Embed Size (px)
Citation preview

60 JCN 2015, Vol 29, No 4
NUTRITION
Awound can be defined as a breakdown in the protective function of the
skin, including a breach in the epithelium with or without the loss of underlying connective tissue (muscle, bone, nerves, etc) (Leaper and Harding, 1998). This results from injury to the skin and/or underlying tissues or organs from surgery, trauma, cuts, chemicals, heat/cold, friction, force, pressure or disease processes such as pressure ulcers, diabetic foot ulcers or carcinomas (Hutchinson, 1992).
Nutrition and hydration play an important role in preserving tissue viability and in supporting tissue repair in the event of damage (Posthauer et al, 2014), and are essential elements in wound care management. Eating a well-balanced
Understanding the link between wound care and nutrition
diet and maintaining a stable healthy weight are also imperative and can reduce the risk of developing several conditions such as diabetes, obesity and heart disease, all of which could predispose an individual to wounds and ulcers (Astrup, 2001). Similarly, wound healing is a complex process which can be further complicated by chronic illness. Poor nutritional status and malnutrition can impair wound healing and increase the risk of infection (Casey, 1998).
A pressure ulcer is an area of localised damage to the skin and/or underlying tissue, usually over a bony prominence as a result of unrelieved pressure, friction and/or shear force (Gandy, 2014). The impact of malnutrition on certain wounds such as pressure ulcers is serious and is only exceeded by nutritional deficiency and impaired immune function (McLaren, 1992).
MALNUTRITION
The Manual of Dietetic Practice(Gandy, 2014) identified four main causes of malnutrition:
Wound care and nutrition are two interlinked areas that will have a serious impact on the caseload of any community nurse. Healthy eating and regular physical activity help to prevent chronic illnesses,
ulcers. In particular, malnutrition can impair wound healing and so
using an evidence-based nutritional screening tool. If a wound has developed, adequate nutritional management plays a key role in the healing process. If necessary, patients should be referred to a registered dietitian for a detailed nutritional assessment and treatment plan. This article looks at the link between nutrition and wound care, as well as highlighting preventative measures that can be encouraged in all patients at risk of developing a wound.
KEYWORDS:Nutrition Wound care Dietitian Malnutrition
Catherine Rabess
WOUND CARE — WHY IT MATTERS...
The government’s policy of moving care closer to home means that not only will community nurses continue to see patients with chronic wounds such as leg ulcers, pressure ulcers and diabetic foot ulcers, they may also start to see an increase in the numbers of patients who have been discharged from hospital with surgical wounds, who might previously have stayed in secondary care for a longer period. It is imperative that community nurses tasked with visiting a range of patients in their own homes have an understanding of the fundamentals of wound development and management to provide basic, evidence-based wound care — this involves having an understanding of nutrition.
Cre
dit:
Esse
nt@
wik
i com
mon
s
Catherine Rabess, specialist nutrition support dietitian, British Dietetic Association member and media spokesperson
Impaired intakeAltered nutrient requirementsImpaired digestion and/or absorption Increased nutrient losses.
Malnutrition can be defined as a state of nutrition in which a deficiency or excess (or imbalance) of energy, protein and other nutrients causes measurable adverse effects both on tissue/body form, body function, and clinical outcome (Elia, 2000).
Malnutrition is a reversible risk factor for pressure ulcers in adults
Nutrition - Rabess - read by BM .indd 24 27/07/2015 17:51
© 2015
Wou
nd C
are P
eople
Ltd
As the UK’s leading provider of nutritionally-balanced frozen ready meals, we’ve built our reputation on delivering good food to people who need it. Our new Nutritious & Delicious range calls on all this expertise to deliver tasty meals that contain less than 400 calories, are low in salt, fat and saturated fat, offer a good source of protein, and contribute to your patient’s 5 a day. With free delivery to the door, it’s perfect for patients in need of a carefully controlled diet at home. You look after the treatment. Let us look after the mealtimes.
A tasty new range of 13 meals, all under 400 calories.
Low on calories, salt and fat. Big on taste.
Introducing Nutritious & Delicious.
674 – Chicken & Spring Vegetable Casserole
wiltshirefarmfoods.com
Try our tasty ranges for FREE or request our brochures by calling
0800 066 3164
© 2015
Wou
nd C
are P
eople
Ltd
62 JCN 2015, Vol 29, No 4
complications including dehydration, infections, vitamin and mineral deficiencies (Elia, 2003). It should also be noted that it is essential that care home residents be screened for malnutrition risk (NICE, 2006).
WEIGHT MANAGEMENT
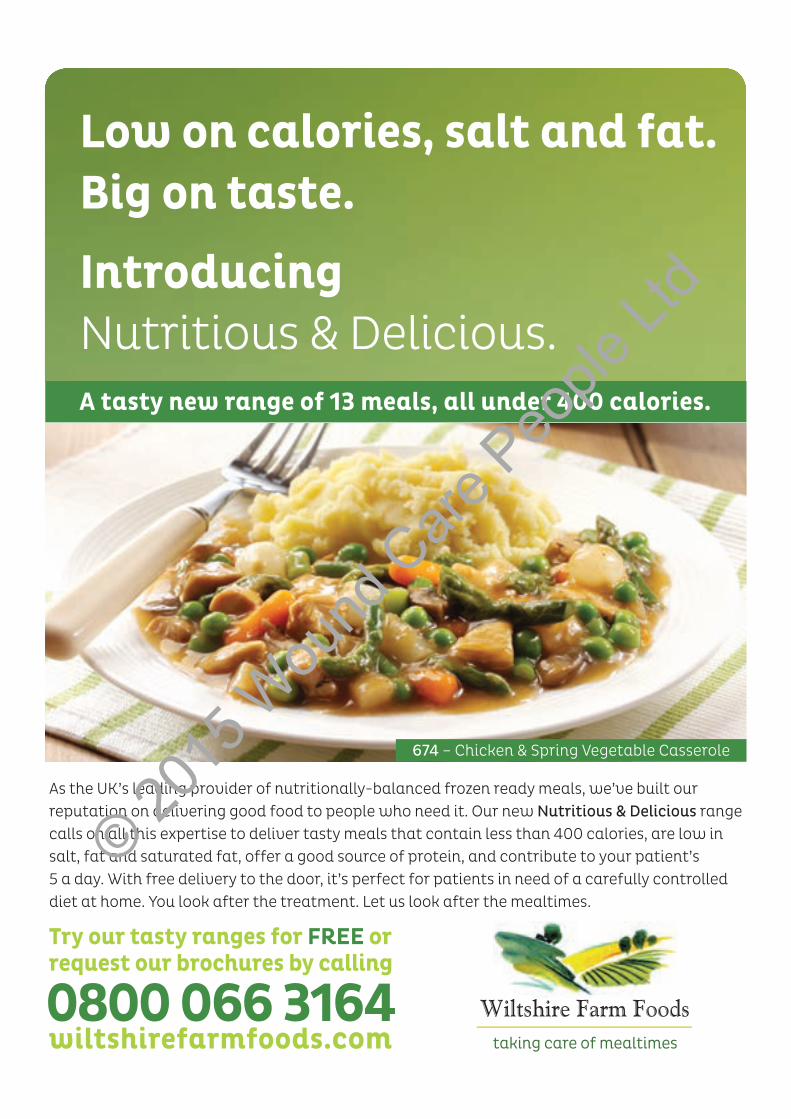
As previously mentioned, following a healthy well-balanced diet (as shown by the Eatwell Plate, Figure 1; Public Health England, [2013]) and regular physical activity can improve general wellbeing and reduce the risk of becoming overweight and/or obese.
A balance of all food groups is required to provide the essential nutrients for wound healing. These groups are: Fruit and vegetables Bread, rice, potatoes and other
starchy foods Meat, fish, eggs, beans and other
non-dairy sources of protein Milk and dairy foods Foods high in fat and/or sugar.
The Eatwell Plate (Figure 1) shows how much of each of these foods should be consumed.
With increased BMI, the risk of developing further comorbidities — including heart disease, diabetes and some cancers — increases (World Health Organization [WHO], 2004).
A higher ratio of fat tissue to blood vessels can impede circulation in obese patients, complicating wound healing and increasing their risk of developing a range of tissue viability-related conditions including:
NUTRITION
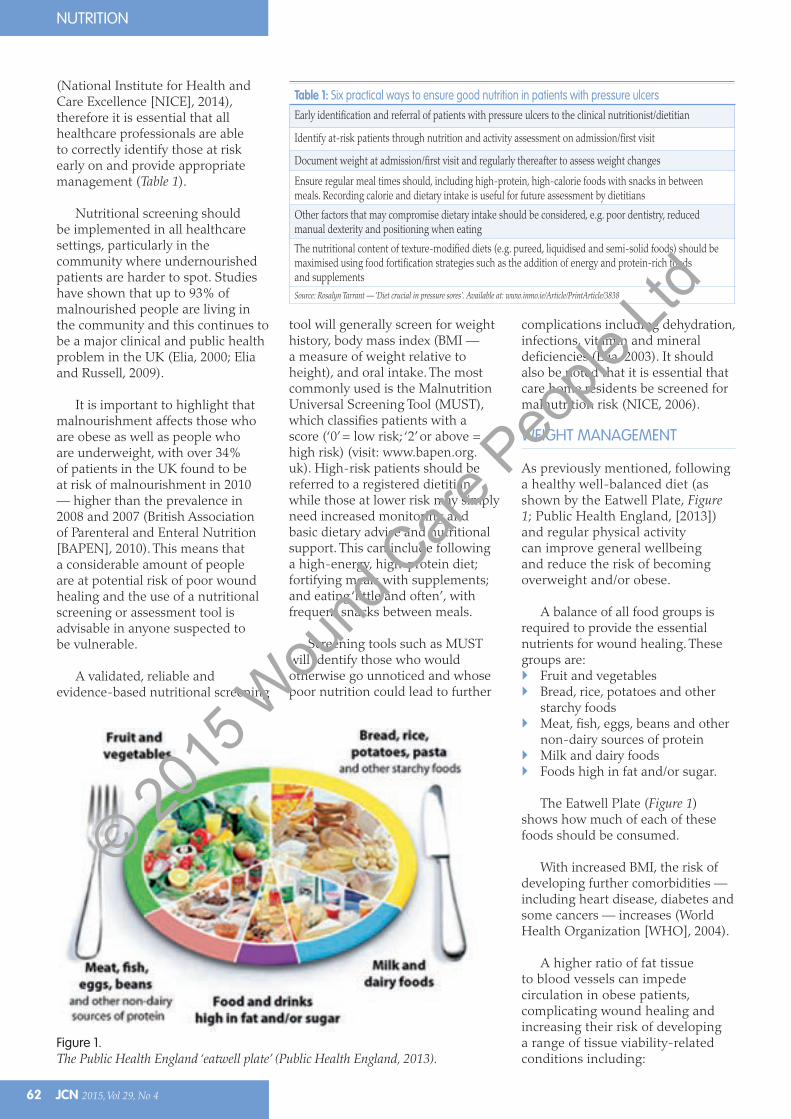
(National Institute for Health and Care Excellence [NICE], 2014), therefore it is essential that all healthcare professionals are able to correctly identify those at risk early on and provide appropriate management (Table 1).
Nutritional screening should be implemented in all healthcare settings, particularly in the community where undernourished patients are harder to spot. Studies have shown that up to 93% of malnourished people are living in the community and this continues to be a major clinical and public health problem in the UK (Elia, 2000; Elia and Russell, 2009).
It is important to highlight that malnourishment affects those who are obese as well as people who are underweight, with over 34% of patients in the UK found to be at risk of malnourishment in 2010 — higher than the prevalence in 2008 and 2007 (British Association of Parenteral and Enteral Nutrition [BAPEN], 2010). This means that a considerable amount of people are at potential risk of poor wound healing and the use of a nutritional screening or assessment tool is advisable in anyone suspected to be vulnerable.
A validated, reliable and evidence-based nutritional screening
tool will generally screen for weight history, body mass index (BMI — a measure of weight relative to height), and oral intake. The most commonly used is the Malnutrition Universal Screening Tool (MUST), which classifies patients with a score (‘0’ = low risk; ‘2’ or above = high risk) (visit: www.bapen.org.uk). High-risk patients should be referred to a registered dietitian, while those at lower risk may simply need increased monitoring and basic dietary advice and nutritional support. This can include following a high-energy, high-protein diet; fortifying meals with supplements; and eating ‘little and often’, with frequent snacks between meals.
Screening tools such as MUST will identify those who would otherwise go unnoticed and whose poor nutrition could lead to further
Figure 1.The Public Health England ‘eatwell plate’ (Public Health England, 2013).
Table 1: Six practical ways to ensure good nutrition in patients with pressure ulcersEarly identification and referral of patients with pressure ulcers to the clinical nutritionist/dietitian
Identify at-risk patients through nutrition and activity assessment on admission/first visit
Document weight at admission/first visit and regularly thereafter to assess weight changes
Ensure regular meal times should, including high-protein, high-calorie foods with snacks in between meals. Recording calorie and dietary intake is useful for future assessment by dietitians
Other factors that may compromise dietary intake should be considered, e.g. poor dentistry, reduced manual dexterity and positioning when eating
The nutritional content of texture-modified diets (e.g. pureed, liquidised and semi-solid foods) should be maximised using food fortification strategies such as the addition of energy and protein-rich foods and supplementsSource: Rosalyn Tarrant — ‘Diet crucial in pressure sores’. Available at: www.inmo.ie/Article/PrintArticle/3838
Nutrition - Rabess - read by BM .indd 26 27/07/2015 17:52
© 2015
Wou
nd C
are P
eople
Ltd
JCN 2015, Vol 29, No 4 63
NUTRITION
Pressure ulcers Cellulitis Venous hypertension Peripheral vascular disease (PVD) Deep vein thrombosis (DVT) Wound infections.
Obesity can also restrict patients’ mobility and lead to pressure damage (Brown, 2004).
Blood glucoseUncontrolled blood glucose levels (HbA1c over 48mmol/mol) can significantly increase the microvascular and macrovascular complications of diabetes. Blood glucose can be affected by nutrition, particularly a diet high in sugar and fats.
Macrovascular complications affect the larger blood vessels, with the most common being cardiovascular disease (CVD), as well as PVD and stroke. Associated risk factors include a high BMI (patients who are overweight/obese), hypertension, high-fat diet, dyslipidaemia (abnormal amount of lipids, e.g. cholesterol and/or fat, in the blood), hyperglycaemia (excess of glucose in the bloodstream) and minimal physical activity (Gandy, 2014).
Conversely, microvascular complications in diabetes affect the smaller blood vessels, especially those in the eyes, kidneys and
nerves. Diabetic neuropathy (nerve damage) is commonly associated with peripheral circulatory damage from persistent high blood glucose levels, which can lead to tissue viability issues, particularly foot ulcers. Appropriate diet and glycaemic maintenance plays an essential role in the management of diabetes and reducing the risk of these complications.
NUTRITIONAL MANAGEMENT IN WOUND HEALING
Optimum nutrition is a key factor in maintaining all phases of wound healing. The basal metabolic rate (the amount of energy expended
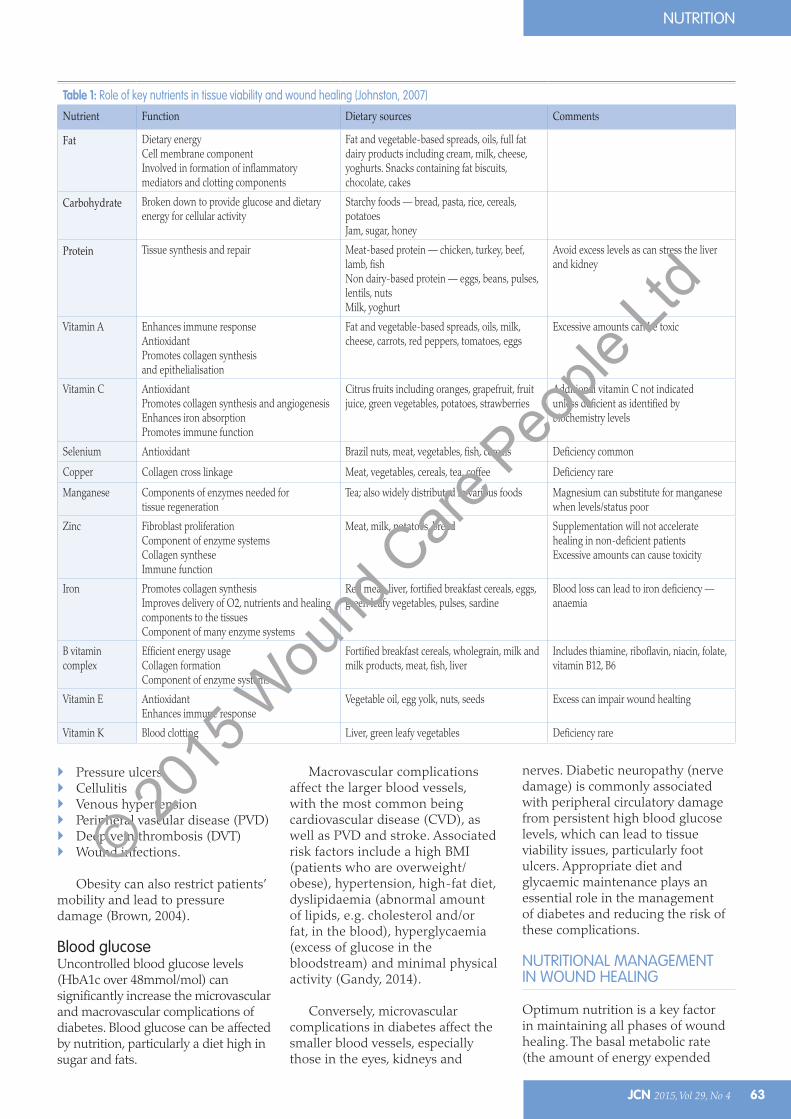
Table 1: Role of key nutrients in tissue viability and wound healing (Johnston, 2007)
Nutrient Function Dietary sources Comments
Fat Dietary energyCell membrane componentInvolved in formation of inflammatory mediators and clotting components
Fat and vegetable-based spreads, oils, full fat dairy products including cream, milk, cheese, yoghurts. Snacks containing fat biscuits, chocolate, cakes
Carbohydrate Broken down to provide glucose and dietary energy for cellular activity
Starchy foods — bread, pasta, rice, cereals, potatoesJam, sugar, honey
Protein Tissue synthesis and repair Meat-based protein — chicken, turkey, beef, lamb, fishNon dairy-based protein — eggs, beans, pulses, lentils, nuts Milk, yoghurt
Avoid excess levels as can stress the liver and kidney
Vitamin A Enhances immune responseAntioxidantPromotes collagen synthesis and epithelialisation
Fat and vegetable-based spreads, oils, milk, cheese, carrots, red peppers, tomatoes, eggs
Excessive amounts can be toxic
Vitamin C AntioxidantPromotes collagen synthesis and angiogenesisEnhances iron absorptionPromotes immune function
Citrus fruits including oranges, grapefruit, fruit juice, green vegetables, potatoes, strawberries
Additional vitamin C not indicated unless deficient as identified by biochemistry levels
Selenium Antioxidant Brazil nuts, meat, vegetables, fish, cereals Deficiency common
Copper Collagen cross linkage Meat, vegetables, cereals, tea, coffee Deficiency rare
Manganese Components of enzymes needed for tissue regeneration
Tea; also widely distributed in various foods Magnesium can substitute for manganese when levels/status poor
Zinc Fibroblast proliferationComponent of enzyme systemsCollagen syntheseImmune function
Meat, milk, potatoes, bread Supplementation will not accelerate healing in non-deficient patientsExcessive amounts can cause toxicity
Iron Promotes collagen synthesisImproves delivery of O2, nutrients and healing components to the tissues Component of many enzyme systems
Red meat, liver, fortified breakfast cereals, eggs, green leafy vegetables, pulses, sardine
Blood loss can lead to iron deficiency —anaemia
B vitamin complex
Efficient energy usageCollagen formationComponent of enzyme systems
Fortified breakfast cereals, wholegrain, milk and milk products, meat, fish, liver
Includes thiamine, riboflavin, niacin, folate, vitamin B12, B6
Vitamin E AntioxidantEnhances immune response
Vegetable oil, egg yolk, nuts, seeds Excess can impair wound healting
Vitamin K Blood clotting Liver, green leafy vegetables Deficiency rare
Nutrition - Rabess - read by BM .indd 27 27/07/2015 17:52
© 2015
Wou
nd C
are P
eople
Ltd

64 JCN 2015, Vol 29, No 4
NUTRITION
The information presented in this article will help community nurses to consider
the effect of nutrition on wounds as well as the ongoing impact of poor nutrition, which can increase the risk of pressure sores.
The author encourages nurses to consider the quality of life of patients with wounds. In today’s economic climate, community nurses are trying to deal with an influx of patients who are unable to afford to eat properly to adequately support their health and manage the risks which develop as a result, e.g. weight loss, low body weight and pressures ulcers. The article also examines the importance of weight management, particularly in
people who are obese and at-risk of pressures ulceration. Managing obesity is equally as important as managing low body weight, but can be overlooked when the focus is so often on malnutrition in underweight patients.
The information the author has provided will help nurses to provide first-line nutrition advice to support patients in making the dietary changes necessary to improve their health and skin integrity. I feel this article is an excellent resource for community nurses and a useful overview of the role of nutrition in wounds. It also provides an interesting discussion point for nurses to take-up with local dietitians.
Expert commentaryEdel McGinley, service lead dietitian for nutrition support, London North West Healthcare NHS Trust
Finally, iron supports the transportation of oxygen in the blood, which aids healing (Woodward et al, 2009). If the patient has a history of iron anaemia deficiency a supplement can be recommended (Table 2).
at rest) rises when people have a wound due to greatly increased cell activity at the wound site (Casey, 1998). It has been estimated that energy levels can increase by up to 10% following minor surgery and can rise by 100% or more in the presence of severe burns (White and Baxtar, 1998).
Reduced energy intake will also lead to a decrease in fat stores and consequently a loss of protective cushioning, thus increasing the likelihood of pressure ulcers (Todorovic, 2003). The role of specific nutrients in tissue viability and wound healing is shown in Table 2.
Carbohydrates — alongside fats — are the primary source of energy required for wound-healing. Glucose (a form of carbohydrate) is the major source of fuel used to provide energy for new tissues and prevent protein depletion (Guo and DiPietro, 2010). Protein energy malnutrition (PEM) has been proven to have a direct effect on non-healing of wounds due to impaired collagen synthesis and deposition. Numerous studies have shown that increasing the dietary protein of patients with chronic ulcers leads to faster healing times than low-protein diets (Hurd, 2003).
Micronutrients also serve a vital role in healing, particularly vitamins A, B1, B2 and B6, as they have a metabolic function in energy production and collagen deposition (Woodward et al, 2009). Copper, zinc and selenium have a role in immune function and significant amounts can be lost through wound exudate in people with burns (Woodward et al, 2009). The author does not routinely recommend that patients are given copper or selenium supplements as there is not enough evidence to support this, however small amounts can be found in the dietary sources highlighted in Table 2.
Although various studies provide conflicting information, there is evidence that vitamin C supplements can help improve pressure ulcers and wound healing in general (Castellanos et al, 2003; Winkler, 2004; Woodward et al, 2009). Vitamin C is also an essential micronutrient
for collagen formation and critical for wound care.
Similarly, vitamin A deficiency, although rare, can result in impaired wound healing and susceptibility to infection due to its function in enhancing the immune system (Cresci, 2005).
Zinc also has a role in all stages of wound healing (Table 2) (Bradbury, 2006) and a zinc deficiency has been shown to delay wound healing by reducing the rate of epithelialisation and decreasing scar strength and collagen synthesis (Andrews and Gallagher-Allred, 1999). It is important to note that excess zinc can cause toxicity — this has been shown to induce both copper and iron deficiency anaemia, which can ultimately lead to reduced oxygen delivery to the wound (Gray, 2003). However, studies appear to show that on balance it is preferable to promote wound healing by providing zinc supplements for patients who are deficient (Bradbury, 2006).
Answer the following questions about this article, either to test the new knowledge you have gained or to form part of your ongoing practice development portfolio.
1 – Can you explain how the community nurse can recognise malnutrition?
2 – What is the main role of nutrition in wound care?
3 – What are some of the key nutrients involved in wound healing?
4 – How mght certain vitamins aid wound healing?
5 – What are the benefits of providing adequate fluids in patients with a wound?
Five-minute test
Nutrition - Rabess - read by BM .indd 30 27/07/2015 17:52
© 2015
Wou
nd C
are P
eople
Ltd
JCN 2015, Vol 29, No 4 65
NUTRITION
FLUIDS
Adequate fluids are required to maintain good skin tone and bloodflow to tissues, which is critical in the prevention of skin breakdown. Dehydration specifically is a substantial risk factor in the development of pressure ulcers, as the skin becomes loose, fragile and more susceptible to breakdown (Horns et al, 2004).
The majority of the adult population require a minimum fluid intake of 1500mL/day (the equivalent of 6–8 cups), however this is a guideline and clinical judgement should be used to adjust the amount depending on the patient’s clinical condition.
CONCLUSION
Any nurse has a duty to promote a healthy lifestyle. A nutritious diet and regular physical activity help to prevent chronic illnesses and wounds and ulcers. If a wound has developed, good nutritional management plays a key role in the healing process.
Malnutrition impairs wound healing and it is essential that at-risk patients are identified at the early stages using an evidence-based nutritional screening tool. If necessary, patients should be referred to a registered dietitian for a detailed nutritional assessment and treatment plan.
Quality of life should always be emphasised, particularly in those patients with non-healing chronic wounds. This means ensuring that a patient-centred approach is followed at all times to achieve an appropriate outcome. Evidence has shown that improving a patient’s nutritional status and reducing the risk of malnutrition with dietary support can help prevent any further deterioration.
Preventative measures, including nutritional management, should be encouraged in all patients at risk of developing a wound. However, not all wounds are preventable and the appropriate guidelines should be
followed to monitor and assess the risks. JCN
REFERENCES
Andrews M, Gallagher-Allred C (1999) The role of zinc in wound healing. Adv Wound Care 12: 137–8
Astrup A (2001) Healthy lifestyles in Europe: prevention of obesity and type II diabetes by diet and physical activity. Public Health Nutr 4(2B): 499–515
Bradbury S (2006) Wound healing: is oral zinc supplementation beneficial? Wounds UK 2(1): 54–61
BAPEN (2010) Nutrition Screening Survey in the UK and Republic of Ireland in 2010. Available at: www.bapen.org.uk/pdfs/nsw/nsw10/nsw10-report.pdf (accessed 6 July, 2015)
Brown J (2004) Nutrition and wound healing. Complete Nutrition 5(1): 14–18
Castellanos WH, Silver HJ, Gallagher-Allred C, Smith TR (2003) Nutrition issues in the home, community and long-term care setting. Nutr Clin Pract 18: 21–36
Casey G (1998) The importance of nutrition in wound healing. Nurs Stand 13(3): 51–6
Cresci G (2005) Nutrition Support for the Critically Ill Patient — A Guide to Practice. CRC/Taylor & Francis, Boca Raton FL, USA
Elia M (2000) Guidelines for Detection and Management of Malnutrition. Malnutrition Advisory Group (MAG), standing committee of BAPEN, Maidenhead
Elia M (2003) Screening for Malnutrition: a multidisciplinary responsibility. Development and Use of the ‘Malnutrition Universal Screening Tool’ (‘MUST’) for Adults. MAG/BAPEN, Redditch
Elia M, Russell CA (2009) Combating Malnutrition: recommendations for action. BAPEN, Redditch
Gandy J (2014) Manual of Dietetic Practice. Fifth edition. Wiley Blackwell, Oxford
Gray M (2003) Does oral zinc supplementation promote healing of chronic wounds? J Wound Ostomy Continence Nurs 30(6): 295–9
Guo S, DiPietro L (2010) Factors affecting wound healing. J Dent Res 89(3): 219–29
Horns D, Bender SA, Ferguson ML, et al (2004) The National Pressure Ulcer Long-term Care Study: pressure ulcer
development in long-term care residents. J Am Geriatr Soc 52: 359–67
Hurd TA (2003) Nutrition and wound-care management/prevention. Wound Care Canada 2(2): 20-4
Hutchinson J (1992) The Wound Programme. Centre for Medical Education, Dundee
Johnston E (2007) The role of nutrition in tissue viability. Wound Essentials 2: 10–21
Leaper DJ, Harding KG (1998) Wounds: biology and management. Oxford University Press, Oxford
McLaren S (1992) Nutrition and wound healing. J Wound Care 1(3): 45–55
NICE (2014) Clinical Guideline 179. Pressure ulcers: prevention and management of pressure ulcers in primary and secondary care. NICE, London
NICE (2006) Clinical Guideline 36. Nutrition Support in Adults: oral nutrition support, enteral tube feeding and parental nutrition. NICE, London
Posthauer ME, Banks M, Dorner B, Schols J (2014) The Role of Nutrition for Pressure Ulcer Management. National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, and Pan Pacific Pressure Injury Alliance
Public Health England (2013) The Eatwell Plate part of: Obesity and healthy eating
Todorovic V (2003) Food and wounds: nutritional factor factors in wound formation and healing. Clin Nutr Update 8(2): 6–8
White B, Baxter M (1998) Hormones and Metabolic Control. 2nd edn. Edward Arnold, London
Winkler MF, Ainsley MM (2004) Medical nutrition therapy for metabolic stress: sepsis, trauma, burns and surgery. In: Mahan K, Raymond JL, Escott-Stump S (eds). Krause’s Food, Nutrition and Diet Therapy. Elsevier, London: 1059–76
Woodward M, Sussman G, Rice J, Ellis T, Fazio V (2009) Nutrition and Wound Healing: expert guide for healthcare professionals. Available at: www.awma.com.au/publications/2009_vic_expert_guide_nutrition_wound_healing.pdf (accessed 6 July, 2015)
WHO (2004) Diet, Nutrition and the Prevention of Chronic Diseases. Available at: http://whqlibdoc.who.int/trs/who_trs_916.pdf (accessed 6 July, 2015)
Nutrition - Rabess - read by BM .indd 31 27/07/2015 17:52
© 2015
Wou
nd C
are P
eople
Ltd

Do you need an evidenced-based source of practical, ‘need-to-know’,key information at your fi ngertips?
The ‘Care Today’ series of annual journals cover specifi c areas of care vital for day-to-day practice:
✓ Wound Care Today (now in its second volume)
✓ Skin Care Today
✓ Respiratory Care Today
Their easy-to-read style combines clinical education with practical tips through:
› Point-specifi c posters — your clinical companions for everyday practice
› Clinical features — written by experts in their fi eld
› Debate and discussion — on what matters most to provide patient-centred care
Visit www.jcn.co.uk for information on forthcoming journals in the series....
... as keeping up to date has never been easier for all those working in the community.
Available in print and online via:
www.jcn.co.uk
Don’t wait for tomorrow — start caring today …. ✓
WOUND CARE TODAY
www.woundcare-today.com
In association with
WOUND CARE TODAY
For what matters in practice
Volume 2Number 1
2015
Are pressure ulcers in danger of landing nurses in the dock?
WCT Cover 15.indd 1 4/23/15 1:30 PM
All Today ad.indd 1 4/23/15 2:46 PM
© 2015
Wou
nd C
are P
eople
Ltd