Embed Size (px)
Citation preview
A publication of the International Myeloma Foundation
Multiple Myeloma | Cancer of the Bone Marrow
© 2
016,
Inte
rnat
iona
l Mye
lom
a Fo
unda
tion,
Nor
th H
olly
woo
d, C
alifo
rnia
–
u-f
l-hl_
2016
_EN
_k3
Improving Lives Finding the Cure®Improving Lives Finding the Cure®
12650 Riverside Drive, Suite 206North Hollywood, CA 91607 USA
Telephone:
800-452-CURE (2873) (USA & Canada)
818-487-7455 (worldwide)
Fax: 818-487-7454
UnderstandingFreelite® and Hevylite® Tests
Table of contents
The Understanding series and 10 Steps to Better Care 4
What you will learn from this booklet 4
Multiple myeloma and monoclonal protein 4
What are free light chains? 5
The role of the Freelite assay 5
Normal vs. abnormal light chain levels 7
The kappa/lambda ratio 7
How can the Freelite assay help detect and monitor myeloma? 8
Freelite levels and the assessment of response to treatment, including stringent complete response 10
Patients who benefit the most from the Freelite assay 11
What is the Hevylite assay? 15
What is a heavy/light chain ratio? 16
How does the Hevylite assay differ from SPEP? 16
The Hevylite assay and monitoring for relapse 16
The Hevylite assay and monitoring for residual disease 17
What are normal Hevylite levels? 17
Can Freelite and Hevylite be used together? 17
Will insurance cover the cost of Freelite and Hevylite assays? 17
In closing 17
Terms and definitions 18
About the International Myeloma Foundation
Founded in 1990, the International Myeloma Foundation (IMF) is the oldest and largest myeloma-specific charity in the world. With more than 350,000 members in 140 countries, the IMF serves myeloma patients, family members, and the medical community. The IMF provides a wide range of programs in the areas of Research, Education, Support, and Advocacy:
RESEARCH The IMF is the leader in globally collaborative myeloma research. The IMF supports lab-based research and has awarded over 100 grants to top junior and senior researchers since 1995. In addition, the IMF brings together the world’s leading experts in the most successful and unique way through the International Myeloma Working Group (IMWG), which is publishing in prestigious medical journals, charting the course to a cure, mentoring the next generation of innovative investigators, and improving lives through better care.
EDUCATION The IMF’s educational Patient & Family Seminars, Medical Center Workshops, and Regional Community Workshops are held around the world. These meetings provide up-to-date information presented by leading myeloma specialists and researchers directly to myeloma patients and their families. Our library of more than 100 publications, for patients and caregivers as well as for healthcare professionals, is updated annually and available free of charge. Publications are available in more than 20 languages.
SUPPORT Our toll-free InfoLine at 800-452-CURE (2873) is staffed by coordinators who answer questions and provide support and information via phone and email to thousands of families each year. The IMF sustains a network of more than 150 support groups and offers training for the hundreds of dedicated patients, caregivers, and nurses who volunteer to lead these groups in their communities.
ADVOCACY The IMF Advocacy program trains and supports concerned individuals to advocate on health issues that affect the myeloma community. Working both at the state and federal level, the IMF leads two coalitions to advocate for parity in insurance coverage. Thousands of IMF-trained advocates make a positive impact each year on issues critical to the myeloma community.
Learn more about the way the IMF is helping to improve the quality of life of myeloma patients while working toward prevention and a cure.
Contact us at 800-452-CURE (2873) or 818-487-7455, or visit myeloma.org.
Improving Lives Finding the Cure®
54 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
M-protein. Other names for M-protein are myeloma protein, paraprotein, or the M-spike. The identification of an M-protein is important for diagnosis, and the mea-surement of its level is an aid both for monitoring the effectiveness of treatment and for identifying a relapse.
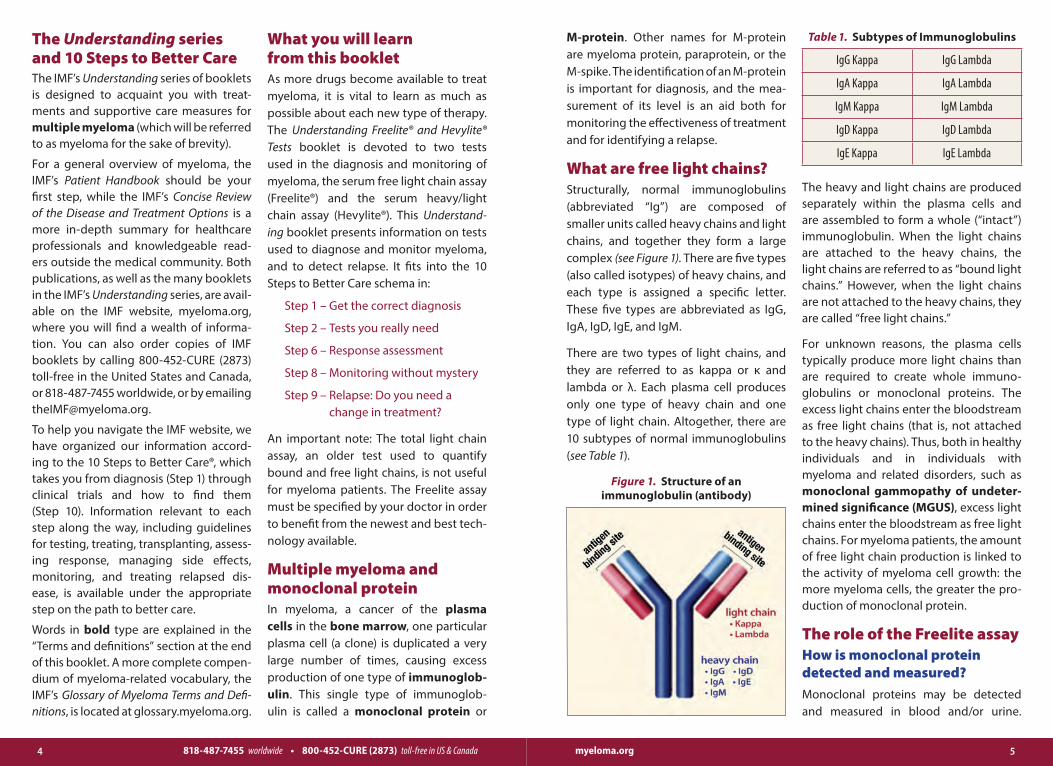
What are free light chains?Structurally, normal immunoglobulins (abbreviated “Ig”) are composed of smaller units called heavy chains and light chains, and together they form a large complex (see Figure 1). There are five types (also called isotypes) of heavy chains, and each type is assigned a specific letter. These five types are abbreviated as IgG, IgA, IgD, IgE, and IgM.
There are two types of light chains, and they are referred to as kappa or κ and lambda or λ. Each plasma cell produces only one type of heavy chain and one type of light chain. Altogether, there are 10 subtypes of normal immunoglobulins (see Table 1).
The heavy and light chains are produced separately within the plasma cells and are assembled to form a whole (“intact”) immunoglobulin. When the light chains are attached to the heavy chains, the light chains are referred to as “bound light chains.” However, when the light chains are not attached to the heavy chains, they are called “free light chains.”
For unknown reasons, the plasma cells typically produce more light chains than are required to create whole immuno-globulins or monoclonal proteins. The excess light chains enter the bloodstream as free light chains (that is, not attached to the heavy chains). Thus, both in healthy individuals and in individuals with myeloma and related disorders, such as monoclonal gammopathy of undeter-mined significance (MGUS), excess light chains enter the bloodstream as free light chains. For myeloma patients, the amount of free light chain production is linked to the activity of myeloma cell growth: the more myeloma cells, the greater the pro-duction of monoclonal protein.
The role of the Freelite assayHow is monoclonal protein detected and measured?Monoclonal proteins may be detected and measured in blood and/or urine.
What you will learn from this bookletAs more drugs become available to treat myeloma, it is vital to learn as much as possible about each new type of therapy. The Understanding Freelite® and Hevylite® Tests booklet is devoted to two tests used in the diagnosis and monitoring of myeloma, the serum free light chain assay (Freelite®) and the serum heavy/light chain assay (Hevylite®). This Understand-ing booklet presents information on tests used to diagnose and monitor myeloma, and to detect relapse. It fits into the 10 Steps to Better Care schema in:
Step 1 – Get the correct diagnosis
Step 2 – Tests you really need
Step 6 – Response assessment
Step 8 – Monitoring without mystery
Step 9 – Relapse: Do you need a change in treatment?
An important note: The total light chain assay, an older test used to quantify bound and free light chains, is not useful for myeloma patients. The Freelite assay must be specified by your doctor in order to benefit from the newest and best tech-nology available.
Multiple myeloma and monoclonal proteinIn myeloma, a cancer of the plasma cells in the bone marrow, one particular plasma cell (a clone) is duplicated a very large number of times, causing excess production of one type of immunoglob-ulin. This single type of immunoglob-ulin is called a monoclonal protein or
The Understanding series and 10 Steps to Better CareThe IMF’s Understanding series of booklets is designed to acquaint you with treat-ments and supportive care measures for multiple myeloma (which will be referred to as myeloma for the sake of brevity).
For a general overview of myeloma, the IMF’s Patient Handbook should be your first step, while the IMF’s Concise Review of the Disease and Treatment Options is a more in-depth summary for healthcare professionals and knowledgeable read-ers outside the medical community. Both publications, as well as the many booklets in the IMF’s Understanding series, are avail-able on the IMF website, myeloma.org, where you will find a wealth of informa-tion. You can also order copies of IMF booklets by calling 800-452-CURE (2873) toll-free in the United States and Canada, or 818-487-7455 worldwide, or by emailing [email protected].
To help you navigate the IMF website, we have organized our information accord-ing to the 10 Steps to Better Care®, which takes you from diagnosis (Step 1) through clini cal trials and how to find them (Step 10). Information relevant to each step along the way, including guidelines for test ing, treating, transplanting, assess-ing response, managing side effects, moni toring, and treating relapsed dis-ease, is available under the appropriate step on the path to better care.
Words in bold type are explained in the “Terms and definitions” section at the end of this booklet. A more complete compen-dium of myeloma-related vocabulary, the IMF’s Glossary of Myeloma Terms and Defi-nitions, is located at glossary.myeloma.org.
Figure 1. Structure of an immunoglobulin (antibody)
Table 1. Subtypes of Immunoglobulins
IgG Kappa IgG Lambda
IgA Kappa IgA Lambda
IgM Kappa IgM Lambda
IgD Kappa IgD Lambda
IgE Kappa IgE Lambda

76 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
When measurements are taken in blood, all of the cells are removed from the blood sample, leaving only the yellow liquid component of the blood that is called “serum.” Several tests can be ordered to detect the M-protein, including serum protein electrophoresis (SPEP), urine protein electrophoresis (UPEP), and the serum free light chain assay (SFLCA, or Freelite). If only one type of light chain (kappa OR lambda and not both kappa AND lambda) is produced in excess, this means that myeloma cells are secreting monoclonal protein. SPEP measures the amount of monoclonal protein in the blood and UPEP measures the amount of monoclonal light chain in the urine, but neither test can identify the type of monoclonal protein. That is done by immunofixation electrophoresis (IFE), which, in turn, only determines if a partic-ular type of monoclonal protein is pres-ent, but does not quantify the amount.
Patients with elevated levels of free light chains have traditionally been diag-nosed and monitored using UPEP; this test has been required in all clinical trials for myeloma. However, a paper from the French myeloma study group recently
published in the journal Haematologica compared serum Freelite and 24-hour urine UPEP results after 2 and 4 cycles of therapy and after stem cell transplanta-tion in patients enrolled in the IFM2007-02 study. The authors “found good agree-ment between methods for response assessment [after 2 cycles of therapy] but the serum free light chain test provided greater sensitivity than urine electro-phoresis for monitoring.” Because light chains are first released into the blood and then filtered by the kidneys before they reach the urine, UPEP is not a highly sensitive test. However, the Freelite assay is a blood test and it quantifies the level of light chains in the blood before the light chains are filtered by the kidneys. More-over, patient compliance with 24-hour urine collection is poor, not surprisingly, making response assessment difficult and compromising the results of clinical trials. As a result of the Haematologica publica-tion, the IMWG is expected to change its guidelines for serum free light chain anal-ysis and to accept the Freelite test in lieu of 24-hour urine collection and urine pro-tein electrophoresis. We anticipate that these new guidelines will be published in early 2016.
The Freelite assayThe Freelite assay is capable of detecting free light chains at their normal (non-el-evated) levels in the blood. Freelite can detect light chains at levels lower than nor-mal concentration (i.e., to detect suppres-sion). Importantly, this assay can detect mildly increased levels of free light chains even when these levels are undetectable by SPEP and IFE. This means that multiple myeloma could be detected earlier than
might be possible with either SPEP or IFE. Moreover, the Freelite assay is particu-larly useful in instances when only small amounts of light chains are produced by the myeloma.
Freelite is best performed on serum rather than urine because of the filtering effects of the kidneys. Part of the normal function of the kidneys is to prevent pro-tein loss from the body into the urine. As a result, an elevated level of M-protein may be detected in the blood before it is detected in the urine. Urine studies are still important, however, in the initial diagnosis and subsequent monitoring of AL amyloidosis. Urine studies show other aspects of myeloma disease, like kidney damage, and should be included in the work-up of myeloma.
Like other tests that detect M-protein, the Freelite assay has advantages and disad-vantages. As discussed above, one advan-tage is greater sensitivity than is available with SPEP, UPEP, and IFE. Another advan-tage is that the Freelite assay is auto-mated and therefore requires less time to perform in the laboratory than SPEP, UPEP, and IFE. However, although the Freelite assay is excellent for detection of free light chains, it is unable to detect whole immunoglobulins. Some types of myeloma secrete only whole immu-noglobulins. Recently, a new laboratory test called Hevylite became available to measure intact immunoglobulin heavy/light chain pairs. Like Freelite, Hevylite can be measured in normal serum and is more sensitive than SPEP. More informa-tion about Hevylite can be found later in this booklet.
Normal vs. abnormal light chain levelsNormal levels of serum free light chains are*: n Kappa: 3.3–19.4 mg/L or
0.33–1.94 mg/dL
n Lambda: 5.71–26.3 mg/L or 0.57–2.63 mg/dL
n Kappa/lambda ratio: 0.26–1.65*
* Note: In patients with renal impairment, it is recommended to interpret the results of the kappa/lambda ratio with a modified reference range of 0.37–3.1.
In the majority of cases, light chains pro-duced by myeloma cells will be exclusively kappa or lambda, depending upon the type of myeloma. Thus, if the myeloma cells produce kappa light chains, the level of kappa free light chains will increase in the blood. If, on the other hand, the myeloma cells produce lambda light chains, the level of lambda free light chains will increase in the blood. Your doctor will need to interpret the results of the Freelite assay together with other clinical information in order to make a final interpretation of the results.
The kappa/lambda ration The Freelite kappa/lambda ratio is as
important for diagnosis and monitor-ing of myeloma as are the levels of kappa and lambda light chains.
n When the level of either kappa or lambda is very high and the other light chain is normal or low, then the ratio is abnormal and indicates that the myeloma is present.
n If levels of both kappa and lambda light chains are increased, the ratio may be
98 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
within the normal range, but this gen-erally indicates a disease other than myeloma, such as poor kidney func-tion. When the kidneys are not working properly, both types of light chains are retained in the blood and are not removed by the kidneys.
n Sometimes the kappa/lambda ratio may be abnormal even though the individual kappa and lambda levels are both within the normal range. This can be indicative of a persistent low level of active myeloma.
n A normal kappa/lambda ratio after treatment signifies a particularly effec-tive response. It is part of the definition of a “stringent complete response” (sCR), which also requires negative urine/serum IFE and absence of clonal cells in the bone marrow. Normaliza-tion of the kappa/lambda ratio cor-relates with possible longer remissions.
How can the Freelite assay help detect and monitor myeloma?Changes in free light chain levels are use-ful for tracking the disease status in almost all people with myeloma, not just those with light chain (Bence-Jones) myeloma or nonsecretory disease. The Freelite test can help in the detection and monitoring of myeloma by quantifying monoclonal protein in multiple disease settings.
Intact immunoglobulin multiple myeloma (IIMM)IIMM accounts for more than 80% of myeloma cases. In IIMM, the cancerous plasma cells produce one type of intact immunoglobulin, and in the majority of these cases, either kappa or lambda free light chains are also produced. Because free light chains are filtered by the kidneys rather quickly (within just a few hours), changes in blood levels in response to treatment occur rapidly. Decreases in free light chain levels can therefore be a very sensitive indicator of early response in IIMM.
Light chain multiple myeloma (LCMM)LCMM comprises 15%–20% of all myelo-mas. In LCMM the myeloma plasma cells produce only light chains. Freelite has 100% proven sensitivity in detection of light chains in these patients. It is a bet-ter indicator of minimal residual disease and disease changes than urine measure-ment, which can be influenced by renal function. The Freelite assay is also more sensitive for monitoring LCMM patients who may not secrete enough protein to be detected by other serum tests or urine tests.
Nonsecretory and oligosecretory myelomaSome myeloma plasma cells produce very little or no M-protein. In the case where there is no M-protein, the result is referred to as nonsecretory myeloma. When the myeloma plasma cells secrete a very low level of M-protein, the disease is called oligosecretory myeloma. These types of myeloma comprise a very small percent-age of all the myelomas. Approximately 70% to 80% of people with M-protein that is too low to detect by other meth-ods have measurable M-protein using the Freelite assay.
Freelite at relapseAt the time of relapse, the sensitivity of the free light chain assays is also very important. Even very small amounts of myeloma that start to grow as part of relapse produce measurable amounts of free light chains in most instances. The serum free light chain levels of either kappa or lambda, depending upon the type of myeloma, may increase before the increases in IgG and IgA and other immunoglobulins can be detected by SPEP or IFE. Other tests such as bone marrow biopsy, and imaging tests such as FDG-PET or PET-CT, are also useful in the assessment of minimal amounts of disease.
Light chain escape (LCE)At the time of relapse, the pattern of myeloma immunoglobulin production can change. For example, plasma cells that produced both intact immunoglob-ulins and free light chains may change so that only free light chains are produced,
or a clone of plasma cells that produced intact immunoglobulin may have been eradicated by therapy, while a small sub-clone that produced only free light chains may have survived and expanded. These situations result in what is called light chain escape (LCE). The most sensitive way LCE can be detected earlier in relapse is by measurement of the blood with the Freelite assay.
Monoclonal gammopathy of undetermined significance (MGUS)Patients who have been diagnosed with MGUS have some blood characteristics of myeloma but do not have active disease, and they do not need to be treated. For example, they may have elevated levels of immunoglobulins and/or free light chains and/or plasma cells. Patients with MGUS can be risk-stratified to assess their chance of developing active disease. A study from the Mayo Clinic showed that patients with MGUS who also have an abnormal free light chain ratio are more likely to progress and develop active myeloma or a related malignant condition.
Smoldering multiple myeloma (SMM) or asymptomatic multiple myelomaPatients with SMM have higher levels of immunoglobulins and/or free light chains and/or plasma cells in the blood than patients with MGUS. They still do not have active disease and have not sustained damage to their bones, kidneys, or red blood cells. However, the chance that they will develop active disease is much greater than patients with MGUS. SMM patients should be monitored at regular inter-vals and should discuss how often they need to be tested for active disease with
1110 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
their doctors. A small percentage of SMM patients have a high risk of progressing to active myeloma. These patients, who have a free light chain ratio ≥ 100 or ≤ 0.01, ≥ 60% bone marrow plasma cells, or more than one focal lesion detected by MRI, are now defined as having active myeloma by the International Myeloma Working Group (IMWG) because they have a greater than 80% risk of progressing to active myeloma within two years (Rajkumar et al., The Lan-cet, vol. 15 no. 12, November 2014). Clinical trials have been initiated to determine if there is any benefit in treating patients with “high-risk” SMM before they have symptoms of active disease.
AL amyloidosis
Amyloid light chain (AL) amyloidosis is a disease that occurs when the light chains are misformed in a characteristic “beta pleating” pattern that results in deposi-tion of rigid fibrils in such places as the kidneys, heart, liver, tongue, and periph-eral nerves. Measurement of serum free light chains has been recommended for the diagnosis and monitoring of AL amyloidosis since 2004.
Enrollment in clinical trialsClinical trials are the only route by which new medicines are made available and a potential cure discovered. People with myeloma may participate in clinical trials to help test the safety and effectiveness of new treatments. In order for a patient with myeloma to be eligible to participate in a trial, there must be a way to monitor their M-protein levels in the blood or urine. People with hyposecretory disease used to be excluded from clinical trials because there was no method to monitor their M-protein levels. With the availability of the Freelite assay, the M-protein level can be monitored in the blood of the majority of these people. Therefore, people with low-secreting disease are often eligible to participate in clinical trials.
Freelite levels and the assessment of response to treatment, including stringent complete responseOne of the goals of myeloma treatment is to reduce the level of M-protein as much as possible, and sometimes to eliminate it entirely. Serum free light chain levels, as measured by the Freelite assay, can be used in the same way as monoclonal pro-tein measurements to assess response to treatment, but they can also be used more frequently in the early weeks of treatment.
With the advent of newer and more sen-sitive laboratory techniques, very small amounts of myeloma disease can be measured by flow cytometry or genome sequencing analysis of bone marrow biopsy samples. This small amount of myeloma disease is called Minimal
Residual Disease, or MRD, and testing for MRD should be potentially performed only after other laboratory tests for the M-protein (i.e., SPEP, Freelite, Hevylite) show no detectable disease. Table 2 details the criteria for assessing patient response to treatment, including strin-gent complete response and measuring minimal residual disease. If the free light chain ratio becomes normal after treat-ment, then this provides a very good and sensitive indication that treatment has been highly effective, and means that the level of light chain paraprotein has been reduced as much as possible.
Normalization of the Freelite ratio is a component of a stringent complete response (sCR). Updated IMWG consensus guidelines on the assessment of minimal residual disease (MRD) defi e sCR as:
n negative IFE on the serum and urine,
n disappearance of any soft tissue plasmacytomas,
n < 5% plasma cells in bone marrow aspirates,
n absence of clonal cells in bone marrow by immunohistochemistry (κ/λ ratio ≤ 4:1 or ≥ 1:2 for k and λ patients, respec-tively, after counting ≥ 100 plasma cells) or 2- to 4-color flow cytometry in bone marrow aspirates, and
n normal free light chain ratio.
In summary, the Freelite assay offers sev-eral advantages for diagnosis and moni-toring of treatment:
n Inclusion of Freelite assay can improve the sensitivity of screening protocols for detection and diagnosis of myeloma.
n The Freelite assay, along with other tests, can provide valuable informa-tion for people with MGUS and SMM.
n Use of the Freelite assay to monitor treatment reveals responses to treat-ment earlier than other laboratory tests such as SPEP.
n The improved sensitivity of the Freelite assay over IFE may allow earlier detec-tion of a relapse of myeloma.
n The Freelite assay is recommended for use in diagnosis, prognosis, and mon-itoring in the guidelines published by the IMWG.
Current National Comprehensive Cancer Network (NCCN) Clinical Practice Guide-lines in Oncology recommend the use of polyclonal serum free light chain assays (Freelite) for diagnosis, prognosis, and monitoring of myeloma.
Patients who benefit the most from the Freelite assayn People with myeloma who have
abnormal serum free light chain results at the start of treatment. Mon-itoring with the serum free light chain
1312 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
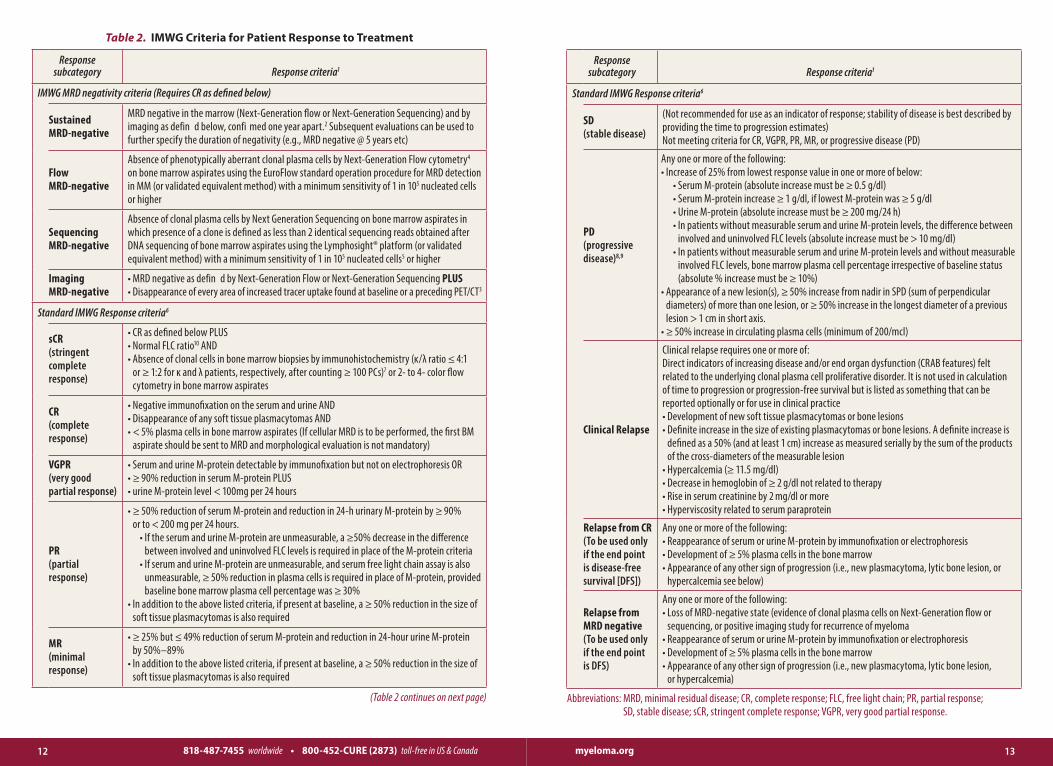
Table 2. IMWG Criteria for Patient Response to Treatment
Response subcategory Response criteria1
IMWG MRD negativity criteria (Requires CR as defined below)
Sustained MRD-negative
MRD negative in the marrow (Next-Generation flow or Next-Generation Sequencing) and by imaging as defin d below, confi med one year apart.2 Subsequent evaluations can be used to further specify the duration of negativity (e.g., MRD negative @ 5 years etc)
Flow MRD-negative
Absence of phenotypically aberrant clonal plasma cells by Next-Generation Flow cytometry4 on bone marrow aspirates using the EuroFlow standard operation procedure for MRD detection in MM (or validated equivalent method) with a minimum sensitivity of 1 in 105 nucleated cells or higher
Sequencing MRD-negative
Absence of clonal plasma cells by Next Generation Sequencing on bone marrow aspirates in which presence of a clone is defined as less than 2 identical sequencing reads obtained after DNA sequencing of bone marrow aspirates using the Lymphosight® platform (or validated equivalent method) with a minimum sensitivity of 1 in 105 nucleated cells5 or higher
Imaging MRD-negative
• MRD negative as defin d by Next-Generation Flow or Next-Generation Sequencing PLUS • Disappearance of every area of increased tracer uptake found at baseline or a preceding PET/CT3
Standard IMWG Response criteria6
sCR (stringent complete response)
• CR as defined below PLUS • Normal FLC ratio10 AND • Absence of clonal cells in bone marrow biopsies by immunohistochemistry (κ/λ ratio ≤ 4:1
or ≥ 1:2 for κ and λ patients, respectively, after counting ≥ 100 PCs)7 or 2- to 4- color flow cytometry in bone marrow aspirates
CR (complete response)
• Negative immunofixation on the serum and urine AND• Disappearance of any soft tissue plasmacytomas AND• < 5% plasma cells in bone marrow aspirates (If cellular MRD is to be performed, the first BM
aspirate should be sent to MRD and morphological evaluation is not mandatory)
VGPR (very good partial response)
• Serum and urine M-protein detectable by immunofixation but not on electrophoresis OR• ≥ 90% reduction in serum M-protein PLUS • urine M-protein level < 100mg per 24 hours
PR (partial response)
• ≥ 50% reduction of serum M-protein and reduction in 24-h urinary M-protein by ≥ 90% or to < 200 mg per 24 hours.
• If the serum and urine M-protein are unmeasurable, a ≥50% decrease in the difference between involved and uninvolved FLC levels is required in place of the M-protein criteria
• If serum and urine M-protein are unmeasurable, and serum free light chain assay is also unmeasurable, ≥ 50% reduction in plasma cells is required in place of M-protein, provided baseline bone marrow plasma cell percentage was ≥ 30%
• In addition to the above listed criteria, if present at baseline, a ≥ 50% reduction in the size of soft tissue plasmacytomas is also required
MR (minimal response)
• ≥ 25% but ≤ 49% reduction of serum M-protein and reduction in 24-hour urine M-protein by 50%–89%
• In addition to the above listed criteria, if present at baseline, a ≥ 50% reduction in the size of soft tissue plasmacytomas is also required
(Table 2 continues on next page)
Response subcategory Response criteria1
Standard IMWG Response criteria6
SD (stable disease)
(Not recommended for use as an indicator of response; stability of disease is best described by providing the time to progression estimates)Not meeting criteria for CR, VGPR, PR, MR, or progressive disease (PD)
PD (progressive disease)8,9
Any one or more of the following: • Increase of 25% from lowest response value in one or more of below:
• Serum M-protein (absolute increase must be ≥ 0.5 g/dl)• Serum M-protein increase ≥ 1 g/dl, if lowest M-protein was ≥ 5 g/dl• Urine M-protein (absolute increase must be ≥ 200 mg/24 h) • In patients without measurable serum and urine M-protein levels, the difference between
involved and uninvolved FLC levels (absolute increase must be > 10 mg/dl)• In patients without measurable serum and urine M-protein levels and without measurable
involved FLC levels, bone marrow plasma cell percentage irrespective of baseline status (absolute % increase must be ≥ 10%)
• Appearance of a new lesion(s), ≥ 50% increase from nadir in SPD (sum of perpendicular diameters) of more than one lesion, or ≥ 50% increase in the longest diameter of a previous lesion > 1 cm in short axis.
• ≥ 50% increase in circulating plasma cells (minimum of 200/mcl)
Clinical Relapse
Clinical relapse requires one or more of:Direct indicators of increasing disease and/or end organ dysfunction (CRAB features) felt related to the underlying clonal plasma cell proliferative disorder. It is not used in calculation of time to progression or progression-free survival but is listed as something that can be reported optionally or for use in clinical practice• Development of new soft tissue plasmacytomas or bone lesions• Definite increase in the size of existing plasmacytomas or bone lesions. A definite increase is
defined as a 50% (and at least 1 cm) increase as measured serially by the sum of the products of the cross-diameters of the measurable lesion
• Hypercalcemia (≥ 11.5 mg/dl) • Decrease in hemoglobin of ≥ 2 g/dl not related to therapy• Rise in serum creatinine by 2 mg/dl or more • Hyperviscosity related to serum paraprotein
Relapse from CR (To be used only if the end point is disease-free survival [DFS])
Any one or more of the following:• Reappearance of serum or urine M-protein by immunofixation or electrophoresis• Development of ≥ 5% plasma cells in the bone marrow• Appearance of any other sign of progression (i.e., new plasmacytoma, lytic bone lesion, or
hypercalcemia see below)
Relapse from MRD negative (To be used only if the end point is DFS)
Any one or more of the following:• Loss of MRD-negative state (evidence of clonal plasma cells on Next-Generation flow or
sequencing, or positive imaging study for recurrence of myeloma• Reappearance of serum or urine M-protein by immunofixation or electrophoresis• Development of ≥ 5% plasma cells in the bone marrow• Appearance of any other sign of progression (i.e., new plasmacytoma, lytic bone lesion,
or hypercalcemia)
Abbreviations: MRD, minimal residual disease; CR, complete response; FLC, free light chain; PR, partial response; SD, stable disease; sCR, stringent complete response; VGPR, very good partial response.
1514 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
1. All response categories require two consecutive assessments made at any time before the institution of any new therapy; for MRD there is no need for two consecutive assessments, but information on MRD after each treatment stage is recommended (e.g.: after induction, HDT/ASCT, consolidation, maintenance). MRD tests should be initiated only at the time of suspected CR. Early indications from studies suggest that bone marrow aspirates for MRD testing by fl w should only be done if there is normalization of Freelite and Hevylite assays. Bone marrow should only be sampled two months after CR is reached in order to ensure that the bone marrow has had time to refle t the nega-tive status. All categories of response and MRD also require no known evidence of progressive or new bone lesions if radiographic studies were performed. However, radiographic studies are not required to satisfy these response requirements except for the requirement of FDG-PET if imaging MRD-negative status is reported.
2. Sustained MRD-negative when reported should also annotate the method used (e.g., Sustained Flow MRD-negative, Sustained Sequencing MRD-negative).
3. Criteria used by Zamagni et al., which, so far, was the only one showing the prognostic value of PET/CT in the MRD setting.106 Imaging should be performed once MRD negativity is determined by MFC or NGS.
4. Bone marrow fl w cytometry should follow Next-Generation Flow (NGF) guidelines.29 The reference NGF method is an 8 color 2 tube approach which has been extensively validated. The 2 tube approach improves reliability, consistency and sensitivity because of the acquisition of a greater number of cells. The 8 color technology is widely available globally and the NGF method has already been adopted in many fl w laboratories across the world. The complete 8 color method is most effici t using the lyophilized mixture of antibodies which reduces errors, time, and costs. It is recommended that 5 million cells be assessed. Flow cytometry method employed should have a sensitivity of detection of plasma cells of at least 1 in 105.
5. DNA sequencing assay on marrow aspirate should use an assay such as Lymphosight® (Sequenta) since this is the only one validated so far.
6. Derived from International uniform response criteria for multiple myeloma. Durie BG, et al. Leukemia. 2006 Sep;20(9):1467-73. Minor response definition and clarifications derived from Rajkumar SV et al. Consensus recom-mendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood. 2011 May 5;117(18):4691-5. For coding CR and VGPR in patients in whom the only measurable disease is by serum FLC levels: CR in such patients indicates a normal FLC ratio of 0.26 to 1.65 in addition to CR criteria listed above. VGPR in such patients requires a ≥ 90% decrease in the difference between involved and uninvolved FLC levels. All response categories require two consecutive assessments made at any time before the institution of any new therapy; all categories also require no known evidence of progressive or new bone lesions or extramedullary plasmacytomas if radiographic studies were performed. Radiographic studies are not required to satisfy these response requirements. Bone marrow assessments need not be confirme . Each category, except for stable disease, will be considered unconfirmed u til the confirm tory test is performed. The date of the initial test is considered as the date of response for evaluation of time dependent outcomes such as duration of response.
7. Presence/absence of clonal cells on immunohistochemistry is based upon the K/L ratio. An abnormal K/L ratio by immunohistochemistry requires a minimum of 100 plasma cells for analysis. An abnormal ratio refle ting presence of an abnormal clone is K/L of > 4:1 or < 1:2.
8. Positive immunofix tion alone in a patient previously classified as CR will not be onsidered progression. For purposes of calculating time to progression and progression-free survival, CR patients and MRD-negative patients should be evaluated using criteria listed above for progressive disease (PD). Criteria for relapse from CR or relapse from MRD should be used only when calculating DFS.
9. In the case where a value is felt to be a spurious result per physician discretion (for example, a possible lab error), that value will not be considered when determining the lowest value.
10. All recommendations regarding clinical utilities relating to serum free light chain levels or FLC ratio is based on results obtained with the Freelite test. Dejoie et al. have recently published a comparison of Freelite and UPEP for the detection of the light chain component of monoclonal immunoglobulins in light chain and intact immunoglobulin myeloma (Haematologica, published ahead of print December 3, 2015) which demonstrates the improved sensitivity of Freelite assay over UPEP for monitoring response to treatment.
Footnotes to Table 2. assays often allows a rapid assessment of the effectiveness of treatment.
n People with very low levels of light chains that are undetectable by other tests such as SPEP, UPEP, and IFE. These are people who generally have non-secretory (also called hyposecretory, oligosecretory, or paucisecretory) myeloma. Approximately 70% of peo-ple with nonsecretory myeloma can have their disease monitored using the Freelite assay.
n People with deposits of light chains in the form of AL amyloidosis. People with AL amyloidosis may or may not have active myeloma. Tracking the light chain levels is very helpful to assess the disease status.
n People with light chain-only (Bence-Jones) myeloma. The major advan-tages of the Freelite assay for these people are:
l Ease of blood testing versus 24-hour urine collection. (It is important to note that periodic 24-hour urine testing is still recommended and necessary, both to double-check the light chain excretion level and monitor for any evidence of kidney damage.)
l Greater sensitivity of blood testing. (Mildly increased levels may be detected in the blood but not detected in the urine.)
What is the Hevylite assay?The serum heavy + light chain isotype (Hevylite) assay is a laboratory blood test for measuring intact immunoglobulins. It is the only automated immunoas-say approved by the US Food and Drug Administration (FDA) for monitoring IgG and IgA myeloma. According to the FDA approval, the Hevylite assay is to be used for previously diagnosed myeloma in conjunction with other clinical and laboratory findings.
M-protein can be made up of just an immu-noglobulin heavy chain (IgG, IgA, IgD, IgE, or IgM), just a free light chain (free kappa or lambda), or, in the majority of cases, a heavy chain with an associated free light chain (IgG kappa and IgG lambda, IgA kappa and IgA lambda, etc.) as seen in Table 1. While the Freelite test quantifies free light chains, and has been most help-ful for patients with light chain disease, low-secreting disease, and amyloidosis,

1716 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
The Hevylite assay and monitoring for residual diseaseThe high sensitivity of the Hevylite assay can also indicate the presence of minimal residual disease (MRD) even in patients classified as being in complete response (CR) or stringent complete response (sCR) by other methods. A lower than normal level of the uninvolved HLC indicates that there is enough myeloma present to sup-press normal immune system cells, even if the amount of abnormal (monoclonal) protein (or iHLC) is undetectable. Early indications from studies suggest that patients in CR or sCR whose bone marrow is being assessed for MRD in clinical trials should first be screened with the Freelite and Hevylite assays. If those sensitive assays show abnormal Freelite and/or Hevylite ratios, the patient is not ready for MRD testing and should therefore delay the bone marrow biopsy until the ratios become normal. Bone marrow biopsy should not be done until approximately two months after CR is reached in order to allow time for the bone marrow to reflect the negative status.
What are normal Hevylite levels?Each laboratory may establish local nor-mal ranges, but for general guidance, normal ranges for Hevylite (HLC) values are listed in Table 3.
Can Freelite and Hevylite be used together?Myeloma cells from a single patient can produce multiple clones that may pro-duce intact immunoglobulins, free light chains, or both. Since the free light chain assay and the heavy + light chain isotype assay measure independent biomark-ers of disease activity, it is important to monitor patients with both tests. Given the heterogeneity of clones in an individ-ual patient’s myeloma, these two assays, when used together, are complementary.
Will insurance cover the cost of Freelite and Hevylite assays? In the United States, the serum free light chain assays are covered by Medicare and most private insurers. Hevylite assays are covered under the same medical billing CPT code as Freelite; the cost to the patient may vary, however, depend-ing upon which laboratory performs the testing.
In closingWhile a diagnosis of cancer is something you cannot control, gaining knowledge that will improve your interaction with your doctors and nurses is something you can control, and it will have a significant impact on how well you do throughout the disease course.
the Hevylite test quantifies the intact, or whole, immunoglobulin heavy and light chains involved in a patient’s myeloma (IgG kappa or IgA lambda, for example).
What is a heavy/light chain ratio?The Hevylite (HLC) assay recognizes when a specific heavy chain is bound to a specific light chain. It can distinguish between the “involved” proteins – the heavy and light chain produced by the myeloma (termed iHLC) – and their “unin-volved” (i.e., normal or polyclonal – not monoclonal, termed uHLC) counterparts that have the same heavy chain isotype but bound to a different light chain. An example would be that of a patient with IgG lambda monoclonal protein (the “involved” heavy and light chain) and the patient’s isotype-paired normal or “unin-volved” protein, IgG kappa. In this case, it would be appropriate to order Hevylite IgG lambda (the iHLC) and IgG kappa (the uHLC). Similarly, for an IgA lambda myeloma patient, Hevylite IgA lambda and IgA kappa would be ordered.
Not only does the Hevylite assay calculate the amount of iHLC and uHLC, but like the Freelite assay, it calculates the ratio between the involved and uninvolved proteins (HLC ratio), and then compares them to normal ranges for these blood proteins. Also like the Freelite assay, the Hevylite assay is very sensitive and is auto-mated, so it can accurately detect mono-clonal immunoglobulins at very low levels in the blood. Hevylite values are import-ant in assessing myeloma activity because they accurately reveal not only the amount of monoclonal protein (iHLC), but the amount of normal uninvolved immu-noglobulin protein (uHLC) as well. When the uHLC is lower than normal, it demon-strates the extent to which the uHLC has been suppressed by the myeloma.
How does the Hevylite assay differ from SPEP?For patients with IgA kappa or IgA lambda myeloma, standard serum protein elec-trophoresis is not a particularly reliable test. The Hevylite assay is an effective alternative for quantifying the M-protein of these IgA patients.
The Hevylite assay and monitoring for relapseThe Hevylite assay can detect relapses earlier than most other methods currently available. If a patient’s Hevylite assay does not produce a normal Hevylite ratio, this is an indication that the myeloma cells are again producing monoclonal protein. Because the Hevylite assay is very sensi-tive, it can detect a relapse before it is picked up by SPEP or IFE.
Table 3. Normal Ranges for HLC Values
HLC Range
IgG kappa (g/L) 4.03–9.78
IgG lambda (g/L) 1.97–5.71
IgG kappa/IgG lambda ratio 0.98–2.75
IgA kappa (g/L) 0.48–2.82
IgA lambda (g/L) 0.36–1.98
IgA kappa/IgA lambda ratio 0.80–2.04
1918 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
Immunofixation electrophoresis (IFE): An immunologic test of the serum or urine used to identify proteins. For myeloma patients, it enables the doctor to identify the M-protein type (IgG, IgA, kappa, or lambda). The most sensitive routine immu-nostaining technique, it identifies the exact heavy and light chain type of M-protein.
Immunofluor scence: This test uses the specificity of antibodies to their antigen to target fluorescent dyes to specific targets within a cell, and therefore allows visu-alization of the distribution of the target molecule through the sample. Immuno-fluorescence makes use of fluorophores to visualize the location of antibodies. A fluorophore is a fluorescent chemical compound that can re-emit light upon light excitation. Fluorophores are used as probes or indicators.
Immunoglobulin (Ig): A protein pro-duced by plasma cells; an essential part of the body’s immune system. Immunoglob-ulins attach to foreign substances (anti-gens) and assist in destroying them. The classes (also called isotypes) of immuno-globulins are IgG, IgA, IgD, IgE, and IgM. The non-medical word for immunoglobu-lin is “antibody.”
Immunohistochemistry (IHC): Immuno-histochemistry refers to the process of detecting antigens (e.g., proteins) in cells of a tissue section by exploiting the prin-ciple of antibodies binding specifically to antigens in biological tissues. Immu-no-histochemical staining is widely used in the diagnosis of abnormal cells such as those found in cancerous tumors.
Minimal residual disease (MRD): The presence of residual tumor cells after treat-ment has been completed and complete
remission (CR) has been attained. Even patients who have attained a stringent complete response (sCR) may have MRD. Very sensitive new testing methods are now able to detect one myeloma cell among one million sampled cells in blood or bone marrow.
Monoclonal gammopathy of undeter-mined significance (MGUS): A category of plasma cell disorder characterized by compara tively low levels of monoclonal protein in the blood and/or urine. Bone marrow plasma cell levels are low (< 5%). Myeloma-related symptoms (i.e., anemia, renal failure, hypercalcemia, and lytic lesions) are absent.
Monoclonal protein (M-protein): An abnormal protein produced by myeloma cells that accumulates in and damages bone and bone marrow. A high level of M-protein indicates that myeloma cells are present in large numbers.
This booklet is not meant to replace the advice of your doctors and nurses, who are best able to answer questions about your specific healthcare management plan. The IMF intends only to provide you with information that will guide you in discussions with your healthcare team. To help ensure effective treatment with good quality of life, you must play an active role in your own medical care.
We encourage you to visit myeloma.org for up-to-date information about mye-lo ma, and to contact the IMF InfoLine with your myeloma-related questions and concerns. The IMF InfoLine con sistently provides callers with the best information about myeloma in a caring and compas-sionate manner. IMF InfoLine specialists can be reached at [email protected], or 800-452-CURE (2873) or 818-487-7455.
Terms and definitionsBone marrow: The soft, spongy tissue in the center of bones that produces white blood cells, red blood cells, and platelets. This is the tissue within which abnormal plasma cells build up to cause myeloma.
Electrophoresis: A laboratory test in which a patient’s serum (blood) or urine mole-cules are subjected to separation accord-ing to their size and electrical charge. For myeloma patients, electrophoresis of the blood or urine allows both the calculation of the amount of myeloma protein (M-pro-tein) as well as the identification of the spe-cific M-spike characteristic for each patient. Electrophoresis is used as a tool both for diagnosis and for monitoring.
Extramedullary plasmacytoma: A tumor made up of monoclonal plasma cells that is found in soft tissue outside of the bone marrow and separate from bone.
Flow cytometry: A technology used in cell counting, cell sorting, and biomarker detection by suspending cells in a stream of fluid and passing them through a laser.
Hyposecretory: Low- or non-secreting disease.
Immunoassay: Test used in the study of biological systems by tracking differ-ent proteins, hormones, and antibodies. Immunoassays rely on the inherent ability of an antibody to bind to the specific struc-ture of a molecule. Because antibodies are developed to the specific three-dimen-sional structure of an antigen, they are highly specific and will bind only to that structure. ELISA (enzyme-linked immuno-sorbent assay) is a commonly used test to detect antibodies in the blood.
2120 myeloma.org818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
Multiple myeloma: A cancer arising from the plasma cells in the bone marrow. The cancerous plasma cells are called myeloma cells.
Plasma cells: Special white blood cells that produce antibodies (immunoglobu-lins). Myeloma is a cancer of the plasma cells. Malignant plasma cells are called myeloma cells. In myeloma, malignant plasma cells produce large amounts of abnormal antibodies that lack the capa-bility to fight infection. These abnormal antibodies are the monoclonal protein, or M-protein, that functions as a tumor marker for myeloma. Plasma cells also produce other chemicals that can cause organ and tissue damage (i.e., anemia, kidney damage, and nerve damage).
Plasmacytoma: See “Extramedullary plas-macytoma” and “Solitary plasmacytoma of the bone (SPB)”
Remission or response: Complete or partial disappearance of the signs and symptoms of cancer. Remission and response are interchangeable terms.
• Stringent complete response (sCR) – sCR is CR (as defined below) plus normal FLC ratio and absence of clonal cells in bone marrow by immunohistochemis-try or immunofluorescence.
• Complete remission (CR) – CR is negative immunofixation on serum and urine, and disappearance of any soft tissue plasmacytomas, and less than or equal to 5% plasma cells in bone marrow. CR is not the same as a cure.
• Very good partial remission (VGPR) – VGPR is less than CR. VGPR is serum M-protein and urine M-protein detect-able by immunofixation but not on electrophoresis, or 90% or greater reduction in serum M-protein, plus urine M-protein < 100 mg per 24 hours.
• Partial remission (PR) – PR is a level of response in which there is at least a 50% reduction in M-protein, and reduction in 24-hour urinary M-protein by at least 90% (or to less than 200 mg/24 hrs).
Solitary plasmacytoma of bone (SPB): A discreet, single mass of monoclonal plasma cells in a bone. The diagnosis of SBP requires a solitary bone lesion, a biopsy of which shows infiltration by plasma cells; negative imaging results for other bone lesions; absence of clonal plasma cells in a random sample of bone marrow; and no evidence of anemia, hypercalcemia, or renal involvement sug-gesting systemic myeloma.
Notes
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________The printing of this patient education booklet was
supported by a grant from The Binding Site.
22 818-487-7455 worldwide • 800-452-CURE (2873) toll-free in US & Canada
Notes
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
One of the most daunting aspects of being diagnosed with multiple myeloma (MM) is learning about – and understanding – an unfamiliar disease that is quite complicated. From diagnosis to long-term survival, the 10 Steps to Better Care® will guide you through the MM journey:
1. Know what you’re dealing with. Get the correct diagnosis.
2. Tests you really need.
3. Initial treatment options.
4. Supportive care and how to get it.
5. Transplant: Do you need one?
6. Response Assessment: Is treatment working?
7. Consolidation and/or maintenance.
8. Keeping Track of the Myeloma: Monitoring without mystery.
9. Relapse: Do you need a change in treatment?
10. New Trials: How to find them.
Visit 10steps.myeloma.org to gain a better understanding of the disease and diagnosis, and proceed through the steps to learn the best tests, treatments, supportive care, and clinical trials currently available.
As always, the International Myeloma Foundation (IMF) urges you to discuss all medical issues thoroughly with your doctor. The IMF is here to equip you with the tools to understand and better manage your MM. Visit the IMF website at myeloma.org or call the IMF InfoLine at 800-452-CURE (2873) or 818-487-7455 to speak with our trained information specialists about your questions or concerns. The IMF is here to help.
A UNIQUE TOOL FOR DIAGNOSTIC AND TREATMENT INFORMATION
10 STEPS TO BETTER CARE®