Embed Size (px)
Citation preview

Conmnmity Dent Oral Epidemiol 1997: 25: 228-32Printed in Denmarii . Ait rights reserved
Copyright © Munk.sgaard 1997
Communify Dentistryand Oral Epidemiology
ISSN 0301-5661
Understanding decision-makingprocesses for sugar consumptionin adolescence
Ruth Freeman^ andAubrey Sheiham^^Dental Public Health Research Group, School ofClinical Dentistry, The Queen's University ofBelfast, Belfast, Northern Ireland and^Department of Epidemiology and Public Health,University College, London Medical School,London, UK
Freeman R, Sheiham A; Understanding decision-making proeesses Ibr sugarconsumption in adolescence. Community Dent Oral Epidemiol 1997; 25; 228-32.© Munksgaard, 1997
Abstraet - The mechanisms by which adolescents make food choices are notclear. The interaction and combination of the many social and psychological fac-tors must be considered when examining adolescents' decision-making processesfor sound food choices. The aim of this investigation is to examine one specificfood choice, namely, the use of sucrose in hot drinks. One hundred and eighty-seven adolescents in their 16th year completed a questionnaire on the consump-tion of sugar using the method developed by AJZEN & FISHBEIN in their Theoryof Reasoned Action'. The group was randomly divided into two groups so thatdecision-making processes with respect to two behavioural intentions - addingsugar to tea and coffee and excluding it - could be examined. The findings suggestthat the immediate pleasurable taste of sugar outweighed and deferred the re-cognition of dangers associated with its eonsumption. Past dental health experi-ences, behaviours and education together with the role of parental figures actedas important influences. An awareness of these factors should assist dental healthprofessionals to highlight the importance of sound food choices when negotiatingdental health goals with adolescents.
Key words: adolescence; decision-making; sugarconsumption; theory of reasoned action
Ruth Freeman, School of Clinical Dentistry, TheQueen's University of Belfast, Belfast BT12 6BP,Northern Ireland
Accepted for publication 2 November 1996
Reducing sugar consumption to preventdental earies is a common goal. Dentalhealth edueation aims to encouragepeople to eat more starchy, fibrousfoods and reduce the frequency of sug-ary snacks and drinks. However, therole of health education, with the res-ulting ability of an adoleseent to makesound food choices, is difficult sincesugar consumption is overlaid withboth sociological and psychologicalmeaning (2, 3). The family (4), peergroups (5), palatability of sugars (2)and concerns about general health (6),dental health (7) and appearance (8) allaffect choices. The interaction andcombination of the above faetors mustbe considered when examining adoles-cents' decision-making processes for'sound food choices'.
The aim of this investigation was to
examine the decision-making processesinvolved when adolescents make a spe-cific food choice, namely, the use ofsucrose in hot drinks. To achieve the aimof the project it was necessary to use amethodology which was known to be ef-fective in examining deeision-making,especially when the behaviour in ques-tion was under volitional control (9).The framework developed by AJZEN &FISHBEIN (1) in their Theory of Rea-soned Action' was particularly suitablesince it had been previously used, suc-cessfully, to examine other aspects offood ehoice in adolescents (10-12).Therefore it was decided to use thetheory of reasoned action (1) to assist inexamining the nature of the intercon-necting factors known to be employed indecision-making.
The theory of reasoned action con-
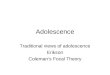
siders that individuals act in a rationalmanner, making decisions based onavailable information, which in turn isaffected by the individual's attitudesand the influence of those who are im-portant to them (subjective norms) (1,9). Attitudes within this framework (1)(Fig. 1) refer to the subject's positive ornegative evaluations of the particularbehaviour. Attitudes are derived frombeliefs about the behaviour togetherwith the outcome evaluations of thosebeliefs. The subjective norm refers tothe normative beliefs and the degree towhieh the subject will comply with thewishes of those important to them. Thesubjective norm is derived frotn the in-dividual's belief that others importantto them wish them to behave in a par-tieular way (normative beliefs) togetherwith their motivation to comply with

Decision-making processes for sugar consumption 229
EXTERNALVARIABLES
Demography
Attitudes ToPeople And Places
PersonalityTraits
Salient
Beliefs\
OutcomesEvaluations
BEHAVIOURALINTENTION
BEHAVIOUR
NormativtBeliefs
\
To Comply
SUB]ECriVE
NORM
• ^ Possible Relationships Between Externiil Variables And Behaviour
^S tab le Theoretical Relations Linking Beliefs To [Jehaviour
Fig. J. The theory of reasoned action. The relations between beliefs, attitudes, subjectivenorms, intention, behaviour and external variables.
the wishes of those important people.When the attitudes and snbjeetivenorms are weighted and regressedagainst the behavioural intention, thenthe behaviour being examined can bepredicted (Fig. 1).
Methods
The investigation used a two-stage sam-pling technique to select the subjects.First, a random selection of a 10 pereent sample from the population of 16-year-old adolescents attending schoolsin the North East Thames Region ofLondon, Fngland, was made. Seeond,from this 10 per cent sample, a stratifiedcluster sample of 200 subjects from 16schools was randomly chosen to give anaccurate representation of the soeio-economic background of the adoles-cents. The selected pupils were thenrandomly divided into two groups. Onegroup reeeived a questionnaire aboutthe addition of suerose to tea and eoffee(Intention 1) whereas the other groupanswered a questionnaire about the ex-elusion of sugar from tea and coffee(Intention 2).
As the study used the theory of rea-soned action, the method of question-naire design reeommended by AJZEN &FiSHBEtN (1) was used to assess the be-haviour under examination. In accor-dance with their questionnaire design, aseries of in-depth interviews with 20 16-
year-old adoleseents was conducted amonth prior to the start of the final in-vestigation. The adolescents were cho-sen to represent as far as possible thosesubjects who would take part in the fi-nal investigation. The interviews tookplace in an interviewing room with easychairs and coffee table. Permission wasobtained from the adolescents to tape-record the interviews. The adoleseentswere encouraged to speak freely and todiseuss their eating habits in generaland their beliefs about sound foodchoices in particular. This is an impor-tant step within the eonstruction of thequestionnaire as it is essential to dis-cover the single actions whieh composethe behavioural complex. In addition,AJZEN & FISHBEIN (1) emphasise the im-portance of identifying the eight mostsalient beliefs and the four most salientreferents (subjective norm) from the in-depth interviews as the first step in theirquestionnaire design.
From the in-depth interviews, it wasnoted that some adolescents relatedtheir beliefs about the use of sucrose inhot drinks to the exelusion of sugarfrom tea and coffee whilst others re-lated the same beliefs to the inclusionof sugar in tea and coffee. What beeameapparent was that the adolescents' be-liefs and their salient referents (othersimportant to them) were the same, irre-spective of whether or not they addedor excluded sugar in tea and coffee.
Therefore the eight beliefs and the foursalient referents assoeiated with the be-havioural intentions to stop takingsugar in tea and coffee or to add sugarwhen drinking tea and coffee could beclearly identified. It was then importantto find out how the same beliefs and sa-lient referents were used in the decision-making process to exclude or add sugarin tea and coffee.
The first step in this proeess was tooperationalise the beliefs. This wasdone simply by asking the respondents,for example, 'How strongly do you be-lieve that adding sugar to your tea andcoffee will cause you to gain weight?'In the exclusion-of-sugar questionnairethe respondents were asked, 'Howstrongly do you believe that stoppingsugar in your tea and eoffee will causeyou to lose weight?' In this way the sa-lience of the beliefs in relation to thebehavioural intentions could be as-sessed.
The next step was to operationalisethe outcome evaluations with respeet toeach of the eight beliefs. This was doneby asking the respondents, 'How impor-tant is it to you, personally, that by add-ing sugar to your tea and eoffee you willgain weight?' In the exclusion-of-sugarquestionnaire the respondents wereasked, 'How important is it to you, per-sonally, that by stopping sugar in yourtea and eoffee you will lose weight?'
The third step was the operationali-sation of the normative beliefs. Theseincluded questions such as, 'Howstrongly do your friends believe that ifyou add sugar to your tea and coffeeyou will gain weight?' and for the exelu-sion-of-sugar questionnaire 'Howstrongly do your friends believe that ifyou stop sugar in your tea and eoffeeyou will lose weight?'
Finally, the motivation to eomplywith each referent (Table 1) was as-sessed. The motivation to comply withthe variables was the same for bothquestionnaires. They included questionssueh as 'Generally, do you want to dowhat your parents want you to do?'
The next part of the model (1) requir-es the ealculation of attitudes towardseither adding or excluding sugar in teaand coffee and the equivalent subjectivenorms. Attitude scores were calculatedas a product of the salient beliefs withthe outcomes evaluations. Attitudeseores were calculated as a product of

230 EREEMAN & SHEIHAM
Table I, Beliefs and salient referents of sugar consumption
Beliefs in relation to sugar consumption Salient referents (important others)
1, Weight gain2, Spots3, Pleasant taste of sugar4, Tooth decay5, Blood disease6, Heart disease7, Craving for sugar - sweet taste8, Having loads of energy
1, Parent2, Friend3, Biology teacher4, Physical education teacher
the salient beliefs which were scoredfrom 7 (most strongly held) to 1 (leaststrongly held) with the outcome evalua-tions. The outcome evaluation wasscored on a scale from 7 (extremely im-portant) to 1 (extremely unimportant).The total attitude score was the sum ofthe eight individual attitude questions.Subjeclive norms are a product of thenormative belief scores (scored as forthe salient beliefs) with those of the mo-tivation to comply with the variables.The range of possible scores being from-1-3 (greatest influence from importantothers) to - 3 (least infiuence). Therange of seores for the intention ques-tion 'Do you intend to add sugar to teaand coffee?' was from 7 (extremely like-ly) to 1 (extremely unlikely). The rangeof scores for the intention question 'Doyou intend to stop taking sugar in teaand coffee?' was from 7 (extremely like-ly) to 1 (extremely unlikely).
Two sets of questionnaires were de-veloped, using equivalent formats tooperationalise the independent vari-ables - that is, the beliefs, tbe outcomeevaluations, tbe normative beliefs andthe motivation to comply with the vari-ables. The only difference between thequestionnaires was the dependent vari-ables - that is, the intention to addsugar to tea and coffee or the intentionto exclude sugar from tea and coffee.The final questionnaires therefore oper-ationalised the eight beliefs and four re-ferents as presented in Table 1.
In addition tbe two sets of question-naires incorporated a series of ques-tions to assess external variables (1).These included questions on dentalhealth knowledge, such as the role ofsugar in causation of dental decay; den-tal health attitudes, such as satisfactionwith teeth; and dental healtb behav-iours, such as dental attendance pat-terns. The questionnaires were piloted
and finally administered by their teach-ers to the adolescents at the 16 schools.
The completed questionnaires wereseored and analysed statistically usingt-tests, correlation and stepwise regres-sion analysis (1).
Results
Of the 200 adolescents invited to takeparl, 187 completed the questionnaires,giving a valid response rate of 94 percent. Approximately half of the adoles-cents (95) completed the questionnaireon the addition of sugar in tea and cof-fee and the remainder (92) the question-naire on the exclusion of sugar. All ofthem were in their 16th year and therewere no statistical differences betweenthe number of males and females in thetwo groups.
A stepwise regression analysis of allof the independent variables against thedependent variables of the behaviouralintention to add sugar to hot drinks(Intention 1) and to exclude sugar fromtea and coffee (Intention 2) was con-ducted. Intention 1 was predicted by thetotal attitude score, toothbrushing be-haviours, and regularity of dental atten-dance. This accounted for 26 per cent ofthe total variance. Eor Intention 2 thesignificant predictors were irregularityof dental attendance and being know-ledgeable about the role of sugar in theaetiology of dental caries. These vari-ables only explained 5 per cent of thetotal variance (Table 2).
Correlation analysis for 'the additionof sugar' group demonstrated that In-tention 1 was significantly assoeiatedwith total attitude score and dental at-tendance. Toothbrushing behaviour wassignificantly and positively associatedwitb regularity of dental attendance,and negatively with Intention 1 and feltneed for dental treatment. An equiva-
lent correlation analysis was carried outon the 'exclusion of sugar' group. Thisdemonstrated significant and positivecorrelations between Intention 2 andtoothbrushing behaviours and know-ledge that sugar causes tooth decay.There was also a negative but significantcorrelation between Intention 2 andregularity of dental attendance. Othersignificant associations were betweentoothbrushing behaviour and beingknowledgeable about sugar and dentalcaries; a negative association existed be-tween dental attendance and felt needfor dental treatment (Table 3).
The motivation of the two groups tocomply with the wishes of the salient re-ferents (Table 1) was compared. Adoles-cents in the 'addition of sugar' grouphad higher mean scores for compliancewith parents compared with the 'exclu-sion' group [t=2.28; P<0.05]. No otherdifferences could be demonstrated be-tween the groups for the influence off"riends or teachers.
The most strongly held attitude forthe adolescents from both the 'additionof sugar' group and the 'exclusion ofsugar' group was the sweet and pleasanttaste of sugar,
Eemales in the 'addition of sugar totea and eoffee' group had significantlyhigher mean scores than males for thebeliefs that sugar was an important fac-tor in weight gain [t=2.30; P<0.05] andin heart disease [t=2.33; P<0.05].Males compared with the females hadhigher mean scores for the beliefs thateating sugar was pleasurable [t = 5.62;P<0.00\] and provided energy [t=2.92;P<0.01]. Male adolescents had signifi-cantly higher mean scores for the out-come evaluations - the importance ofthe pleasurable taste of sugar [t=3.95;P<0.001] and the need not to cravesugar [t=2.65; P<0.05]. The femalecompared with the male adoleseentsscored higher for the importance ofweight gain [t=2.00; P<0.05].
In the 'exclusion of sugar from teaand coffee' group no significant differ-ences in mean scores for any of the be-liefs could be demonstrated between themale and female adolescents. However,the females had significantly higherscores for the outcome evaluations - theimportance of preventing spots [t=2.20;P<0.05], the importanee of preventingtooth decay [t=4,47; P<0.00\] and theimportance of heart disease [t=2,65;

Decision-tnaking processes for sugar consumption 231
Table 2. Stepwise regression analysis results: the addition (Intention 1) and exclusion (Inten-tion 2) of sugar in tea and coffee as dependent variables; knowledge, attitudes and behavioursas independent explanatory variables
Beta coefticient t
Explanatory variables for Intention 1 -the addition of sugar to tea and coffee
Total attitude seore 0.04 2.45*Toothbrushing behaviour 0.85 3.00**Regularity of dental attendance 0.10 2.11*
R- = 0.26
Explanatory variables for Intention 2 -the exclusion of sugar from tea and coffee
Regularity of dental attendanceDental health knowledge
-0.370.64
-5.61***5.26***
R-=0.05
* = F<0,05.**=0.01>P<0.05.
***=P<0.001.
Table 3. Correlation coefficients with intention to add sugar to tea and coffee (Intention 1)and intention to exclude sugar from tea and coffee (Intention 2)
Correlations F
Correlations for Intention 1 -addition of sugar to tea and coffee
Intention 1 with total attitudeIntention 1 with total subjective normIntention 1 with toothbrushingIntention I with dental attendanceIntention I with dental health knowledgeIntention 1 with felt treatment needIntention I with appearance of teethIntention 1 with state of gumsToothbrushing behaviour with dental attendanceToothbrushing behaviour with felt need for treatment
Correlations for Intention 2 -exclusion of sugar from tea and coffee
Intention 2 with total attitudeIntention 2 with total subjective normIntention 2 with toothhrushingIntention 2 with dental attendanceIntention 2 with dental health knowledgeIntention 2 with felt treatment uccdIntention 2 with appearance of teethIntention 2 with state of gumsToothbrushing behaviour with denial health knowledgeDental attendance with appearance of teeth
0.250.020.290.250.050.010.120.040.200.23
0.030.070.210.240.230.110.130.020.240.31
<0.05>0.05<0.05<0.05>0.05>0.05>0.05>0.05<0.05<0.05
>0.05>0.05<0.05<0.05<0.05>0.05>0.05>0.05<0.05<0.01
P<0.05]. The male pupils had highermean scores compared with females forthe outcome evaluation - the import-ance of craving sugar [t=2.47; /'<0.05].
Discussion
The theory of reasoned action (1) al-lows complex behaviours to be studiedby identifying and describing beha-vioural intentions which are identifiable
as a single behaviour. The aim of thisstudy was to examine the decision-making processes adolescents undergowhen making sound food choices. It isimportant, when considering decision-making processes, to examine a behav-iour which is distinct, well defined andhas the same target as that of the inten-tion being investigated. The intentionand its associated behaviour must beperformed within a short time period ofassessment (1). The behavioural inten-
tion chosen for prediction was the deci-sion to use sucrose in hot drinks.
The decision to examine two behav-ioural intentions - the intention to addsugar to tea and coffee and the inten-tion to exclude sugar from tea and cof-fee - arose from the in-depth interviews.It seemed that the behavioural complexunder examination - the use of sucrosein hot drinks - was well defined by twosingle actions, that is, the addition andthe exclusion of sugar in tea and coffee.Comparing two groups of subjects isthe recommended method to explainchoice as presented in this paper, wherethe two groups compared are one groupwith a relatively strong intention to addsugar to coffee and tea and one groupwith a relatively strong intention to ex-clude sugar from coffee and tea. In ad-dition, the intention to add sugar tocoffee and tea and the intention to ex-clude sugar from coffee and tea may beviewed as the choice between perform-ing or not performing the behaviouralintention.
It was interesting therefore that fac-tors associated with dental healthknowledge, attitudes and behaviourswere the main predictors of both of thebehavioural intentions to add or to ex-clude sugar in tea and coffee. The asso-ciated behaviours of dental attendanceand toothbrushing behaviours were im-portant in the predictions of the behav-ioural intentions. Although equivalentvariables predicted the addition or ex-clusion of sugar in tea and coffee, thedirection of their infiuence differed. Theregularity of dental attendance pre-dicted adding sugar to hot drinks whilstirregularity of dental attendance pre-dicted exclusion. For the 'addition ofsugar' group, regularity of dental atten-dance was positively related to the in-tention and with toothbrushing where-as toothbrushing was negatively relatedto the intention and felt need for dentaltreatment. For the 'exclusion' group,dental attendance was negatively associ-ated with the intention and feeling goodabout the appearance of one's teethwhereas toothbrushing was positivelyrelated to the intention and to dentalhealth knowledge about sugar and den-tal caries. Behavioural infiuencesseemed to act in opposing directionswith respect to decision-making, withsimilar correlations of dental health be-haviours existing for both the addition

232 FREEMAN & SHEIHAM
and the exclusion of sugar groups. Forthose who continue to take sugar in hotdrinks there is a reliance upon the den-tal profession to care for their dentalhealth. For those who make the deci-sion to exclude sugar there is an aware-ness of self-reliance (10, 11), with dentalhealth information being convertedinto action and preventive behavioursused to promote dental health.
The 'addition of sugar' group wasmore reliant on parental figures as re-flected in the finding that their parentsacted as more important referents forthis behavioural intention than those inthe 'exclusion of sugar' group. Thisfinding differs from RISE & H0LUND'S(5), They highlighted the importance ofpeer groups as referents in the predic-tion of sugar consumption. However,their finding that 'there is a symbolicfunetion of [sugar] consumption' isstrongly supported in the present studysince the most salient attitude, for all,was the sweet, pleasant taste of sugar.The idea that decision-making with re-speet to sugar intake may be influencedby the immediate pleasure of tastingsugar, and such deferred dangers asdental earies or heart disease, is high-lighted by the differences between maleand female adolescents irrespective ofbehavioural intention. For the tnales, itwas the need for the pleasure of sugarand with it the belief that sugar pro-vided energy. For females, the beliefsconcerning weight control and the pre-vention of dental caries and heartdisease prevailed (12), Such findings asthese may suggest that differential be-
liefs and attitudes may be more appro-priate in this ehoice situation than areseparate measures of these individualvariables with respect to eaeh behav-ioural option.
This study shows that decision-making to consume sugar in adoles-ceiiee is eomplex. There are the immedi-ate pleasures as well as the realisation ofdeferred dangers associated with sugarconsumption. There are influences ofpast dental behaviours, dental healtheducation and parental figures, such asthe dentist, who can be made responsi-ble for dental health after sugar is con-sumed. Furthermore, differences existin the underlying cognitive structuresbetween those adolescents who haveand have not decided to exclude sucrosefrom their hot drinks. Those adoles-cents who do so appear to have the abil-ity to convert dental health informationinto action by praetising preventivehealth behaviours. Dental health pro-fessionals involved in dental health edu-cation and promotion should be awareof the complex nature of decision-making proeesses when negotiatinghealth goals with adolescents (13),
References
1. AJZEN I, FISHDEIN M . Understanding at-
titudes and predicting social behaviour.Englewood-Cliff; N J Prentice-Hall Inc.,1980.
2. YuDKiN J. Nutrition and palatabilitywith special reference to obesity, myocar-dial infarction and other diseases of civi-lisation. Laticet 1963; /.• 1335-8.
3. BARIC L, BLINKHORN AS, MACARTHURC. A health education approach to nut-
rition and dental health education.Health Educ J 1974; 33: 79-90.
4. BIRCH LL. The relationship betweenchildren's food preferences and those oftheir parents. J Nutr Educ 1980; 1: 14-8.
5. RISE J, HOLUND U. Prediction of sugarbehaviour. Community Dent Health1990; 7: 267-72.
6. DEPARTMENT OF HEALTH. COMMITTEE ONTHLI MEDICAL ASPECTS OF FOOD POLICY.Report of the panel on dietary sugarsand human disease. No 37. London:HMSO, 1989.
7. KINIRONS M,I, BEATTIE G , STEELE PA,The pattern of sugar consumption in so-cial class groups of young adolescents inNorthern Ireland. Gotnniimity DetitHealth 1992; 9: 329-33.
8. FREEMAN R, MAIZELS J, WYLIE M , SHEI-HAM A. The relationship between dentalheallh related knowledge, attitudes anddental health behaviour in 14 to 16-yeai-old adolescents. Cotntminity Dent Hecdth1993; 10: 397^04.
9. S0GAARD AJ. Theories and models ofhealth behaviour. In: SHOU L, BLINK-HORN AS, eds. Orcd hecdth promotion.Oxford: Oxford Medical Publications,1993.
10. MESTERS I, OosTVEEN T. Wily do adoles-cents eat low nutrient snacks betweenmeals? An analysis of behavioural deter-minants with the Fishbein and Ajzenmodel. Nutr Health 1994; 10: 33-47.
11. PATTISON K, FREEMAN R , KUUSELA S,HONKALA E. Adolescents' sugar choicesin Belfast and Kuopio. / Inst HecdthEduc 1996; 34: 75-9.
12. AsTR0M AN, RISE J. Expectancy-valueapproach to drinking of non-sugarymineral water among adolescents. Com-tniinity Dent Oral Epidetniol 1996; 24:72-8.
13. TONES K, TILFORD S, ROBINSON Y.Health eare contexts. In: Health educa-tion effectiveness and effieieticy. London:Chapman and Hall, 1993.