Embed Size (px)
Citation preview

Original Article
Understanding the causation of primary angleclosure disease using the sufficient componentcause modelRavi Thomas MD FRANZCO,1 Kerrie Mengersen PhD,2 Aleysha Thomas BSc2 andMark J Walland FRANZCO FRACS3
1Queensland Eye Institute & University of Queensland, 2Discipline of Mathematical Sciences, Queensland University of Technology,Brisbane, Queensland and 3Glaucoma Investigation and Research Unit, Royal Victorian Eye and Ear Hospital, Melbourne, Victoria,Australia
ABSTRACT
Background: Several risk factors have been associatedwith primary angle closure disease, but their actualrole in causation of an individual case is not clear.
Design: Concept paper.
Participants/Samples: No patient participation.
Methods: The sufficient component cause model isbriefly explained in the context of primary angleclosure disease. The framework is used to conceptu-alize the role of individual mechanisms of disease.The possibility of personalized treatment for primaryangle closure disease is discussed in this context.
Main Outcome Measures: Qualitative concepts indisease causality may refine research and treatmentin primary angle closure disease.
Results: The minimum set of conditions that are suf-ficient for primary angle closure disease to occur isconsidered the sufficient component cause model forthat individual case. Described risk factors (includinggenes) as well as currently unknown influencesplay a role in the model. There may be many suchmodels and all complementary components in anysufficient-cause model must be present for disease tooccur. Interruption of any one component in thatmodel can be used for treatment. Pupillary block is
likely a component of most such models and maycurrently be considered a universally necessary com-ponent of these models.
Conclusions: The sufficient component cause modelcan be used as a framework to explain the role ofindividual mechanisms of causation and treatment ofprimary angle closure disease. It also aids understand-ing of the proportion of disease due to specific causes.
Key words: angle closure, causation, glaucoma, lasersurgery, sufficient component cause.
INTRODUCTION
All clinicians have an understanding of cause andeffect and when needed, most probably invoke thecommonly used criteria based on ‘considerations’proposed by Bradford Hill in moving from associa-tion to causation.1 For most clinicians, however, thestudy of causation of disease remains an arcane areaof scientific understanding; even the word ‘causa-tion’ hints at some opaque and mysterious threat.The situation becomes more complex with diseases,such as glaucoma, that have a multifactorial aetiol-ogy.2,3 Causal inference in such conditions requiresconcepts and models more sophisticated than thelinear, temporal trap of post hoc, ergo propter hoc (itfollows, therefore because of), or a confusion overwhether a factor is, in fact, causal, merely associatedor even perhaps coincidental.
■ Correspondence: Dr Mark Walland, 1/55 Victoria Parade, Fitzroy, Melbourne, Vic. 3065, Australia. Email: [email protected]
Received 13 May 2013; accepted 16 September 2013.
Competing/conflicts of interest: No stated conflict of interest.
Funding sources: No stated funding sources.
bs_bs_banner
Clinical and Experimental Ophthalmology 2014; 42: 522–528 doi: 10.1111/ceo.12245
© 2013 Royal Australian and New Zealand College of Ophthalmologists

Primary angle closure disease (PACD) affects alarge number of people worldwide.4 PACD incorpo-rates the entire spectrum of primary closure andincludes primary angle closure suspect, primaryangle closure (PAC, both appositional and syne-chial), primary angle closure glaucoma (PACG) aswell as acute angle closure.5–7
Many factors are known to be associated withPACD, and recent investigations using evolvingtechnology have added novel factors to this growinglist.2 The role of the choroid and iris in PACD hasbeen emphasized, and the first positive results haveemerged from ongoing genetic studies.8–12 The estab-lished factors such as short anterior chamber depth,short axial length, female gender, East Asian ethnic-ity and the newly identified anatomical, physiologi-cal and genetic factors have been summarized.2
The factors identified in these extensive studiesshould eventually translate into treatment targets. Itis hoped that further study of the factors describedearlier will lead to identification of a predominantmechanism, resulting in personalized, more effectivetreatment for each case.2,13
For the present, when treatment is indicated, theinitial approach for most PACD is laser iridotomy.13,14
Laser iridotomy on its own is, however, not alwaysanatomically or functionally successful.15,16 On theother hand, there are patients in whom multiple riskfactors are present and yet disease does not occur;9,17
it is likely that there is a missing crucial component(or components) that, if added, would precipitatedisease.
From a public health perspective, we also needto understand the strength of effect of the variousfactors as well the proportion of disease burden dueto the specific causes.
The aim of this article is to apply the sufficientcomponent cause model – as detailed by Rothman –to better understand the role of multiple factors inthe causation of PACD.18
METHODS
A basic understanding of causation is crucial to elu-cidating the role of putative factors. PACD is clearlya multifactorial disease that cannot be explained bya single factor being necessary or sufficient.3,13 Itsunderstanding and treatment requires a frameworkthat considers all known and unknown factors.2,13,14
The sufficient component cause model (also referredto as sufficient-cause model) is a useful approach toclarifying individual mechanisms of causation.18
It is important to point out that the examplemodels in the Results section have been used toillustrate concepts and demonstrate how the frame-work of the model can be used to understand thecausation of PACD. While many risk factors are
established, the models are thus far unsupported byeven qualitative evidence to allow their use as theactual model acting in clinical situations. (The pro-portion designated ‘unknown’ has been varied spe-cifically to avoid the impression that this proportionis actually known to be the same in each model.) Weare at this time not aware of a model proposed ascomplete explanation in any clinical scenario.
RESULTS
Sufficient cause refers to a minimum set of causalconditions that are sufficient for a disease (in thiscase PACD) to occur.18
If we consider PAC, the sufficient-cause model isthe collection of all the factors and events requiredfor that case of PAC to occur.18 All components of thatsufficient-cause model must have occurred or bepresent for PAC to occur in this individual case atthat particular time (Table 1).2,6,11,19–30 In this concept,onset of disease can refer to the earliest stage ofdisease (PAC) or transition to another stage, forexample, transition from primary angle closuresuspect to PAC or PACG.
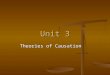
One hypothetical sufficient component causalmodel for PAC is shown in Figure 1. The model inFigure 1 implies that the onset of PAC in this caserequires the components of Eastern ethnicity, short
Table 1. Risk factors identified for primary angle closuredisease
Demographic2,19–23
• East Asian ethnicity• Increasing age• Female gender
Morphological6,20,21,24–29
• Shallow anterior chamber• Shorter axial length• Thicker lens• Anterior position of the lens• Smaller corneal diameter• Thicker iris• Prominent last roll of iris• More anterior origin of the iris• Plateau iris
AS-OCT2,30
• Anterior chamber width (ACW)• Anterior chamber area (ACA)• Anterior chamber volume (ACV)• Iris – thickness, area, and curvature• Iris – changes in volume with dilation• Lens – lens vault
UBM11,20,21,25
• Choroid – choroidal expansion/effusion• Choroidal thickness
Genetic12
AS-OCT, anterior segment optical coherence tomography;UBM, ultrasound biomicroscopy.
Sufficient cause model in angle closure 523
© 2013 Royal Australian and New Zealand College of Ophthalmologists

axial length, anterior lens position, short anteriorchamber depth as well as other factors that are cur-rently unknown.
For each component in a sufficient cause, the set ofother factors in that model form the complementarycomponent causes. For example, in Figure 1, thecomplementary causes of the component Eastern eth-nicity are small axial length, short anterior chamber,anterior lens position and all the unknown causes inthat model. PAC will occur when the last comple-mentary component of this model occurs.
It is important to note that Figure 1 does notinclude all the known causal factors for PAC. Allknown factors need not be operational in everymodel; all factors that appear in the models are causaland not just associations. It is obvious that East Asianethnicity may play a causal role in some sufficientcomponent cause models but not in others. East Asianethnicity on its own is not sufficient to produce PAC,and its absence is not enough to protect against PAC.There are other sufficient component models throughwhich the disease might occur in those of differentethnicity. The same can be said for most individualfactors involved in PAC. The minimum number ofcomponents required to produce PAC (minimallysufficient set) needs to be considered for each model.In that model, none of these causes is superfluous:they must all be present. Additionally, there arecauses for that case that are currently unknown(or unsuspected) and represented as such.
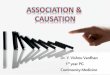
Another sufficient-cause model for PAC mayinvolve some common risk factors, but have othersthat are different (Fig. 2). In this model, for example,short axial length and anterior chamber depthpersist, flat corneal curvature and lens vault areadded, but Eastern ethnicity is absent. The unknownfactors, too, may be the same, or dissimilar. This setis also minimally sufficient for PAC to occur. Thecomplementary causes for small axial length in thismodel are therefore short anterior chamber depth,flat corneal curvature, lens vault and the componentof unknown factors. Once the last complementary
component comes into play, the sufficient componentcausal model is complete, and PAC will occur.
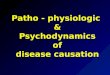
Known causative genes, if present, could bedepicted in a different model. Figure 3 depicts amodel similar to Figure 2, where flat corneal curva-ture is absent but the recently described genes are acomponent sufficient to complete the model. Genes asyet unknown would be incorporated in the unknowncomponent of other (and even these) models.
According to this framework, there may be severalsuch sufficient-cause models involved in the spec-trum of PAC. PAC that involves synechiae formationmay require additional factors (perhaps a componentof inflammation) and their interactions, which arecurrently unknown. Other models involving differentcombinations of known and unknown factors may beoperational in PACG. Some of the factors that make anoptic disc susceptible to damage may be commonwith models for primary open-angle glaucoma.
A model for acute primary angle closure is likelyto be different from PAC and PACG in some respects;a speculative model is shown in Figure 4. Thisparticular model involves short axial length, shortanterior chamber depth, increased lens thickness,increase in iris thickness on dilatation, choroidalexpansion and unknown factors.
Unknown
Anterior Lens
Position
Short Anterior
Chamber Depth
Short Axial Length
Eastern Ethnicity
Figure 1. Possible model for primary angle closure 1.
Unknown
Anterior Lens
Position
Flat Corneal
Curvature
Short Anterior
Chamber Depth
Short Axial Length
Figure 2. Possible model for primary angle closure 2.
Unknown
Anterior Lens
Position
Anterior Lens
Vault
Genes
Short Anterior
Chamber Depth
Short Axial Length
Figure 3. Possible model for primary angle closure 3.
524 Thomas et al.
© 2013 Royal Australian and New Zealand College of Ophthalmologists

The diagrams show a fraction of the pie as‘unknown’; that component may be more or less. Itremains possible that most of the sufficient compo-nents for a particular model are already known andare merely awaiting the recognition to combine themin that model. As the number of known factorsincreases, the unknown component will decrease(Figs 1–5), but it is unlikely that we will decreasethis to zero, at least in foreseeable future. Clinically,this is less crucial than it might initially seem, as it isa defining feature of the sufficient-cause model thatinterruption of any one component in that model will preventthe disease from occurring.
A factor that is present in all sufficient-causemodels of PAC or PACG would be termed a univer-sally necessary component cause. From what weknow about PACD and its treatment, it is possiblethat pupillary block may come close to beingregarded as a universally necessary componentcause for PACD. Pupillary block could be producedby interaction of lens mass or volume, lens position/vault, short axial length, short anterior chamberdepth and/or width and other unknown factors. Themere presence of the lens is neither a sufficientcause alone (most phakic patients do not develop
PACD) nor is it a universally necessary componentcause, as there are certainly cases of what we wouldstill call ‘primary’ ACD occurring in pseudophakicand aphakic eyes through the mechanism ofpupillary block or plateau iris. These factors can bequantified, but it is important to keep in mind thateach component cause must be defined with refer-ence to a distinct alternative reference condition.If pupillary block was considered as an independ-ent risk factor, it would need to be defined alongwith an explicit physiological level of block as thereferent.
DISCUSSION
With a view to prevention and treatment of PACD, itis especially important to identify the factors thatcause PAC and PACG. Increasing attention to thecausation of PACD has resulted in the discovery ofmultiple risk factors for this condition.2,12 Ongoingpopulation-based studies and the application ofnewer technology are likely to identify even moreputative causal factors and more genes. The role ofthese individual risk factors and how they interact inthe causation of PACD is, however, not clear. Wehave drawn extensively from Rothman to explainand apply the concepts of a sufficient componentcause model to understand the role of individualmechanisms of causation in PACD.13,18
A naïve concept of causation applied to PACDwould seek a deterministic relationship betweeneach factor and its effect: in other words, each factoris considered both necessary and sufficient.18 Suchan approach will lead to consternation when afactor with a high relative risk is present but diseaseis not; or vice versa, when disease is present but thefactor is not. A patient with short axial lengthand short anterior chamber depth who does nothave any sign of PAC (or acute angle closure)despite years of ‘exposure’ to these risks is a sce-nario that frequently puzzles clinicians. The fact thatChinese have a higher prevalence of PACD, but thedepth of their anterior chambers and their axiallengths are not significantly different from Cauca-sian eyes, raises questions about the role of anteriorchamber depth and axial length in this condition.9,17
Perhaps, the differences in corneal curvaturedescribed in Chinese eyes (or other factors) play arole in a model of disease and partly explains thisdiscrepancy.
Similarly, the absence of a newly described genein established PACG may disappoint investigatorswho expect to find these in every case of disease.11
Such ‘anomalies’ are created by the deterministicapproach seemingly wired into the human cognitiveprocess, an approach that is clearly not applicable todiseases of multifactorial aetiology.18,31 Unidentified
Short Anterior
Chamber Depth
Increased Lens
Thickness
Increased Iris
Thickness on
DilationChoroidal
Detachment
Unknown
Short Axial Length
Figure 4. Possible model for primary angle closure.
Unknown Known
Figure 5. As the number of known factors increases, theunknown component will decrease but is unlikely ever to be zero.
Sufficient cause model in angle closure 525
© 2013 Royal Australian and New Zealand College of Ophthalmologists

genetic factors in such cases would currently bedepicted in the unknown component of the causalmodel.
Most diseases – including PACD – are multifacto-rial and require a different conceptual approach tounderstand the individual mechanisms underlyingtheir causation.18 We have applied the framework ofthe sufficient component model to the potentialcausative factors associated with PACD. Use of thisframework allows us to understand the possible roleof individual mechanisms in their causation. Fromthis view, it is clear that a single factor need not benecessary and sufficient to produce PACD. A factor’scausative role lies in its being one component of asufficient-cause model. Once the model is completedby the occurrence of all the complementary causes(including currently unknown causes – and thesemay be different for each case), the disease willoccur. It is important to remember that all the com-ponents do not need to act simultaneously. They canact at different times; disease occurs when the lastcomplementary cause is completed.
Each component cause will act with the othercomplementary factors in the set to produce PACD.Each of the cases that can be causally ascribed to onecomponent in the model will also be attributed toall the other components in the models in which itacts. The contribution of a factor to the total inci-dence of PACD is called its attributable fraction.18 Thesufficient-cause model allows us to appreciate thatattributable fractions added across the componentcauses of the same disease (in this case, PACD) neednot sum to one. If pupillary block is indeed a uni-versally necessary component cause in PACD, itwill, by definition, appear in all models of PACDand, on its own, have an attributable fraction of onewithout counting the attributable fractions of theother components. As each case of PACD can beattributed to every component cause in its causalmechanism, the attributable fractions for differentcomponent causes will have to sum to more thanone. For example, axial length, iris volume and iristhickness – all component causes of PACD models –will also contribute their attributable fractions tothat of pupillary block and increase the sum: onlythe fraction attributed to a single component in amodel cannot exceed 100%.
Understanding this idea prevents misconceptionsabout how much we currently know about PACD,how much remains unknown and whether it is worthcontinuing to search for other factors. If, for example,80% of PACD is attributable to lens vault, axiallength, AC depth and iris thickness, 100% of it canstill be attributable to other known causes or thoseunknown at this time which act in a model. A newgene, for example, will contribute 100% to the modelin which it acts. As Rothman writes using examples
of lung cancer and coronary artery disease, there is noproblem with such figures: they just reflect the mul-tifactorial nature of the disease. Failure to understandthis concept can lead to errors of inference in causalityand affect predictive models as well as future researchin PACD. The sufficient-cause framework aids anunderstanding of this important concept.
Application of the framework of the sufficientcomponent cause model also allows us to understandthe role of genetics and the environment and canhelp guide further research. The fractions of thedisease attributable to genes and environmentoverlap: it makes no sense to try and determine theproportion of a multifactorial disease caused bygenes versus environment.18
As more factors are discovered, the unknown com-ponent in each model will decrease. However, againas Rothman states, unless we have found a set ofconditions and events in which the disease does notoccur at all, it is reasonable to assume that somecausal components remain unknown. We can makean educated guess as to what the currently unknownfactors may be. Undiscovered genes are one possibil-ity, as are undiscovered interactions between factorsthat we know and do not know about.
This form of thinking not only has obviousepistemic and research implications but also allowsmanagement inferences. If a disease is produced bythe aggregation of the entire complement of suffi-cient causes, interrupting any of these componentscan prevent/treat the condition. As a component ofpupillary block (produced perhaps by interaction ofindividual factors) is likely present in most modelsof PACD, addressing this component would beexpected to be preventive or therapeutic in mostcases: that explains the usual use of laser iridotomyas a logical first step in most cases where treatment isneeded. Laser iridoplasty acts by decreasing periph-eral iris thickness and could prevent increased iristhickness on dilatation. It also allows access ofaqueous to the trabecular meshwork, relievespupillary block and helps in acute primary angleclosure by addressing the interaction of causal factorsin that patient. This may validate an ‘either/or’conceptualization of treatment strategy, in that treat-ments may disrupt different – but nonetheless nec-essary – components of that sufficient componentmodel. It is not necessary to identify all the compo-nent causes in order to prevent disease.
Following this reasoning, lens extraction prob-ably acts by the same primary mechanism of reliev-ing the ‘universal’ pupillary block as well asdiminishing the threat from iris thickness per se andits increase on dilatation. The incomplete state of ourknowledge does not prevent logical interventionsbased on what we do know.14 The initial approachwe use for clinical management is, however, a
526 Thomas et al.
© 2013 Royal Australian and New Zealand College of Ophthalmologists

question of choosing the best procedure for the indi-vidual patient. Such decisions involve use of clini-cal epidemiologic concepts that, while reasonablysimple, are beyond the scope of this article.
The sufficient-cause model also allows an under-standing of what determines the strength of an effect,and why that effect may be different with differenceversus ratio measures. The reader is referred to theoriginal work for a detailed explanation of thatimportant concept.18
While we have taken a simplistic, qualitativeapproach to PACD, the model can allow for dosedependence. A set of sufficient causes would needto be postulated with a different dose for the factorunder consideration.18 Further specifying levels ofthe factors does complicate matters but could helpimprove the recent attempts at prediction of PAC, forexample, using anterior segment optical coherencetomography.30 A probabilistic component includingdose response can be accommodated in this con-ceptual framework (although validation actuallyneeds a clinical group different from what the citedauthors used29).
The sufficient component causal framework is justone model of causal thinking that is essentiallyqualitative and considers the mechanism of causa-tion as the unit of analysis for causal problems. Themodel can also be applied to other diseases of mul-tifactorial aetiology such as primary open angle glau-coma. It cannot, however, identify biases or considerthe uncertainty that would result from errors ofinitial measurement that can lead to increased uncer-tainty in outcomes (chaotic behaviour) and furtherlimit predictions. There are other models such ascounterfactual and graphical causal models that canaddress the problem of potential biases and are com-plementary. As more data become available, theapplication of concepts such as ‘completion poten-tials’ could allow calculation of the likelihood ofcausing disease for various classes of sufficientcauses.32 Comparison of completion potentials acrossdifferent populations can provide information aboutthe unknown complements in the populations.32
CONCLUSION
We have explained and applied the concept of thesufficient component model to examine the mecha-nisms of causation of PACD. This approach allows usto understand the role of individual causal factors inPACD and explains why some high-risk factors maybe absent in any individual case. The framework alsoexplains why attributable fractions of the variousfactors can sum to more than one. We feel that thisframework explains current treatment strategy andcan also help elucidate/guide and interpret futureresearch and treatment approaches.
REFERENCES
1. Hill AB. The environment and disease: association orcausation? Proc R Soc Med 1965; 58: 295–300.
2. Nongpiur ME, Ku JY, Aung T. Angle closure glau-coma: a mechanistic review. Curr Opin Ophthalmol 2011;22: 96–101.
3. Lowe RF. The natural history and principles oftreatment of primary angle-closure glaucoma. Am JOphthalmol 1966; 61: 642–51.
4. Quigley HA, Broman AT. The number of people withglaucoma worldwide in 2010 and 2020. Br J Ophthalmol2006; 90: 262–7.
5. Foster PJ, Thomas R. Glaucoma care in developingcountries. In: Grehn F, Stamper R, eds. Glaucoma Care inDeveloping Countries. Vol. 2. Berlin: Springer, 2006; 109–22.
6. Sihota R. Classification of primary angle closuredisease. Curr Opin Ophthalmol 2011; 22: 87–95.
7. Thomas R. Glaucoma in developing countries. IndianJ Ophthalmol 2012; 60: 446–50.
8. Aptel F, Denis P. Optical coherence tomographyquantitative analysis of iris volume changes afterpharmacologic mydriasis. Ophthalmology 2010; 117:3–10.
9. Quigley HA, Friedman DS, Congdon NG. Possiblemechanisms of primary angle-closure and malignantglaucoma. J Glaucoma 2003; 12: 167–80.
10. Quigley HA, Silver DM, Friedman DS et al. Iris cross-sectional area decreases with pupil dilation and itsdynamic behavior is a risk factor in angle closure.J Glaucoma 2009; 18: 173–9.
11. Arora KS, Jefferys JL, Maul EA, Quigley HA. Thechoroid is thicker in angle closure than in open angleand control eyes. Invest Ophthalmol Vis Sci 2012; 53:7813–8.
12. Vithana EN, Khor CC, Qiao C et al. Genome-wide asso-ciation analyses identify three new susceptibility locifor primary angle closure glaucoma. Nat Genet 2012; 44:1142–6.
13. Thomas R, Walland MJ. Primary angle closure is amultifactorial disease. Clin Experiment Ophthalmol 2011;39: 593–4.
14. Thomas R, Walland MJ. Management algorithmsfor primary angle closure disease. Clin ExperimentOphthalmol 2013; 41: 282–92.
15. Aung T, Ang LP, Chan SP, Chew P. Acute primaryangle-closure: long-term intraocular pressure outcomein Asian eyes. Am J Ophthalmol 2001; 131: 7–12.
16. Choi JS, Kim YY. Progression of peripheral anteriorsynechiae after laser iridotomy. Am J Ophthalmol 2005;140: 1125–7.
17. Congdon NG, Youlin Q, Quigley H et al. Biometryand primary angle-closure glaucoma among Chinese,white, and black populations. Ophthalmology 1997; 104:1489–95.
18. Rothman KJ, Greenland S, Lash TL. Modern Epidemiol-ogy, 3rd edn. Philadelphia, PA: Lippincott Williams &Wilkins, 2008.
19. Foster PJ, Johnson GJ. Glaucoma in China: how big isthe problem? Br J Ophthalmol 2001; 85: 1277–82.
Sufficient cause model in angle closure 527
© 2013 Royal Australian and New Zealand College of Ophthalmologists

20. He M, Friedman DS, Ge J et al. Laser peripheraliridotomy in eyes with narrow drainage angles: ultra-sound biomicroscopy outcomes. The Liwan Eye Study.Ophthalmology 2007; 114: 1513–9.
21. Kumar RS, Tantisevi V, Wong MH et al. Plateau iris inAsian subjects with primary angle closure glaucoma.Arch Ophthalmol 2009; 127: 1269–72.
22. Lavanya R, Wong TY, Friedman DS et al. Determinantsof angle closure in older Singaporeans. Arch Ophthalmol2008; 126: 686–91.
23. Seah SK, Foster PJ, Chew PT et al. Incidence of acuteprimary angle-closure glaucoma in Singapore. Anisland-wide survey. Arch Ophthalmol 1997; 115: 1436–40.
24. Alsbirk PH. Primary angle-closure glaucoma.Oculometry, epidemiology, and genetics in a highrisk population. Acta Ophthalmol Suppl 1976; 127: 5–31.
25. Kumar RS, Baskaran M, Chew PT et al. Prevalence ofplateau iris in primary angle closure suspects an ultra-sound biomicroscopy study. Ophthalmology 2008; 115:430–4.
26. Lee DA, Brubaker RF, Ilstrup DM. Anterior chamberdimensions in patients with narrow angles and angle-closure glaucoma. Arch Ophthalmol 1984; 102: 46–50.
27. Tello C, Tran HV, Liebmann J, Ritch R. Angle closure:classification, concepts, and the role of ultrasoundbiomicroscopy in diagnosis and treatment. SeminOphthalmol 2002; 17: 69–78.
28. Wang N, Wu H, Fan Z. Primary angle closure glaucomain Chinese and Western populations. Chin Med J (Engl)2002; 115: 1706–15.
29. Wojciechowski R, Congdon N, Anninger W,Teo Broman A. Age, gender, biometry, refractiveerror, and the anterior chamber angle among AlaskanEskimos. Ophthalmology 2003; 110: 365–75.
30. Nongpiur ME, Haaland BA, Friedman DS et al. Classi-fication algorithms based on anterior segment opticalcoherence tomography measurements for detection ofangle closure. Ophthalmology 2013; 120: 48–54.
31. Tversky A, Kahneman D. Judgment under uncertainty:heuristics and biases. Science 1974; 185: 1124–31.
32. Lee WC. Completion potentials of sufficient compo-nent causes. Epidemiology 2012; 23: 446–53.
528 Thomas et al.
© 2013 Royal Australian and New Zealand College of Ophthalmologists