Embed Size (px)
Citation preview

Understanding Historical and Contemporary Fertility
Transitions: A Birth Interval Approach
George Alter
University of Michigan
–
Date of last revision: (November 2016)
DO NOT CITE WITHOUT AUTHORS’ PERMISSION

1
Abstract
In a widely cited article, Knodel and van de Walle attributed the European fertility transition
to the emergence of "stopping" behavior (terminating childbearing before the end of the end
of a woman's reproductive years) and suggested that this model was being repeated in other
regions. The prevalence of "stopping" has become especially important for understanding
fertility trends in Africa, where some observers see increasing use of modern contraception to
increase the spacing between births. This paper uses a new approach based on the analysis of
birth intervals to identify the extent of stopping and spacing in German villages, Taiwan,
Cameroon, Ghana, and Mali. The German and Taiwanese data largely confirm Knodel and
van de Walle's description, but stopping appears at very low family sizes more rapidly than
they expected. There is no evidence that stopping was related to birth order in the African
case studies, but spacing between births did increase.

2
Introduction
In 1979 John Knodel and Etienne van de Walle summarized more than two decades of
research in historical demography in the form of “Lessons from the Past” (Knodel and van de
Walle 1979). They presented a set of hypotheses about the European fertility decline with
important implications for population policy in countries still experiencing unprecedented
rates of population growth. A central feature of their interpretation is the view that the
diffusion of knowledge about and attitudes favorable to contraception triggered European
fertility transitions.
The steady and irreversible increase in the practice of family limitation under a
diversity of social and economic conditions in Europe suggests that the idea of
controlling the number of children born rather than leaving it to fate has a wide appeal,
once the possibility of control is realized. The steady decline in marital fertility may
reflect a combination of increasing efficiency in the practice of family limitation and
falling desired family sizes. Indeed, these two factors may interact. Only after the
possibility of effectively limiting childbearing becomes a reality and its advantages
become fully appreciated does it make sense to couples to aim for even smaller family
sizes.
If our hypothesis is correct, the high and relatively constant fertility that
characterizes predecline societies corresponds essentially to a period in which it is not
widely acknowledged that reproduction can be manipulated within marriage. Couples
do not have target family sizes. They accept, in some cases reluctantly, as many
children “as God sends.” … The appearance of articulated desires concerning family
size may coincide with or shortly precede the realization that reproduction can be
manipulated; and once methods are on hand by which smaller and smaller family sizes
can be attained by successive cohorts of couples, the norm about size starts to evolve
downward. (Knodel and van de Walle 1979: 235)
In 1979 the debate over population policy was between promoters of family planning
programs and advocates of economic development (“development is the best birth control”).
Knodel and van de Walle came down squarely in favor of family planning but with an
emphasis on the importance of culture values, especially the status of women.
The last two decades have cast considerable doubt on the lessons drawn by Knodel and van de
Walle. In particular, fertility rates in Sub-Saharan Africa began to come down, but they do
not appear to be following the same script. Caldwell, Orubuloye, and Caldwell (1992) were
among the first to predict that African fertility declines would be different. It was well known
that birth spacing tended to be wider in Africa than in most other regions, and research by
Bledsoe and others began to find evidence that women were using modern contraception to
extend birth intervals without intending to limit their family size (Bledsoe 2001; Johnson-
Hanks 2007; Timaeus and Moultrie 2013).
One of the problems in this literature has been distinguishing between spacing (longer birth
intervals) and stopping (intentional termination of childbearing). Most of the literature in
historical demography has inferred the presence of family limitation from age-specific fertility

3
rates, which are affected by both spacing and stopping (Okun 1994, 1995). While the
principles for estimating stopping and spacing for birth intervals have been known for some
time, they have only recently been applied to these data.
In this paper I revisit well known data to provide new estimates of stopping and spacing for
cases in Europe (Germany), East Asia (Taiwan), and Africa (Cameroon, Ghana, and Mali).
The results support Knodel and van de Walle’s view that European and East Asian fertility
transitions were due to parity dependent family limitation, i.e. stopping. However, I find that
couples rapidly moved to very small families, rather than the stepwise decline in family size
described in the quote above. I also show important roles for both spacing and stopping in
African fertility transitions, but in patterns that suggest a different kind of decision making
than occurred in either Europe or East Asia.
Stopping, Spacing, Postponement, Timing
In historical demography stopping and spacing are usually discussed in reference to Louis
Henry’s (1961) concept of “natural fertility.” Henry argued that large differences in levels of
fertility are possible among populations that are not practicing family limitation. Extended
breastfeeding and post-partum abstinence reduce fertility by lengthening birth intervals, but
they are consistent with “natural fertility” as long as they are practiced after every birth
regardless of birth order. Natural fertility is often linked to the hypothesis that family
limitation was not practiced in pre-transition populations because methods of birth control
were either unknown or culturally unacceptable (“unthinkable”) (Aries 1960; Coale 1973).
Knodel and van de Walle (1979) point out that fertility declines in Europe were not related to
the level of infant mortality, which implies that couples were having more children than they
wanted. In other words, the “supply” of children exceeded “demand” well before the
transition to low fertility began.
Critics of the “natural fertility” hypothesis have attached several different meanings to the
concept of spacing. Some have argued that birth spacing was used to increase the intervals
between births with the goal of reducing completed family size. Research on Utah and
Quebec suggest that birth spacing was a way to achieve smaller families in groups with strong
religious opposition to family limitation (Anderton and Bean 1985; Gervais and Gauvreau
2003). Other studies argue that evidence of birth spacing contradicts the hypothesis that
couples in pre-industrial Europe were unable or unwilling to intervene in the process of
reproduction. Alfred Perrenoud (1988) suggested that couples may have substituted stopping
for spacing as knowledge of birth control increased in the nineteenth century.
Timaeus and Moultrie (2008) proposed the term “postponement” to describe fertility control
that is neither stopping nor spacing. “By postponement, we mean delaying having another
birth for reasons other than the age of one’s youngest child (i.e., spacing) or one’s existing
family size (i.e., stopping).” (Moultrie, Sayi and Timaeus 2012:241) They point out that
couples in the West often postpone childbearing for economic, professional, or other reasons
(Morgan 1991). If a couple in the West delays their first child until they are established in
their careers, we do not think of this as birth spacing but as a choice enabled by effective
contraception. When African couples have access to contraception, they should be expected
to postpone births in response to opportunities and adversities in their lives too. Agadjanian
describes this behavior as “waiting.” “Women and men want to wait and see how their
material conditions and marital relations will evolve, whether their children will survive, and

4
even whether their relatives, friends, or neighbors will have another child.” (Agadjanian
2005:628)
In my opinion “postponement” leads to terminological complications that can be avoided by
the using “timing” to describe these decisions. “Postponement” refers to an event that is
expected to happen in the future, but some authors use postponement in a way that is difficult
to distinguish from “stopping.” For example, Lightbourne (1985) uses “permanent
postponement” to describe women whose desire for another child at some point in the future
is much weaker than their motivations to avoid childbearing in the present, but this
“postponement” is “permanent” only in retrospect. A woman may prefer want another birth
but never decide that the “time” is right. We should recognize that reproductive decisions
reflect the interplay of preferences, capabilities, and resources that are constantly changing.
“Timing” is about the circumstances that motivate couples in the present, and it implies that
we can study the events and conditions that cause couples to delay their next birth.
Historical demographers have ample evidence that fertility responded to economic conditions
long before the advent of family limitation. Many studies report correlations between births
and prices before and after the Industrial Revolution, including Dorothy Thomas’s (1941;
1927) classic work on demographic responses to business cycles (Galloway 1988). The
Eurasia Project devoted an entire volume to the analyzing the effect of harvest prices on
fertility in nineteenth-century Belgium, China, Italy, Japan, and Sweden (Tsuya 2010). Birth
control is not the only factor linking economic conditions to fertility. Malnutrition could
reduce both fecundity and libido, and couples were often separated when men sought work in
more distant places. But avoiding births in bad times did not require modern contraceptives.
How many men slept in the barn, because it was a bad year to have another child? (See also
Johnson-Hanks 2002 on the use of periodic abstinence in Cameroon.) Bengtsson and Dribe
(2006) find that farmers in southern Sweden were reduced fertility in anticipation of a bad
harvest not when their provisions ran out months later.
Caroline Bledsoe (Bledsoe, Banja and Hill 1998; Bledsoe and Banja 2002; Bledsoe et al.
1994) offers insights into the reasoning of African women that explain behaviors that
contradict demographers’ expectations. Bledsoe and colleagues (Bledsoe et al. 1998) find
that African women are very conscious of the physical toll that reproduction takes on their
health. Each pregnancy reduces a woman’s limited capacity to bear and nurse children, and
adverse events, like an infant death, miscarriage, or stillbirth, hasten that depletion.
Lengthening the time between births allows more time for the mother to rest and recover her
strength, which increases the chances that her next birth will survive. Consequently, Gambian
women use modern contraception after an infant death in order to have more children. This
reasoning is completely contrary to conventional expectations in demography, in which a
child death provokes a “replacement effect” increasing the likelihood of another birth.
Another implication of this “body resource expenditure” view is that the process of aging is
more strongly linked to reproductive events than to calendar age. When she finishes
childbearing a woman will be physically “spent” and dependent on her husband and sons to
reward her for sacrificing her health by providing support in her old age. Thus, this view
implies that women will retire from childbearing when their reproductive health has been
successfully converted into moral capital.
This paper looks at stopping and spacing in the way most closely aligned to Henry’s natural
fertility hypothesis. Percent stopping and median birth intervals are estimated by birth order
for birth cohorts of women before and during fertility transitions. Organizing the data by

5
birth cohort avoids distortions due to changes in age at marriage and birth intervals, the
“tempo” of childbearing (Rodriguez 2006), that affect period estimates of fertility. However,
birth cohort estimates have their own drawbacks. Events influencing the entire population,
like a new family planning program or an economic shock, affect successive cohorts at
different ages. This paper also does not look for changes in the timing of births in response to
life course events. If women were becoming more likely to delay births for reasons other than
family size, it will appear as an increase in birth spacing in this analysis. The methods used
here are not well suited for identifying timing effects. In other work, I have begun using
regression-like methods that are more appropriate for measuring responses to life course
events, like a child death, harvest failure, unemployment, or migration (Alter 2013;
Yamaguchi and Ferguson 1995)
Methods
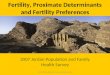
The method used here to estimate stopping and spacing is illustrated in Figure 1. The data for
this figure are drawn from women who had at least two births in the 1987 Taiwan KAP. The
downward sloping curve is the “survival curve” for a birth interval reconstructed by the
Kaplan-Meier method (Cleves et al. 2010; Kaplan and Meier 1958). Its height is the percent
of women who were still waiting for another birth. In this example three fifths of women had
their third birth within 33 months, reducing the survivor curve from 100% to 40%. After this
point the slope of the curve levels off and converges to a horizontal line, meaning that no
additional births are likely to occur. I follow the Casterline and Odden (2016) in choosing the
height of the survivor curve at 144 months as the percent of women who will not have another
birth. In the example illustrated in Figure 1 18% of birth intervals have not been completed
by 144 months. In other words, 18% of women in Taiwan stopped childbearing after their
second child.
The median length of a completed birth interval can also be determined from the survivor
curve by removing those who will never have another birth. Again, I follow Casterline and
Odden (2016) in using the height of the survival curve at 144 months to adjust the survivor
curve for women who will never have another birth.
𝑆𝑡∗ =
(𝑆𝑡 − 𝑆144)
(1 − 𝑆144)
In this formula St is the proportion of all women who have not had a birth t months after the
previous child, and S*t is the proportion of ever-completed intervals that have not been
completed by month t. In Figure 1 the median completed birth interval occurs between 24
and 25 months, when the proportion of ever-completed birth intervals drops from 53% (= (62
- 18)/72) to 48% (= (58 - 18)/72)).
Percentages of incomplete birth intervals by birth order can be used to estimate parity
progression ratios. The two quantities are complements:
PPRi = 1 - S144,i
where PPRi is the parity progression ratio from parity i to parity i+1, and S144,i is the
percentage of incomplete birth intervals 144 months after birth i. This also means that the
birth interval survival function can be used to estimate the total fertility rate for a cohort
(TFRC) by

6
𝑇𝐹𝑅𝐶 =∏(1 − 𝑆144,𝑖)
𝑘
𝑖=0
Data
Germany Historical data about Germany come from family reconstitution studies of sex villages
collected by John Knodel (1987; 1988) from village genealogies. Four villages come from
Protestant areas: Braunsen (Waldeck), Massenhausen (Waldeck), Middels (East Friesland),
and Oshelbronn (Würtetemburg). Two villages (Kappel and Rust) are in Baden, which was
predominantly Catholic. The data begin as early as 1583, and end in the twentieth century.
While some villages have data after 1940, most of the twentieth century data refer to the early
part of the century, and the average birth year for children in the study was 1918. The
transition to low fertility in these villages occurred at the end of the nineteenth century.
Knodel (1988:288-293) finds little evidence of family limitation before 1875.
The analysis presented here follows the rules for analyzing family reconstitution data
developed by Louis Henry. Henry (1980:67) restricts fertility analysis to family histories that
ended with the death of either the husband or wife. Family histories ending with the date of
birth or date of death of a child, are biased toward higher fertility rates. Indeed, it is
impossible to study stopping in such families, because all birth intervals are closed by a birth.
The implication of Figure 1 is that family limitation will increase the percentage of
incomplete (open) birth intervals in a population. Unfortunately, this important lesson has
been forgotten in some recent studies, which makes their analyses of birth spacing highly
questionable (Van Bavel 2004; Van Bavel and Kok 2004).
Taiwan Fertility histories for Taiwan were collected in five waves of “knowledge, attitude, practice”
(KAP) surveys which were conducted in 1965, 1967-68, 1973, 1979, and 1986 (Chow, Chen
and Chang 2005a, 2005b; Sun and Chang 2002, 2005; Sun et al. 2005). Each of these surveys
collected a detailed fertility history from each woman, which in later waves included dates of
miscarriages and induced abortions. Unfortunately, women older than age 40 were not
interviewed, but this has a limited effect on the analysis conducted here, which focuses on the
six birth intervals. Data from all five waves have been pooled without weighting for this
analysis.
The KAP surveys cover a period of rapid fertility decline in Taiwan, which went from a Total
Fertility Rate (TFR) of 6.5 children per woman in 1956 to 2.2 in 1983 (Freedman, Chang and
Sun 1994). Non-governmental agencies began offering family planning services in Taiwan
during the 1950s, and family planning became government policy in the 1960s. By the 1980s
knowledge and practice of contraception was nearly universal (Freedman et al. 1994:326-
328).
Cameroon, Ghana, and Mali Three African countries are included here as examples of recent fertility transitions that
appear to be slow and incomplete. Data are drawn from Demographic and Health Surveys
(DHS), which are identified in Appendix Table 1. Surveys conducted in each country have

7
been pooled without any weighting. I have omitted the marriage to birth interval from these
data, because the dating of marriage is problematic in some countries.
Table 1 shows UN estimates of TFRs for these three countries since 1950. Each of these
countries shows a reduction in fertility since the 1980s. For example, the TFR in Cameroon
peaked at 6.7 children per woman in 1980-85 and declined to 4.8 in 201-15. The largest
decreases are in Cameroon and Ghana, where the TFR dropped by about two children.
Fertility in Mali remains higher (6.4), but its TFR has fallen by about 0.8 since 1985.
Results Tables 2-6 present three measures for each population: mean age at previous birth, percent of
intervals not completed, and median birth interval. Each measure is shown by birth cohort
and number of previous births. Thus, women with 0 previous births were in the interval
between marriage and first birth. Computations in this paper were done in Stata(StataCorp.
2015)
The length of birth cohorts vary across tables. I use 25 year intervals for the German villages,
where the fertility transition developed slowly, and 5 year intervals for Taiwan, which
experienced a very rapid transition.
Mean Age at Previous Birth Ages at birth are included in Tables 2-6 to show differences in age at marriage. The numbers
presented are the average ages of women at the beginning of each birth interval. This means
that the first column, “0 previous births,” shows the average age at marriage. Since results are
arranged by birth cohort, this table is also useful for locating these results in time.
The noteworthy feature of ages at birth is the much higher ages in the German villages due to
the late age at marriage in Europe. In most birth cohorts women in these villages were over
age 26 when they married and older than 28 at the birth of their first child. In contrast,
women in Taiwan married at age 21 and had their first birth a year later. Women in the
African samples were even younger: 19 years old in Cameroon and Mali and 20 in Ghana.
German Villages The results in Table 2 add interesting details about the fertility transition in these villages.
Most important is the broad increase in stopping behavior across all birth orders in the cohort
born 1875-1899. Stopping increased by 5% among those with only one previous birth and by
10% for those at parities 2 to 5. These changes are more important than they may appear,
because stopping at low parities has a cumulative effect on completed family size. Women
who stop after two births are not at risk of having 3, 4, or 5 children. A 10% increase in
stopping for women with two children reduces average completed family size by about half a
child. Consequently, average completed family size fell from 6.5 children in the 1800-25
birth cohort to 4.4 in the 1875-99 cohorts.
The increase in stopping offset the effects of small decreases in spacing. Median birth
intervals in the 1875-99 birth cohort were mostly one or two months shorter than they had
been for the same birth order before 1825. There does appear to be an increase in birth
spacing at low parities among women born after 1900, a pattern described by Casterline and
Odden (2016).

8
Taiwan Table 3 shows the rapid increase in family limitation in Taiwan during the 1960s and 1970s.
The percent of women not completing the interval after their second birth increased from
3.0% in the 1931-35 birth cohort to 19.7% in the 1951-55 cohort. The increase in stopping
among women with three previous births is even larger – from 7.6% to 56.5% in the 1931-35
and 1951-55 birth cohorts respectively. In contrast, stopping among women with only one
previous child rose from 1.3% to 3.0% across the same cohorts. Even in the 1961-65 birth
cohort only 9.3% of women stopped after one birth, which is 5% lower than in the transitional
1875-99 cohort of German villages. Thus, Taiwanese couples demonstrated a remarkable
convergence to 2-3 child families. In the 1961-65 birth cohort 69% of families stopped after
2 or 3 children compared to 10% in the 1931 birth cohort. This demonstrates not only the
pervasive adoption of contraception but also the broad consensus on desired family size in
Taiwan.
As we saw in the German villages, birth spacing decreased while stopping was increasing.
The median interval between the first and second birth fell from 25 months for women born in
the early 1930s to only 19 months in the 1961-65 cohort.
Cameroon, Ghana, and Mali The African populations described in Tables 4, 5, and 6 are a marked contrast to what we
observed in Germany and Taiwan. The proportion of women who stopped having children
before their sixth birth hardly changed at all. The only place showing any sign of stopping
behavior is Ghana, where women in the 1960-69 birth cohort were less likely to complete
birth intervals than earlier or later cohorts. Even in Ghana, however, there are no cells in
Table 5 where stopping increased by more than 6% over the 1940-49 birth cohort.
Table 7 shows that stopping behavior does show up at higher birth orders (6 to 10 previous
births) in Cameroon, Ghana, and Mali. The most recent DHS surveys find that ideal family
sizes remain high in these countries: 5.5 in Cameroon, 4.3 in Ghana, 5.9 in Mali (Cellule de
Planification et de Statistique (CPS/SSDSPF) et al. 2014; Ghana Statistical Service (GSS),
Ghana Health Service (GHS) and ICF International 2015). But there is little evidence of
parity-dependent family limitation in Table 7 with the possible exception of Ghana. Even in
Ghana there seems to have been a reversal of the trend toward more stopping in the 1970-79
birth cohort.
Median birth intervals tell a different story. Birth intervals grew longer in each of these
countries. The largest increases were in Ghana, where the intervals after first, second, and
third births increased from 31 months in the 1940-49 birth cohort to 37 or 38 months in the
1980-89 birth cohort. Median birth intervals in Mali increased by 4 to 8 months, and in
Cameroon the increase was three months at all birth orders.
This does not mean that stopping played no role in reducing fertility in these countries.
When we change our perspective from birth order to age, a clear pattern emerges. Table 8
shows increasing percentages of women in Cameroon, Ghana, and Mali stopped having
children after they passed age 35. Although there is no evidence of increased stopping at ages
under 35, all three countries show a higher percentage of incomplete birth intervals at ages
35-39 and in Cameroon and Ghana stopping at ages 40-44. In contrast, stopping increased at
all ages in the German villages and over age 25 in Taiwan.

9
Conclusions
The results presented here suggest that when we look closely at fertility transitions different
patterns of stopping and spacing emerge. The transitions in Germany and Taiwan fit the
classic pattern of parity-dependent family limitation described by Knodel and van de Walle
(1979). The KAP surveys captured the rapid movement of Taiwan to 2-3 child families. In
the 1960s and 1970s women with two or three children stopped having more children, but
there was no change in progress from marriage to first birth or first to second birth until the
1980s. There is little evidence of convergence to a normative family size in the German
villages, and no sign that the desired family size gradually descended from 6 to 5 to 4 in
successive generations. Instead we see some couples moving to 2- and even 1-child families
very early in the transition to low fertility.
The African countries examined are following very different trajectories in two key ways.
First, increased spacing between births is evident in each of the African cases, but birth
intervals were becoming shorter in both the German and Taiwanese fertility transitions.
Second, stopping behavior appears to be much more closely tied to age than to birth order in
the African cases. The evidence of parity-dependent family limitation is very weak even for
birth intervals above the ideal family sizes (4-5 children) reported in the DHS surveys (see
Table 7).
The implication of these comparisons is that fertility transitions in Africa are following a
different script. Although the fertility transition in Taiwan began almost a century after the
German transition, in both places fertility went down because couples stopped having
children when they reached a target family size. Few couples in Cameroon, Ghana, and Mali
appear to be aiming for target family sizes. But more and more of them are using
contraception to increase the spacing between births and to stop having children at older ages.
Overall, the African pattern appears to fit Caroline Bledsoe’s (2002) account of reproduction
in Gambia. At younger ages women use contraception to control the timing of births in the
interest of assuring the health of the child and the potential for future reproduction of the
mother. Older women retire from childbearing when their husbands and children repay the
sacrifices that they sustained through reproduction.

10
Figure 1. Birth Interval Survival Curve

11
Table 1.
Total Fertility Rates by Period,
Cameroon, Ghana, and Mali
Total fertility (children per woman)
Country Cameroon Ghana Mali
1950-1955 5.49 6.44 6.95
1955-1960 5.53 6.64 6.95
1960-1965 5.81 6.84 7.00
1965-1970 6.09 6.95 7.10
1970-1975 6.31 6.90 7.15
1975-1980 6.47 6.69 7.15
1980-1985 6.70 6.35 7.15
1985-1990 6.60 5.88 7.15
1990-1995 6.22 5.34 7.15
1995-2000 5.77 4.81 6.95
2000-2005 5.49 4.57 6.85
2005-2010 5.21 4.29 6.70
2010-2015 4.81 4.25 6.35
Source: (United Nations 2015)

12
Table 2
Mean Age at Previous Birth, Percent of Intervals Not Completed, and
Median Birth Interval by Birth Cohort and Number of Previous Births
German Village Reconstitutions
Number of previous births
Birth cohort 0 1 2 3 4 5
Mean age at previous birth
1725-1749 27.0 28.5 30.2 31.8 33.8 35.4
1750-1774 26.4 28.1 30.1 32.3 34.1 35.9
1775-1799 26.1 28.1 29.7 31.4 33.1 34.7
1800-1824 20.0 26.2 28.3 30.3 32.1 33.9
1825-1849 26.3 28.4 30.3 32.0 33.7 35.4
1850-1874 25.8 27.5 29.5 31.3 33.0 34.6
1875-1899 26.0 28.0 29.8 31.3 32.9 34.5
1900+ 25.6 28.0 30.5 33.0 33.9 34.2
Percent not completing the birth interval
1725-1749 1.2% 7.8% 7.8% 11.4% 11.0% 13.8%
1750-1774 0.2% 9.4% 5.8% 8.0% 8.9% 12.8%
1775-1799 0.6% 14.8% 8.2% 8.4% 8.2% 13.1%
1800-1824 0.2% 8.1% 7.4% 8.2% 9.8% 14.5%
1825-1849 0.2% 9.7% 9.0% 9.4% 13.1% 14.0%
1850-1874 0.5% 9.2% 7.5% 9.5% 12.1% 15.1%
1875-1899 0.7% 14.1% 19.6% 19.7% 22.2% 25.9%
1900+ 0.3% 17.7% 25.5%
Median birth interval
1725-1749 11 22 26 28 28 30
1750-1774 11 25 27 29 29 29
1775-1799 10 24 26 27 28 28
1800-1824 9 23 25 26 26 26
1825-1849 10 22 24 25 26 27
1850-1874 10 18 22 23 24 24
1875-1899 10 21 23 25 25 27
1900+ 10 30 36 Note: Estimates based on fewer than 100 births are omitted.

13
Table 3
Mean Age at Previous Birth, Percent of Intervals Not Completed, and Median
Birth Interval by Birth Cohort and Number of Previous Births
Taiwan KAP Surveys
Number of previous births
Birth cohort 0 1 2 3 4 5
Mean age at previous birth
1931-1935 20.5 21.9 24.1 26.5 28.5 30.5
1936-1940 21.2 22.4 24.4 26.3 27.8 29.3
1941-1945 21.1 22.1 23.9 25.9 27.4 29.0
1946-1950 21.2 22.1 23.8 25.2 26.7 27.5
1951-1955 21.4 22.4 23.7 25.1 26.1 26.2
1956-1960 21.2 21.8 23.1 23.7 24.6 27.6
1961-1965 20.3 20.9 21.5 22.6
Percent not completing the birth interval
1931-1935 1.5% 1.3% 3.0% 7.6% 17.7% 23.2%
1936-1940 0.5% 1.2% 4.9% 19.7% 40.7% 49.7%
1941-1945 0.4% 1.4% 9.0% 34.2% 56.9% 53.9%
1946-1950 1.0% 1.3% 14.7% 47.3% 58.6% 67.0%
1951-1955 0.4% 1.6% 19.7% 56.5% 58.3% 74.3%
1956-1960 1.5% 3.0% 22.2% 57.7% 72.5% 56.3%
1961-1965 2.8% 9.3% 41.4% 63.9%
Median birth interval
1931-1935 14 25 27 27 28 28
1936-1940 12 23 25 26 25 25
1941-1945 11 22 24 25 25 29
1946-1950 11 21 24 25 26 23
1951-1955 10 21 25 23 27 23
1956-1960 10 21 25 25 24 27
1961-1965 8 19 21 26 Note: Estimates based on fewer than 100 births are omitted.

14
Table 4
Mean Age at Previous Birth, Percent of Intervals Not Completed, and Median
Birth Interval by Birth Cohort and Number of Previous Births
Cameroon DHS Surveys
Number of previous births
Birth cohort 0 1 2 3 4 5
Mean age at previous birth 1940-1949 19.4 22.1 24.5 26.8 29.1
1950-1959 19.4 22.1 24.5 26.9 29.0
1960-1969 19.2 21.9 24.3 26.6 28.8
1970-1979 19.1 21.7 24.1 26.1 28.0
1980-1989 18.3 20.6 22.4 24.1 25.4
1990-1999 16.8
Percent not completing the birth interval 1940-1949 5.8% 6.8% 8.5% 6.2% 7.0%
1950-1959 5.1% 4.5% 5.9% 7.7% 9.7%
1960-1969 4.3% 4.8% 6.2% 7.7% 11.3%
1970-1979 4.3% 4.7% 4.9% 5.6% 5.5%
1980-1989 2.8% 0.9% 3.8% 3.3% 4.2%
1990-1999 0.0%
Median birth interval 1940-1949 26 26 26 28 28
1950-1959 28 26 26 28 28
1960-1969 28 28 28 28 29
1970-1979 29 29 29 31 31
1980-1989 29 29 29 31 31
1990-1999 31 Note: Estimates based on fewer than 100 births are omitted.

15
Table 5
Mean Age at Previous Birth, Percent of Intervals Not Completed, and Median
Birth Interval by Birth Cohort and Number of Previous Births
Ghana DHS Surveys
Number of previous births
Birth cohort 0 1 2 3 4 5
Mean age at previous birth
1940-1949 20.4 23.3 26.1 28.6 31.0
1950-1959 20.5 23.7 26.4 28.8 31.1
1960-1969 20.3 23.3 26.1 28.6 31.0
1970-1979 20.6 23.6 26.3 28.8 30.9
1980-1989 20.4 23.2 25.2 27.1 28.3
1990-1999 18.9
Percent not completing the birth interval
1940-1949 2.5% 3.6% 4.6% 6.4% 8.0%
1950-1959 2.9% 3.7% 5.9% 7.9% 10.5%
1960-1969 3.7% 5.1% 7.9% 11.5% 13.7%
1970-1979 3.3% 5.0% 6.8% 9.5% 12.5%
1980-1989 1.8% 0.9% 1.1% 6.6% 11.3%
1990-1999 2.4%
Median birth interval
1940-1949 31 31 31 32 32
1950-1959 32 34 34 34 34
1960-1969 34 34 35 35 36
1970-1979 37 37 38 38 38
1980-1989 37 38 37 35 35
1990-1999 36 Note: Estimates based on fewer than 100 births are omitted.

16
Table 6
Mean Age at Previous Birth, Percent of Intervals Not Completed, and
Median Birth Interval by Birth Cohort and Number of Previous Births
Mali DHS Surveys
Number of previous births
Birth cohort 0 1 2 3 4 5
Mean age at previous birth
1940-1949 19.8 22.5 24.8 26.9 29.0
1950-1959 19.8 22.2 24.6 26.8 29.0
1960-1969 19.5 22.1 24.3 26.5 28.4
1970-1979 18.9 21.4 23.6 25.6 27.5
1980-1989 18.0 20.3 22.4 24.2 25.7
1990-1999 16.8 18.5
Percent not completing the birth interval
1940-1949 3.8% 4.7% 4.9% 6.4% 6.7%
1950-1959 3.3% 2.9% 3.5% 4.5% 5.2%
1960-1969 3.3% 2.9% 3.7% 4.0% 5.7%
1970-1979 2.1% 2.3% 3.4% 3.2% 4.6%
1980-1989 1.1% 1.9% 2.7% 5.8% 3.1%
1990-1999 3.0% 4.3%
Median birth interval 1940-1949 25 25 26 26 26
1950-1959 26 26 26 26 26
1960-1969 26 26 26 28 28
1970-1979 28 28 28 29 31
1980-1989 29 31 31 31 34
1990-1999 33 34 Note: Estimates based on fewer than 100 births are omitted.

17
Table 7
Percent of Intervals Not Completed by Birth Cohort and Number of Previous
Births (6 to 10)
Cameroon, Ghana, and Mali DHS Surveys
Number of previous births Birth cohort 6 7 8 9 10
Cameroon 1940-1949 9.8% 14.4% 29.5% 26.3% 1950-1959 11.4% 19.5% 24.2% 29.1% 38.4%
1960-1969 15.2% 17.9% 22.4% 25.5% 38.2%
1970-1979 8.4% 9.1% 20.9% 21.5% 25.0%
1980-1989 9.6% 6.1%
Ghana 1940-1949 11.9% 15.0% 19.4% 29.6% 46.9%
1950-1959 15.1% 21.7% 25.0% 31.6% 34.9%
1960-1969 17.3% 25.0% 32.1% 33.8% 1970-1979 14.6% 24.7% 27.3% 1980-1989 6.8%
Mali 1940-1949 8.4% 12.7% 12.9% 22.5% 29.7%
1950-1959 6.7% 10.0% 14.9% 21.7% 32.1%
1960-1969 7.9% 9.1% 14.9% 20.4% 29.4%
1970-1979 6.3% 9.7% 11.5% 13.1% 31.0%
1980-1989 6.6%

18
Table 8
Percent of Intervals Not Completed by Birth Cohort and Age
German Village Reconstitutions, Taiwan KAP, Cameroon DHS, Ghana DHS, Mali DHS
Age of Mother
Birth
cohort 15-19 20-24 25-29 30-34 35-39 40-44 45-49
German villages
1725 4.9% 4.0% 4.0% 7.2% 30.6% 1750 2.7% 5.5% 2.7% 7.3% 26.2% 1775 8.8% 9.3% 5.8% 8.5% 21.3% 1800 16.1% 4.3% 3.3% 6.2% 23.5% 1825 7.7% 6.3% 6.0% 7.4% 30.3% 1850 10.6% 4.9% 5.5% 8.8% 31.7% 1875 22.1% 11.6% 14.3% 17.7% 60.1% 1900 14.3% 22.0%
Taiwan 1931 8.4% 1.5% 2.0% 15.0% 33.5% 53.8% 1936 4.5% 1.4% 3.7% 33.2% 66.9% 69.8% 1941 10.3% 1.9% 11.0% 45.5% 71.9% 98.9% 1946 3.5% 0.0% 14.0% 52.6% 73.9% 1951 13.9% 0.0% 23.7% 50.4% 1956 0.0% 0.0% 30.7% 1961 17.5% 22.6%
Cameroon 1940 0.0% 6.6% 4.2% 6.0% 12.8% 35.3% 1950 4.3% 2.4% 3.9% 6.6% 16.6% 39.3% 68.2%
1960 3.2% 3.7% 4.0% 8.0% 15.8% 41.9% 60.1%
1970 4.6% 3.8% 4.4% 6.8% 15.4% 1980 4.5% 2.5% 2.6% 3.1%
Ghana 1930 4.6% 2.4% 4.6% 5.1% 1940 3.0% 1.5% 2.5% 3.3% 8.7% 25.4% 59.6%
1950 0.0% 1.7% 2.4% 4.5% 11.7% 30.8% 53.6%
1960 7.0% 2.2% 4.1% 6.4% 14.7% 35.6% 66.2%
1970 9.5% 3.9% 3.1% 5.8% 13.8% 41.9% 1980 18.0% 4.3% 1.6% 1.2% 1990 11.9% 2.4%
Mali 1930 6.7% 4.2% 3.7% 3.3% 1940 4.9% 3.5% 3.3% 4.9% 8.9% 30.8% 68.4%
1950 3.7% 2.3% 2.3% 3.8% 8.6% 29.4% 60.4%
1960 5.4% 2.7% 2.3% 4.0% 10.8% 32.5% 57.2%
1970 6.4% 2.1% 2.0% 4.6% 12.8% 25.0%

19
1980 0.0% 1.5% 1.9% 3.2% 1990 5.6% 2.7%
Note: Estimates based on fewer than 100 births are omitted.

20
Appendix Table 1.
DHS Surveys
Country Phase Implementing Organization Fieldwork
Cameroon DHS-II
Ministère du Plan et de l’Aménagement du
Territoire
April 1991 - September
1991
DHS-III
Bureau Central des Recensements et Études
de Population
February 1998 - June
1998
DHS-IV Institut National de la Statistique
February 2004 -
August 2004
DHS-VI Institut National de la Statistique (INS)
January 2011 - August
2011
Ghana DHS-I Ghana Statistical Service
February 1988 - June
1988
DHS-III Ghana Statistical Service
September 1993 -
February 1994
DHS-IV Ghana Statistical Service
November 1998 -
February 1999
DHS-IV
Ghana Statistical Service/Health Research
Unit (GSS/HRU)
April 2002 - September
2002
DHS-IV Ghana Statistical Service
July 2003 - October
2003
DHS-VII Ghana Statistical Service (GSS)
September 2014 -
December 2014
DHS-VII Ghana Statistical Service (GSS)
September 2014 -
December 2014
Mali
DHS-I
Centre d'Etudes et de Recherches sur la
Population pour le
Développement(CERPOD) de l'Institut du
Sahel
March 1987 - August
1987
DHS-III
CPS/MSSPA et DNSI, Cellule de
Planification et Statistique du Ministère de
la Santé; Direction de la Statistique et de
l'Informatique du Ministère de l'Économie
et des Finances
November 1995 - May
1996
DHS-IV
CPS/MSSPA et DNSI, Cellule de
Planification et Statistique dur Ministère de
la Santè; Direction de la Statistique e de
l'Informatique du Ministère de l'Économie
et des Finances
January 2001 - May
2001
DHS-V
Cellule de Planification et de Statistique
(CPS), Direction Nationale de la Statistique
et de L'Informatique (DNSI)
May 2006 - December
2006

21
DHS-VI
INFO-STAT in collaboration with
government agencies, the National Institute
of Statistics (INSTAT) and the Cellule de
Planification et de Statistique (CPS), which
is the technical department in charge of
statistics and the DHS at the Ministry of
Health.
November 2012 -
February 2013

22
Appendix Table 2.
Number of Births by Birth Cohort and Birth Order
Number of Previous Births
0 1 2 3 4 5
German Villages 1725-1749 718 650 566 460 379 301
1750-1774 435 404 372 330 286 232
1775-1799 491 497 428 369 320 259
1800-1824 596 681 606 521 437 353
1825-1849 667 691 601 515 423 340
1850-1874 699 680 592 510 441 349
1875-1899 701 650 503 384 281 200
1900-1924 292 242 149 92 50 32
Taiwan 1931-1935 5023 4906 4688 4144 3079 1995
1936-1940 3960 3745 3131 2021 911 327
1941-1945 3855 3274 2439 1278 420 130
1946-1950 3054 2597 1709 655 193 48
1951-1955 2310 1823 1045 315 81 12
1956-1960 1212 804 355 84 13 3
1961-1965 375 192 56 7 0 0
1966-1970 5 0 0 0 0 0
Cameroon 1940-1949 343 320 295 276 252
1950-1959 1703 1613 1494 1335 1145
1960-1969 4211 3823 3335 2761 2113
1970-1979 4597 3764 2929 2101 1404
1980-1989 3004 2056 1228 629 295
1990-1999 318 97 17 5 1
Ghana 1930-1939 81 76 75 71 66
1940-1949 915 880 828 760 673
1950-1959 2910 2705 2333 1866 1330
1960-1969 4796 3904 2953 2066 1356
1970-1979 4005 2983 2074 1328 764
1980-1989 1828 1115 590 256 101
1990-1999 179 50 9 5 0
Mali 1930-1939 85 79 76 68 60
1940-1949 952 907 852 780 713
1950-1959 4659 4474 4207 3823 3378

23
1960-1969 9678 8883 7942 6740 5457
1970-1979 10667 8763 6679 4703 3011
1980-1989 6256 4111 2408 1211 482
1990-1999 739 254 64 12 0

24
References
Agadjanian, V. 2005. "Fraught with ambivalence: Reproductive intentions and contraceptive
choices in a sub-Saharan fertility transition." Population Research and Policy Review
24(6):617-645.
Alter, G. 2013. "Stopping and Spacing in Historical Europe and Contemporary Africa." in
International Seminar on Past and Present: Revisiting the Demographic Transitions
in the South through Individual Longitudinal Data. International Institute for
Population Sciences, Mumbai, India.
Anderton, D.L.and L.L. Bean. 1985. "Birth Spacing and Fertility Limitation - a Behavioral-
Analysis of a 19Th-Century Frontier Population." Demography 22(2):169-183.
Aries, P. 1960. "Interpretation pour une histoire des mentalites." Pp. 311–327 in La
prévention des naissances dans la famille: ses origines dans les temps modernes,
edited by H. Bergues. Paris: Presses universitaires de France.
Bengtsson, T.and M. Dribe. 2006. "Deliberate control in a natural fertility population:
Southern Sweden, 1766-1864." Demography 43(4):727-746.
Bledsoe, C., F. Banja, and A.G. Hill. 1998. "Reproductive Mishaps and Western
Contraception: An African Challenge to Fertility Theory." Population and
Development Review 24(1):15-57.
Bledsoe, C.H. 2001. The bodily costs of childbearing: Western science through a West
African lens.
Bledsoe, C.H.and F. Banja. 2002. Contingent lives: fertility, time, and aging in West Africa.
Chicago: University of Chicago Press.
Bledsoe, C.H., A.G. Hill, U. D'Alessandro, and P. Langerock. 1994. "Constructing Natural
Fertility: The Use of Western Contraceptive Technologies in Rural Gambia."
Population and Development Review 20(1):81-113.
Caldwell, J.C., I.O. Orubuloye, and P. Caldwell. 1992. "Fertility Decline in Africa: A New
Type of Transition?" Population and Development Review 18(2):211-242.
Casterline, J.B.and C. Odden. 2016. "Trends in Inter-Birth Intervals in Developing Countries
1965–2014." Population and Development Review 42(2):173-194.
Cellule de Planification et de Statistique (CPS/SSDSPF), Institut National de la Statistique
(INSTAT/MPATP), INFO-STAT, and ICF International. 2014. "Enquête
Démographique et de Santé au Mali 2012-2013." Rockville, Maryland, USA
Chow, L.P., H.-C. Chen, and M.-C. Chang. 2005a. "Knowledge, Attitudes, and Practice of
Contraception in Taiwan: First Province-Wide Fertility Survey (KAP I), 1965." Inter-
university Consortium for Political and Social Research (ICPSR) [distributor].
—. 2005b. "Knowledge, Attitudes, and Practice of Contraception in Taiwan: Second
Province-Wide Fertility Survey (KAP II), 1967." Inter-university Consortium for
Political and Social Research (ICPSR) [distributor].

25
Cleves, M., W.W. Gould, R.G. Gutiérrez, and Y. Marchenko. 2010. "Introduction to survival
data analysis with Stata." College Station, TX: Stata Press.
Coale, A.J. 1973. "The Demographic Transition Reconsidered." Pp. 53-72 in International
Population Conference, Liege 1973. Liege, Belgium: International Union for the
Scientific Study of Population.
Freedman, R., M.-C. Chang, and T.-H. Sun. 1994. "Taiwan's transition from high fertility to
below-replacement levels." Studies in Family Planning 25(6):317-331.
Galloway, P.R. 1988. "Basic Patterns in Annual Variations in Fertility, Nuptiality, Mortality,
and Prices in Pre-industrial Europe." Population Studies: A Journal of Demography
42(2):275-302.
Gervais, D.and D. Gauvreau. 2003. "Women, priests, and physicians: Family limitation in
Quebec, 1940-1970." Journal of Interdisciplinary History 34(2):293-+.
Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF International. 2015.
"Ghana Demographic and Health Survey 2014." Rockville, Maryland, USA.
Henry, L. 1961. "Some data on natural fertility." Eugenics Quarterly 8:81-91.
Henry, L. 1980. Techniques d'analyse en démographie historique. Paris: Éditions de l'Institut
national d'études démographiques.
Johnson-Hanks, J. 2002. "On the Modernity of Traditional Contraception: Time and the
Social Context of Fertility." Population and Development Review 28(2):229-249.
Johnson-Hanks, J. 2007. "Natural intentions: Fertility decline in the African demographic and
health surveys." American Journal of Sociology 112(4):1008-1043.
Kaplan, E.L.and P. Meier. 1958. "Nonparametric estimation from incomplete observations."
Journal of the American Statistical Association 53(282):457-481.
Knodel, J. 1987. "Starting, Stopping, and Spacing during the Early Stages of Fertility
Transition - the Experience of German Village Populations in the 18Th and 19Th
Centuries." Demography 24(2):143-162.
Knodel, J.and E. van de Walle. 1979. "Lessons from the Past: Policy Implications of
Historical Fertility Studies." Population and Development Review 5(2):217-245.
Knodel, J.E. 1988. Demographic behavior in the past a study of fourteen German village
populations in the eighteenth and nineteenth centuries. Cambridge Cambridgeshire,
New York: Cambridge University Press.
Lightbourne, R.E. 1985. "Individual preferences and fertility behaviour." Pp. 165-198 in
Reproductive change in developing countries: insights from the World Fertility
Survey, edited by J.G. Cleland, J. Hobcraft, B. Dinesen, and M.G. Kendall. London ;
New York: Oxford University Press.
Morgan, S.P. 1991. "Late 19th-Century and Early 20th-Century Childlessness." American
Journal of Sociology 97(3):779-807.
Moultrie, T.A., T.S. Sayi, and I.M. Timaeus. 2012. "Birth intervals, postponement, and
fertility decline in Africa: A new type of transition?" Population Studies-a Journal of
Demography 66(3):241-258.
Okun, B.S. 1994. "Evaluating Methods for Detecting Fertility-Control - Coale and Trussells
Model and Cohort Parity Analysis." Population Studies-a Journal of Demography
48(2):193-222.

26
—. 1995. "Distinguishing Stopping Behavior from Spacing Behavior with Indirect Methods."
Historical Methods 28(2):85-96.
Perrenoud, A. 1988. "Espacement et arrêt dans le contrôle des naissances." Annales de
Démographie historique:59-78.
Rodriguez, G. 2006. "Demographic translation and tempo effects: An accelerated failure time
perspective." Demographic Research 14(6):85-110.
StataCorp. 2015. " Stata Statistical Software: Release 14." College Station, TX: StataCorp LP.
Sun, T.-H.and M.-C. Chang. 2002. "Knowledge, Attitudes, and Practice of Contraception in
Taiwan: Fifth Province-Wide Fertility Survey (KAP V), 1979." Inter-university
Consortium for Political and Social Research (ICPSR) [distributor].
—. 2005. "Knowledge, Attitudes, and Practice of Contraception in Taiwan: Fourth Province-
Wide Fertility Survey (KAP IV), 1973." Inter-university Consortium for Political and
Social Research (ICPSR) [distributor].
Sun, T.-H., M.-C. Chang, M.-L. Lee, and H.-S. Lin. 2005. "Knowledge, Attitudes, and
Practice of Contraception in Taiwan: Sixth Province-Wide Fertility Survey (KAP VI),
1986." Inter-university Consortium for Political and Social Research (ICPSR)
[distributor].
Thomas, D.S. 1941. Social and economic aspects of Swedish population movements, 1750-
1933. New York: The Macmillan Company.
Thomas, D.S.T. 1927. Social aspects of the business cycle. New York: Knopf.
Timaeus, I.M.and T.A. Moultrie. 2008. "On postponement and birth intervals." Population
and Development Review 34(3):483-+.
—. 2013. "DISTINGUISHING THE IMPACT OF POSTPONEMENT, SPACING AND
STOPPING ON BIRTH INTERVALS: EVIDENCE FROM A MODEL WITH
HETEROGENEOUS FECUNDITY." Journal Of Biosocial Science 45(3):311-330.
Tsuya, N.O. 2010. Prudence and pressure : reproduction and human agency in Europe and
Asia, 1700-1900. Cambridge, Mass.: MIT Press.
United Nations, D.o.E.a.S.A., Population Division. 2015. "World Population Prospects: The
2015 Revision." edited by U. Nations.
Van Bavel, J. 2004. "Deliberate birth spacing before the fertility transition in Europe:
Evidence from nineteenth-century Belgium." Population Studies-a Journal of
Demography 58(1):95-107.
Van Bavel, J.and J. Kok. 2004. "Birth spacing in the Netherlands. The effects of family
composition, occupation and religion on birth intervals, 1820-1885." European
Journal of Population-Revue Europeenne De Demographie 20(2):119-140.
Yamaguchi, K.and L.R. Ferguson. 1995. "The Stopping and Spacing of Childbirths and Their
Birth-History Predictors - Rational-Choice Theory and Event-History Analysis."
American Sociological Review 60(2):272-298.