Embed Size (px)
Citation preview

Robert Macpherson, PhD
Work Wellness Institute Public WebinarSeptember 9, 2020
Understanding gender-based differences in work-related health outcomes

About the Partnership for Work, Health and Safety
• Partnership between WorkSafeBC (BC Workers’ Compensation Board) and the University of British Columbia
• Data partner: Population Data BC• Diverse and multidisciplinary group of faculty, staff, and students• Many collaborators:
• Institute for Work & Health• Insurance Work and Health Research Group• Occupational Cancer Research Centre• CAREX Canada
• Multiple funders across 20 active projects

Overview
• What do we mean by gender and sex?• Why should we study gender and sex-based differences in work-related
health outcomes?• What does the research show?• What are the implications for policy and practice?

Source: Canadian Institutes of Health Research, 2020
Sex• Biological construct• Encompasses hormones, genes, anatomy,
physiology• Affects prevalence, course and treatment of
health conditions and diseases
Gender• Social construct (roles, identity, relations)• Linked to power and economic and social status• Culturally specific and temporal

Why does gender/sex matter in work-related health?
• Desire to live in an equal and equitable society
• Workforce productivity
• Social and economic costs of health
• Research has traditionally neglected gender and sex

Factors linking gender/sex and work-related health
Injury characteristics Job characteristics Income
Domestic responsibilities Experience of health care and compensation systems

Snapshot of British Columbia
Source: WorkSafeBC Statistics 2018

Percentage of female claimants in British Columbia, 2009-2018
Source: WorkSafeBC Statistics 2018:50

Serious injury claims by gender
Source: WorkSafeBC Statistics 2018:31

Gender/sex differences in workplace injuries

• In general, women experience and report more work-related musculoskeletal pain and disorders
• Mechanisms that explain gender/sex differences in risk of these disorders are multifactorial
• Gendered division of labour, women and men dominating different occupations with different exposures and risks
• However, even in similar occupations and similar tasks, gender/sex differences persist

• Activity-related soft tissue disorders (ASTDs) are disorders of the extremities (arms and legs) involving muscles, tendons and/or ligaments
• Caused or aggravated by over-use and repetitive activities or exposure to mechanical vibrations
Objective: • To examine gender/sex differences in rates of accepted
short-term disability claims for ASTDs, by time period, occupation and type of disorder

Methods
• Data: WorkSafeBC claims and Labour Force Survey
• Rates: # of ASTDs per 1,000 workers, for women and men (accepted STD claims)/(counts of BC workers (Labour Force Survey)
• Time periods: 2003-07, 2008-12, 2013-17• Age bracket: 15-64 years, 10-year groupings• Occupation: 1/2-digit National Occupational Classification (2006)• ICD diagnoses: tendonitis, bursitis, carpal tunnel
• ASTD claims: • Accepted short-term disability claims• Combination of diagnosis and claim assignment type of ASTD

Rates of activity-related soft tissue disorders per 1,000 workers Women and men, by time period and age group

Age-adjusted rates of activity-related soft tissue disorders per 1,000 workers Women and men, by time period and disorder

Age-adjusted rates of activity-related soft tissue disorders per 1,000 workers Women and men, by time period and occupation groups

Gender/sex differences in return-to-workand work disability duration

Evidence and jurisdictional variation
• Gender-specific studies• No differences in RTW, differences in LRTW (De Rijk et al. 2008)• Differences beyond 12 months, transition slowed for men (Lederer and Rivard, 2014)
• Multi-jurisdictional studies• Women less likely to transition off disability benefits (Collie et al. 2016)• Women associated with 1.9 days more of work disability duration (Shraim et al. 2015)
• Results are likely to vary due to differences in factors such as health care systems, workers’ compensation systems, legal systems, in addition to different values such as gender norms.

Research questions:
• Are gender differences in work disability duration consistent by jurisdiction?
• Are gender differences consistent by duration of work disability?

Method
• Data• Claim-level from British Columbia, Manitoba and Ontario• Restrictions:
• Accepted claims with ≥ 1 work disability day paid• Aged ≥ 15 at time of injury• Injured 2007-2011 • Excluded disease and fatal claims
• Analysis:• Time-to-event analysis
• Time: Cumulative disability days paid• Event: Transitioning off disability benefits within one year of injury

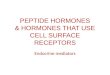
BC | all occupations | all injuries | 2007-2011Kaplan-Meier survival estimates of claims transitioning off work disability benefits

BC | all occupations | all injuries | 2007-2011Hazard model of gender-by-time interaction on claims transitioning off work disability benefits
Wom
en m
ore
likel
y to
tr
ansit
ion
off b
enef
itsLe
ss li
kely

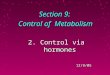
All occupations | all injuries | 2007-2011Hazard models of gender-by-time interaction on claims transitioning off work disability benefits
Wom
en m
ore
likel
y to
tr
ansit
ion
off b
enef
itsLe
ss li
kely

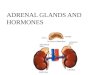
All occupations | back strain injuries | 2007-2011Hazard models of gender-by-time interaction on claims transitioning off work disability benefits
Wom
en m
ore
likel
y to
tr
ansit
ion
off b
enef
itsLe
ss li
kely

Discussion
• What is causing the time-varying differences between men and women?
• What is driving differences by jurisdiction?
• Policy implications• Tailoring prevention and rehabilitation interventions to meet the needs of men
and women

Gender/sex differences and health care services

Objective:• To determine whether patients’ sex affects physicians’
decision to refer a patient for, or to, perform, total knee arthroplasty
Findings:• 42% of physicians recommended the procedure to the male
but not female• 8% of physicians recommended the procedure to the female
but not the male• Odds of orthopedic surgeon recommendation 22 times
higher for male• Odds of family physician recommendation 2 times higher for
male

Objective:• To examine gender differences in surgery among workers in
British Columbia with accepted workers’ compensation claims for musculoskeletal injury

Methods
• Data: WorkSafeBC and Ministry of Health• Study population:
• Accepted lost-time claims for the following injury diagnoses:• Knee meniscus tear• Rotator cuff tear• Thoracic/lumbar intervertebral disc displacement
• Injured between May 1st, 2009 and December 31st, 2010
• Analysis: • Time-to-event analysis
• Time: Calendar days between injury and surgery• Event: Surgery

Adjusted hazard ratios with 95% confidence intervals for surgery for workers with accepted workers’ compensation claims by injury type
Knee meniscus tear Rotator cuff tear Intervertebral disc
Men (reference) 1 1 1
Women 0.87 [0.69-1.09] 0.35 [0.25-0.48] 0.54 [0.31-0.95]

Take home messages
• Growing evidence of gender/sex-based differences in work-related health outcomes
• Efforts should be made to reduce bias in how conditions are assessed
• Compensable injuries and rehabilitation may require different strategies and different accommodations to meet the needs of men and women
• Greater awareness of work-life balance


Questions for the audience?
• Are there gender/sex-specific policies or practices regarding workplace injury prevention and/or disability management within your organisation?
• Which study example resonated the most with you in your job role?
• Has this made you think more about how your gender/sex and position in your workplace may contribute to bias in decisions?
• What measures can your workplace introduce to help reduce gender differences in work-related health outcomes?

Questions?