Embed Size (px)
Citation preview

Ui
La
Sb
Tc
Td
T
a
ARR1AA
KMPCK
1
icfaboaif
tC
0d
Leukemia Research 33 (2009) 1194–1198
Contents lists available at ScienceDirect
Leukemia Research
journa l homepage: www.e lsev ier .com/ locate / leukres
nique cytogenetic features of primary myelodysplastic syndromesn Chinese patients
in Lia, Xu-Ping Liub, Ling Niea, Ming-Hua Yuc, Yue Zhangd, Tie-Jun Qind, Zhi-Jian Xiaoa,d,∗
The State Key Laboratory of Experimental Hematology, Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medicalciences and Peking Union Medical College, Tianjin 300020, ChinaLaboratory of Cytogenetics, Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College,ianjin 300020, ChinaLaboratory of Morphology, Institute of Hematology and Blood Diseases Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College,ianjin 300020, ChinaDepartment of Clinical Hematology, Institute of Hematology and Blood Diseases Hospital, Chinese Academe of Medical Sciences and Peking Union Medical College,ianjin 300020, China
r t i c l e i n f o
rticle history:eceived 8 October 2008eceived in revised form9 November 2008ccepted 24 November 2008vailable online 6 January 2009
eywords:yelodysplastic syndromes
rimary
a b s t r a c t
Myelodysplastic syndromes (MDS) are a heterogeneous group of myeloid neoplasms. Chromosomalabnormalities have been detected in 40–70% patients with primary MDS and are heterogeneous amongpatients of different races and from different backgrounds. In the current study, 351 Chinese adult patientswith primary MDS were retrospectively analyzed for their chromosomal abnormalities by karyotyping.Among the 237 cases (67.5%) of chromosomal abnormalities, 99 were copy number changes alone (41.7%),70 were structural abnormalities alone (29.5%), and 68 displayed both of these changes (28.8%). Over-all, the frequency of −5/5q−/del(5)(q13–33) was 5.1% in these Chinese MDS patients, which was lowerthan that in the MDS patients of western countries (8.7–23.4%), and the incidence of 5q− syndromewas only 0.3% in Chinese MDS patients. On the other hand, the frequencies of trisomy 8 (19.1%) and
ytogeneticsaryotype
−20/20q−/del(20)(q11-13) (9.4%) were higher than those in western countries (1.2–7.0% and 2.0–3.5%,respectively). Chromosomal translocations were also detected in 31 cases (13.1%) including 12 raretranslocations that have not been reported in MDS patients before. In addition, i(17)(q10) was detected innine cases (3.8%), of which six cases only had this single abnormality. According to the IPSS chromosomalprognostic classification, the incidence of poor-risk karyotypes increased in the advanced WHO subtypes(p < 0.001). Together, we detected the unique cytogenetic features of chromosomal abnormalities and
of MD
some rare translocations. Introduction
In 2006, myelodysplastic syndromes (MDS) were defined explic-tly, on the Working Conference in Vienna, as myeloid neoplasmsharacterized by a genetic instability with increased risk of trans-ormation to acute myeloid leukemia (AML) [1]. Chromosomalbnormalities may cause intrinsic genomic instability, which haseen implicated in the pathogenesis of MDS. According to the eti-
logy, MDS are classified as primary diseases, which occur withoutprevious event, and secondary ones, which developed follow-ng a known mutagenic event. Chromosomal abnormalities arerequently detected in secondary MDS and are also common in pri-
∗ Corresponding author at: Department of Clinical Hematology, Institute of Hema-ology, Chinese Academy of Medical Sciences, 288 Nanjing Road, Tianjin 300020,hina. Tel.: +86 22 23909184; fax: +86 22 27219070.
E-mail address: [email protected] (Z.-J. Xiao).
145-2126/$ – see front matter © 2008 Elsevier Ltd. All rights reserved.oi:10.1016/j.leukres.2008.11.021
S among Chinese patients.© 2008 Elsevier Ltd. All rights reserved.
mary MDS. Chromosomal abnormalities were reported in 40–70%patients with primary MDS [2]. Studying the features of chromoso-mal karyotypes of MDS patients would help clarify the pathogenesisof disease onset and progression.
MDS represents a heterogeneous disease group and its featuresof chromosomal karyotypes are diversified. In 2005, Chen et alreported that isolated −5/5q− and −7/7q− in Chinese patientswith MDS were not as common as in patients of western countries(2.2% vs. 17.8–42.5%) [3]. The author suspected that environmen-tal factors, including chemical contamination and infectious agentsmay also play a role in the disparity in addition to the ethnic anddemographic reasons. Matsuda et al. also reported that Japanesepatients with FAB-RA, a subset of MDS which included most the
patients with 5q− syndrome as WHO classification, had a signifi-cantly lower frequency of 5q− than German patients with FAB-RA(3/102 vs. 39/199) [4]. There were several reports in other Asiancountries (such as Korea and Thailand) supporting the differencesin chromosomal karyotypes between eastern and western MDS
L. Li et al. / Leukemia Research 33 (2009) 1194–1198 1195
nges
pb
FHsnaRmra5rucMsricw
2
2
aMc1wfcowcw1yeto
2
Knlogs
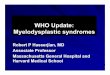
Fig. 1. Distributions and incidences of the copy number cha
atients [5,6]. Verifying and tracking the disparities may help usetter understand the mechanisms of MDS.
However, most of these previous studies were based onrench–American–British (FAB) classification. Currently, the Worldealth Organization (WHO) has established a new classification
ystem that has been widely used because of its advantages in diag-ostic and prognostic stratification. WHO classification representsn extension of the FAB proposal and it includes the removal ofAEB-T (now considered to belong to the AML section) and chronicyelomonocytic leukemia (now in MDS/MPD-interface group), the
ecognition of the impact of multilineage dysplasia in RA and RARS,nd the delineation of a cytogenetically defined subvariant, theq− syndrome [1]. The removal of certain subsets of MDS and theeduced standard of AML transformation when patients are eval-ated by the WHO classification may lead to different counting ofhromosomal aberrations when compared to the previous system.oreover, there have been no cytogenetic studies of MDS on a large
cale with rigorous case entry in China. Therefore, in this study, weetrospectively analyzed 351 adult MDS patients recruited in ournstitution according to the WHO classification in order to betterlarify the features of chromosomal karyotypes in Chinese patientsith primary MDS.
. Patients and methods
.1. Patients
Adult patients with primary MDS diagnosed between July 1990 and March 2008t the Institution of Hematology and Blood Disease Hospital, Chinese Academe ofedical Sciences (CAMS) were enrolled in this study only if they had obtained valid
ytogenetic results before treatment. The results were considered valid if at least5 metaphase cells were analyzed. We were careful to exclude the diseases thatere easy to be confused with MDS such as other disorders of bone marrow (BM)
ailures (e.g. aplastic anemia and paroxysmal nocturnal hemoglobinuria) or reactivehanges of BM due to severe infections or immune disorders or other hematopoieticr non-hematopoietic malignancies. MDS patients who had previously been treatedith antineoplastic drugs or ionizing radiation were considered as secondary MDS
ases and thereby excluded from the analyses. As the result, 351 Chinese patientsith primary MDS were recruited in our study. There were 239 (68.1%) males and
12 (31.9%) females with the median age of 45 years and the age range of 16–79ears. All of the 351 patients were reclassified according to the WHO criteria after re-xamination of the blood and BM smears at diagnosis [7]. This study was approved byhe ethical committee of Institute of Hematology, CAMS according to the guidelinesf the Declaration of Helsinki.
.2. Cytogenetic analysis
Chromosomes were R- or G-banded on unstimulated BM cells after 24 h culture.
aryotypes were classified according to International System for Human Cytoge-etic Nomenclature (1995). Clonal abnormality is defined according to the sameoss of chromosomal material in at least three metaphase cells or the same gainr structural aberration in at least two metaphase cells [1]. For cytognetic cate-orization, patients were classified according to international prognostic scoringystem (IPSS) [8] related to karyotypes: good–normal,)Y,del(5q), and del(20q);
or the abnormalities of chromosomal arms. G: gain; L: loss.
poor–complex (three or more abnormalities) and chromosome 7 anomalies; andintermediate–other abnormalities.
2.3. Statistical analysis
Count data were compared by Pearson’s Chi-square analyses. P values less than0.05 were considered statistically significant. All statistical analyses were performedwith SPSS 13.0 software.
3. Results
3.1. Incidences of chromosomal abnormalities in MDS patients
Among the 351 patients with valid cytogenetic results, 237cases (67.5%) demonstrated chromosomal abnormalities. Of those,99 were copy number changes alone (41.7%), 70 were structuralabnormality alone (29.5%), and 68 displayed both of these changes(28.8%). In addition, among the 237 patients with chromosomalabnormalities, 130 cases (54.8%) showed single abnormality, 54cases (22.8%) showed double abnormalities and 53 cases (22.4%)showed complex abnormalities (more than two independentaberrations). There were three cases (1.3%) of tetraploid, one case(0.4%) of multiploid, one case (0.4%) of hyperdiploid and threecases (1.3%) of hypodiploid. Aneuploidy or anomaly of chromoso-mal arm were detected across all of the 24 chromosomes. Theirdistributions and incidences are shown in Fig. 1. The abnormalitiesfrequently detected are listed in Table 1. Chromosome transloca-tions were detected in 31 cases (13.1%), among them four cases witht(1;7)(q10;p10), two cases with t(1;3)(p36;q21), two cases witht(3;3)(q21;q26) and each one case with other types. There were 12translocations not reported in MDS, which were validated by searchin the following databases: http://AtlasGeneticsOncology.org;http://cgap.nci.nih.gov/Chromosomes/Mitelman;http://www.ncbi.nlm.nih.gov. These rare translocations arelisted in Table 2. Eight cases were present with single balancedtranslocation and other cases simultaneously involved additionalcopy number changes. In addition, i(17)(q10) was detected in ninecases (3.8%). Chromosomal duplications were present in sevencases (3.0%), of which four cases involved chromosome 1.
3.2. Distributions of chromosomal abnormalities among WHOsubtypes
The distribution of WHO subtypes of 351 patients is listed
in Table 3. There was no statistical difference in the incidencesof chromosomal aberrance in each WHO subtype (�2 = 0.733,p = 0.865). Trisomy 8 (+8) was present in all subtypes exceptRARS and mostly seen in MDS-U (33.3%); monosomy 20, eitherinterstitial or complete loss of the long arm of chromosome 20
1196 L. Li et al. / Leukemia Research 33 (2009) 1194–1198
Table 1Chromosomal abnormalities frequently detected in MDS patients.
Chromosomal abnormalities Case (n) Incidence (%) Proportion in chromosomal abnormality (%) Single abnormality (n) Single abnormality (%)
+8 67 19.1 28.3 33 49.3−20/20q−/del(20)(q11–13) 33 9.4 13.9 13 39.4−7/7q−/del(7)(q21–32) 31 8.8 13.1 4 12.9−5/5q−/del(5)(q13–33) 18 5.1 7.6 5 27.8−18 10 2.8 4.2 0 0−11/11q−/del(11)(q23–25) 9 2.6 3.8 0 0+21 9 2.6 3.8 3 33.3−Y 8 2.3 3.4 2 25.0−21 7 2.0 3.0 0 0−10 7 2.0 3.0 0 0−16 6 1.7 2.5 0 0−22 6 1.7 2.5 0 0+9 5 1.4 2.1 1 20.0del(12)(p12) 5 1.4 2.1 3 60.0
Table 2Rare chromosomal translocations detected in MDS patients.
Case no. Diagnosis Chromosomal karyotype
1 RCMD 47,XY,+8,der(11)t(1;11)(q11;q25) [7]/46,XY [2]2 RCMD 46,XY, der(11)t(1;11)(q11;p15) [15]3 RAEB-I 45,X,−Y,der(12)t(1;12)(q10;q10) [7]/43–44,X,−Y, der(12)t(1;12)(q10;q10),−14,−18,−20,−21 [cp5]4 RCMDRS 46,XY,der(19)t(1;19)(q23:p13)[8]/46,XY [2]5 RAEB-II 45,XY,t(3;9)(p21;p23),−7 [5]6 RAEB-I 44,XY,add(4)(q35),t(5;13)(q21;q31),del(7)(q32), ins(12;?) (q14;?),−15,add(22)(q13) [12]/44,XY,idem,+18q+ [1]/46,XY [3]7 RCMD 46,XX,der(16)t(5;16)(q14;p13) [1]/41–45,XX, der(16)t(5;16)(q14;p13) [cp4]8 RARS 45,XY,−16,der(19)t(5;19)(q22;q13) [2]/46,xy [13]9 RAEB-I 46,XY,t(6;9)(p23;p11),del(5)(q13;q33), der(7)t(1;7)(q10;p10) [3]/46,idem,del(20)(q11) [5]/46,XY,idem,−10, del(20)(q11),+mar [1]
10 RA 42–45,XX,del(5)(q14;q32),−5,der(6)t(6;9)(p10;q10), −6, der(7)t(1;17)(q10;q10),del(11)(p13),−17,−19, del(20)(q11), −22 [cp10]/46,XX [1]y, t(7;17)(p15;q11),del(22)(q11) [2]/46,xy [6]
(Mem(Ri(isto(afsIrsw
TD
W
RRRRRRM5
11 RA 45,XY,t(7;17)(p15;q11),−18,del(22)(q11)[1]/46,x12 RA 46,XX,t(x;6)(p10;p10) [11]/46,XX [4]
−20/20q−/del(20)(q11–13)) was present in all subtypes exceptDS-U and most commonly seen in RARS (9.1%); monosomy 7,
ither interstitial or complete deletion of the long arm of chro-osome 7 (−7/7q−/del(7)(q21–32)) was mostly seen in RAEB-II
15.2%); monosomy 18 (−18) was observed in all subtypes exceptCMDRS and mostly seen in RARS (9.1%); monosomy 11, either
nterstitial or complete deletion of the long arm of chromosome 11−11,11q−, del(11)(q23–25)), and monosomy 16 (−16) were presentn all subtypes except for RA, RARS and MDS-U subtypes, and mostlyeen in RCMDRS (both were 6.7%); trisomy 21 (+21) and segmen-al deletion of short arm of chromosome 12 (del(12)(p12)) werenly observed in RCMD, RAEB-I and RAEB-II; monosomy 21 and 10−21,−10) were present in all subtypes except for RARS, RCMDRSnd MDS-U; monosomy Y (−Y) was present in all subtypes exceptor RA, RARS and RCMDRS, and mostly seen in MDS-U (16.7%); tri-omy 9(+9) was only observed in RCMD and RAEB-I. According to
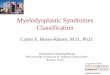
PSS chromosomal prognostic classification, the incidence of poor-isk karyotypes increased in the following order: RA, RARS, 5q−yndrome; RCMD, RCMDRS; RAEB-I and RAEB-II. Such increasesere statistically significant (p < 0.001)(Fig. 2).Fig. 2. Distributions of karyotype subgroups of IPSS among MDS subtypes based onWHO classification.
able 3istribution of chromosomal abnormalities among MDS subtypes based on WHO classification.
HO subtype Case (n) No. of cases with chromosomal abnormality (%) Chromosomal abnormality frequently seen
A 47 33 (70.2) +8,−7/del(7q),del(20q),−5/del(5q),−18,−21,−22,−10ARS 11 5 (45.5) −7/del(7q),del(20q),−5/del(5q),−18CMD 154 109 (70.8) All of the chromosomal abnormalities listed in Table 1 are frequently seenCMDRS 15 10 (66.7) +8, −7/del(7q),del(20q),−5/del(5q),−11,−16AEB-I 68 45 (66.2) All of the chromosomal abnormalities listed in Table 1 are frequently seenAEB-II 46 29 (63.0) All of the chromosomal abnormalities listed in Table 1 are frequently seen except del(20q)DS-U 6 5 (83.3) −Y
q− syndrome 1 1 (100) del(5q)

search
4
macmsmdtaittbt[
aa7cNrT−siMiiMnmmbtapc
oai−t1tit[ctpratwtwcptet
[
L. Li et al. / Leukemia Re
. Discussion
Unlike other hematological malignancies with balanced chro-osome translocations resulting in dominant mutations and
ctivation of oncogenes, MDS is usually associated with unbalancedhromosomal abnormalities [9]. Our study showed that the chro-osomal anomalies common in MDS are copy number changes
uch as losses and/or gains of the whole chromosome or abnor-alities of the chromosomal arms, implicating the changes of gene
osage. It has been known that gene dosage changes can contributeo the onset or development of diseases by the mechanisms suchs overexpression of some crucial genes, or loss of heterozygos-ty and haploinsufficiency, which are related to the inactivation ofumor suppressor genes (TSG). For instance, it was suspected thathe involvement of TSGs like CTNNA1, IRF-1, EGR1, SPARC and RPS14y loss of 5q or the overexpression of some genes due to +8 may con-ribute to the onset of MDS or prompt its leukemic transformation10].
In addition to the copy number changes of chromosome or thenomaly of chromosomal arms, chromosomal translocations werelso detected in 13.1% cases in our study. The chromosomes 1, 3, 5, 6,, 9, 11, 12, 13, 17, 18, 19 and 21 were frequently involved in translo-ations, which led to the abnormalities of genes such as MEL1,UP98, HOXD13, HOXA9, TEL and PBX1/E2A. Among them, the
ecurrent translocations were t(1;3) (p36;q21) and t(1;7)(q10;p10).he two recurrent translocation and another structural anomalyi(17)(q10), which was also recurrent in MDS, respectively pos-
ess distinct characteristics in clinical manifestations, morphology,mmunology and cytogenetics. Our previous studies found that
DS patients with I(17q) account about 1% of MDS, majory affect-ng male, severe anemia and hyposegmentation of neutrophil,ncreased micromegakaryocyte, with a poor prognosis and that
DS patients with t(1;3)(p36;q21) showed macrocytic anemia,ormal or elevated platelet counts, hyperplasia with dysplasia ofegakaryocytes, and poor prognosis and proposed these abnor-alities as novel clinical-pathologic subsets of MDS that need to
e confirmed by more cases in the future [11,12]. In addition to theranslocations recurrently reported in MDS, we identified 12 bal-nced translocations that had not yet been found in MDS patientsreviously. Their roles in the MDS pathogenesis remain to be dis-overed.
Among the known chromosomal aberrations in MDS patientsf western countries, the incidences of copy number changesnd abnormalities of chromosomal arms decreased in the follow-ng order: −5/5q−/del(5)(q13–33), −7/7q−/del(7)(q21–32), +8 and20/20q−/del(20)(q11–13); while in our Chinese MDS patients
hey decreased in the following order: +8, −20/20q−/del(20)(q11-3), −7/7q−/del(7)(q21–32) and −5/5q−/del(5)(q13–33). Consis-ent with previous reports from China and Southeast Asia, thencidences of +8 and −20/20q−/del(20)(q11–13) were higher thanhose in western countries(1.2–7.0% and 2.0–3.5%, respectively)2,3,6,13–15]. In addition, as reported previously by some Asianountries, the incidence of −5/5q−/del(5)(q13–33) was lowerhan that in western countries (0.8–6.3%) [3–5,13,16,17]. Moreover,atients with −5/5q−/del(5)(q13–33) as a single abnormality rep-esented only a small portion of cases, and most of them haddditional chromosome changes or were accompanied by morehan 5% blasts in BM, implying that the cases with 5q− syndromeere even less. Consistent with previous reports, the disparities in
he cytogenetics of MDS patients from eastern and western countiesere confirmed in our study. Given that chromosomal aberrance
ould be induced by chemicals or radiation in habitats, we sup-ose that the differences in chromosomal aberrance may reflecthe disparities in the living environment and customs betweenastern and western populations. However, this hypothesis needso be verified by international epidemiological investigations. It is
[
[
33 (2009) 1194–1198 1197
worth noting that previously the disparities in the clinical and lab-oratory features between eastern and western patients with MDShave already been reported [3]. A further study is in anticipationto test whether the different clinical and laboratory manifestationsbetween eastern and western MDS patients are resulted from thedifference in karyotypes, which may be an important mechanismunderlying MDS.
According to the WHO classification, the incidence of−7/7q−/del(7)(q21–32) was higher in RAEB-II patients than inother MDS subtypes, which indicated that the aberrations of chro-mosome 7 mainly exist in advanced WHO defined MDS subtypewith higher BM blast and predict poor risk. According to IPSSchromosomal prognostic classification, the incidences of poor-riskkaryotypes increased in the advanced WHO subtypes, which sup-ported the prognostic significance of WHO classification.
Overall, the current data indicated the features of chromoso-mal abnormalities in Chinese primary MDS patients be distinctfrom those in western countries. Further studies are necessary toreveal the disparity in the pathogenesis related to the occurrenceand the AML transformation of MDS between eastern and westernpatients.
Conflict of interest
None.
Acknowledgements
Supported partially by the National Natural Science Funds (No.30670899), Tianjin Key Natural Science Funds (08JCZDJC19200),Specialized Research Fund for the Doctoral Program of Higher Edu-cation (20050023033) and Program for New Century ExcellentTalents in University (NCET-05-0173).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.leukres.2008.11.021.
References
[1] Valent P, Horny HP, Bennett JM, et al. Definitions and standards in the diagnosisand treatment of the myelodysplastic syndromes: Consensus statements andreport from a working conference. Leuk Res 2007;31:727–36.
[2] Bernasconi P, Klersy C, Boni M, et al. World Health Organization classification incombination with cytogenetic markers improves the prognostic stratificationof patients with de novo primary myelodysplastic syndromes. Br J Haematol2007;137:193–205.
[3] Chen B, Zhao WL, Jin J, et al. Clinical and cytogenetic features of 508 Chinesepatients with myelodysplastic syndrome and comparison with those in Westerncountries. Leukemia 2005;19:767–75.
[4] Matsuda A, Germing U, Jinnai I, et al. Difference in clinical features betweenJapanese and German patients with refractory anemia in myelodysplastic syn-dromes. Blood 2005;106:2633–40.
[5] Lee JH, Lee JH, Shin YR, et al. Application of different prognostic scoring systemsand comparison of the FAB and WHO classifications in Korean patients withmyelodysplastic syndrome. Leukemia 2003;17:305–13.
[6] Intragumtornchai T, Prayoonwiwat W, Swasdikul D, et al. Myelodysplastic syn-dromes in Thailand: a retrospective pathologic and clinical analysis of 117 cases.Leuk Res 1998;22:453–60.
[7] Vardiman JW, Harris NL, Brunning RD, et al. The Wor1d Health Organization(WHO) classification of the myeloid neoplasms. Blood 2002;100:2292–302.
[8] Greenberg P, Cox C, LeBeau M, et al. International scoring system for evaluatingprognosis in myelodysplastic syndromes. Blood 1997;89:2079–88.
[9] Olney HJ, Le Beau MM. Evaluation of recurring cytogenetic abnormalities in thetreatment of myelodysplastic syndromes. Leuk Res 2007;31:427–34.
10] Virtaneva K, Writht FA, Tanner SM, et al. Expression profiling reveal fundamental
biological differences in acute myeloid leukemia with isolated trosomy 8 andnormal cytogenetics. PNAS 2001;98:1124–9.11] Xiao Z, Liu Z, Yu M, et al. Ischromosome 17q in patients with myelodysplasticsyndromes: six new cases. Haematologica 2003;88:714–5.
12] Xiao Z, Zhang M, Liu X, et al. MEL1s, not MEL1, is overexpressed in myelodys-plastic symdromes patients with t(1;3)(p36;q21). Leuk Res 2006;30:332–4.

1 search
[
[
[
[scoring systems, the French–American–British (FAB) and World Health Orga-
198 L. Li et al. / Leukemia Re
13] Pfeilstöcker M, Reisner R, Nösslinger T, et al. Cross-validation of prognosticscores in myelodysplastic syndromes on 386 patients from a single institution
confirms importance of cytogenetics. Br J Haematol 1999;106:455–63.14] Belli C, Acevedo S, Bengio R, et al. Detection of risk groups in myelodysplasticsyndromes. A multicenter study. Haematologica 2002;87:9–16.
15] Lorand-Metze I, Pinheiro MP, Ribeiro E, et al. Factors influencing survival inmyelodysplastic syndromes in a Brazilian population: comparison of FAB andWHO classifications. Leuk Res 2004;28:587–94.
[
33 (2009) 1194–1198
16] Müller-Berndorff H, Haas PS, Kunzmann R, et al. Comparison of five prognostic
nization (WHO) classifications in patients with myelodysplastic syndromes:results of a single-center analysis. Ann Hematol 2006;85:502–13.
17] Navarro I, Ruiz MA, Cabello A, et al. Classification and scoring systems inmyelodysplastic syndromes: a retrospective analysis of 311 patients. Leuk Res2006;30:971–7.