Embed Size (px)
Citation preview

Understanding Mechanical Ventilation
A Learning Resource for ICU Nursing Staff
Mairi Mascarenhas Clinical Educator ICU
Raigmore Hospital November 2019

What is mechanical ventilation?
Mechanical ventilation is used on patients who are unable to sustain adequate ventilation that is needed to maintain normal levels of gas exchange. Mechanical ventilation helps normalize arterial blood gas levels and acid-base imbalance by providing oxygenation and by removing carbon dioxide (ventilation)
Mechanical ventilation can decrease the patient’s work of breathing by unloading respiratory muscles in a synchronous manner. Mechanical ventilation can also maintain long-term respiratory support of patients with chronic ventilatory problems.
What is a Mechanical Ventilator?
A mechanical ventilator is a machine that aids in a patient’s ability ventilate. In other words, their ability to take in oxygen and remove carbon dioxide. This machine is most often used for patients with breathing difficulties and those recovering from surgery or critical illness.
Whilst on a mechanical ventilator, a tracheal tube connects the patient to the machine. A patient stays on a mechanical ventilator until he or she is able to achieve spontaneous breathing on their own.
Mechanical ventilation is considered an invasive procedure because it involves placing a tracheal tube inside the patient’s airway. It is important to keep in mind that the use of this machine does not completely heal the condition of the patient. Rather, it helps the patient achieve a stable condition while medications and other treatments actually promote healing.
Mechanical ventilation is also called positive pressure ventilation – using pressure or volume derived modes.
Following an inspiratory trigger, a predetermined mixture of oxygen and air is forced into the central airways and then flows into the alveoli. As the lungs inflate, the intra-alveolar pressure increases. A termination signal eventually causes the ventilator to stop forcing air into the central airways and the central airway pressure then decreases. Expiration follows passively, with air flowing from the higher pressure alveoli to the lower pressure central airways.
1.

What are the benefits of mechanical ventilation? The principle benefits of mechanical ventilation during respiratory failure are improved gas exchange and decreased work of breathing:
Provision of adequate oxygenation and elimination of carbon dioxide
Improves gas exchange by improving ventilation-perfusion (V/Q) matching
Can assume some or all of the increased work of breathing, allowing the ventilator muscles to
recover from their fatigue
Provision of a patent airway Complications of mechanical ventilation
1. Barotrauma
- This is a condition in which the tiny air sacs within the lungs known as alveoli, burst or rupture due to increased pressure. As a result, the lungs collapse and this can lead to very serious lung conditions that can affect breathing. In most cases, barotrauma is highly prevalent in patients with chronic obstructive pulmonary disease (COPD) that are receiving mechanical ventilation.
2. Volutrauma
- This condition occurs when the alveoli become filled with fluid due to high tidal volumes. Tidal volume refers to the amount of the air transported into the lungs when you inhale. Volutrauma commonly occurs in mechanically-ventilated patients who have acute respiratory distress syndrome (ARDS)
3. Ventilator-Associated Pneumonia (VAP)
- This condition is a form of lung infection induced by mechanical ventilation. Because mechanical ventilation often involves the insertion of tracheal tubes into the airway of the patient, there is a chance that various micro-organisms can enter the lungs and cause infection. Ventilator-associated pneumonia can also occur when a mechanically-ventilated patient accidentally aspirates gastric contents into the lungs.
4. Intrinsic positive end-expiratory pressure or auto-PEEP
- Intrinsic positive end-expiratory pressure, also known as AutoPEEP, is characterized by over-inflation of the lungs due to large tidal volumes, restrictive airways, or prolonged inhalation time. If left untreated, this condition can progress to barotrauma and collapsed lungs.
2.

How do Ventilators Work? Before a patient is connected to a mechanical ventilator, a patent airway must be established by the following methods
Intubation – this involves placing a considerably long tube i.e. endotracheal tube (or ET tube) into the mouth (or nose) and down into the trachea of the patient to establish an airway.
Tracheostomy – a tracheostomy involves either creating an incision into the patient’s neck using either a surgical (ENT surgery) or percutaneous (ICU Intensivist) approach. This enables a shorter tracheal tube i.e. tracheostomy tube to be inserted into the patient’s trachea to establish an airway.
Once a tracheal tube is secured, the tube can then be connected to the mechanical ventilator. The ventilator works by blowing pressure (air plus oxygen as needed) into a patient’s lungs. With this process, the machine can do all the breathing or just assist with the patient’s breathing.
Indications for mechanical ventilation Mechanical ventilation can fully or partially replace spontaneous breathing. It is indicated for acute or chronic respiratory failure, which is defined as insufficient oxygenation, insufficient alveolar ventilation, or both.
Insufficient oxygen levels
- Inadequate oxygenation, known as hypoxia, can damage the tissues and other vital organs in the body if left untreated. Mechanical ventilation helps treat hypoxia by providing a sufficient amount of oxygen into the patient’s lungs that can then be distributed throughout the body to its tissues.
Inadequate ventilation
- A mechanical ventilator helps the patient take in oxygen during inhalation and excrete carbon dioxide during exhalation.
Inability to protect the airway
- Unconscious patients with breathing difficulties are at increased risk for aspiration. Aspiration occurs when the patient accidentally inhales nasal, oral or gastric secretions directly into the lungs. Establishing a patent airway and maintaining spontaneous breathing through mechanical ventilation can help minimise this risk.
3.

Volume Control Ventilation Settings
Volume Control mode
Volume-derived modes enable delivery of fixed tidal volume.
This means that breath by breath the tidal volume usually remains constant.
Volume-derived modes have no respect for increasing airway pressures. This means that if compliance and resistance is increased, then the machine will still attempt to deliver the fixed tidal volume, but the airway pressure becomes compromised. The airway pressure will increase. It can often increase beyond 30cm especially if ventilator alarms aren’t appropriately set. There is a need to inform medical staff if the airway pressure increases beyond 30.
Nursing staff need to ensure that the airway pressure alarm is appropriately set.
Volume Control/SIMV basic settings
4.
500
VT
FiO2
FiO2 is abbreviation for Fraction Inspired Oxygen and ranges 21% (room air) to 100%.
0.30 = 30%, 0.40 = 40% etc and 1.0 = 100% The value displayed on the ventilator may be
recorded on the patient’s observation chart as a fraction or as a percentage.
The value may be recorded as a fraction or percentage on the patient’s observation chart
VT
VT is abbreviation for Tidal Volume. A fixed amount of tidal volume is delivered with each
breath. If the tidal volume is set at 500ml and the respiratory rate is 12 breaths per
minute, the total minute ventilation delivered is 6 litres ( 600ml x 12 breaths per minute).
On the observation chart this is expressed as Vent TV.
Ti
Ti is abbreviation for Inspiration Time. Using 12 breaths per minute as an example, if we
divide 60 seconds by 12 – this informs us that one breath will be completed over 5
seconds. If the inspiration time is 1.7 seconds then the expiration time will be 3.3
seconds (1.7 + 3.3 = 5 seconds for one breath). The inspiration:expiration ratio or I:E
ratio is derived from these figures e.g. divide 3.3 by 1.7 to obtain I:E ratio of 1.9 or 1:1.9.
Normal I:E ratio approximates 1:2 in healthy individuals so expiration time is twice as long
as inspiration. However the I:E ratio may be changed to 1:3 or even 1:4 for certain patient
groups e.g. asthma sufferers. When the Ti parameter is touched the I:E ratio is displayed.

5.
RR
RR is abbreviation for Respiratory Rate. In VC mode this parameter means that all
patients will get mandatory breaths e.g. 12 breaths per minute. On the observation
chart this is expressed as Vent Rate. All patients that are deeply sedated will require
mandatory breaths – so that they can safely breathe. For most patients, an initial
respiratory rate between 12 and 16 breaths per minute is reasonable, although it may
be modified according to the ventilator mode. If the patient’s sedation level is
improving and the patient starts to make spontaneous breathing effort, the total
respiratory rate will be higher. On the observation chart this is expressed as Spont
Rate.
RR X Tidal volume = minute ventilation and this can range 6.0 to 10.0 litres (average
8.0 litres)
PEEP
PEEP is abbreviation for Positive End Expiratory Pressure. This is the application of a
constant positive pressure so that at the end of expiration, the airway pressure does
not return to 0 baseline. Therefore PEEP helps prevent alveoli collapsing during
expiration and helps to recruit collapsed alveoli by keeping the alveoli expanded. A
typical level initiated is around 5cm H20. However, a higher level of PEEP (up to 20cm
H20) is sometimes used to improve refractory hypoxaemia or reduce ventilator-
associated injury in patients with acute lung injury, acute respiratory distress
syndrome or other types of hypoxaemic failure. Elevated levels of PEEP can have
adverse consequences such as reduced preload (decreases cardiac output), elevated
plateau airway pressure (increases risk of barotrauma), and impaired cerebral venous
outflow (increases intracranial pressure).
P
Supp
P supp is abbreviation for Pressure Support. Whenever the patient initiates a
spontaneous breath, the ventilator delivers support to the breath according to the
preset pressure level. The pressure support level can range from around 5cm H2O up
to 20cm H2O. On the observation chart this is expressed as ASB (assisted
spontaneous breathing) The tidal volume that results is dependent on the preset
pressure and the patient’s lung compliance. Some patients may need higher levels of
support if the tidal volume is reduced. As the patient is weaned from mechanical
ventilation, the level of support is gradually reduced down to around 5cm H2O.
Titration of support usually involves increasing or decreasing by 2cm H20.
Slope
Slope refers to the inspiratory rise time. The inspiratory rise time determines the amount
of time it takes to reach the desired airway pressure. The default setting is 0.2 seconds and
usually results in a square shaped pressure waveform. Patients with stiff lungs e.g. brittle
asthmatics/ARDS may benefit from a slightly slower rise time e.g. 0.35 seconds. However,
if the rise time is too slow (e.g. > 0.5 seconds) the pressure waveform becomes more
rounded or slanted in appearance when it should be more square. This may also potentially
risk a decrease in the delivery of the tidal volume.

Volume Control Ventilation or SIMV - appropriate tidal volume & safe airway pressures
Respiratory Rate (or frequency) x Tidal volume = Minute volume
Example: RR 12 x 500ml = 6000ml or 6.0 litres per minute.
This is a volume-derived mode
Volume-derived modes enable delivery of fixed tidal volume.
This means that breath by breath the tidal volume usually remains constant.
Volume-derived modes have no respect for increasing airway pressures. This means that if compliance and resistance is increased, then the machine will still attempt to deliver the fixed tidal volume, but the airway pressure becomes compromised. The airway pressure will increase. The airway pressure alarm limit needs to be carefully set so that nursing and medical staff can be alerted to the higher airway pressures. If the ventilator’s airway pressure alarm isn’t appropriately set – then there’s a risk that any high airway pressures generated may go unnoticed. There is a need to inform medical staff if the airway pressure increases beyond 30.
The initial tidal volume depends on numerous factors, most notably the disease for which the patient requires mechanical ventilation
Acute Respiratory Distress Syndrome (ARDS) – randomised trials found that mechanical ventilation using tidal volumes of ≤ 6ml/kg ideal bodyweight improved mortality in patients with ARDS.
Non-ARDS patients – the optimal tidal volume for patients who are mechanically ventilated for reasons other than ARDS is unclear. Based upon limited data, a tidal volume of 6 to 8 ml per kg of ideal bodyweight is a reasonable tidal volume in patients without ARDS.
Example of fixed tidal volume ventilation
Good Compliance Poor Compliance
No. of resps Tidal volume AP No. of resps Tidal volume AP
Breath 1 500ml 25 Breath 1 500ml 25
Breath 2 500ml 25 Breath 2 500ml 26
Breath 3 500ml 25 Breath 3 500ml 27
Breath 4 500ml 25 Breath 4 500ml 28
Breath 5 500ml 25 Breath 5 500ml 29
Breath 6 500ml 25 Breath 6 500ml 30
Breath 7 500ml 25 Breath 7 500ml 31
Breath 8 500ml 25 Breath 8 500ml 32
Breath 9 500ml 25 Breath 9 500ml 33
Breath 10 500ml 25 Breath 10 500ml 34
Breath 11 500ml 25 Breath 11 500ml 35
Breath 12 500ml 25 Breath 12 500ml 36
Airway pressure is determined by the airway resistance, lung compliance, and chest wall compliance. When compliance is poor the ventilator will still deliver 500ml unless the airway pressure parameter has been set to alarm when it exceeds 30. When the airway resists the 500ml tidal volume, the ventilator will alarm ‘volume not constant’.
6.

Autoflow
Autoflow is a not a ventilator mode but it is a function that helps to regulate the pressure at the level of the plateau (represents alveolar ventilation) and is commonly used in volume control modes.
Autoflow should always be switched on when using SIMV mode – go to Extra settings and switch on.
SIMV + Autoflow – the tidal volume is delivered at the level of the plateau.
If autoflow is not switched on: the waveform is volume control and there may be a noticeable difference between peak and plateau pressures. SIMV + Autoflow is generally safer than VC alone as in poor lung compliance it (1) helps to avoid excessive shearing pressures during the onset of inspiration (2) distributes the tidal volume evenly throughout the inspiratory phase and (3) reduces significant differences of pressures recorded between peak and plateau pressures.
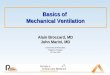
When mode is changed from VC without autoflow → SIMV with autoflow the following is observed
1. Figure 1 shows a volume control breath without autoflow. Note the difference between the peak and the plateau pressure. The waveform shape is irregular.
2. Figure 2 shows what happens when the autoflow function is switched on. A ‘test’ breath searches for the level of the plateau.
3. Figure 3 shows how autoflow enables delivery of the tidal volume at the level of the plateau. The
waveform morphology is more regular and square-shaped. Observe that the peak and the plateau pressures are now the same.
7.
Figure 1 Figure 2 Figure 3
------- = 25
Peak = 35 ------
--

Pressure Control Ventilation Settings
Pressure Control-BIPAP mode enables the patient to breathe between 2 pressure levels
P. insp = inspiration pressure. This equates to peak airway pressure. What you set on the PINSP means the airway pressure is the same. So if the Pinsp is set at 24, the peak airway pressure (Peak AP on the patient’s observation chart) will be 24. Pressure control helps protect the lung from rising pressures as the PINSP is fixed and kept ≤ 30.
PEEP = expiration pressure. PEEP = Positive-End Expiratory Pressure. This is the application of a constant positive pressure so that at the end of expiration, the airway pressure does not return to 0 baseline. Therefore PEEP helps prevent alveoli collapsing during expiration and helps to recruit collapsed alveoli by keeping the alveoli expanded. A typical level initiated is around 5cm H20.
Pressure Control/PC-BIPAP basic settings
8.
Pinsp
FiO2
FiO2 is abbreviation for Fraction Inspired Oxygen and ranges 21% (room air) to 100%.
0.30 = 30%, 0.40 = 40% etc and 1.0 = 100% The value displayed on the ventilator may be
recorded on the patient’s observation chart as a fraction or as a percentage.
The value may be recorded as a fraction or percentage on the patient’s observation chart
Pinsp
Pinsp is abbreviation for Inspiration pressure. A fixed amount of pressure is delivered with
each breath. There is no preset tidal volume key in the pressure control mode. Instead,
the level of pressure set determines the tidal volume. If the recorded tidal volume is low,
the Pinsp may need to be increased. The Pinsp is the same as the airway pressure and
should not exceed 30. If the recorded tidal volume is high, the Pinsp may need to be
decreased. On the observation chart this is expressed as Pinsp/PC
Ti
Ti is abbreviation for Inspiration Time. Using 12 breaths per minute as an example, if we
divide 60 seconds by 12 – this informs us that one breath will be completed over 5
seconds. If the inspiration time is 1.7 seconds then the expiration time will be 3.3
seconds (1.7 + 3.3 = 5 seconds for one breath). The inspiration:expiration ratio or I:E
ratio is derived from these figures e.g. divide 3.3 by 1.7 to obtain I:E ratio of 1.9 or 1:1.9.
Normal I:E ratio approximates 1:2 in healthy individuals so expiration time is twice as long
as inspiration. However the I:E ratio may be changed to 1:3 or even 1:4 for certain patient
groups e.g. asthma sufferers. When the Ti parameter is touched the I:E ratio is displayed.
20

9.
RR
RR is abbreviation for Respiratory Rate. In VC mode this parameter means that all
patients will get mandatory breaths e.g. 12 breaths per minute. On the observation
chart this is expressed as Vent Rate. All patients that are deeply sedated will require
mandatory breaths – so that they can safely breathe. For most patients, an initial
respiratory rate between 12 and 16 breaths per minute is reasonable, although it may
be modified according to the ventilator mode. If the patient’s sedation level is
improving and the patient starts to make spontaneous breathing effort, the total
respiratory rate will be higher. On the observation chart this is expressed as Spont
Rate.
RR X Tidal volume = minute ventilation and this can range 6.0 to 10.0 litres (average
8.0 litres)
PEEP
PEEP is abbreviation for Positive End Expiratory Pressure. This is the application of a
constant positive pressure so that at the end of expiration, the airway pressure does
not return to 0 baseline. Therefore PEEP helps prevent alveoli collapsing during
expiration and helps to recruit collapsed alveoli by keeping the alveoli expanded. A
typical level initiated is around 5cm H20. However, a higher level of PEEP (up to 20cm
H20) is sometimes used to improve refractory hypoxaemia or reduce ventilator-
associated injury in patients with acute lung injury, acute respiratory distress
syndrome or other types of hypoxaemic failure. Elevated levels of PEEP can have
adverse consequences such as reduced preload (decreases cardiac output), elevated
plateau airway pressure (increases risk of barotrauma), and impaired cerebral venous
outflow (increases intracranial pressure).
P
Supp
P supp is abbreviation for Pressure Support. Whenever the patient initiates a
spontaneous breath, the ventilator delivers support to the breath according to the
preset pressure level. The pressure support level can range from around 5cm H2O up
to 20cm H2O.
The tidal volume that results is dependent on the preset pressure and the patient’s
lung compliance. Some patients may need higher levels of support if the tidal volume
is reduced. As the patient is weaned from mechanical ventilation, the level of support
is gradually reduced down to around 5cm H2O. Titration of support usually involves
increasing or decreasing by 2cm H20.
Slope
Slope refers to the inspiratory rise time. The inspiratory rise time determines the amount
of time it takes to reach the desired airway pressure. The default setting is 0.2 seconds and
usually results in a square shaped pressure waveform. Patients with stiff lungs e.g. brittle
asthmatics/ARDS may benefit from a slightly slower rise time e.g. 0.35 seconds. However,
if the rise time is too slow (e.g. > 0.5 seconds) the pressure waveform becomes more
rounded or slanted in appearance when it should be more square. This may also potentially
risk a decrease in the delivery of the tidal volume.

Pressure Control mode (PC) or Bi-Phasic Positive Airway Pressure mode (BIPAP)
Respiratory Rate (or frequency) x Tidal volume = Minute volume
Example: RR 12 x 500ml = 6000ml or 6.0 litres per minute.
BIPAP enables the patient to breathe between 2 pressure limits
1. P. insp = Inspiration pressure. This equates to peak airway pressure. What you set on P.insp means the airway pressure is the same. Avoid peak airway pressure ≤ 30. P.insp helps protect the lung from rising pressures as inspiration pressure is fixed at a preset value and usually maintained ≤ 30.
2. PEEP = Expiration pressure. PEEP = Positive-End Expiratory Pressure. It helps inflate alveoli and keep alveoli open at the end of expiration. Useful to augment FIO2. If the PEEP level is increased the tidal volume may drop. This means that the P.insp may need to be increased too. Conversely if the PEEP level is decreased, the tidal volume may increase. This may mean that the P.insp needs to be decreased too.
TV – the tidal volume generated occurs between the 2 levels – inspiration and expiration.
TV in PC/ BIPAP mode will often vary breath by breath and will depend on lung compliance.
Inspiration pressure is fixed so the peak airway pressure will equalise the PINSP setting. So if the P.INSP is set at 20, then the peak pressure will be 20.
If lung compliance is good then 12 breaths x 500ml should remain fairly constant and MV = 6.0 litres.
10.
1. Inspiration pressure = Pinsp
2. Expiration pressure = PEEP
-----------------------------------------------------------------
-------- - ----------------------------------------------------
-------------

However if lung compliance is poor, along with increased resistance, the TV is likely to vary breath by breath.
Example –
- Breath 1 = 200ml AP 22 - Breath 2 = 400ml AP22 - Breath 3 = 250ml AP22 - Breath 4 = 150ml AP22 - Breath 5 = 300ml AP22 - Breath 6 = 100ml AP22 - Breath 7 = 200ml AP22 - Breath 8 = 400ml AP22 - Breath 9 = 250ml AP22 - Breath 10 = 150ml AP22 - Breath 11 = 300ml AP22 - Breath 12 = 100ml AP22
___________________
12 breaths = total of 2.8 litres minute ventilation.
Manipulating the tidal volume delivered or minute ventilation in PC mode
To increase tidal volume or minute ventilation
Consider increasing the Pinsp (Maintain Pinsp or peak pressure ≤ 30)
Consider increasing the respiratory rate
A combination of the above may be needed
To decrease tidal volume or minute ventilation
Consider decreasing the Pinsp
Consider decreasing the respiratory rate.
A combination of the above may be needed
To increase PACO2
Consider reducing the respiratory rate.
Consider reducing the Pinsp.
A combination of the above may be needed
To decrease PACO2
Consider increasing the respiratory rate.
Consider increasing the Pinsp (but avoid Pinsp or peak pressure greater than 30).
A combination of the above may be needed 11.
In Pressure Control mode or BIPAP mode the
airway pressure remains constant at the pre-set level so if
the Pinsp is set at 22, the airway pressure will not exceed 22.
However, the tidal volume will vary breath by breath and
may well decrease depending on lung compliance
22 14

Spontaneous breathing whilst in VC/SIMV or PC/BIPAP modes In either of these modes, the ventilator delivers a set minimum number of mandatory breaths each minute, but also allows the patient to breathe spontaneously in between the mandatory breaths.
Observe the image below - M refers to delivery of mandatory breaths & S refers to spontaneous breaths.
The mandatory breath is square-shaped in appearance whilst the spontaneous breath is less pronounced and is more triangle-shaped in appearance. When spontaneous breathing occurs, the inspiratory and expiratory flow changes in colour (red circles)
When increased and sustained evidence of spontaneous breathing is observed – and depending on the patient’s underlying condition – it may be useful to consider changing the patient from a mandatory mode i.e. VC/SIMV or PC/BIPAP to a spontaneous mode i.e. Pressure Support (or SPN-CPAP/PS). This may also be appropriate during sedation interruption as it may enable the opportunity of a spontaneous breathing trial.
12.
M M M S S S

time
Airw
ays p
ressure
cm
H2O
0
5
CPAP with Pressure Support (CPAP ASB)
There is always positive airways pressure
The ventilator senses the inspiratory effort of the patient and
applies the Pressure Support (arrow)
CPAP set a 5 cm H2O, PS set at 10 cm H2O
Peak pressure is therefore 5 + 10 = 15 cm H2O
15
Pressure Support Mode
Draeger terminology is SPN-CPAP/PS – so nursing staff record this on the patient’s observation chart. SPN refers to ‘spontaneous’ and is of course a spontaneous breathing mode. This mode consists of spontaneous ventilation with all of the patient’s spontaneous breaths supported or augmented by the ventilator. In other words, a set pressure is added to each spontaneous breath. The initial pressure support level is determined by measuring the patient’s airway resistance. The pressure support level can range from around 5cm H2O up to 20cm H2O. Weaning from Pressure Support Ventilation → Start the PS level at 5 to 15 cm H2O – or as directed by medical staff - and adjust it gradually until the agreed target tidal volume is achieved.
The level of pressure support is only delivered when the ventilator senses the patient’s inspiratory effort. If the patient is too weak – pressure support won’t be delivered. Similarly if the patient is over sedated, then pressure support won’t be delivered. The level of pressure support selected should be appropriately titrated (usually this means either increasing or decreasing the level of pressure support by 2cm H20) to achieve the target tidal volume or tidal volume agreed by medical staff. The higher the level of pressure support selected, the greater the level of assistance is provided. If the patient becomes tachypnoeic, it may be due to the level of pressure support being set too low. This is usually confirmed by a low tidal volume. If this occurs, the level of pressure support should be increased so that a larger tidal volume (bigger breath) can be given to the patient and this in turn will help slow down the patient’s respiratory rate If the patient does not make any spontaneous respiratory effort, then no assistance will be provided and ‘Apnoea ventilation’ will alarm. It may be that the patient remains too sleepy or too weak and is not quite ready for weaning. Apnoea Ventilation must always be switched ON in spontaneous breathing modes.
13.

Continuous Positive Airway Pressure Mode (CPAP)
Continuous positive airway pressure is obtained using Positive-End Expiratory Pressure (PEEP)
In this mode the patient is breathing spontaneously and without any pressure support
Mandatory breaths are not delivered in this mode i.e. all ventilation is spontaneously initiated by the patient
Pressure support is not set in this mode. CPAP therefore may be regarded as the final stage of weaning the patient from mechanical ventilation. Some (but not all) clinicians prefer to use this mode to evaluate the patient’s readiness for extubation.
PEEP involves maintaining a constant preset pressure within the ventilator breathing circuit and the lungs. PEEP increases the end expiratory or baseline airway pressure greater than atmospheric pressure
This constant pressure is maintained throughout both the inspiratory and expiratory phases of the breath
This helps to keep the alveoli from collapsing, resulting in better oxygenation and increases functional residual capacity along with reducing the patient’s work of breathing.
Apnoea Ventilation must always be switched ON in spontaneous breathing modes.
In this mode, it may be useful to consider the use of automatic tube compensation as this adjunct may assist to overcome the airway resistance that’s required to move the gas through the resistance of the tracheal tube.
14.
Above: Constant pressure e.g. 5cm = PEEP

Automatic Tube Compensation (ATC)
Background
ATC is an adjunct to spontaneous breathing modes.
A method of overcoming the airway resistance that’s required to move the gas through the resistance of a tracheal tube.
The tracheal tube, of course, constitutes a major constriction within the airways and can increase the work of breathing for the patient.
The smaller the diameter of the tube, the greater resistance/work of breathing.
It has thought that the increased work of breathing imposed by the resistance of the ETT may contribute to weaning intolerance
ATC compensates for the flow in regulating the pressure difference between the 2 ends of the tracheal tube
ATC is not required in mandatory modes e.g. BIPAP/PC or VC/SIMV.
How does it work?
The flow of gas through the tracheal tube results in a difference in pressure between the 2 ends (y-connector end and carinal end)
The respiratory muscles have to compensate for this difference by creating a powerful negative pressure in the lung.
This greater work of breathing can be cancelled out by increasing the pressure at the top end of the tube so that pressure at the lower end (carina) is decreased thereby reducing the patient’s work of breathing.
When ATC is activated, the dimensions and physical properties of the tube are known, so the ventilator can continuously calculate the pressure difference across the tube and regulate accordingly.
15.

Automatic Tube Compensation (ATC)
Research Studies
SPN-CPAP/PS – the use of low pressure support levels e.g. 5 to 10cmH20 has also been proposed to compensate the effect of resistance caused by the tracheal tube.
Majority of our ICU patients are managed with SPN-CPAP/PS
Very few patients are managed with just CPAP i.e. PEEP set – but PS not set.
No statistical difference between ATC and PS.
Evidence from low quality randomised trials and meta-analyses suggest that although no single spontaneous breathing trial (SBT) method (i.e. T-piece, low level of PS, ATC or CPAP) is clearly superior to the other, that SBT with low levels of PS is preferred.
ATC used at the discretion of the ICU Consultant.
How to activate ATC
Ventilation settings →Additional settings
Select ATC tab
Tube Comp (ATC) → on → click rotary knob to confirm
Select tube type → Touch ET or Trach → click rotary knob to confirm
Enter the patient’s tube size.
Enter the degree of compensation → 100%
16.
By increasing the pressure at the top of the tube,
the patient is deliberately relieved of the
artificially increased work of breathing.
This can be illustrated using a simple example
shown opposite: a person pulling a car will have
to work less hard the more the person at the
back pushes.

Automatic Tube Compensation (ATC)
Visual confirmation that ATC is activated
ATC is displayed below SPN-CPAP/PS - see figure 2
The tube size is displayed to the right of ATC - see figure 2
The tracheal pressure curve is shown as a green line on the ventilator screen.
The green line represents the pressure of the carina.
Figure 1
Figure 2
Note
If ATC is used in mandatory modes, the compensation only works during exhalation and when the patient triggers a spontaneous breath. If ATC is used in mandatory modes the digital recordings for airway pressure may appear very different e.g. PC setting is 28 (pre-ATC) but digital value often higher when ATC is used so could be demonstrating airway pressure readings of 30+. The figure above right shows this.
Avoid using in mandatory modes i.e. VC/SIMV or PC/BIPAP mode.
17.
SPN-CPAP-PS
Green line = carinal pressure

What are Ventilator Alarms?
If an alarm occurs, this indicates that there is a problem with the pressure, volume, or rate of air being delivered. In most cases, the bedside nurse should always check and assess the patient first prior to troubleshooting the mechanical ventilator.
1. Kinked or blocked circuits or tubing Always check and assess the patient first - When an alarm sounds, the role of the bedside nurse is to immediately check the patient’s
condition to assess the severity of the problem and determine the need for immediate resuscitation. If the patient is stable, the next step is to find kinked or blocked tubing that’s impairing air flow.
- Ventilator/circuit problems can sometimes be more easily distinguished from ET/patient problems by disconnecting the patient from the ventilator and manually bagging the patient with a manual resuscitation bag.
2. Problems causing high airway pressure alarms - high-pressure alarms occur if the mechanical ventilator reaches the set limit or if the breath ends and the following are commonly associated Always check and assess the patient first
- Accumulation of mucus or other secretions in the patient’s airway due to inadequate humidity.
- Biting of the ET tube
- Bronchospasm
- Coughing, gagging, or “fighting” the ventilator breath
- Decreased respiratory system compliance e.g. due to pneumothorax, tracheal tube displacement or decreased ventilation in the lungs
- Inappropriate settings e.g. excessive tidal volume, shorter inspiratory time, or a very low preset high airway pressure alarm)
- Kinked or blocked circuits or tubing
- Ventilator malfunction
- Water in the ventilator circuit or filter – change the ventilator filter when heavy condensate appears.
18.

3. Problems causing low airway pressure alarms – low-pressure alarms occur if the pressure inside the breathing circuit falls below the set limit on the mechanical ventilator
Always check and assess the patient first
- ET tube is disconnected from the ventilator circuit.
- The tracheal tube cuff is not adequately inflated
- Loose circuit and tubing connections
- Poorly connected humidifier sensor probes
- The patient requires higher levels of air than the mechanical ventilator is delivering.
4. Problems causing high respiratory and low respiratory rate alarms
High and low rate alarms can be caused by increases or decreases beyond the limit set for the alarm.
Always check and assess the patient first
- A low rate alarm, or also known as “apnoea alarm”, indicates that the patient has stopped breathing.
- This alarm is usually triggered by disconnected tubing. On the other hand, high rate alarm occurs when the patient experiences an increase in respiratory rate due to agitation or fatigue.
5. Problems causing high and low rate alarms
High and low rate alarms can be caused by increases or decreases beyond the limit set for the alarm.
Always check and assess the patient first
- A low rate alarm, or also known as “apnea alarm”, indicates that the patient has stopped breathing.
- This alarm is usually triggered by disconnected tubing. On the other hand, high rate alarm occurs when the patient experiences an increase in respiratory rate due to agitation or fatigue.
6. Problems caused by high and low inspiratory volume alarms
Always check and assess the patient first
- High volume inspiratory alarms can be caused by several factors such as leaking or disconnected tubes, increased respiratory rate, or increased demand for air due to pain, anxiety, or improper ventilator settings.
- On the other hand, low volume inspiratory alarms may be caused by accumulation of mucus secretions, tube obstruction, or a lower respiratory rate.
19.

7. Problems caused by high and low minute ventilation alarms
Always check and assess the patient first
- Low MV alarms → check that the lower alarm limit hasn’t been set too high → check for any loose circuit connections and check tracheal tube has not migrated → could there be an obstruction e.g. mucous plug? → attempt passing a suction catheter. Check that the tracheal cuff pressure is adequately inflated. Has a sedative bolus been given recently? Could the patient be over-sedated?
- High MV alarms → check that the upper alarm limit hasn’t been set too low. Is the tidal volume level, Pinsp or level of pressure support set too high? Is the patient more awake? Check that the ventilator filter is not water-logged.
8. Apnoea ventilation alarm
Always check and assess the patient first
- The apnoea ventilation alarm is activated in spontaneous modes of breathing i.e. Pressure Support or CPAP modes. This means that if the patient fails to initiate a spontaneous breath within a set period of time (apnoea alarm limit) then the ventilator will automatically deliver mandatory or rescue breaths to the patient.
- At the start of each shift the bedside nurse should check the apnoea ventilation settings and record them on the ICU observation chart. The default settings are 12 breaths and 450ml tidal volume. The apnoea alarm limit is usually set to 20 seconds and this can be found under the ‘alarms’ key.
- When the apnoea ventilation alarm is triggered → assess the patient → check apnoea alarm limit → check oxygen saturations → prompt the patient to take a breath in → press the alarm reset button if the patient appears to respond. However, if the patient is showing signs of increasing fatigue, and the apnoea ventilation alarm continues → the patient needs to resume a mandatory mode of ventilation i.e. either PC/BIPAP or VC/SIMV.
- It’s also important that the bedside nurse checks and records the flow trigger at the start of each shift. The default flow trigger setting is 2 litres per minute. Do not reduce the flow trigger below 2 litres as this will increase the risk of auto-cycling – see image below. Observe the relative uniformity of the ‘breaths’ which helps distinguish this from just rapid breathing, where there will be some variability.
20.

Trigger sensitivity, rise time and intrinsic PEEP explained
Trigger Sensitivity
The point at which the act of drawing breath is detected
Trigger sensitivity determines how easy it is for the patient to trigger the ventilator to deliver a breath.
A trigger sensitivity that is too sensitive may cause a breath to be delivered in response to patient movement or subtle pressure deflections caused by water moving within the ventilator tubing.
In contrast, a trigger sensitivity that is not sensitive enough increases patient effort. This may cause a prolonged period between the initial effort and the ventilator breath or patient-ventilator asynchrony.
Rise Time
Time taken (in seconds) to inflate the lung to set pressure
Determines speed of rise of flow or pressure
Very short rise times may be more uncomfortable for the patient (especially for those with brittle lung disease)
Long rise times may result in a lower tidal volume being delivered
Intrinsic PEEP – the inability to fully exhale
Occurs when inspiratory time is too long and expiratory time is short.
Can also occur when respiratory rate is high – so expiratory time is short.
Often seen in chronic obstructive pulmonary disease/asthma.
Insufficient expiratory time results in insufficient time for the alveoli to empty before the next breath. Also referred to as “gas trapping”.
Can be measured on some ventilators (expiration hold control) or by observing flow or pressure patterns.
21.