Embed Size (px)
Citation preview
UNICEF communicationfor development support topublic health preparednessand disaster risk reductionin East Asia and the Pacific:A review Young Child Survival and Development SectionUNICEF EAPRO
UNICEF communication for development supportto public health preparedness and disaster risk reductionin East Asia and the Pacific: A review
© UNICEF East Asia and Pacific Regional Office, July 2013
Design and layout: Quo Keen (www.quo-global.com), Bangkok, Thailand
Cover © UNICEF/NYHQ2012-1695/MaitemPage 1 © UNICEF/NYHQ2012-1692/MaitemPage 3 © UNICEF/NYHQ2010-0771/JerryPage 4 © UNICEF/NYHQ2011-1814/PerawongmethaPage 7 Faiz ZakiPage 8 PaulaphotoPage 9 Tamil SelvamPage 10 Muellek JosefPage 21 Stephen BuresPage 24 Warren Goldswain
UNICEF East Asia and Pacific Regional Office19 Phra Atit RoadBangkok 10200 Thailand
Tel: (66 2) 356-9499Fax: (66 2) 280-3563E-mail: [email protected]/eapro
ISBN 978-974-685-144-2
UNICEF communicationfor development support topublic health preparednessand disaster risk reductionin East Asia and the Pacific:A review Young Child Survival and Development Section
UNICEF EAPRO
AADMER ASEAN Agreement on Disaster Management and Emergency ResponseADB Asian Development BankADPC Asian Disaster Preparedness CentreAIDS Acquired immunodeficiency syndrome ASEAN Association of Southeast Asian NationsAusAID Australian Agency for International DevelopmentBCC Behaviour change communicationC4D Communications for developmentCATS Community Approaches to SanitationCBA Community-based analysisCCA Climate change adaptation CIEH Center for Information and Health EducationCRC Convention on the Rights of the ChildDCDM District Disaster Committees for ManagementDFID (UK) Department for International DevelopmentDIP-ECHO Disaster Preparedness-European Commission Humanitarian Aid DeparmentDRM Disaster risk managementDRR Disaster risk reductionEPI Expanded Programme of ImmunizationEAPRO East Asia and the Pacific Regional OfficeGFDRR Global Facility for Disaster Reduction and RecoveryH1N1 Sub-type of influenza AHIV Human immunodeficiency virusIASC Inter-Agency Standing CommitteeICT Information and communication technologyIDRL International Disaster Response LawIEC Information, education and communicationIFRC International Federation of the Red CrossM&E Monitoring and evaluationMNCH Maternal, neonatal and child healthNCDC National Centre for Communicable DiseaseNCDM National Committee for Disaster ManagementNCHP National Centre for Health PromotionNDMO National Disaster Management OfficeNEMA National Emergency Management AssociationNGO Non-governmental organizationOCHA Office for the Coordination of Humanitarian AidODA Official development assistance PCDM Provincial Disaster Committees for ManagementPMTCT Prevention of mother-to-child transmissionPRSP Poverty Reduction Strategy PapersSARS Sudden acute respiratory syndromeUN United NationsUNADF United Nations Development Assistance FrameworkUNCT United Nations Country TeamsUNDP United Nations Development ProgrammeUNFPA United Nations Population FundUNICEF United Nations Children’s FundUNISDR United Nations Office for Disaster Risk ReductionUSAID United States Agency for International DevelopmentWASH Water, sanitation and hygieneWHO World Health Organization
Acronyms
Foreword: The impetus for a strategic review
1. Introduction: Vulnerability in East Asia and the Pacific
1.1 Promoting disaster risk reduction and resilience
2. Preparedness in perspective
3. Communication for development, disaster risk reduction
and public health preparedness
4. The enabling environment
4.1 Global and regional mechanisms and processes
4.2 Donor funding and priorities
4.3 Institutional preparedness
4.4 Public health preparedness
4.5 Providing leadership and coordination
5. C4D and subnational presence
6. Opportunities and recommendations
Bibliography
i
1
3
4
8
10
11
12
14
17
20
21
24
28
Contents
Thematic and technical debates about communication for development (C4D) and related programmatic approaches have evolved rapidly within UNICEF in recent years. Certainly, the use of communication to support development is, and has, always been important; but since 2005, global funding for H1N1 flu and other public health interventions has provided a much needed boost to the role and profile of C4D within UNICEF and among partners.
Participatory, dialogue-based approaches to programming have a long history in social development. There is also a rich, although not well documented or widely understood, history of positive experiences with participatory and dialogue-based development programming as well as with campaign and interpersonal communication-based behaviour change communication.
Among development partners, UNICEF has played a leading role on C4D and community-based programming approaches, even as other United Nations agencies and international non-government organizations increasingly strengthen their own ability to use communications for programmatic as well as advocacy and external relations purposes. Globally and in East Asia and the Pacific, UNICEF undertakes a range of C4D interventions that benefit vulnerable children and families and expands skills and capabilities among communities and local partners. UNICEF is also increasingly engaged with partners in advocacy work aimed at raising the profile of a variety of C4D-related interventions for disaster risk reduction (DRR), prevention and preparedness and in developing both national and subnational capacity for community-based and consultative approaches to improving health and sanitation.
In that light, UNICEF commissioned in 2012 a review of its C4D programming in relation to DRR, preparedness, communicable disease control, institutional systems strengthening and community resilience, as well as programming strategies currently being shaped to reach the most-at-risk, vulnerable and marginalized communities. This was carried out by an international consultant, Mr Karl Spence.
With support from UNICEF country offices, the consultant conducted assessment and fact-finding visits to Cambodia (26-31 August), Lao People’s Democratic Republic (12-17 August) and Mongolia (19-25 August). The purpose was to solicit and contrast the views, perceptions and recommendations of UNICEF colleagues, donors, government and health ministry partners and international NGOs and civil society representatives. Structured, thematically focused and informal discussions were conducted around a range of issues linked to DRR, C4D and health systems challenges and priorities. UNICEF EAPRO is grateful for the contributions of all who participated in the review.
Although regional in perspective, the review draws only on experiences related to UNICEF cooperation in those three countries visited and thus does not reflect the full diversity of contexts and programme responses across the region. Nevertheless, both vulnerability and resilience have some common characteristics in most locations, and the challenges and barriers observed in all three countries visited surface in various forms throughout the region. The insights thus should be useful to a broad audience.
Daniel TooleRegional Director UNICEF East Asia and the Pacific
Foreword: The impetus for a review
i


Although the Asia-Pacific region generated only one quarter of the global gross domestic product, it accounted for 85 per cent of disaster-related deaths and 38 per cent of global economic losses between 1980 and 2009 (UNISDR, 2010).1 The region is confronting a variety of potential, sometimes geographically or event-specific catastrophic scenarios that have grave economic and human consequences, including the very real potential to profoundly undermine fragile social development and human rights gains.2
The potential for communicable disease outbreak remains as considerable as ever, either as a consequence of disaster or as a result of animal-human transmission of zoonotic diseases. A host of underlying factors aggravate problems around communicable disease control, including acute rural and urban poverty, environmental degradation, child malnutrition, urbanization and pollution, poor sanitation and limited access to clean water, and the absence of easily accessible services for the poor.
Recent examples of disaster and potential public health emergencies in East Asia and the Pacific include flooding and drought in Cambodia, Lao PDR and Thailand, earthquakes in China, eruptions and tsunamis in Sumatra, cyclones in Myanmar, dzuds in Mongolia, avian influenza in Indonesia, and foot and mouth disease outbreaks in Cambodia.
Rapid urbanization and poor infrastructure, burgeoning but largely unregulated and often exploitive economic activity, unlawful or exploitive land acquisition, climate change and environmental hazards further exacerbate the level of disaster vulnerability among already impoverished communities and diminish their capacity to sustain livelihoods and maintain physical and psychological well-being.
Within these contexts, C4D strategies can help support programming to reduce vulnerability. For UNICEF, these strategies also offer an entry point and vehicle for child and multilayered human rights-based advocacy across humanitarian and developmental concerns, including DRR and climate change adaptation (CCA). Consequently, and in line with calls from international partners for a greater emphasis on building national, subnational and local capacity for DRR and preparedness, it is prudent to begin assessing the past and future role of UNICEF in promoting and enabling C4D capacities in the region that facilitate cross-sector awareness of preventive strategies.
C4D emphasizes dialogue, empowerment and participation. UNICEF (and partner) C4D capacities should be both integral to the effectiveness of local interventions and approaches, and to meeting broader obligations in relation to the Convention on the Rights of the Child, the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) and other human rights mechanisms.
1. Introduction: Vulnerability in East Asia and the Pacific
1 The damage caused by natural disasters should not be underestimated. Over the 10 years from 2000 to 2009, more than 2.2 billion people worldwide were affected by 4,484 natural disasters. These disasters killed close to 840,000 people and cost at least US$891 billion in economic damage (Kellet and Sparks, 2012). For South Asia and East Asia and the Pacific, flooding, droughts and other weather-related events are by far the most destructive in terms of numbers of affected people; this emphasizes the critical links between DRR and CCA.2 A recent example is post-disaster impoverishment and the impact this has on the capacity of individuals, families and communities to provide and/or access essential services, which in turn has health implications as the cost of services and of service provision becomes prohibitive. Following the 2011 flooding in rural Cambodia, many families were forced to seek loans from short-term money lenders at exorbitant rates – the dire consequences and implications of debt-induced impoverishment require further consideration.
2
1.1 Promoting disaster risk reduction and resilience
In this review, DRR and ‘resilience’ are considered in general, but also more specifically in relation to public health programming and implementation at the national, subnational and local levels. Improving quality, access, use and demand for health (and water and sanitation) services as well as catalysing more resilient public health systems that include appropriate early warning, risk communication protocols and capacity are all integral to DRR and to the broader tenets of resilience: mitigation, prevention, preparedness and response.
In the current fiscal and policy environment, public health preparedness, prevention and response cannot be separated – for practical purposes – from DRR and resilience issues. Agency-generated efforts (such as this review) and collaborative efforts with partners to conceptualize and enliven a resilience approach may generate incentives and resources for a better coordinated, more integrated and more strategically reinforced approach to development programming – at all levels.
Communication for development is a practice already fragmented by discrete funding, individual sector’s expectations and lack of operational autonomy and strategic influence. A more grounded approach to C4D and capacity development, a wider recognition of the potential importance of C4D-based interventions and an improved capture of lessons and local-level results may create a more practical application of participatory and communicative methods and a more realistic appraisal of their efficacy.
Lessons and good practices identified from UNICEF and partner experience can and should be better used to build an accessible and more triangulated evidence base for future objectives and approaches. It will be useful, at the same time, to remain mindful of how past efforts with C4D have been undermined by unrealistic ambitions, the de-politicization of local processes, tokenism, donor pressure for quick implementation and ‘concrete’ results, a top-heavy focus on paradigm building and methodological validation over grass-roots consultation and the absence of sustained institutional, financial and political support.
3

2. Preparedness in perspective
Strategies around DRR, CCA and resilience are communicated via a dizzying array of terminology and acronyms. The following offers a brief overview of the concepts relevant to arguments in this review.
Climate change adaptation (CCA) is gaining currency (including within DRR forums). CCA issues clearly intersect with DRR issues. There is momentum for consideration of DRR that incorporates CCA and vice versa (such as climate-smart disaster risk management3). A focus on resilience presents opportunities to envelope DRR, CCA and systems strengthening interventions in a way that bridges humanitarian and developmental strategies and establishes rallying points for improved collaboration and a platform for advocacy with donors and governments.
The United Nations Office for Disaster Risk Reduction (UNISDR) provides the normative lead for DRR within the broader United Nations system and oversees the operation of the International Strategy for Disaster Reduction.4 UNISDR defines disaster risk as “the potential disaster losses in lives, health status, livelihoods, assets and services, which could occur to a particular community or a society over some specified future time period”. It also notes that the definition “reflects the concept of disasters as the outcome of continuously present conditions of risk”. Disaster risk entails different types of potential losses that are often difficult to quantify; but with knowledge of the prevailing hazards and the patterns of population and socio-economic development, disaster risks can be assessed and mapped. It is important to realize that people do not necessarily have the same perceptions of the significance and underlying causes of different risks.
Addressing vulnerability is a core priority for UNICEF. Evidence shows that children and women, especially poor children and women, are the most deleteriously affected by disasters. As well, fragile developmental gains in health and education can be acutely undermined by disaster and public health risks.5 A disaster thus exacerbates vulnerability and inequity; the greater the vulnerability, the more acutely a disaster impacts on the very capacities that reduce vulnerability and mitigate risk.
The organization’s Core Commitments for Children in Humanitarian Action enumerates the principles, approaches and specific interventions that cover preparedness, response and early recovery and attempt to bridge the gap between development and humanitarian programming. Moving from an emphasis on disaster management to both DRR and resilience, however, will require a deeper interrogation of objectives and processes. Disaster risk management (DRM) is the “systematic process of using administrative directives, organizations and operational skills and capacities to implement strategies, policies and improved coping capacities to lessen the adverse impacts of hazards and the possibility of disaster,” according to the UNISDR (2009) definition. It is “an extension of the more general term ‘risk management’ to address the specific issue of disaster risks. DRM aims to avoid, lessen or transfer the adverse effects of hazards through activities and measures for prevention, mitigation and preparedness.”
This definition is now considered vague, due the term evolving over time. UNICEF currently distinguishes between i) conventional disaster management (preparedness and response), which does not reduce risk, and ii) full-fledged DRR, which focuses on prevention and mitigation of disaster risk. In this perspective, DRM combines all four categories: preparedness, response, prevention and mitigation.
3 For more information, see: http://community.eldis.org/.59e0ccc04 For details of the International Strategy for Disaster Reduction (General Assembly resolution 54/219), see: www.unisdr.org and www.unisdr.org/who-we-are/international-strategy-for-disaster-reduction5 Children typically represent 50-60 per cent of disaster victims; Save the Children estimates that the number of children affected by weather-related hazards will increase from 67 million per year in the late 2000s to 175 million per year in the late 2010s. For UNICEF Asia and Pacific’s latest thinking on child-centred DRR, see: United Nations Children’s Fund, Child-Centred Disaster Risk Reduction: Guidance notes for UNICEF Asia-Pacific, Unpublished manuscript, Bangkok, 2012.
5

Effective preparedness implies the existence of:<–> properly functioning early warning systems and communication links between state and non-state actors;<–> contingency plans, protocols and standard operating procedures;<–> pre-positioning and stockpiling of supplies;<–> arrangements for coordination, evacuation and public information dissemination; and<–> associated trainings and field exercises to test preparedness and response mechanisms.
The related term ‘readiness’ describes the ability to quickly and appropriately respond when required.6
Public health preparedness, or the capacity to address public health crises (and to provide and sustain services), is of course also fundamental to DRR and resilience. UNISDR (2009) defines preparedness as “the knowledge and capacities developed by governments, professional response and recovery organizations, communities and individuals to effectively anticipate, respond to and recover from the impacts of likely, imminent or current hazard events or conditions”. Preparedness actions are carried out within the context of DRM and aim to build the capacities needed to best manage all types of emergencies and to achieve transition from response to sustained recovery. Preparedness must be supported by formal institutional, legal and budgetary abilities and be based on a sound analysis of risks (including communicable disease control risk).
UNISDR (2009) defines resilience as “the ability of a system, community or society exposed to hazards to resist, absorb, accommodate to and recover from the effects of a hazard in a timely and efficient manner, including through the preservation and restoration of its essential basic structures and functions”. It further explains, “Resilience means the ability to ‘resile from’ or ‘spring back from’ a shock. The resilience of a community in respect to potential hazard events is determined by the degree to which the community has the necessary resources and is capable of organizing itself both prior to and during times of need.”
Resilience is associated with the capacity (resources, access to rights, skills and knowledge) of individuals (or a group of people), a community or a society to cope with disasters. Particularly relevant to the UNICEF work at the subnational level are notions of resilience as correlating with local government and community capacity and with social and economic vulnerability. Within this approach – as a minimum – a better understanding of social capital and the machinations of social cooperation (including how local power relations manifest) is fundamental to developing DRR and resilience programming, either as stand-alone interventions or as a part of sector-based approaches. The regular UNICEF focus on reducing vulnerability and developing capacity to cope is already broadly synergistic, with efforts to bolster and support resilience at both the national and subnational levels. What is important now is to manage relations to the varying approaches to resilience, DRR and CCA, and to carve out programmatic niches that provide examples of good practice and an evidence base for advocacy.
A variety of conceptual frameworks can be used for assessing local-level resilience and capacity. Most conceptualize disaster resilience in similar ways and focus on the factors that reduce vulnerability and increase community resilience.7 Those factors include economic resources, assets and skills, information and knowledge, support and supportive networks, access to services and shared community values. Assessing and mapping subnational and community vulnerability and existing resilience are vital for effective programming. It is important that any assessment of community resilience take into account the multitude of interactions between people (including children), communities and governments as well as the political, economic and hazardous environments.
6 Response capacity is causally related to preparedness and also integral to DRR, CCA and disaster and risk management in that effective response mitigates risk and loss, and accelerates recovery, hence bolstering and enabling resilience. However, this analysis is focused on the role of C4D and related strategies via DRR, resilience and preparedness; a comprehensive assessment of both the actual and potential mechanisms and components of UNICEF and partner C4D response capacity is beyond the scope of this review. Suffice to say, C4D preparedness is a reflection on response capacity and vice versa.7 Characteristics of a Disaster-Affected Community: A guidance note, 2007, prepared by the DFID Disaster Risk Reduction Interagency Coordination Group, is a tool widely used by international NGOs and other partners to assess resilience and to assist programme design. It contains excellent detail on characteristics of resilience and on how to plan interventions with communities and local elites. See: See: https://practicalaction.org/docs/ia1/ community-characteristics-en-lowres.pdf or for an updated 2009 version, see: http://community.eldis.org/.59e907ee/Characteristics2EDITION.pdf
6
Vulnerability has many faces. In the context of disasters and threats to public health, UNISDR (2009) defines vulnerability as “the characteristics and circumstances of a community, system or asset that make it susceptible to the damaging effects of a hazard” and is exacerbated – especially for the most vulnerable – “by underlying physical, political, social, economic and environmental factors”. For example, participation and engagement are innately more problematic for the poor and vulnerable, whose access is typically limited by critical livelihood responsibilities, income poverty and diminished social status.
Examples of conditions that exacerbate vulnerability
<–> Poor quality and unregulated building standards. <–> Inadequate system for the protection of assets and land tenure.<–> Lack of public information and/or institutional awareness of the means and capacity to rapidly scale up public awareness.<–> Critical problems with health service delivery.<–> Absence of risk transfer mechanisms and insurance.<–> Limited evidence of adequate government and/or institutional recognition or understanding of risk or preparedness measures, or of their consequences for planning, budgeting and implementation.
7


The academic and institutional literature on the role of communications within DRR and preparedness is extensive. In practice, however, strategic communications for DRR and preparedness remain hampered by old foes: C4D design and implementation tends to encounter systemic challenges, which raise reasonable questions on how C4D is operationalized, existing capacities, the level of attention paid and the funding it attracts.
C4D-related strategies, including participatory and community-based approaches, advocacy at different levels, risk communication and inter-agency, interdepartmental and intergovernmental dialogue, reinforce the effectiveness of DRR and preparedness efforts – as they do for regular social sector programming. (UNICEF country office C4D strategies and participatory approaches to advocacy, social development and DRR are discussed in Sections 4 and 5 of this review)
It can be argued that dialogue-based approaches that address acute vulnerability also can complement DRR and resilience programming. Indeed, C4D and the interactions that its planning and implementation require can help to establish many links between sector actors and discrete health sector interventions and improve the connections across all sectors and programmes. Integral to the mix are access and rights to information,8 ensuring that the design of behaviour change communication (BCC) is cognizant of service access and quality, enabling participation and dialogue between communities and local government, and promoting positive and health-reinforcing behaviours.9
As the UNISDR (2011) Global Assessment Report on Disaster Risk Reduction: Revealing risk, redefining development points out:
“One of the most important drivers of accountability is access to information, particularly to information on disaster risks. However, access to information is only effective when governments actively support the right to information and when citizens are aware of their legal right and are willing to assert it. A culture of social accountability directly improves the effectiveness of governance and service delivery.”
3. Communication for development, disaster risk reduction and public health preparedness
8 For a revealing review of the information rights and needs of disaster-affected communities see BBC World Trust, Left in the Dark: The unmet need for information in humanitarian response, Policy Briefing #2, London, 2008. Available at: http://downloads.bbc.co.uk/worldservice/trust/pdf/ humanitarian_response_briefing.pdf9 UNICEF, WHO and other development partners have published a variety of programme guidance and policy briefings on the role of communications within preparedness and on risk communication protocols and priorities, in addition to a wealth of material on the role of C4D in emergencies. Covello (2003) and Glick (2007) provide excellent reviews of risk communication protocols, theory and good practice. Available at: www.asph.org/userfiles/ Competencies-Resources/37_GlikRC.pdf and http://classweb.gmu.edu/gkreps/705/readings/008.%20Covello,%20Best%20Practices.pdf
9

4.1 Global and regional mechanisms and processes
The Hyogo Framework for Action 2005-2015 is an overarching multilateral and intergovernmental agreement on DRR that explains, describes and details the work that is required from different actors to reduce disaster losses.10 Subtitled Building the Resilience of Nations and Communities to Disasters, the agreement was endorsed by 168 governments participating in the World Conference on Disaster Reduction in Japan in 2005 and by the United Nations General Assembly. According to UNISDR, the Hyogo Framework prescribes “priorities for action and offers guiding principles and practical means for achieving disaster resilience”. Its goal is “to substantially reduce disaster losses by 2015 by building the resilience of nations and communities to disasters” (UNISDR website).11
Reinforcing the Hyogo Framework is the ASEAN Agreement on Disaster Management and Emergency Response (AADMER), signed by the ASEAN foreign ministers in 2005 and ratified in 2009. AADMER is the first-ever Hyogo Framework-related DRR instrument to be agreed that is legally binding regionally. It affirms the ASEAN commitment to the Hyogo Framework and the measures that will be used to support its implementation.
Even though both the Hyogo Framework and the AADMER implicitly address public health preparedness, the International Health Regulations (of the World Health Organization) focus specifically on public health preparedness. After the emergence of severe acute respiratory syndrome (SARS), the World Health Assembly established an intergovernmental working group in 2003 to review and recommend a draft revision of the International Health Regulations, which were adopted in 2005 and entered into force in 2007. The Regulations are used “to prevent, protect against, control and provide public health responses to the international spread of disease in ways commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade” (WHO, 2010).12
In the context of communicable disease control and regional public health security, the 2005 WHO Asia Pacific Strategy for Emerging Diseases recognizes eight focus areas for prioritized technical and financial investment: surveillance, risk assessment and response; laboratories; zoonoses; infection prevention and control; risk communication; public health emergency preparedness; regional preparedness, alert and response; and monitoring and evaluation.
4. The enabling environment
10 For a full list of organizations and programmes that support the Hyogo Framework objectives see: www.preventionweb.net/english/hyogo/progress/ priority1/?pid:22211 The five priority actions under the Hyogo Framework are: i) Ensure that DRR is a national and a local priority with a strong institutional basis for implementation; ii) identify, assess and monitor disaster risks and enhance early warning; iii) use knowledge, innovation and education to build a culture of safety and resilience at all levels; iv) reduce underlying risk factors; and v) strengthen disaster preparedness for effective response at all levels. See: www.unisdr.org/we/coordinate/hfa12 The 2005 International Health Regulations cover: i) a scope not limited to any specific disease or manner of transmission but covering “illness or a medical condition, irrespective of origin or source that presents or could present significant harm to humans”; ii) state party obligations to develop certain minimum core public health capacities; iii) obligations on states parties to notify the World Health Organization (WHO) of events that may constitute a public health emergency of international concern, according to defined criteria; iv) provisions authorizing the WHO to take into consideration unofficial reports of public health events and to obtain verification from state parties; v) procedures for the determination by the WHO director-general of a “public health emergency of international concern” and issuance of corresponding temporary recommendations after taking into account the views of an emergency committee; vi) protection of the human rights of persons and travellers; and vii) the establishment of national focal points and WHO contact points for urgent communication between States parties and the WHO.
11
4.2 Donor funding and priorities
Although the proportion of official development assistance (ODA) linked to DRR programming represents a small percentage of total humanitarian assistance, major donors have an increasing interest in, and engagement with, DRR and related programming, especially the United Kingdom’s Department for International Development (DFID), the Australian Agency for International Development (AusAID), the European Commission (through the European Commission Disaster Preparedness Programme), the Swiss Agency for Development and Cooperation and the United States Agency for International Development (USAID).
Of particular interest are DRR and CCA-related capacity development across legislative and policy forums. The World Bank (through its Global Facility for Disaster Reduction and Recovery) and the Asian Development Bank (ADB) are also investing in DRR and CCA and working to expand their own technical capacity and policy influence.
Although trends in the financing for DRR to the top 40 recipients of humanitarian assistance seem upon first impression positive, funding for DRR represents a very small proportion of the overall development assistance spent in those same countries.13
Funding for CCA has been similarly lacklustre, and even in the Asia-Pacific region, which has received the most funding, it covers only a fraction of the anticipated need. The World Bank estimates that from 2010 to 2050, the cost of CCA will be US$22.25 billion for the Asia-Pacific region. Nonetheless, the Climate Funds Update website reports that only a total of US$1.73 billion for Asian countries was approved between 2004 and October 2011 from dedicated climate funds. Approximately US$866 million of this approved funding has been disbursed, including US$60 million in 2011 (Nakhooda, et al., 2011). The Government of Japan has since 2003 pledged 51 per cent of all CCA-related funding, followed by Great Britain, at 16 per cent and the United States, at 8 per cent (Climate Funds Update, 2013).
Funding for both DRR and CCA is also not always, or even usually, commensurate with a country’s needs and vulnerabilities. For example, 22 Small Island Developing States and least developed countries are located in the Asia-Pacific region; their low-lying coastlines, remoteness and exposure to weather-related hazards leave them particularly vulnerable to climate change risk (even though they contribute less than 1 per cent of global greenhouse gas emissions) (Climate Funds Update, 2013).
A comparison of data relating to the effects of flooding and flooding-related DRR expenditures received is also revealing. Although the top 40 ODA recipients regularly account for the largest proportion of deaths due to flooding (even before the massive Pakistan flood of 2010), and in many years for a sizeable proportion of the people affected, DRR funding frequently goes to countries outside the top 40 ODA recipients. Only in 2000 and 2001 did the top 40 ODA recipients receive more than 50 per cent of all flood-related DRR funding. From 2003 to 2009, the figure never crept above 38 per cent; in 2005 it was only 6.7 per cent. Clearly, as is often the case, geo-political concerns are tempering the preferences of donors (Climate Funds Update, 2013).
Despite funding shortfalls, however, there does appear to be a strong and growing donor interest in funding DRR and CCA-related interventions (particularly within the ADB and the World Bank, both of which have prominence in mobilizing and leveraging resources for disaster risk and climate action) and through preferential loans. Currently, multilateral banks are in the process of harmonizing their climate finance tracking systems and recently finalized a joint approach for mitigation finance reporting. A Joint Report on Mitigation Finance for 2011 was released, and the ADB and World Bank both engaged in a parallel effort to develop a joint approach for adaptation finance tracking that was presented during the 2012 UN Climate Change Conference in Doha, Qatar (in December).14
13 In East Asia and the Pacific, only Cambodia, Indonesia, the Philippines and Viet Nam are among the top 40 ODA recipients. For a ranked list of the top 40 ODA recipients from 2000-2009, see Global Trends, Disaster Risk Reduction: Spending where it should count, 2012. Available at: www.globalhumanitarianassistance.org/wp-content/uploads/2012/03/GHA-Disaster-Risk-Report.pdf NB: This report appears to be the only publicly available assessment of DRR funding as a percentage of total humanitarian assistance and ODA. This report notes the extreme complexity of disentangling aid flows and determining the level of investments in DRR. Data on the total funding for DRR in the East Asia and Pacific region and national data within Cambodia, Lao PDR and Mongolia are currently unavailable; what data is available has not as yet been systematically assessed. 14 For more details, see: http://climatechange.worldbank.org/sites/default/files/MMF_2011_version_21.pdf
12
Donor priorities within humanitarian assistance funding continue to show a preference for response over risk reduction, despite the need for increased investment in mitigation and preparedness. Nevertheless, all major donors and multilateral agencies recognize and articulate the importance of resilience and have exhibited a clear interest in programming that bridges CCA, DRR and humanitarian concerns.
DFID has been leading debates about resilience and where it fits within DRR and CCA programming. In February 2012, DFID released a strategy paper set within the context of its “commitment to go beyond a focus on responding to crises and to invest in approaches that promote resilience”.15 A core focus of the strategy is to work with policymakers and practitioners to deepen their understanding of the concept and application of resilience, particularly in fragile and conflict-affected situations. AusAID also has an interest in DRR; according to its website, “Much can be done to minimise the impacts of natural disaster” and, importantly, “in order to be sustainable, key sectors of development – such as health, education, water and sanitation, and food security – must ensure that their activities and infrastructure are disaster-resilient”.16
Donor interest in DRR and CCA is concurrent with and potentially complementary to the ongoing UNICEF child- and human rights-based advocacy and sector programming. Community and dialogue-based approaches should be embraced but with the realization that these need sustained investments of time and resources. They also need the articulation of measures of progress, which are more qualitative in nature and less tangible as visible development products. It will be useful to invest in clearly communicated and profiled information and analytical narratives on how UNICEF can add value through the work with partners to facilitate DRR, improve resilience and reduce vulnerability.
Management and human resource issues
C4D capacity in UNICEF is critical to meet the demands of participatory methodologies, which are more difficult to design, implement and evaluate than simple awareness campaigns. It is equally important to invest in personnel capacities and activities when looking to build up the resiliency of communities.
Considering the equity agenda and the emphasis placed on C4D and on local dialogue-based interventions, it is still surprising that these approaches are so critically under-resourced. In addition to providing core support to programmes and representing a set of capacities that have implications in terms of rights to participation and information and in relation to corporate management and external relations, C4D could – if enabled – serve to build bridges across programmes (including, across components within health sector programming) and to support improved collaboration and communication at all levels of country programme design, implementation and evaluation.
In the context of funding opportunities, investments could be made to improve the sourcing and presenting information in a manner that responds to donors’ concerns and UNICEF obligations to promote rights to participation and self-determination. ‘Building resilience’ offers an opportunity to package social sector development programming in a way that supports, in tandem, DRR, preparedness and integrated local service delivery capacity. Understanding local contexts and proposing interventions within these contexts will help ensure both their credibility and viability.
15 For more details, see: www.dfid.gov.uk/Documents/publications1/prom-innov-evi-bas-appr-build-res-resp-hum-cris.pdf16 For more details, see: www.ausaid.gov.au/aidissues/drr/Pages/default.aspx
13
4.3 Institutional preparedness
Establishing and supporting institutional and legal mechanisms that embrace DRR and preparedness is critical work. UNISDR noted in 2009 that significant progress has been made in strengthening capacities, institutional systems and legislation to address deficiencies in disaster preparedness and response (UNISDR, 2009).
To a varying extent, all countries in East Asia and the Pacific have made some progress towards developing institutional mechanisms for DRR and disaster management and are making progress towards implementing the International Disaster Response Law (IDRL) Guidelines, which cover DRR matters. A full consideration of progress towards national preparedness and DRR capacity in the region was beyond the scope of this review; however, the institutional barriers to national and subnational preparedness in Cambodia, Lao PDR and Mongolia reflect the broader regional and systemic issues that impede progress across the region.17
For risk-informed planning and programming, seismic, hydrological or climate-related data, combined with quantitative data indicative of vulnerability and systemic weaknesses and deficits, can help in assessing hazard and risk. Additionally, a deeper and more nuanced understanding of risk requires consideration of the less understood and locally specific causes of vulnerability and their patterns.
The IFRC and UNDP efforts in all three countries have resulted in the use of the IDRL Guidelines and the preparation and/or refinement of appropriate legal mechanisms. DRR and disaster management are currently covered in all three countries by a variety of decrees and orders, but there is a need to strengthen and streamline the legal preparedness by developing and adopting comprehensive DRM laws.18
The following table outlines the institutional progress in each of the three countries.
Interventions across the three countries
Fairly typical of DRR interventions undertaken by international NGOs is the recent Reducing Multi Hazard Induced Risks and Building Community Resilience to Disaster in Cambodia, implemented by Danish Church Aid, Concern and ActionAid (with funding from the European Commission’s Disaster Preparedness Programme). The project aimed to strengthen disaster management capacity through joint actions to raise awareness of DRR preparedness and boost local capacities for disaster planning and response, and to implement mitigation measures with communities and schools. Other initiatives in Cambodia include Plan International’s child-centred approaches to DRR and CCA; CARE’s integrated DRR and livelihood projects in cooperation with local authorities and Village Development Committees; and projects under the AusAID Humanitarian Partnership Agreement via a consortium of NGOs, including CARE Australia, Caritas Australia, Oxfam Australia, Plan International, Save the Children Australia and World Vision Australia.
In all three countries there is a range of DRR and CCA programmes and projects funded by ADB, the World Bank, the Government of Japan, the USAID Millennium Challenge Account (mostly simulation exercises) and the European Union. Many of them focus on the rehabilitation of infrastructure or provide technical assistance for CCA, multilateral information sharing and the strengthening of warning systems.19
17 The Guidelines for the Domestic Facilitation and Regulation of International Disaster Relief and Initial Recovery Assistance (IDRL Guidelines) were unanimously adopted in 2007 by State parties to the Geneva Convention and the International Red Cross Red Crescent Movement at the 30th International Conference of the Movement. In 2008, the UN General Assembly adopted three resolutions (Res. 63/139, 63/141 and 63/137) encouraging States to make use of them. The IDRL Guidelines were designed to assist governments to become better prepared for the common legal problems in international response operations. For more details, see: www.ifrc.org/PageFiles/53419/MAA0000411myr.pdf18 The IFRC and UNDP are working on a joint project to research, compare and consult on the efforts of various countries to strengthen how their laws support the reduction of disaster risks, particularly at the community level. A synthesis report of the findings is expected in the first quarter of 2013. See: www.ifrc.org/en/what-we-do/idrl/about-disaster-law/legislation-for-disaster-risk-reduction/law--drr/--drr/19 For a reasonably comprehensive list of DRR projects in the Asia–Pacific region, see: www.drrprojects.net/drrp/drrpp/project/list
14
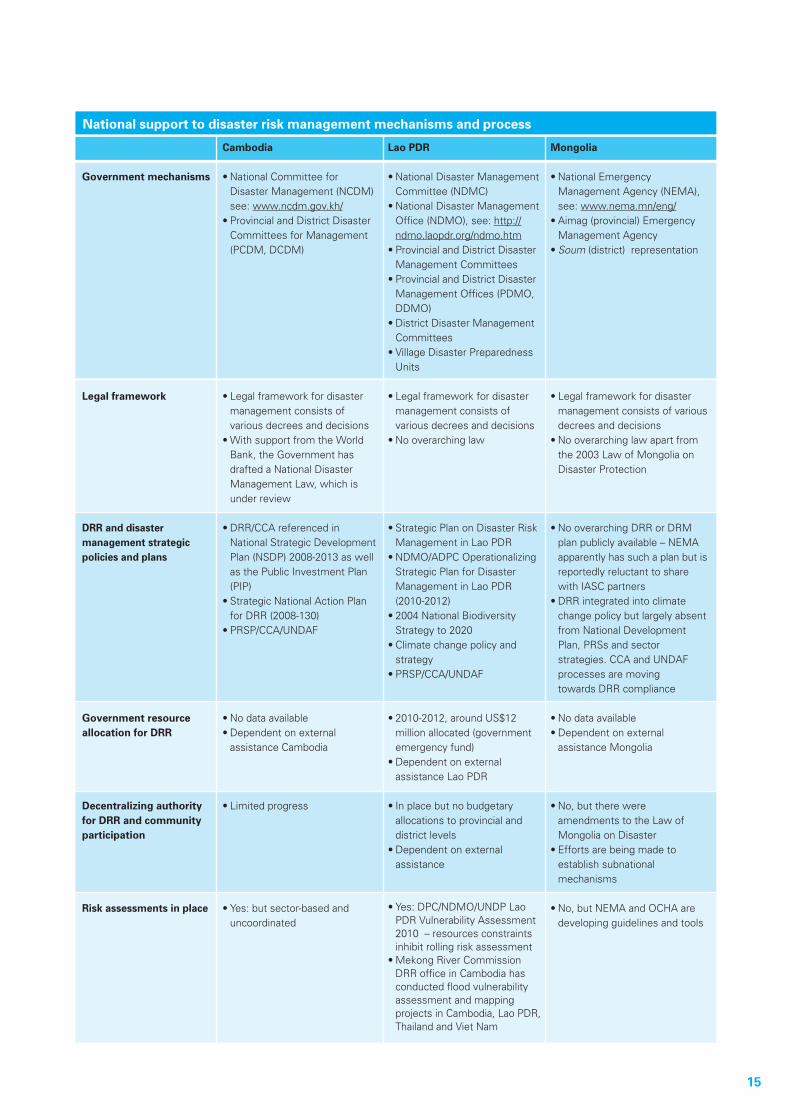
Government mechanisms
Legal framework
DRR and disaster management strategic policies and plans
Government resource allocation for DRR
Decentralizing authority for DRR and community participation
Risk assessments in place
National support to disaster risk management mechanisms and process
Cambodia
•NationalCommitteefor Disaster Management (NCDM) see: www.ncdm.gov.kh/•ProvincialandDistrictDisaster Committees for Management (PCDM, DCDM)
•Legalframeworkfordisaster management consists of various decrees and decisions •WithsupportfromtheWorld Bank, the Government has drafted a National Disaster Management Law, which is under review
•DRR/CCAreferencedin National Strategic Development Plan (NSDP) 2008-2013 as well as the Public Investment Plan (PIP)•StrategicNationalActionPlan for DRR (2008-130)•PRSP/CCA/UNDAF
•Nodataavailable•Dependentonexternal assistance Cambodia
•Limitedprogress
•Yes:butsector-basedand uncoordinated
Lao PDR
•NationalDisasterManagement Committee (NDMC)•NationalDisasterManagement Office (NDMO), see: http:// ndmo.laopdr.org/ndmo.htm•ProvincialandDistrictDisaster Management Committees•ProvincialandDistrictDisaster Management Offices (PDMO, DDMO)•DistrictDisasterManagement Committees•VillageDisasterPreparedness Units •Legalframeworkfordisaster management consists of various decrees and decisions •Nooverarchinglaw
•StrategicPlanonDisasterRisk Management in Lao PDR•NDMO/ADPCOperationalizing Strategic Plan for Disaster Management in Lao PDR (2010-2012)•2004NationalBiodiversity Strategy to 2020•Climatechangepolicyand strategy•PRSP/CCA/UNDAF
•2010-2012,aroundUS$12 million allocated (government emergency fund)•Dependentonexternal assistance Lao PDR
•Inplacebutnobudgetary allocations to provincial and district levels•Dependentonexternal assistance
•Yes:DPC/NDMO/UNDPLao PDR Vulnerability Assessment 2010 – resources constraints inhibit rolling risk assessment •MekongRiverCommission DRR office in Cambodia has conducted flood vulnerability assessment and mapping projects in Cambodia, Lao PDR, Thailand and Viet Nam
Mongolia
•NationalEmergency Management Agency (NEMA), see: www.nema.mn/eng/•Aimag(provincial)Emergency Management Agency•Soum (district) representation
•Legalframeworkfordisaster management consists of various decrees and decisions•Nooverarchinglawapartfrom the 2003 Law of Mongolia on Disaster Protection
•NooverarchingDRRorDRM plan publicly available – NEMA apparently has such a plan but is reportedly reluctant to share with IASC partners•DRRintegratedintoclimate change policy but largely absent from National Development Plan, PRSs and sector strategies. CCA and UNDAF processes are moving towards DRR compliance
•Nodataavailable•Dependentonexternal assistance Mongolia
•No,buttherewere amendments to the Law of Mongolia on Disaster•Effortsarebeingmadeto establish subnational mechanisms
•No,butNEMAandOCHAare developing guidelines and tools
15

Early warning systems functioning
National platform for DRR
Protocols and systems for DRR information sharing
Public awareness strategy that includes outreach
Social policies that reduce vulnerability
Partners
National support to disaster risk management mechanisms and process (continued)
Cambodia
•DepartmentofHydrology and River Work reviews, maintains and disseminates flood and weather forecasts
•Yes:DRRForum,althoughlinks with NCDM and PCDMs apparently are limited
•Noformalcommunication systems or protocols•Ad hoc communication through NCDM to PCDM and DCDM •DRRforum
•Noformalstrategy,only ad hoc government and partner interventions to raise awareness
•Nosystematicinsuranceor modalities for cash transfers, limited microfinance access
•WorldBankGFDRR,ADB, ADPC, UNCT, DIP-ECHO
Lao PDR
•DepartmentofMeteorology and Hydrology provides flood forecasting along the Mekong and main tributaries during the monsoon season from June to October
•Nascenteffortsunderwayby NDMC and IASC to establish multi-stakeholder DRR forum •NDMO is responsible for further dissemination of information to DM committees at local levels (PDMCs and DDMC), usually undertaken via fax and telephone and to VDPUs and all communities at risk
•Noformalstrategy,only ad hoc government and partner interventions to raise awareness
•Nosystematicinsurance, modalities for cash transfers, limited microfinance access
•WorldBankGFDRR,ADB, ADPC, UNCT
Mongolia
•No,capacityforseismicanalysis also very limited
•Establishedandfirstmeeting on 6 June 2012
•Noformalcommunication systems or protocols•Ad hoc communication through NEMA to aimag and district levels•DRRforum
•Noformalstrategy
•Nosystematicinsuranceor modalities for cash transfers, limited microfinance access
•WorldBankGFDRR,ADB,UNCT
Misplaced priorities in Mongolia
The International Federation of the Red Cross’ projects and programmes in Mongolia cover vulnerability and capacity assessment, primary and secondary school risk reduction and strengthening the DRR legal framework to support national and subnational activities. It has supported community-based disaster preparedness programmes, aiming at increased knowledge, awareness and practice of locally appropriate disaster preparedness, protection and mitigation methodologies to bolster resilience and protect livelihoods. Engagement with herder communities to develop solutions that include building snow breaks, water kiosks and water distribution centres for flood- and drought-affected communities and establishing firefighting teams is ongoing.
According to an IFRC officer, however, there has been too much focus on rural DRR when rapid urbanization and poor quality construction have made Ulaanbaatar acutely vulnerable to earthquake-related disasters.
16

4.4 Public health preparedness
Progress towards ensuring public health preparedness has followed a similar trajectory as DRR in Cambodia, Lao PDR and Mongolia in that it has been promoted in relation to a binding multilateral framework (the International Health Regulations) and has suffered from similar resource and capacity constraints. Following concerns about SARS and avian influenza in the mid-2000s, however, there has been a focused effort to support preparedness for communicable disease control and for communication approaches that raise risk awareness.
The World Health Organization and major donors (such as the World Bank, USAID and the Government of Japan) have strongly pushed for H1N1 flu and pandemic preparedness interventions, with the WHO providing technical assistance to health ministries. The Food and Agriculture Organization of the United Nations is doing similar with agriculture ministries. Amid these preparedness efforts, the UNICEF role has been to support the ability of health ministries to institutionally support social change and dialogue-based interventions (radio talk shows on H1N1, for example) and to oversee the design, testing and use of materials, including radio and television public service announcements, leaflets, banners and flyers. Because funding for H1N1 has waned, it has proven challenging for UNICEF to maintain institutional capacity development strategies for health and risk communication in Cambodia, Mongolia and Lao PDR (and undoubtedly in other countries).
Continuing efforts – albeit on a reduced scale – to build capacity and channel additional outreach and a range of behaviour change communication and information interventions through health ministry agencies charged with health communication responsibilities seem to be faltering. With hindsight, it seems that a critical mass of investment in information, education and communication (IEC) production and dissemination was needed to mobilize and engage what are otherwise underfunded and marginalized health ministry functions.
Health departments with nominal responsibilities for promoting health and risk awareness were once enlivened and strengthened with avian influenza and pandemic interventions (as well as by efforts to revitalize primary health care approaches in the early 2000s) but are now floundering without active and budgeted public health communication strategies to implement.
In all countries, there were repeated reports that nominally vertical health ministry programmes, such as HIV/AIDS, Expanded Programme of Immunization (EPI) and maternal and child health, typically bypass health promotion and communication departments, and undertake their own campaigns and trainings to promote behaviour change and disseminate information. Inversely, it appears that when H1N1 and communicable disease control funding was relatively abundant and avian influenza C4D implementation was in full swing, the health promotion and communication departments were engaged and activated, their interdepartmental influence was wider and their advice more frequently sought.
Interpersonal communication development for front-line health workers (such as ongoing and cascade trainings that include interpersonal and risk communication) are considered an integral part of diffusion and BCC interventions, and can – and should – critically support disease surveillance, early warning and risk communication at the subnational levels. Sustained interpersonal communication capacity development, however, is usually resource intensive and often proves difficult to maintain for a variety of complicated reasons, including high rates of attrition, critical human resource complications and deficiencies within the health sector. Consequently, adequate and properly resourced approaches to building such skills and motivation are at times jettisoned under pressure to develop and disseminate behavioural information messages, preferably through physical mediums that, in and of themselves, communicate tangible evidence of action to donors and partners.
Preparedness constraints
In all three countries, communication capacity underpins health preparedness but is marred by the absence of clearly defined departmental mandates and standard operating procedures for risk communication as well as by deep financial and technical resource deficits. Risk communication and public outreach are not institutionally well understood, with interventions almost always externally supported and focused on IEC dissemination.
17

Health system strengthening and convergence
Too little attention and focus is paid to the working conditions and concerns of often overburdened front-line health workers (nurses, auxiliary nurses, midwives), the role and effectiveness of village health committees and/or other community mechanisms and the usefulness of unpaid village health workers and/or other community programme focal points who are stretched by obligations and requests to undertake community outreach without adequate support.
Similarly, a more collaborative, dynamic and purposeful approach to strategic communications, C4D and dialogue-based approaches offers UNICEF internal opportunities to build links, facilitate programme integration where appropriate and engender a more communication-focused and responsive country programme.
BCC and campaign-based public health interventions that can include a combination of social mobilizing strategies, mechanisms for media engagement, health worker training and community participation are UNICEF’s bailiwick and make a tremendous contribution to reductions in morbidity and mortality globally, and across the region.
Schools have served as an effective entry point for a range of WASH and resilience interventions. Yet, the significant opportunities presented by health and education sector collaborations for youth empowerment, community mobilization, DRR, public health preparedness – and to support health communication and literacy more generally – seem to receive little concerted attention.
Progress
Despite endemic resource constraints, progress has been made towards DRR and in relation to preparedness and communicable disease control. This includes increased awareness among government and development partners about the need for effective risk communication and the broader role that communication strategies (including interpersonal communication-based strategies) can and should have within preventive health strategies. But if national and subnational health sector capacity for health and risk communication is to further improve, a closer examination of local-level achievements, process and barriers is needed. For example:
Cambodia
Avian influenza provided the impetus for public health preparedness interventions and the development of a National Comprehensive Avian and Human Influenza Plan in 2007. Cambodia does not yet have a comprehensive legislative framework for communicable disease control, and the regulations that do exist lack binding legal authority. The Ministry of Health, however, developed a Health Strategic Plan, which is currently in its second phase (spanning 2008-2015). One of its three goals is to “reduce mortality and morbidity of communicable disease in Cambodia”, including by reducing the occurrence of communicable diseases, whether they be vaccine preventable, emerging or re-emerging. The National Centre for Communicable Disease Control is the lead agency with the Ministry of Health on preparedness but it has limited authority and capacity when it comes to enabling effective risk communication.
The National Centre for Health Promotion (NCHP) was supported for H1N1 communication interventions, to undertake capacity development for primary health care approaches in the early 2000s and, more recently, for maternal, neonatal and child health (MNCH) BCC interventions.20 But the NCHP remains focused on IEC materials and unable to step up to a more strategic role within the Ministry of Health. The NCHP, sister departments in other countries and development partners also have been unable to sustain momentum around primary health care approaches, which focus on systematically building (and supporting with appropriate health systems development) health worker interpersonal communication capacity, as was envisaged under a now defunct primary health care framework in Cambodia (and in many other developing countries).21
20 In the early 2000s the European Commission promoted and supported primary health care approaches in Cambodia – a draft policy and implementation guidelines were completed but efforts to address primary health care systems development faltered, with some partners arguing that the approaches were too comprehensive and that this undermined prioritization. 21 NB: The term ‘primary health care’ is being increasingly used with a seeming lack of awareness about its main tenets (as articulated in the 1978 Alma Ata Declaration, for example), principles and history in post-war development. A jumble of disease control programmes, MNCH and EPI interventions implemented through various local service providers, and with various levels of efficacy, is not primary health care, even if interventions do start to intersect at facilities by default rather than design.
18

The National IEC Coordinating Committee within the NCHP is mostly – sometimes only – active when mandated and financially supported to undertake IEC commodity-based interventions; as has been the case in other countries, its authority to strategically guide health promotion and education efforts continues to be hampered by vertical programmes that direct funds under its control for the development of materials and trainings as they and their patrons consider appropriate.
In recent years, UNICEF has been a driver of efforts to build national health promotion capacity. But internal and extraneous influences (many beyond UNICEF control) have at times undermined the external support to the institutional strengthening for sector-wide strategic health communication. There has been inadequate investment in the development of structured risk communication capacity, the testing of operational protocols and standard operating procedures and efforts to instil dedicated human resources within the Ministry of Health structure for promoting health-seeking behaviours and for internal advocacy for the necessary supportive policies and enabling budgets.
Lao PDR
Momentum generated by SARS led to the formation of a National Coordination Committee on Communicable Diseases. When also confronted with the threat of avian influenza, the Government created the National Avian and Human Influenza Coordination Office in 2006. The National Centre for Laboratory and Epidemiology is responsible for surveillance, investigation and laboratory diagnosis of communicable diseases and is the International Health Regulations national focal point.
In 2006, the Government finalized the National Avian Influenza Control and Pandemic Preparedness Plan, which was developed with assistance from a United Nations interagency team to strengthen the prevention of and response to potential outbreaks in both animals and humans. In addition to the avian influenza plan, a detailed National Pandemic Influenza Response Plan for the Health Sector was prepared in December 2007. This plan is specifically directed to the health sector’s response to a WHO declaration of a phase 6 pandemic; thus, it is intended for use in conjunction with a broader disaster management plan addressing the non-health sector response to a communicable disease emergency. The components of the Response Plan are divided into the following areas: coordination and decision-making; surveillance and reporting; public health measures; essential health services; and communications.
UNICEF supported the Centre for Information, Education and Health (CIEH) with its communication interventions to prevent avian to human transmission of H1N1 in 2006 and 2007. UNICEF has since attempted to work with CIEH on a range of interventions, including communications work for exclusive breastfeeding and other MNCH priorities.
The momentum correlated with H1N1 interventions has dwindled, however, and UNICEF now struggles to gain traction with the CIEH on its potential role within the UNICEF/UNFPA/WHO joint programme on MNCH and within health systems reform more generally. Recently, UNICEF suggested supporting CIEH to undertake an internal capacity review, but the suggestion has yet to attract critical support within the Ministry of Health.
Mongolia
The National Centre for Communicable Disease (NCDC) is nominally responsible for preparedness, although as in Cambodia and Lao PDR, responsibility is fragmented across health sector capacities and vertical functions. Other agencies with public health preparedness responsibilities include the National Emergency Management Authority, the Department of Veterinary Services of the Ministry of Food and Agriculture, and provincial and district counterparts. Responding to the threat posed by avian influenza, the Government in 2007 prepared a three-year National Strategy and Action Plan for Avian and Human Pandemic Influenza, which has – as in other countries – served as the default setting for general preparedness in relation to all communicable disease. Recently, the NCDC established a cross-sector risk communication forum; the WHO is assisting in the development of a Public Health Emergency Plan in compliance with the International Health Regulations requirements.
In recent years, trainings have been provided on media relations and crisis communications. Additionally, sustained efforts to build institutional capacity for risk communication have resulted in the establishment of risk communication committees and forums as well as the integration of risk communication priorities within broader preparedness activities.
19
In combination with other capacity-improving activities, including the strengthening of subnational surveillance, these efforts generally have not sustained the bottom-up, top-down and horizontal flows of health information and dialogue needed to achieve a genuine communications readiness or develop sector-wide capacity for a rapid scaling up of risk communication and public outreach. Ultimately, though, this reflects much more on the acute structural and resource problems within the health system and their underlying causes than it does on a failure of developmental interventions.
Mongolia’s Department of Health Promotion, although well regarded, was never adequately funded and supported to undertake interdepartmental and cross-sector capacity development within the Ministry of Health. Now that the department no longer exists within the Ministry structure, vertical disease control programmes manage health promotion and communication along with a recently established Health Promotion Foundation. Focused on non-communicable diseases, the Health Promotion Foundation is nominally independent of the Ministry of Health structures and has access to new and significant streams of revenue from recently introduced taxes on tobacco and alcohol.
What to do with that taxation revenue is an issue gripping the attention of the health ministry apparatchiks across former Soviet health systems in Europe and Central Asia in recent years. In Mongolia, where non-communicable diseases (such as cancer and heart disease) are on the rise, the Health Promotion Foundation increasingly focuses on health promotion on such diseases; but across Central and Eastern Europe and the Commonwealth of Independent States and in Mongolia, revenues from new taxes have not been consistently passed on to institutions or health departments with responsibility for preventive health.
4.5 Providing leadership and coordination
Thematic leadership for C4D by UNICEF can be further strengthened by simultaneously working both on advocacy with duty bearers for influencing upstream policy as well as enhancing understanding and knowledge among the right holders. Improving awareness and capacities among children, their caregivers and social service providers can assist in withstanding better the impact of disasters and/or avoid negative the consequences of diseases.
UNICEF is about to conclude a position paper on resilience that will provide a framework with clear objectives and proposed methodologies. This hopefully can also assist by providing guidance through a clear agency-wide commitment.
Although UNICEF does implement dialogue-based approaches, it is, at the core of its mandate, an intergovernmental organization with responsibilities to build national and subnational government capacity. As such, it may be wise to focus less on the actual implementation of C4D and dialogue-based programming and instead concentrate more on understanding (culturally and historically) how these programmes add value to social development and the role of partners and their technical needs. As well, UNICEF should look at how it can reconfigure its efforts in such a way that it increasingly functions as a technical and knowledge hub for C4D and dialogue-based approaches, globally, regionally and within countries.
Finally, additional efforts should be made to overcome a gap between organizational commitment by UNICEF about C4D and sustained human and financial resource allocation. With support by leadership in their offices, C4D colleagues should step up to proactively pursue cross-sector fundraising. To ensure C4D is pursued in a multi-sectoral fashion, country office priorities should be agreed, in relation to how communication and community-based approaches can best support programme results. Longer-term C4D capacity strengthening and behaviour change needs should also be factored in.
Certainly UNICEF provides informal leadership in many contexts, but it has not yet stepped up to the full implications of an overtly articulated C4D stewardship and to reach its full potential to influence policy setting by Governments and empower services providers to be a conduit to improve the lives of children and women.
20

Institutional progress towards DRR – patchy as it is – and the level of discussion around DRR, CCA, preparedness and resilience is at least testimony to the active interest and commitment of many development partners to ensuring appropriate protocols and functional systems at the national, and to a lesser extent, subnational levels. Although representing the roll-out of an important suite of interventions, they are also indicative of the top-heavy channelling of what are already limited resources. This, it could be argued, has been necessary in recent years to establish functioning systems, however rudimentary and despite systemic weaknesses within them or specific mechanisms.
Nonetheless, in 2009 the Global Network of Civil Society Organisations for Risk Reduction published the findings from a survey of local government, civil society and community representatives in 48 countries that revealed a “significant gap between national and local action” with “reports of progress fading as activities get closer to vulnerable people”. The lowest scores were attributed to the level of attainment of community participation in decision-making. The findings also indicated that “many governments have legislation and to some extent structures in support of decentralized ways of working – but with huge gaps in implementation and working culture” (Global Network, 2009). Similarly, internal surveys of the IFRC (2010) found that “national prioritization and profiling is not translating into community-level actions, with very limited community participation in national decision-making”.
Previously there was too much focus among partners on national enabling environments for DRR, preparedness and public health-related programming and too little consideration of the enabling and disabling factors at the subnational level, including local government. A somewhat recent DFID-funded review of DRR programming noted (2011):
“...efforts are focused on managing projects at the grass-roots, community level and/or carrying out high-level advocacy for policy change; but the local and ‘middle’ levels of government tend to be neglected. This is a significant omission, since it is widely acknowledged that local and other subnational levels of government play important roles in risk reduction. Greater emphasis on these levels could be a key to sustainability and scaling up community-based initiatives.”
Rather than attempt to describe and analyse the array of various subnational interventions, it is more useful to look at some of the challenges faced and examples of good practice. Indeed, simply quantifying, assessing and evaluating the full range of UNICEF and NGO approaches and their convergences, contradictions and efficacy in relation to DRR and resilience is, and should be, a significant and ongoing task within countries.
Top-down prioritization: The generally top-heavy prioritizing of C4D interventions, which runs against notions of local-level self-determination, and inputs to programme design, implementation and evaluation were cited during the review interviews as constraints. Programme interventions that include C4D and dialogue-based approaches are usually driven by donor priorities, which in turn steer the prioritizing at the national level. In a similar vein, too little emphasis is placed on subnational enabling environments and in assuring that local governments are encouraged and supported to engage productively in programme implementation and evaluation.
International NGOs, particularly Save the Children, Oxfam, Action Aid, Concern, Plan International, Christian Aid and CARE, are working in Cambodia, Lao PDR and Mongolia to redress this situation through local DRR programming and capacity development, particularly through education sector interventions that include the mainstreaming of DRR in the school curricula.
5. C4D and subnational presence
<–>
22
Decentralization: Shifts in government authority are underway in Cambodia, Lao PDR and Mongolia to varying degrees and offered opportunities to work directly with local governments on DRR and preparedness issues. Still, the links and communication channels between national, provincial and district authorities, and between authorities and development partners are often weak. Mirroring development efforts, national rhetoric and policy and legal reform do not always translate into action at the local level. Partners are working with local authorities to integrate DRR concerns into regular service delivery programmes, even if the results and the barriers they face are not well understood. Limited capacity, resource constraints and competing priorities are all commonly flagged as barriers to subnational capacity development; but these restraints need to be understood within a more nuanced analysis of local dynamics, social influence and incentives.
In this context, UNICEF is making considerable contribution and is the only United Nations development agency with the potential capacity to implement community-based approaches at an appropriate scale. Efforts to date and the lessons they impart are critical to making ongoing improvements to subnational programming and advocacy; they are also critical to fundraise for subnational capacity development and positive health seeking-behaviour change.
With some notable exceptions found in countries with large well-funded country programmes (India, for example) and supportive governments, UNICEF mostly implements dialogue-based approaches through partnership with NGOs, local governments and civil society groups, primarily because it does not have the financial or human resources to undertake such interventions at scale.
Although UNICEF has initiated proven BCC interventions, these approaches are often limited in terms of sustainability and levels of institutional integration and in terms of making a systemic contribution to health systems strengthening efforts through improved preventive health capacity.
The challenges to campaign-based C4D interventions are generally less acute than they are for dialogue and community-based approaches; an analysis of such challenges, however, has little relevance for this review. Being focused on resilience, on the enablers of resilience and on how they might be better conceptualized for improved results and fundraising purposes necessitates a clearer demarcation between campaign-based C4D and C4D targeting dialogue and participation. This is necessary as much for the social benefits that such processes beget as it is for the support they can provide for BCC and IEC-based health campaigning and social marketing.
Elite capture and the importance of local dynamics: In relation to youth and community participation, elite capture is common. The hierarchical lines of communication and authority evident in Cambodia, Lao PDR and Mongolia extend right down to the local level and can profoundly undermine any professed democratizing intent that might be planned for participatory processes.
Interventions that promote a strong focus on participation and empowerment (including for children, youth and women) should not be confused with BCC interventions that are supported with participatory approaches. Ensuring equitable participation is particularly worthwhile for the confidence it can generate within vulnerable communities but also in the context of promoting and supporting child and human rights, civil society and good governance. Although politically charged and potentially divisive, participatory processes also can do what they frequently aspire to do – which is bring people together in solidarity around important social issues.
Facilitating genuine participation for vulnerability reduction continues to be a significant challenge and necessitates parallel efforts to strengthen the enabling and supportive environments (including services), particularly at the subnational level. Recognizing within programme designs that participation is not always democratic (or even, at times, representative) would allow for a more pragmatic approach. This would include an emphasis on the need to ensure that participatory processes with local government are supported in a manner that builds their capabilities to then, in turn, facilitate the participation of local actors and communities and afford them a greater say in subnational development planning and implementation (especially in the context of DRR and preparedness). In the context of decentralization, this should be a much higher priority for all UN agencies, funds and programmes than it currently is.
Understanding local contexts and their dynamics is an imperative in the design of participatory approaches to ensure that participation actually takes place and to contextualize the results and objectives of such processes. Additionally, in future approaches to BCC and public health campaigning, it will be important to explore the potential that new media offer in relation to youth participation and empowerment.
<–>
<–>
23

The integral and supportive cross-sector functionality of C4D and its role as a driver of innovation and ‘out-of-the-box’ thinking is worthy of deeper institutional appreciation within UNICEF.
Additionally, an intensified approach to subnational monitoring and research would lead to a more nuanced understanding of socio-political contexts and consequently reveal pathways to increased programme effectiveness and potential for scaling up. Important narratives about positive change and innovative strategies for the strengthening of local capacities and resilience will most likely emerge from a more nuanced interpretation of the programming context and an increased subnational engagement.
In the context of the many competing priorities and pressure to operationalize equity programming, it is difficult to see how DRR, CCA and preparedness activities can move beyond the ad hoc preparation activities and preparedness materials. If DRR can be repackaged within a resilience framework that emphasizes links between it and social sector programming, then there is chance for its integration into programming.
Based on this review, the following observations and recommendations may be offered for UNICEF and the partners:
There is now scope to nurture a more considered understanding of what constitutes C4D. This will enable a clearer internal articulation of the implications – and of the comparative utility and efficacy of – campaign-based BCC approaches, such as those that emphasize local participation and empowerment. A more measured organizational positioning of C4D that is cognizant of both the barriers and opportunities present within different approaches could facilitate C4D programming that is more grounded in local contexts and responsive to needs and aspirations. It is critically important to understand the context and local barriers to C4D and dialogue-based approaches. This is increasingly recognized as critical for subnational programming. There is a need for greater investment in research that explores: existing local-level resilience and coping mechanisms; strategies that motivate and incentivize the participation of the most vulnerable; and the extraneous influences that can exacerbate local vulnerabilities and diminish collective resilience, local cohesion and participatory communication between government and citizens. In this context, core cross-sector competencies of those working on C4D-related issues might be reviewed, as a basis to consider widening and redefining academic and institutional partnerships to build applied research capacity.
Institutionally, C4D and dialogue-based approaches not only support sector programmes but are also of central importance to health service delivery and to health systems strengthening. Ultimately, the effectiveness of C4D approaches to improve population health is fundamentally linked to the capacity of health workers and health systems to support messages and promote health-seeking behaviours. In this context, increase organization-wide advocacy efforts to promote the role of communication within preventive health and the health systems strengthening agenda (including in relation to preparedness and DRR-related interventions) while also recognizing that the practice and articulation of C4D strategies has untapped potential to strengthen links across programmes and vertical health sector interventions.
C4D and dialogue-based approaches as focal areas for operational research and programme modelling that have a direct bearing on social policy and advocacy support and actions. Modelling interventions and subnational programme strategies and then using the emerging evidence to advocate for integrated approaches to C4D and community and dialogue-based approaches offers the means to enable and enhance local capacities as well as the processes that can be used to test assumptions about local-level programming. They can illuminate how social policy reforms impact – or do not impact – at the local level, and they can expand the evidence base for policy advocacy at the national and subnational levels.
6. Opportunities and recommendations
<–>
<–>
<–>
<–>
25
There is great potential to position UNICEF cooperation as an innovator of community-based approaches. The organization should respond to the lack of coordination for C4D and dialogue-based approaches to DRR, preparedness and improved population health by filling current leadership gaps. Although resources and capacity to design and implement C4D and dialogue-based approaches on a large scale are not usually available, such positioning could help to reconfigure priorities and allow the organization to serve more as a technical and strategic hub for C4D dialogue.
It will be opportune to expand the use of both quantitative and qualitative evidence to monitor and assess C4D interventions. Quantitative indicators are useful to determine increases in knowledge and behaviour changes where they occur, but they generally do not capture how C4D and dialogue-based approaches add value in ways that are not quantifiable. Additionally, results that address such notions as social norms and empowerment (for example, ‘adolescent boys and girls from lower social strata are empowered to participate and make informed decisions affecting their lives’) are particularly difficult to measure with quantitative indicators. Recent C4D guidance outlines appropriate qualitative approaches to collecting and analysing data. Such a formal approach will better enable the results and findings of these qualitative evaluations to feed back into overall M&E frameworks and programme design (UNICEF, 2011).
There is a need to invest time and human resources to leverage funding for C4D, and to ensure that UNICEF C4D capacity is progressively expanded to address the challenges at hand and respond to the expectations of partners. This will also assist in understanding the broad cross-sector relevance of C4D and its strategic potential as a medium for inter- sectoral connectivity.
There are important opportunities to harness and support improved partnerships for C4D and dialogue-based approaches with NGOs that envelope child-centred risk reduction and preparedness, including, for example, with Plan International, Save the Children and World Vision, which are NGO partners in the Children in a Changing Climate Coalition.22 The Asian Disaster Preparedness Centre and IFRC, both of which have invested heavily in research into DRR and DRR mainstreaming and are important authorities on these and related issues and progressive partners in developing national and subnational DRR capacity. Priorities in such cooperation should include supporting the complementarity of regional research and NGO partners’ efforts, backstopping subnational community-based interventions with focused inter-governmental advocacy at all levels and leveraging resources for partner-implemented C4D and dialogue-based approaches.
The above efforts together will support a more nuanced and systematic approach to C4D monitoring and evaluation that enables lessons to emerge and broadens the evidence and advocacy base for C4D to including qualitative ethnographic and sociological analysis. On-going documentation of lessons learned, good practices and barriers can be used to better inform programme design and programme-related advocacy (particularly at the subnational level). This work can heighten the recognition of the role of C4D in promoting rights-based interventions that can build subnational resilience and capacity and enable increased focus on DRR and improved health outcomes for the most vulnerable. Developing an improved understanding of both the shortcomings and potential of C4D and dialogue-based approaches – and better packaging and sharing of that understanding and the guidance it informs – will help to ensure the ongoing relevance of strategic communications within the broader child rights mandate and equity focus.
<–>
<–>
<–>
<–>
<–>
22 For more information, see www.childreninachangingclimate.org/home.htm
26
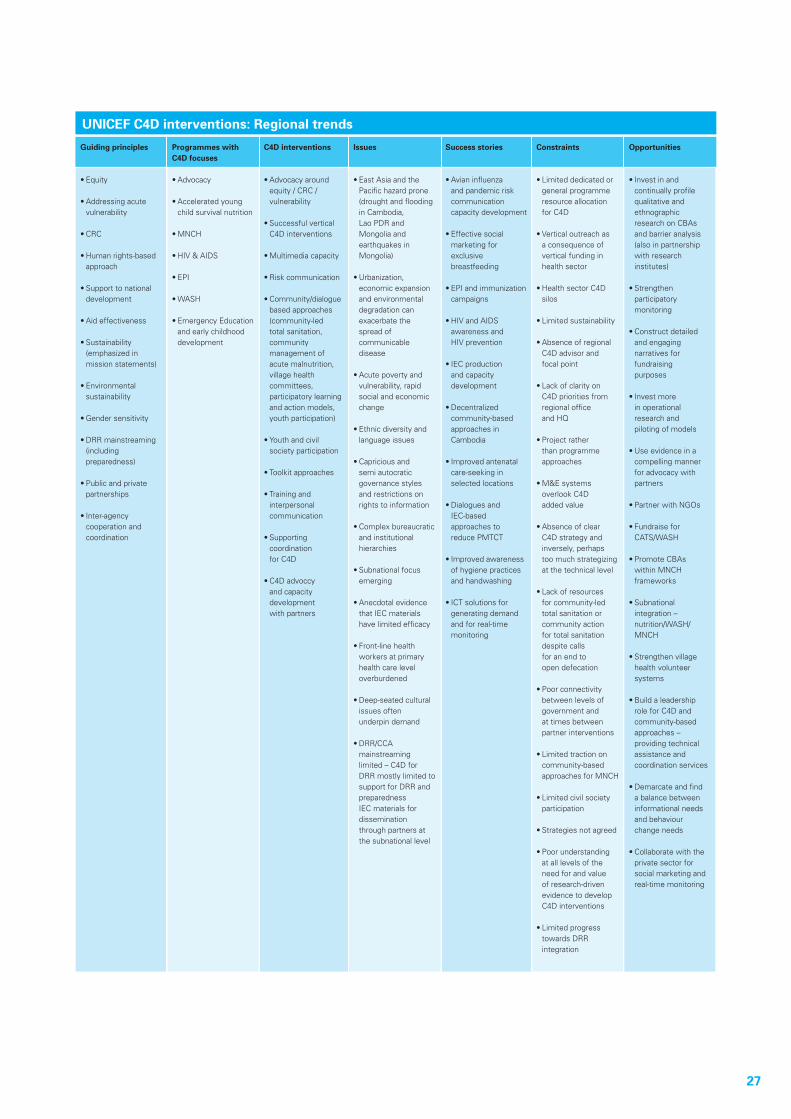
Guiding principles
•Equity
•Addressingacutevulnerability
•CRC
•Humanrights-basedapproach
•Supporttonationaldevelopment
•Aideffectiveness
•Sustainability (emphasized in mission statements)
•Environmental sustainability
•Gendersensitivity
•DRRmainstreaming(including preparedness)
•Publicandprivatepartnerships
•Inter-agency cooperation and coordination
Programmes withC4D focuses
•Advocacy
•Acceleratedyoungchild survival nutrition
•MNCH
•HIV&AIDS
•EPI
•WASH
•EmergencyEducationand early childhood development
C4D interventions
•Advocacyaroundequity / CRC / vulnerability
•SuccessfulverticalC4D interventions
•Multimediacapacity
•Riskcommunication
•Community/dialoguebased approaches (community-led total sanitation, community management of
acute malnutrition, village health committees, participatory learning and action models, youth participation)
•Youthandcivil society participation
•Toolkitapproaches
•Trainingand interpersonal communication
•Supporting coordination
for C4D
•C4Dadvoccy and capacity development
with partners
Issues
•EastAsiaandthePacific hazard prone (drought and flooding in Cambodia,
Lao PDR and Mongolia and
earthquakes in Mongolia)
•Urbanization, economic expansion
and environmental degradation can
exacerbate the spread of communicable disease
•Acutepovertyandvulnerability, rapid social and economic change
•Ethnicdiversityandlanguage issues
•Capriciousand semi autocratic governance styles and restrictions on rights to information
•Complexbureaucraticand institutional
hierarchies
•Subnationalfocusemerging
•Anecdotalevidencethat IEC materials have limited efficacy
•Front-linehealthworkers at primary health care level overburdened
•Deep-seatedculturalissues often
underpin demand
•DRR/CCA mainstreaming
limited – C4D for DRR mostly limited to support for DRR and
preparedness IEC materials for dissemination
through partners at the subnational level
Success stories
•Avianinfluenza and pandemic risk
communication capacity development
•Effectivesocial marketing for exclusive
breastfeeding
•EPIandimmunization campaigns
•HIVandAIDS awareness and
HIV prevention
•IECproduction and capacity
development
•Decentralized community-based approaches in
Cambodia
•Improvedantenatalcare-seeking in
selected locations
•Dialoguesand IEC-based approaches to reduce PMTCT
•Improvedawarenessof hygiene practices and handwashing
•ICTsolutionsforgenerating demand and for real-time
monitoring
Constraints
•Limiteddedicatedorgeneral programme resource allocation
for C4D
•Verticaloutreachas a consequence of vertical funding in
health sector
•HealthsectorC4Dsilos
•Limitedsustainability
•AbsenceofregionalC4D advisor and
focal point
•Lackofclarityon C4D priorities from
regional office and HQ
•Projectrather than programme approaches
•M&Esystems overlook C4D
added value
•Absenceofclear C4D strategy and inversely, perhaps
too much strategizing at the technical level
•Lackofresources for community-led
total sanitation or community action
for total sanitation despite calls
for an end to open defecation
•Poorconnectivitybetween levels of
government and at times between partner interventions
•Limitedtractiononcommunity-based
approaches for MNCH
•Limitedcivilsocietyparticipation
•Strategiesnotagreed
•Poorunderstandingat all levels of the need for and value of research-driven evidence to develop C4D interventions
•Limitedprogresstowards DRR
integration
Opportunities
•Investinand continually profile
qualitative and ethnographic research on CBAs
and barrier analysis (also in partnership with research
institutes)
•Strengthen participatory monitoring
•Constructdetailed and engaging
narratives for fundraising
purposes
•Investmore in operational research and piloting of models
•Useevidenceinacompelling manner for advocacy with partners
•PartnerwithNGOs
•Fundraisefor CATS/WASH
•PromoteCBAs within MNCH frameworks
•Subnational integration – nutrition/WASH/
MNCH
•Strengthenvillagehealth volunteer systems
•Buildaleadership role for C4D and community-based
approaches – providing technical assistance and coordination services
•Demarcateandfinda balance between informational needs and behaviour change needs
•Collaboratewiththeprivate sector for social marketing and real-time monitoring
UNICEF C4D interventions: Regional trends
27
Climate Funds Update, ‘The latest information on climate funds, 19 Feb 2013. Available at: http://www.climatefundsupdate.org/
Covello, Vincent, Message Mapping: Risk and Crisis Communication, Center for Risk Communication, New York, 2003.Department for International Development (DFID), Disaster Risk Reduction: Inter-Agency Group learning review,London, 2011. Available at: http://community.eldis.org/?233@@.59eb15c6!enclosure=.59eb15c7&ad=1
Glik, Deborah, FIRST NAME, Risk Communication for Public Health Emergencies, School of Publich Health, University of California Los Angeles, 2007. Available at: www.asph.org/userfiles/Competencies-Resources/37_GlikRC.pdf
Global Network of Civil Society Organisations for Disaster Reduction, “Clouds but Little Rain: A local perspective of progress towards implementation of the Hyogo Framework, Middlesex, UK, 2009. Available at: www.preventionweb.net/files/9822_9822VFLfullreport06091.pdf
‘Hyogo Framework for Action’, UNISDR website. Available at: www.unisdr.org/we/coordinate/hfa
International Federation of the Red Cross, Hyogo Framework for Action: Red Cross and Red Crescent mid-term review, Geneva, 2010. Available at: www.preventionweb.net/files/18197_midterm.pdf
Kellet, Jan and Sparks, Dan, Disaster Risk Reduction: Spending where it should count, Briefing paper, Global Humanitarian Assistance, Somerset, UK, 2012.
Nakhooda, Smita et al., Climate Finance Fundamentals, 2011. Available at: www.odi.org.uk/resources/docs/7475.pdf
United Nations Economic and Social Commission for Asia and the Pacific (ESCAP) and United Nations Office for Disaster Risk Reduction - Regional Office for Asia and Pacific (UNISDR AP), Protecting Development Gains Reducing Disaster Vulnerability and Building Resilience in Asia and the Pacific The Asia-Pacific disaster report, Bangkok, 2010.
United Nations Office for Disaster Risk Reduction (UNISDR), Terminology, 2007. Available at: http://www.unisdr.org/we/inform/terminology
Global Assessment Report on Disaster Risk Reduction, Geneva, 2009. Available at: http://www.unisdr.org/we/inform/gar
Terminology, 2009. Available at: http://www.unisdr.org/we/inform/terminology
Global Assessment Report on Disaster Risk Reduction: Revealing risk, redefining development, Geneva, 2011. Available at: www.unisdr.org/we/inform/publications/19846
United Nations Children’s Fund, ‘Assessing Social and Cultural Factors and Bottlenecks Related to UNICEF’s Strategic Result Areas’, Draft, C4D Unit, Bangkok, October 2011.
Children and Disaster Risk Reduction in Asia and the Pacific: A way forward, Bangkok, 2010. Available at: www.unicef.org/eapro/AsiaPacific_DRR_final.pdf
World Health Organization, ‘Asia Pacific Strategy for Emerging Diseases’, Geneva, 2010. Available at: www.wpro.who.int/emerging_diseases/documents/docs/ASPED_2010.pdf
Bibliography
28


UNICEF East Asia Pacific Regional Office, EAPRO19 Phra Atit RoadBangkok 10200ThailandTel +66(02)3569420www.unicef.org