Embed Size (px)
Citation preview
Pakistan Oral & Dent. Jr. 23 (1) June 2003
ORTHODONTICS
UNILATERAL MAXILLARY MOLAR DISTALIZATION APPLIANCE USING AN EXPANSION SCREW
*NASSER M. AL-JASSER, BDS., MSc
ABSTRACT
Objectives: An appliance to correct unilateral Class II molar relationship was described, the clinical and laboratory procedures for the construction of the appliance were explained. The clinical application for the unilateral molar distalization was illustrated by a case report. Other methods of distalizaton were reviewed and compared with the present appliance. The advantages and disadvantages of the appliance were presented.
Methods and Materials: The appliance is attached to the maxillary dentition through the bands of the maxillary molars and premolars. The anchor molar and premolar bands are connected to each other by 0.9 mm stainless steel wire that was soldered to the lingual surface of the bands. The wire from the anchor teeth was then soldered to the wire of the expansion screw. The expansion screw was also soldered to the molar band that need distalization. An acrylic button was added to the wire crossing the palatal slope above the rougae for more anchorage
Results: The clinical application showed a unilateral class H molar and canine relationships were corrected by the appliance. The posttreatment panoramic radiograph showed that the roots of the teeth were fairly parallel, and the maxillary left lateral incisor was positioned into the arch. The supporting tissues appeared healthy. The posttreatment cephalometric radiograph and superimposed tracing showed no significant changes in the skeletal measurements after treatment, as expected, with no orthopedic treatment. Conclusion: The appliance was found to be effective in correcting unilateral molar Class H, and therefore it is recommended for clinical use on cases indicated for its use.
Key words: Molar distalization, Class II malocclusion, Orthdontic appliance, Anchorage.
INTRODUCTION
Maxillary molar distalization is the most recent modality in the treatment ofclass II malocclusion with moderate crowding of the maxillary arch and aligned mandibular arch where the skeletal relationship is accepted. Several methods for maxillary molar distalization were described that include the extra-oral traction, the Wilson distalizing arches, the removable springs, and the sliding jigs. The interest in the use of extra-oral traction goes back to the time of Oppenheim1 and Kloehn2-4 who recommended the application of
extra-oral forces for the mass distal movement of maxillary teeth. The extra-oral traction has proved to be a reliable method of correcting class II molar relationship for over hundred years, and was used with varying frequency worldwide.5 Although, the distal movement of the maxillary molars was a classical treatment method by the headgear therapy,3,6-16 tthe unilateral distal movement of maxillary molars was attempted for many years without the expected suc-cess.17-19 It has been reported that the use of the asymmetric headgear generates lateral forces that cause unilateral cross-bite.20 However, with the head-
* Associate Professor, Orthodontic Division, Department of Preventive Dental Sciences, Dental College, King Saud University, P.O. Box 53923 Riyadh 11593 Kingdom of Saudia Arabia, Fax no.: 00 966 1 4195367, E-mail address: [email protected]
11
gear therapy the cooperation of the patient is the key success for effective and efficient results. Through the years a combination of fixed and removable intra-oral appliances was developed for molar distalization with different modifications in the design and applications taking the advantage of minimizing the dependence on the patient's cooperation.21-22 These include the mag-nets23-25, the super elastic Ni-Ti coil springs26-28, the pendulum appliances29 and the intra oral bodily molar distalizer.30 The selection of unilateral distalization method and technique is related to the preference, experience and availability of the required materials. The aim of this paper was to introduce a method of unilateral distalization of the maxillary first molar and to illustrate the laboratory procedure of constructing the appliance and demonstrate its clinical application.
MATERIALS AND METHODS
The material needed for the construction of the appliance consists of orthodontic molar and premolar bands, expansion screw, 0.9 mm stainless steel hard orthodontic laboratory wire, acrylic and orthodontic silver solder and alginate impression material.
Appliance Design
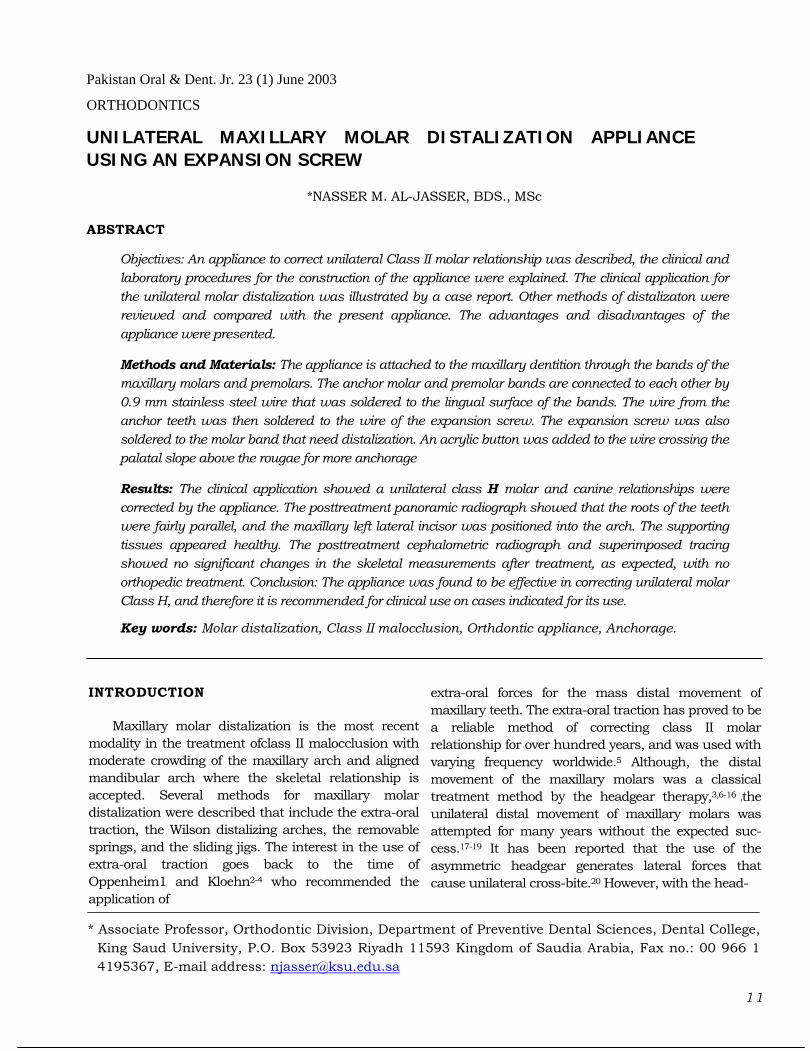
The appliance is attached to the maxillary denti-tion by means of the bands of the maxillary molars and premolars. The anchor molar and premolar bands are connected to each other by 0.9 mm stainless steel wire that was soldered to the lingual surface of the bands. The wire from the anchor teeth was then soldered to the expansion screw. The expansion screw was also soldered to the molar band that needs distalization. An acrylic button was added to the wire crossing the palatal slope above the rougae for more anchorage (fig. 1 a and b).
Appliance construction
1) Bands were fitted on the maxillary molars and maxillary first premolars. An alginate impression of the maxillary arch with the bands in place was taken.
2) The bands were removed from the teeth and placed in the impression, and secured with sticky wax. The impression was disinfected and sent to the laboratory for pouring.
3) After the work model was poured and rough-trimmed, the lingual attachments of the bands (if present) were removed. The stone at the periphery
12
of the lingual surfaces of the bands were removed to facilitate the soldering process.
4) The outline of the appliance design was drawn on the model.
5) The stainless steel wire was bent according to the design.
6) The stainless steel wire was soldered to the anchor molar and premolar bands.
7) The expansion screw was soldered to the anchor wire and to the molar that needs distalization.
8) An acrylic button was fitted on the wire for extra anchorage.
9) The appliance was smoothed, polished, cleaned and disinfected and prepared for delivery.
Delivery and activation
The appliance was placed passively in the mouth with all bands fitting properly on the teeth. Thereafter it was cemented using highly adhesive cements (e.g, glass ionomer or compomer). The expansion screw of the appliance was activated twice a week until molar distalization was achieved. As with all distalizing mechanics, it was recommended that the maxillary molars be over-corrected to a position of "super-class I molar relationship" to allow for some settling in the molar relationship that may occur during the next phase of treatment; on average, four to six months of molar distalization with twice a week activation is required.
Case report
The clinical efficiency of the described appliance to unilaterally distalize the maxillary molar and correct the molar relationship is illustrated with a clinical case.
History
A girl, aged 17 years, had a chief complaint of crowded upper anterior teeth. Her medical history indicated heart problem and the patient was under medication and the dental history showed good dental care with multiple restorations. The cause of malocclu-sion was presumed to be a combination of genetic and developmental factors.
Clinical finding
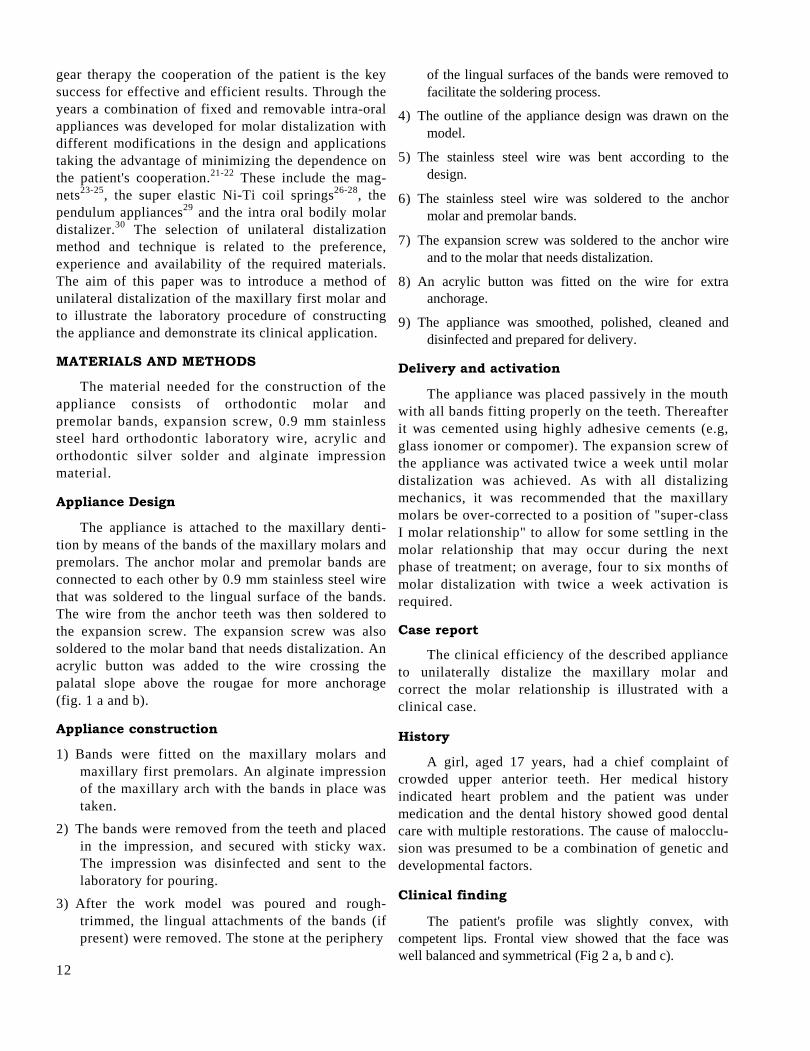
The patient's profile was slightly convex, with competent lips. Frontal view showed that the face was well balanced and symmetrical (Fig 2 a, b and c).
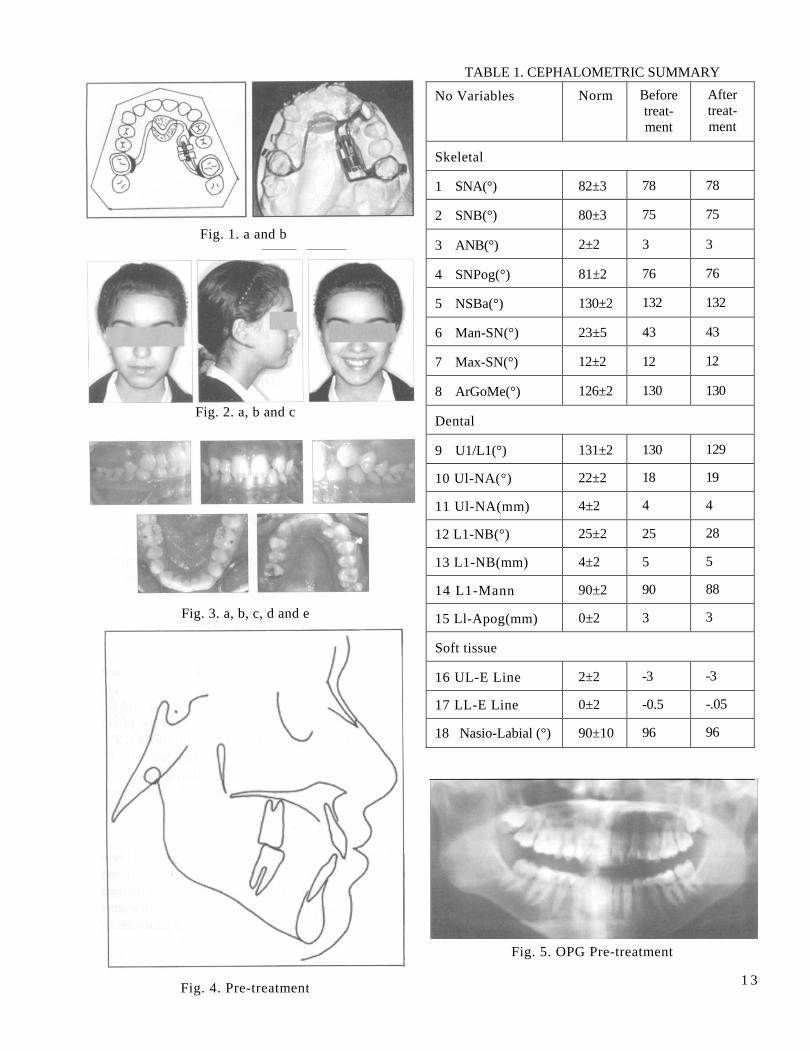
Fig. 1. a and b
Fig. 2. a, b and c
Fig. 3. a, b, c, d and e
Fig. 4. Pre-treatment
TABLE 1. CEPHALOMETRIC SUMMARY
No Variables Norm Before treat- ment
After treat- ment
Skeletal
1 SNA(°) 82±3 78 78
2 SNB(°) 80±3 75 75
3 ANB(°) 2±2 3 3
4 SNPog(°) 81±2 76 76
5 NSBa(°) 130±2 132 132
6 Man-SN(°) 23±5 43 43
7 Max-SN(°) 12±2 12 12
8 ArGoMe(°) 126±2 130 130
Dental
9 U1/L1(°) 131±2 130 129
10 Ul-NA(°) 22±2 18 19
11 Ul-NA(mm) 4±2 4 4
12 L1-NB(°) 25±2 25 28
13 L1-NB(mm) 4±2 5 5
14 L1-Mann 90±2 90 88
15 Ll-Apog(mm) 0±2 3 3
Soft tissue
16 UL-E Line 2±2 -3 -3
17 LL-E Line 0±2 -0.5 -.05
18 Nasio-Labial (°) 90±10 96 96
Fig. 5. OPG Pre-treatment
1 3
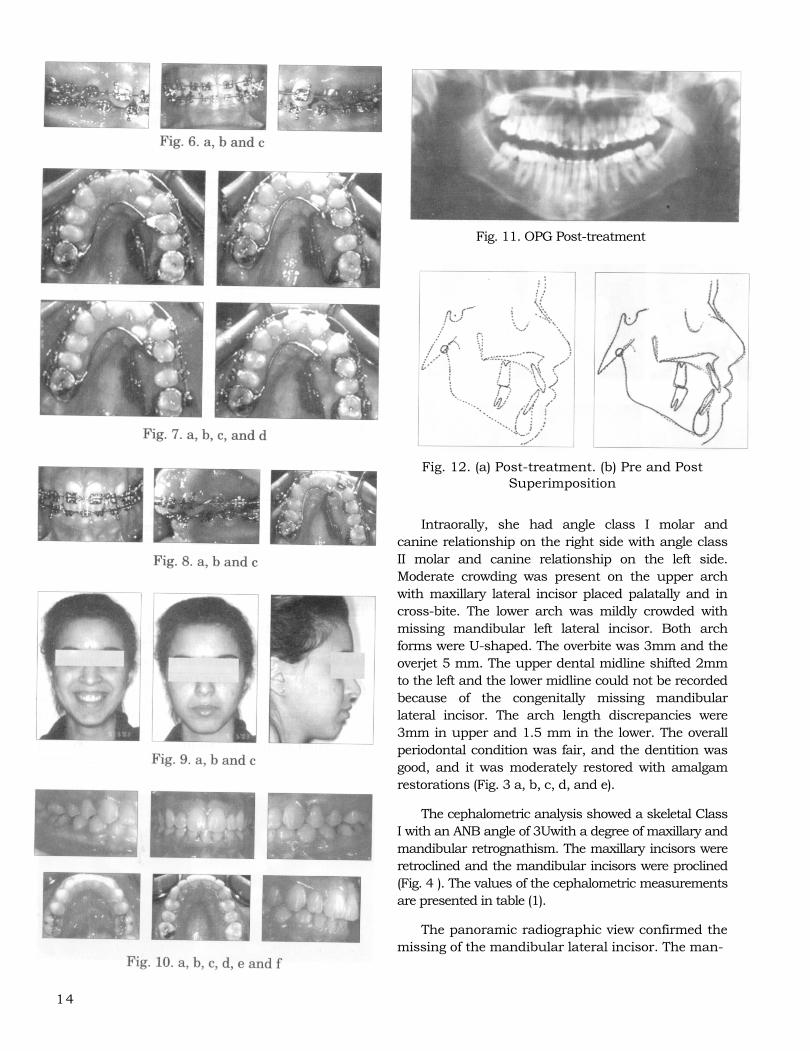
Fig. 11. OPG Post-treatment
14
Fig. 12. (a) Post-treatment. (b) Pre and Post Superimposition
Intraorally, she had angle class I molar and canine relationship on the right side with angle class II molar and canine relationship on the left side. Moderate crowding was present on the upper arch with maxillary lateral incisor placed palatally and in cross-bite. The lower arch was mildly crowded with missing mandibular left lateral incisor. Both arch forms were U-shaped. The overbite was 3mm and the overjet 5 mm. The upper dental midline shifted 2mm to the left and the lower midline could not be recorded because of the congenitally missing mandibular lateral incisor. The arch length discrepancies were 3mm in upper and 1.5 mm in the lower. The overall periodontal condition was fair, and the dentition was good, and it was moderately restored with amalgam restorations (Fig. 3 a, b, c, d, and e).
The cephalometric analysis showed a skeletal Class I with an ANB angle of 3Uwith a degree of maxillary and mandibular retrognathism. The maxillary incisors were retroclined and the mandibular incisors were proclined (Fig. 4 ). The values of the cephalometric measurements are presented in table (1).
The panoramic radiographic view confirmed the missing of the mandibular lateral incisor. The man-

15
dibular third molars were not formed and considered absent. There was no apparent pathology in the den-toalveolar structures (Fig. 5).
Treatment objectives
Due to the heart problem the objectives of treating this malocclusion was non-extraction utilizing unilateral molar distalization appliance to eliminate the crowding and correct the cross-bite of tooth #21 and align the teeth.
Treatment progress
The medical consultation indicated the need for antibi-otic coverage for any dental surgical procedure. The plaque control and oral hygiene instruction were given to the patient. The described appliance above was constructed and placed in the upper arch in order to distalize the maxillary left molar with the fixed appli-ance (Fig. 6 a, b and c). The molar distalization was achieved in a period of 6 months. The second premolar was moved distally then the 0.9 mm stainless steel wire which was soldered to the first premolar cut to allow for distalization of the first premolar. The appliance was kept in its place to act as an anchorage then the first premolar and canine were moved distally (Fig. 7 a, b, c, and d). When enough space that could occupy the lateral incisor was created, a band was placed on the maxillary lateral incisor (Fig. 8 a, b and c). The upper arch was leveled and aligned with 0.014" Nitinol and working up to 0.019x0.25 stainless steel archwire.
Treatment results
The arch length deficiency was eliminated in both arches, and excellent alignment obtained. A class I molar and canine relationship was achieved but the overjet remained increased which was related to the missing mandibular lateral incisor (Fig. 9 a, b and c, Fig. 10 a, b, c, d and e). The post-treatment panoramic radiograph showed that the roots of the teeth were fairly parallel, and the maxillary left lateral incisor was positioned into the arch (Fig. 11). The supporting tissues appeared healthy. The post-treatment cephalo-metric radiograph and superimposed tracing showed no significant changes in the skeletal measurements after treatment, as expected, with no orthopedic treatment (Fig 12 a and b).
DISCUSSION
The aim of the treatment was achieved and the unilateral class II molar relationship was corrected by
the molar distalization appliance described above. The appliance was developed to avoid using extra-oral traction1-4 which involved active participation of the patient in the treatment process. The molar moved bodily through the occlusal plane.29-33 The rationale for this sequence is based on the concept that the initial movement of one molar is supported by all the other teeth including the opposite molar, thus maximizing anchorage.29 Careful attention to anchorage is critical during distalizing the molar. Anchorage must be con-trolled to make sure that ideal class I molar relationship was achieved. The maxillary second premolar will drift posteriorly, due to the pull of the transseptal fibers. This spontaneous movement improves the Class II correction with minimal anchorage loss.34
In contrast to the using of Pendulum and Pendex appliances29 which require the placement of "Quick Nance"35 to maintain molar distalization and expan-sion, the described appliance in this paper achieved molar distalization and stabilization without the need to remove the distalizing appliance and cementing another appliance for stabilization which would have increased the chair-side time and the cost of treatment. Recent clinical studies on the Pendulum and Pendex appliances have shown that, the appliances were efficient in producing distal movement of the maxillary molars36,37 without the need for high level of patient's cooperation as with the extra-oral traction.38 However, as a result of molar distalization a slight amount of bite opening was reported with this type of appliance but was reported as not significant clinically.39 The bite opening reported could be due to distal tilting of the molars and/or lingual movement. The expansion screw appliance described and used above has many distinct advantages. First, the appliance design and construction is simple and available in most clinical set-up. Second, the maxillary molars distalization was mainly bodily movement without the distal and/or lingual tilting that occurs with the pendulum appliance. Third, the appliance was converted to a holding arch after molar distalization was completed without the need for another appliance and orthodontic treatment could continue without discontinuity in the treatment mechanics.
CONCLUSIONS
The result demonstrated that for this case the expansion screw appliance was an effective device to distalize molars unilaterally and bodily and open up the space for maxillary lateral incisor. The advantage of this appliance was the ease of activation and reactiva-
tion by the patient or the clinician, molar expansion and short chairside time. In addition it is easy to construct and can be used during the fixed appliance therapy. There is the possibility to design it as all-metal with no acrylic plate, the primary advantage being comfort and improved hygiene for the patient.
ACKNOWLEDGEMENT
Author is thankful to Associate Professor Dr Muhammed Bukhary and Professor A L Nwoku for reviewing the manuscript and the post graduate stu-dents from KSU College of Dentistry for their help in taking photographs.
REFERENCES (Old r e f e r en c e s a r e o f h i s t o r i c a l in t e r e s t )
1- Oppenheim A. Biologic orthodontic therapy and reality. Angle Orthod 1936; 6:153-183.
2- Kloehn SJ. Guidance alveolar growth and eruption of teeth to reduce treatment time and produce a more balanced denture and face. Angle Orthod 1947; 17:10-23.
3- Kloehn SJ. Orthodontics-force or persuasion. Angle Orthod 1953; 23: 56-65.
4- Kloehn SJ. Evaluation of cervical anchorage force in treatment. Angle Orthod 1961; 31:91-104.
5- Kingsley NW. Treatise on oral deformities as a branch of mechanical surgery, New York, 1980, Appleton.
6- Tweed CH. A philosophy of orthodontic treatment. Am J Orthod Oral Surg 1945; 31: 74-103.
7- Merrifield LL. Edgewise sequential directional force technology. J Charles Tweed Found 1986; 14: 22-37.
8- Holdaway R. Changes in relationship of points A and B during orthodontic treatment. Am J Orthod 1956; 42: 176-193.
9- Cangialosi TJ, Meistrell ME, Jr, Leung MA, Ko JY. A cepha-lometric appraisal of edgewise Class II nonextraction treatment with extraoral force. Am J Orthod Dentofac Orthob 1988; 93: 315-324.
10- Poulton DR. Changes in Class II Malocclusion with and without occipital headgear therapy. Angle Orthod 1959;29:234250.
11- Nelsson BG. Extroral anchorage in the treatment of Class II division 1 Malocclusions- its possibilities and limitations. Angle Orthod 1953;23:121-133.
12- Graber TM. Extraoral force- facts and fallacies. Am J Orthod 1955;41:490-505.
13- King EW. Cervical anchorage in Class II division 1 treatment, a cephalometric apprasisal. Angle Orthod 1957; 27: 98-104.
14- Ricketts RM. The influence of orthodontic treatment on facial growth and development. Angle Orthod 1960; 30:103-133.
15- Poulton DR. The influence of extraoral traction. Am J Orthod 1967; 53: 8-18.
16- Epstein W. Analysis of change in molar relationships by means of extraoral anchorage (head-cap) in treatment of malocclusion. Angle Orthod 1948;18:63-70.
17- Haak DC, Weinstein S. The mechanics of centric and eccentric cervical traction. Am J Orthod Dentofacial Orthop 1958; 44: 236-257.
16
18- Oosthuizen L, Dickman JFP, Evans WG. A mechanical ap-praisal of the Kleochn extraoral assembly. Angle Orthod 1973; 43: 221-232.
19- Baldini G. Unilateral headgear: Lateral forces as unavoidable side effects. Am J Orthod Dentofacial Orthop 1980; 77: 333-339.
20- Yoshida N, Jost-Brinkmann P, Miethke R, Konig M, Yamada Y. An experimental evaluation of effects and side effects of asymmetric face bow in the light of in vivo measurements. Am J Orthod Dentofacial Orthop 1998; 26: 706-714.
21- Cetlin NM, Ten Hoove A. Non-Extraction treatment.J. Clinical Orthodont 1993; 17: 396-413.
22- Warren DW. Clinical application of the A.C.C.O Appliance Part 1. Am J Orthod 1992; 101:101-111.
23- Blechman AM., Smiley H. Magnetic force in orthodontics. Am J Orthod Dentofacial Orthop 1978; 74: 435-443.
24- Gianelly AA, Bonds PW, Johnson WM. Distalization of molars with repelling magnets. J Clin Orthod 1988; 22: 40-44.
25- Bondemark L, Kurol J. Distalization of maxillary first and second molars simultaneously with repelling magnets. Eur J Orthod 1992; 14: 264-272.
26- Gianelly AA, Bednar J, Dietz VS. Japanese Ni-Ti coils used to move molars distally. Am J Orthod Dentofacial Orthop 1991; 99: 564-566.
27- Bondemark L, Kurol J. Repelling magnets versus superelastic Ni-Ti coils in simultaneous distal movement of maxillary first and second molars. Angle Orthod 1994; 63: 189-198.
28- Carano A, Testa M, Siciliani G. The lingual distalizer system. Eur J Orthod 1996; 18: 445-448.
29- Hilgers JJ. The Pendulum appliance for Class II non-compli-ance therapy. J Clin Orthod 1992; 26: 706-714.
30- Keles A, Sayinsu K. A new approach in maxillary molar distalization: Intraoral bodily molar distalizer. Am J Orthod Dentofacial Orthop 2000; 117: 39-48.
31- Bennett RK, Hilgers JJ. The Pendulum appliance: Creating the gain. Clin Impression 1994; 3: 14-18.
32- Bennett RK, Hilgers JJ. The Pendulum appliance: Maintaining the gain. Clin Impression 1994; 3: 6-9,14-22.
33- Snodgrass DJ. A fixed appliance for maxillary expansion. Molar rotation and molar distalization. J Clin Orthod 1996; 30: 156-159.
34- McNamara JJ, Brudon WL. Orthodontics and Dentofacial Orthopedics
35- Hilgers JJ, Bennett RK. The Pendulum appliance, Part II: Maintaining the gain. Clin Impression 1994; 3: 5-9, 14-18,22.
36- Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofac Orthop 1996; 110: 639-646.
37- Joseph AA, Butchart CJ. An evaluation of the Pendulum distalizing appliance. Semon Orthod 2000; 6: 129-135.
38- Byloff FK, Darendeliler MA. Distal molar movement using the Pendulum appliance. Part 1: Clinical and Radiological evalu-ation. Angle Orthod 1997; 67: 249-260.
39- Bussick TJ, McNamara JA.,Jr. Dentoalveolar and Skeletal changes associated with the Pendulum appliance. Am J Orthod Dentofac Orthop 2000;117: 333-343.





























