Embed Size (px)
Citation preview

UNEXPECTED CAUSE(S) OF CEREBRAL MICROEMBOLISATION INVESTIGATED BY
TRANSCRANIAL DOPPLER DUPLEX COLOUR SONOGRAPHY
Muriel SPRYNGERCardiology-AngiologyCHU Sart Tilman, Liège
BSTH, November the 27th, 2009

CASE REPORT
• 72-year old hypertensive man • december 2008 : right internal carotid thrombotic
occlusion with left hemispheral stroke + 80% left internal carotid stenosis
• january 2009 : stenting of the left internal carotid• october 2009 : admitted for suspected worsening
left hemiparesia and cerebral confusion• Medication : clopidogrel + simvastatine

CAROTID ULTRASOUND
– Right internal carotid occlusion
– Moderate narrowing at the distal part of the left internal carotid stent

CEREBRAL MRI
• bilateral ischemic parietal sequellae

TEE + CONTRAST
• multiple irregular aortic plaques
• interatrial septal aneurysm + right-to-left interatrial shunt through a patent foramen ovale (PFO)

CONTRAST TCD
• Saline contrast TCD with injection of 10 cc of 9°/°° saline infusion in the right forearm
• Bilateral middle cerebral artery recording

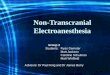
CONTRAST TCD : middle cerebral artery
Microembolic signals (MES) were recorded on both sides

DISCUSSION

CARDIOEMBOLIC STROKE• approximately 20% of strokes are cardioembolic (40% in younger
populations)• atrial fibrillation• valvular heart disease• endocarditis• mitral valve prolapse• prosthetic heart valves,• recent myocardial infarction (0,8% strokes, 1-2%/y),• intracardiac thrombus,• dilated cardiomyopathy• sick sinus syndrome, • patent foramen ovale,• hypokinetic/akinetic left ventricular segment• calcification of the mitral valve• cardiac surgical procedures : 1-7% perioperative stroke

TEE• « gold standard » for the
detection of :– PFO :
• < 20 bubbles : small shunt• > 20 bubbles : large shunt
– Atrial septal aneurysm
• PFO is found in 25% of the healthy population
• PFO + aneurysm : dangerous association?
• 15% of patients who underwent PFO closure had AF detected 3 to 6 months afterwards. PFO closure patients warrant antiplatelet medication at a minimum

CLINICAL RELEVANCE OF TCD AND TEE IN PFO DETECTION
• cTEE = gold standard ? Semi-invasive
• 90% concordance• cTCD :cTCD :
– 20’’ after 1st MB 20’’ after 1st MB – at rest, more sensitive than at rest, more sensitive than
cTEEcTEE– sensitivity 97%, specificity sensitivity 97%, specificity
78%78%– Semi-quantitative Semi-quantitative
(« curtain »)(« curtain »)– Intrapulmonary shuntIntrapulmonary shunt

Bilateral MES
• despite or because of right internal carotid occlusion
• Origins ?– Venous– Aortic– Supra-aortic
(heterolateral carotid)– Cardiac (AF)

CONCLUSION
• In case of right-to-left shunts, cTCD can complete cTEE : – better sensitivity– Semi-quantitative method
• cTCD can also detect potential ME in unexpected cerebral areas and/or explain unexpected strokes.

CONCLUSION
• Contrast-TCD can diagnose large PFO


PFO - CLOSING DEVICE ?• The data supporting risk factors (ie, atrial
septal aneurysm or large PFO) are weak.
• Right-to-left shunting may not be the only possible mechanism for stroke ? More AF.
• High-level evidence for PFO management is desperately needed.

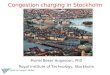
TCD and PFO Contrast Transcranial Doppler Can Diagnose Large Patent Foramen
Ovale
• Small PFO : 19 MES/78 (24%)
• Large PFO : 27 MES/27 (100%)
• No PFO : 3 MES/216• 2 MES is the cutoff to
predict large PFO : – Sensitivity : 96,3%– Specificity : 96.8%– Accuracy : 96.9%
When two or more MES were determined by c-TCD, large PFO could be accurately diagnosed.