment Programmes – lowered wages, reduced food subsidies, slashed education and public health budgets
Gulf between rich and poor widening
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
130
3. The Third World has been subjected to ongoing, systematic underdevelopment by the First World, in the name of ‘development’. The ongoing agenda has been the transfer of wealth from the Third World to the First World; and this has harmed rather than benefited a great number, possibly the majority, of people of the Third World.
6 THE EVOLUTION OF HEALTH POLICIES IN THE THIRD WORLD
In the first paragraph of the Werner and Sanders (1997) reading we are told that, “Changing perspectives of development strongly influence prevailing models of medical and health services and affect who benefits most and who benefits least or is harmed in some way” (1997:13). You now have some insight into these changing perspectives and against this background you can now analyse how they affected health policies in the Third World.
TASK 5 – Plot the development of health policies in Third World countries
READING
Werner, D. & Sanders, D. (1997). Ch 2 - The Historical Failures and Accomplishments of the Western Medical Model in the Third World. In Questioning the Solution: The Politics of Primary Health Care and Child Survival. Palo Alto: HealthWrights: 13-17.
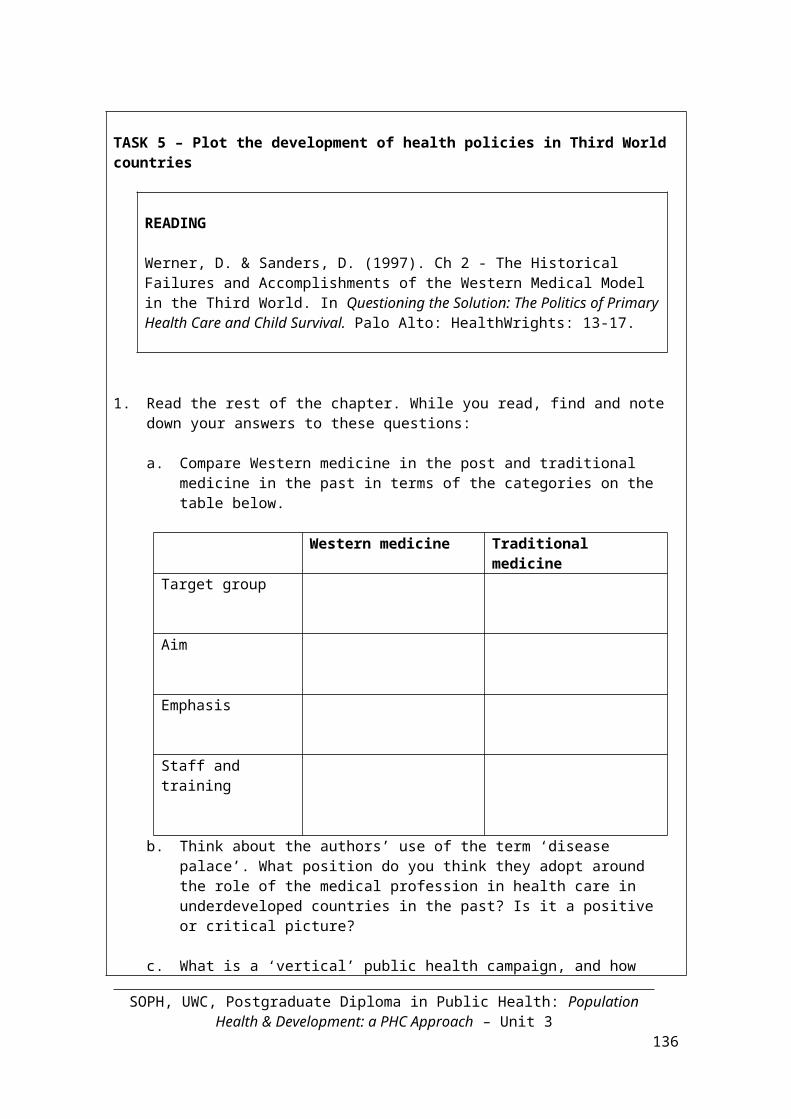
1. Read the rest of the chapter. While you read, find and note down your answers to these questions:
a. Compare Western medicine in the post and traditional medicine in the past in terms of the categories on the table below.
Western medicine Traditional medicine
Target group
Aim
Emphasis
Staff and training
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
131
b. Think about the authors’ use of the term ‘disease palace’. What position do you think they adopt around the role of the medical profession in health care in underdeveloped countries in the past? Is it a positive or critical picture?
c. What is a ‘vertical’ public health campaign, and how effective have they been?
d. What is the basic needs approach? How did it attempt to provide basic services to more people?
e. What is Community-based health care? How did it attempt to provide basic services to more people?
FEEDBACK
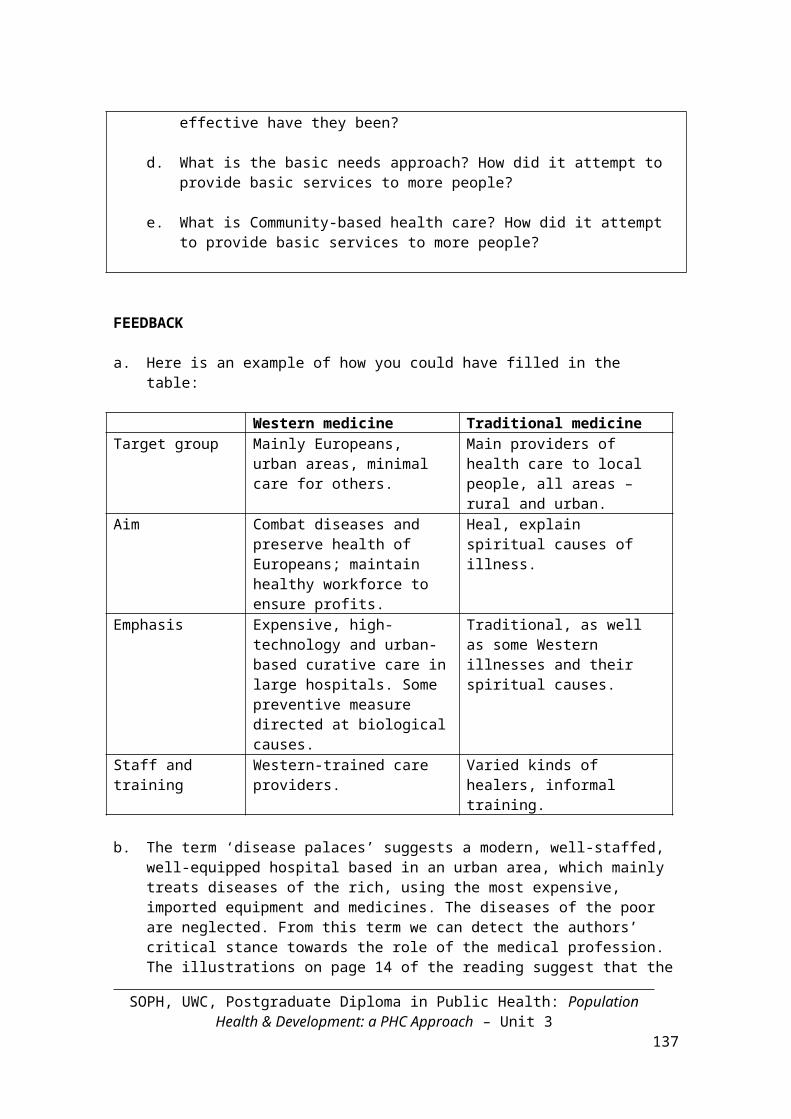
a. Here is an example of how you could have filled in the table:
Western medicine Traditional medicine Target group Mainly Europeans, urban
areas, minimal care for others.Main providers of health care to local people, all areas – rural and urban.
Aim Combat diseases and preserve health of Europeans; maintain healthy workforce to ensure profits.
Heal, explain spiritual causes of illness.
Emphasis Expensive, high-technology and urban-based curative care in large hospitals. Some preventive measure directed at biological causes.
Traditional, as well as some Western illnesses and their spiritual causes.
Staff and training Western-trained care providers.
Varied kinds of healers, informal training.
b. The term ‘disease palaces’ suggests a modern, well-staffed, well-equipped hospital based in an urban area, which mainly treats diseases of the rich, using the most expensive, imported equipment and medicines. The diseases of the poor are neglected. From this term we can detect the authors’ critical stance towards the role of the medical profession. The illustrations on page 14 of the reading suggest that the people who benefited most from these disease palaces were the doctors themselves.
c. Vertical campaigns were preventive campaigns, narrowly aimed at a single disease, such as smallpox or malaria. They were expensive to run and were generally not comprehensive. They were preventive campaigns and often organised under a separate authority, such as the provincial authorities, rather than by the Ministries of Health, which were mainly responsible for hospitals.
d. The basic needs approach was based on the growing understanding that health care was a basic human right and that more effective ways of providing basic
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
132
services to all people needed to be found. Auxiliaries were introduced as a more appropriate category than medical doctors and nurses, particularly in areas where nutritional and communicable diseases were predominant. They were able to deliver relatively simple interventions required to improve the health of the majority of people. However auxiliaries had little attachment or accountability to the communities they served, and many dropped out or migrated up the medical hierarchy.
e. Community-based health care focused on preventive measures, health education and involvement and leadership of members of the community. Community health workers or health promoters were selected from and by their own communities and received training in how to help their community diagnose the underlying causes of poor health and meet their most important health needs. The approach was focused on taking action to reduce poverty and to improve the circumstances in which people lived, and in this way address the major diseases affecting communities.
7 COMMUNITY-BASED APPROACHES AND NATIONAL HEALTH SYSTEMS
One of the reasons why the barefoot doctor programme in China was so effective was that it took health care right into the communities that needed it the most. In addition the programme had the full backing of the central government. In other words, there was a strong political will and commitment on the part of the government to ensuring comprehensive health care for all. (The development of political will on the part of government is extremely important for ensuring that the necessary financial, institutional and human resources are allocated for health development and for a reduction of inequalities.) The results grabbed the attention of other health planners from around the world.
In 1978 health ministers met at Alma-Ata in Kazakhstan, at that time a socialist republic of the USSR, to adopt what was called, the Declaration of Alma Ata, which expressed the need for urgent action by all governments to protect and promote the health of all the people of the world. Health was seen as a socio-economic issue and health care as a basic human right, and the State was seen as being responsible for providing adequate health and social measures. Primary health care was seen as the route to ensure ‘health for all’. The Alma Ata Declaration put health equity on the international political agenda. You will read more about the Alma Ata Declaration and Primary Health Care in the next sessions.
8 SESSION SUMMARY
This session has provided a broad history into the ‘underdevelopment’ and the ongoing high prevalence of ill-health in underdeveloped countries of the South. Through the readings we discussed how the concept of development for most of the 20th century was synonymous with economic growth, rather than human development. We
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
133
discussed the evolution of health policies in the Third World, from the adoption of the Western Medical Model to community-based approaches.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
134
Unit 3 – Study Session 2 The Declaration of Alma Ata and the Primary Health Care Approach
“Too often, in planning strategies to improve health, the people whose lives are most vulnerable have not been consulted. However, the Alma Ata Conference of 1978 was something of an exception. Among its participants were pioneers of community-based health care initiatives from several countries. They emphasized the need, in the pursuit of Health for All, to confront the underlying social, economic and political causes of poverty and poor health. The result was the potentially revolutionary Alma Ata Declaration, which promoted a comprehensive, multi sectoral approach named Primary Health Care. This called for a New Economic Order based on equity and "social justice", to be achieved through strong community participation.”
(David Werner, Health and Equity: Need for a People’s Perspective in the Quest for World Health, 1998)
Introduction
In this study session we focus on health care and the changes that have taken place in recent times. We start with a brief overview of the Declaration of Alma Ata which was drawn up and adopted in 1978, and discuss the principle of the Primary Health Care Approach that it embodies. We then track the implementation of these principles and the four-pronged strategy that it advocated as a holistic response to health care and the factors that determine ill-health.
Session contents
1 Learning outcomes of this session2 Readings and references3 The evolution of the Primary Health Care Approach4 The main features of the Primary Health Care Approach5 Rehabilitative, Curative, Preventive, Promotive6 Session summary
Timing of this session
This session has two readings and three tasks. It should take about three hours to complete.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
135
1 LEARNING OUTCOMES OF THIS SESSION
By the end of this session you should be able to:
Public Health Outcomes
Describe the origins, evolution and main features of the Primary Health Care approach
Explain the terms rehabilitative, curative, preventive and promotive
Describe the implementation of the Primary Health Care Approach since 1978
Academic outcomes
Preview texts Read in detail for meaning Take notes as you read Summarise texts Make comparisons Work out the meaning of concepts
from their root words
2 READINGS AND REFERENCES
You will be referred to the following readings in this session.
Author/s Publication detailsWalt, G. & Vaughan, P.
Walt, G. & Vaughan P. (1981). Introduction. In An introduction to the primary health care approach in developing countries, London: Ross Institute of Tropical Hygiene: 1–12.
Werner, D. & Sanders, D.
(1997). Ch 3 - Alma Ata and the institutionalization of Primary Health Care In Questioning the Solution: The Politics of Primary Health Care and Child Survival. Palo Alto: HealthWrights: 18-22.
2 THE EVOLUTION OF PRIMARY HEALTH CARE
In 1978 health ministers and their advisers from 134 countries from around the world met in the city of Alma Ata in Kazakhstan (then in the USSR) at an International Conference organised by the World Health Organisation (WHO) and UNICEF on Primary Health Care. Their purpose was to develop a plan to achieve: ‘Health for All by the Year 2000’.
The final document adopted by the Conference was the Alma Ata Declaration, which called for, “urgent and effective national and international action to develop and implement primary health care throughout the world and particularly in developing countries.”
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
136
Alma Ata, the capital of Kazakhstan, now called Almaty, was the site of the 1978 WHO/UNICEF conference ‘Health for All by the Year 2000’.
The two readings in this session provide you with a good overview of how primary health care developed historically and what the original approach involved, as set out in the Alma Ata Declaration. Each reading focuses on slightly different principles from the Declaration.
TASK 1 – Read about the history of the Primary Health Care Approach
READING
Walt, G. & Vaughan P. (1981). Introduction. In An introduction to the primary health care approach in developing countries, London: Ross Institute of Tropical Hygiene: 1–12.
1. Preview the above reading: What is the title of the reading? What do you expect it is going to cover? Look at the headings. Skim the first three lines of each numbered section. Notice that each begins with some dates. What does this tell you about the likely content of each of these sections?
2. Read through the text in detail. As you read, underline what you think is really important.
3. Summarise in a few sentences the main purpose of the reading and the main
ideas.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
137
FEEDBACK
This reading gives you an introduction to the Primary Health Care (PHC) Approach. It attempts to define the concept of primary health care and outline the main principles of the approach. The Alma Ata Declaration was a declaration of principles and a broad strategy for implementation of PHC.
To sum up this reading, the evolution of Primary Health Care included: Changing theories of development which demonstrated the impact that
socioeconomic and environmental factors have on health. (Remember you studied this in Unit 2 and saw the results than can be achieved when underdevelopment and social determinants of health are addressed, e.g. the case example of 19th Century England and Wales).
Concern about population growth which later led to support for material and child health services.
A realisation that the Western medical model did not address the social determinants of health.
The reported success of the health achievements that community-based health projects had achieved in China as well as in several other countries. These demonstrated the impact of a comprehensive approach to health and health care.
4 THE RATIONALE AND PRINCIPLES OF THE PRIMARY HEATH CARE APPROACH
The Primary Health Care Approach that was embodied in the Declaration of Alma Ata signalled a shift in attitude about health and health care. No longer was health simply seen as the absence of disease as a result of biomedical interventions; it was now also seen as a result of social determinants which impacted on health. The spirit of the Declaration also broadened the focus of development from economic growth to the development of people and communities. It recognised the basic right to health for each individual and called for an approach that rested on the principle of equitable use of health resources.
The basic principles and requirements of Primary Health Care are:
Universal accessibility: The total coverage of the population with basic, but essential health care, with particular attention being given to the needy, vulnerable groups (equity).
Comprehensive care: An emphasis on disease prevention and health promotion.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
138
Community and individual involvement and self-reliance: Communities should participate actively in the planning, implementation and evaluation of health services.
Intersectoral action for health: Health services should co-ordinate with other sectors involved in development, since progress in health leads to and depends on socio-economic progress.
Appropriate technology and cost-effectiveness in relation to available resources: Health care services should focus on the major health problems, should be affordable, and employ technologies that are locally appropriate as well as acceptable.
The elements or programmes of Primary Health Care as stated in the Alma Ata Declaration are:
The promotion of proper nutrition and adequate supply of safe water and basic sanitation
Maternal and child health care, including family planning
Immunisation against the major infectious diseases
Prevention and control of locally endemic diseases
Appropriate treatment of common diseases and injuries
Health education concerning prevailing health problems and methods of prevention and control.
The table below shows the change in focus, content, organisation and responsibility from Primary Medical Care to Primary Health Care. It was developed for a European audience and hence emphasises doctors (specialists, physicians, general practitioners) who may not be the most numerous or important health personnel in developing countries.
Table 1: From Primary Medical to Primary Health Care
From Primary Medical Care
To Primary Health Care
Focus IllnessCure
Health needsPrevention and care
Contents TreatmentEpisodic curative careSpecific problems
Health promotionContinuous careComprehensive carePerson-centred
Organisation SpecialistsPhysiciansSingle-handed
General practitionersOther personnel groupsTeam
Responsibility Health sector aloneProfessional dominance
Intersectoral collaboration Community participation
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
139
Passive reception Self-responsibility – people are partners in managing their own health and that of their community
The second reading will help you to consolidate your understanding of Primary Health Care and describe developments after Alma Ata.
TASK 2 - Read the Declaration of Alma Ata
READING
Werner, D. & Sanders, D. ((1997). Ch 3 - Alma Ata and the institutionalization of Primary Health Care. In Questioning the Solution: The Politics of Primary Health Care and Child Survival. Palo Alto: HealthWrights: 18-22.
1. Preview the above reading and answer these questions:a. What is the title of the reading? What does institutionalisation mean? b. Look at the headings in the reading. Skim the first three lines of each
section. What do you expect the reading to cover?
2. Read through pages 18–19 of Chapter 3 (up until Resistance to Primary Health Care) and the Declaration of Alma Ata on pages 21–22. As you read, note down the key points. Try to use your own words. Here are some questions to help direct your reading and note-taking:
a. How is health defined in the Declaration?b. What does it mean that health is a fundamental human right? c. What does the Declaration identify as the causes of poverty and poor health
that need to be addressed? d. Who has rights and responsibilities to participate in health care? e. How must governments fulfil their responsibility for the health of their
people?f. How is Primary Health Care (PHC) described in the Declaration? Give some
examples of what it includes. g. Who should be involved in the health team?h. How was it envisaged that health for all people by the year 2000 could be
attained throughout the world?
3. Now read through pages 19-20 of the reading. On a table like the one below, write the five basic principles of PHC in Column 1. In Column 2 write brief notes about the resistance to these principles and the implementation of PHC.
Principles of PHC Resistance1.
2.
3.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
140
4.
5.
FEEDBACK
Question 2:a. Alma Ata’s definition of health was based on the WHO’s definition, that health is
not just the absence of disease, but also includes a state of physical, mental and social well-being.
b. Human rights are rights and freedoms that everyone has, just because they are human. For example, everyone has the right to life. No once can take these rights from us. Health is classified as one of these basic rights, rather than a luxury for a privileged few. Human rights must be respected, protected, promoted and fulfilled.
c. The Declaration emphasises the need to address the underlying social, economic and political causes of poverty and poor health.
d. The Declaration calls for the participation of individuals, families and communities in controlling their own health, being involved in health programmes, and decisions that affect them.
e. Governments must provide adequate and equally accessible health services to all, as well as social measures to ensure the health of their people.
f. PHC was defined as the first (primary) contact people have with the national health system; bringing health care to where people live and work. It is also seen as the first step in the ongoing health care process. The approach to health care addresses the main health problems and health care needs in a community as well as the underlying social determinants of poor health. It calls for a more equitable response to basic health care needs.
g. The health team should include local health workers, doctors, nurses, midwives, auxiliaries, community workers, and traditional healers.
h. All countries needed to cooperate with each other to ensure primary health care for all. This would provide a more equitable distribution and use of the world’s resources.
Principles of PHC Resistance1. Health services must be equally
accessible to all. They must be available to rural as well as urban people.
Social justice agenda and addressing root causes of poor health threatened leaders of many countries.
2. There must be maximum community and individual involvement in health care decisions and self-reliance.
National programmes launched but PHC treated as extension of old top-down approach. Often resistance to true participation by communities. Central control of PHC and weak community participation. Not seen as agents of change.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
141
3. The PHC programmes must provide comprehensive care involving four main components: promotive, preventive, curative and rehabilitative services, with an emphasis on disease prevention and health promotion.
Western medical system remained with emphasis on curative services.
4. The methods and technology used in the health system must be appropriate, easy to use and cost-effective in terms of available resources.
One example was continuing use of nonessential drugs in contrast to PHC ethos of responsible and limited use of medicines.
5. Health must be seen as only part of total care which includes all the other essential requirements. There should be intersectoral collaboration to address the social and environmental determinants of health.
Global health institutions stripped PHC of its comprehensive and transformative potential and reduced it to a narrow, technical approach.
Before ending this session, it is important to clarify some important terms in the four-pronged approach of comprehensive primary health care.
5 REHABILITATIVE, CURATIVE, PREVENTIVE, PROMOTIVE
TASK 3 – Clarify terms
1. Brainstorm what you understand by the terms: rehabilitative, curative, preventive and promotive. Give an example of each term if you can.
2. Which of the four approaches is primarily individually focused, and which is primarily population focused?
FEEDBACK
Your answers may differ but could include the following:
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
142
Rehabilitative comes from the word, ‘rehabilitate’ which means to help someone to live a healthy active life again after some illness. So rehabilitative services are all those services involved in assisting the person to recover from a disease. For example, making sure that the person eats a balanced and healthy diet to help the immune system recover. These services are primarily individually focused.
Curative comes from the word, ‘cure’, which means to treat an illness or condition in some way so that it clears up and goes away. For example, by giving the person medication. These services are primarily individually focused.
Preventive comes from the word, ‘prevent’, which means to stop an illness spreading or infecting someone, before it starts. For example, by ensuring that the person is well nourished and lives a healthy lifestyle. These services are primarily population focused.
Promotive comes from the word, ‘promote’; this means to encourage or persuade people to support or use something. For example, to teach people how to prevent illness through keeping themselves and their environment safe and healthy, or to lobby government for better social services to prevent illness and infection. These services are primarily population focused.
Academic learning skills
Whenever you need to explain a term or concept, look for the root word that the concept comes from. You can usually work out the meaning of the word from its root.
In the comprehensive Primary Health Care Approach, the following four strategies are used together in a holistic way, rather than only one strategy selected and focused on:
1. The rehabilitative approach: Emphasises restoring people with an acute or chronic illness to a state of improved health. For example, exercises to improve chronic backache pain, or nutrition rehabilitation after a severe childhood illness, or in the case of TB, both medical and social rehabilitation may be required. This approach is primarily focused on the individual who is ill.
2. The curative approach: Emphasises the treatment of the biological and psychological causes and symptoms of disease, through the use of medicine and other therapies. For example, the use of Oral Rehydration Therapy (ORT) for children with chronic diarrhoea or the use of antiretrovirals for people living with HIV/AIDS. This approach is also mainly focused on the individual.
3. The preventive approach: Emphasises preventing or avoiding sickness in populations and individuals. For example, through anti-malarial tablets, the use of bed nets to protect against mosquitoes, health education and immunisation programmes. The focus is primarily on populations but some are individually focused, such as vaccination.
4. The promotive approach: Emphasises addressing basic social, economic and political causes of ill-health through advocacy and lobbying government and policy
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
143
makers, for example, to ban smoking in public places. It also focuses on intersectoral interventions directed at households or communities to improve water supply, sanitation, housing and so on. The focus is primarily on populations.
6 SESSION SUMMARY
This session has focused on the origins, evolution and rationale for the Primary Health Care approach. We discussed how the comprehensive PHC approach incorporates four elements or strategies – rehabilitative, curative, preventive and promotive.
In Unit 4 you will learn more about the PHC Approach and how it has been implemented since 1978.
SOPH, UWC, Postgraduate Diploma in Public Health: Population Health & Development: a PHC Approach – Unit 3
144





























