Embed Size (px)
Citation preview
Understanding and Responding to the Role of Mental Health
Diagnoses in Challenging Behavior
Melissa Cheplic, MPH, CHESThe Boggs Center on Developmental Disabilities
Theodosia Paclawskyj, Ph.D., BCBA-D, NADD-CCKennedy Krieger Institute and The Johns Hopkins University
of Medicine
Intellectual Disability
Psychiatric Diagnosis
Dual Diagnosis
Intellectual Disability
Challenging Behavior
Psychiatric Diagnosis
An Additional Challenge
ID and Mental Health and Problem
Behavior • 30-35% of all persons with intellectual or developmental
disabilities have a psychiatric disorder (NADD, 2013)
• 10-20% have challenging behavior (self-injury, aggression, destructive behavior) severe enough to impair daily life (Lundqvist, 2013)
• Statistics vary on how many have both; however,
• Challenging behaviors increase the probability of almost all psychiatric disorders (Rojahn, Matson, Naglieri, & Mayville, 2004)
• General psychopathology highly correlated with challenging behaviors (Myrbakk & von Tetzchner, 2008)
• Challenging behavior the number one barrier to
community living, relationships, employment, and
staff retention
What does this mean for the people we support and their
quality of life?
What does this mean for us in our every day work and
practice?
Setting Events
• Events and circumstances that predict likelihood of problem behavior
• Make behavior more likely or less likely at a later time by changing the importance/impact of that maintaining consequence
• ABA: Conditions in the environment that can alter the strength of reinforcers (Motivating Operations)
• Can be internal or external/environmental events
Problem Behavior: Hitting
Others
In what context does it occur?
Problem Behavior: Hitting
Others
Depression“I just want to be left alone”“I don’t want to do anything”“I feel sad and angry”
Problem Behavior: Hitting
Others
Anxiety“I’m scared of this”“I don’t want to be here”“I can’t do this”
Problem Behavior: Hitting
Others
ADHD“I can’t focus”“I need to move around”“I didn’t hear the instructions”
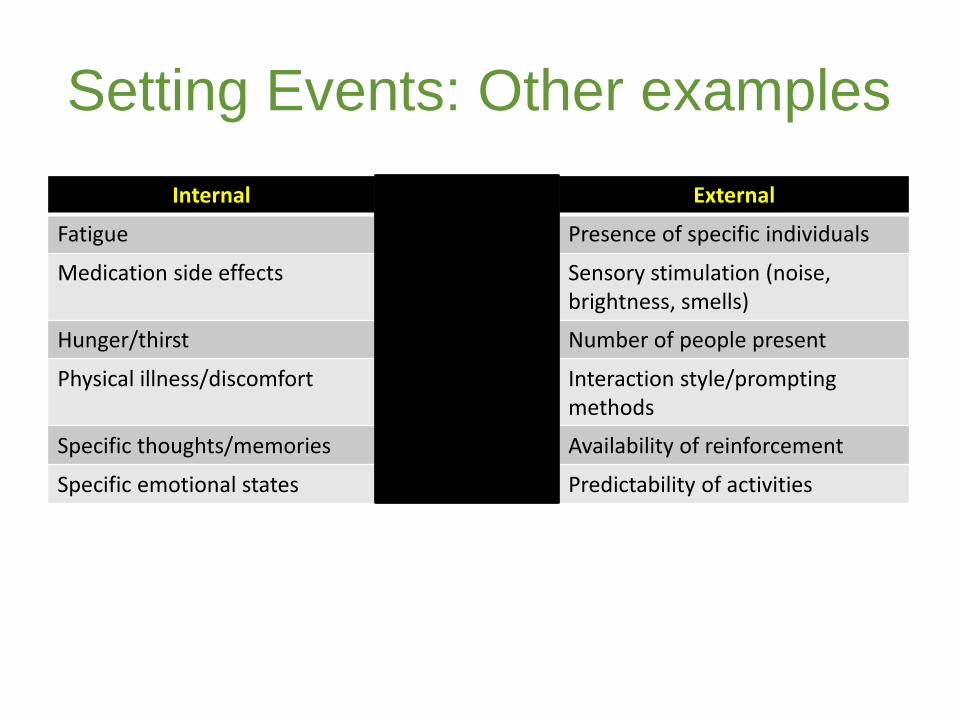
Setting Events: Other examples
Internal External
Fatigue Presence of specific individuals
Medication side effects Sensory stimulation (noise, brightness, smells)
Hunger/thirst Number of people present
Physical illness/discomfort Interaction style/prompting methods
Specific thoughts/memories Availability of reinforcement
Specific emotional states Predictability of activities
Understanding Setting Events
• Ask what symptoms of a psychiatric disorder are exhibited by that specific person
– What should you look for to know that (s)he has a ___________________ disorder?
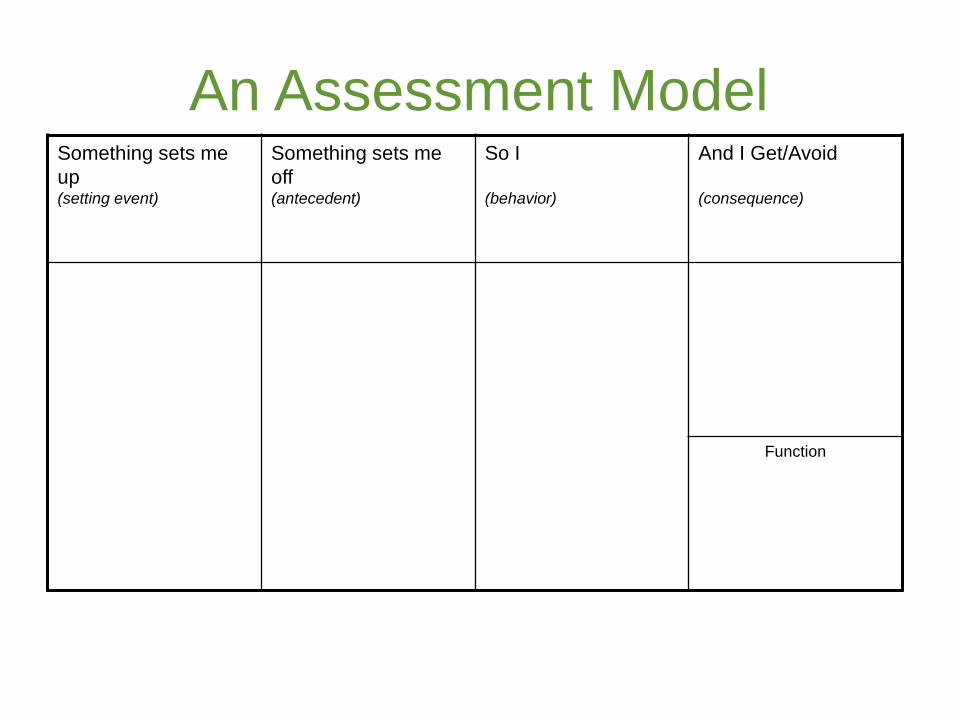
An Assessment ModelSomething sets me
up (setting event)
Something sets me
off (antecedent)
So I
(behavior)
And I Get/Avoid
(consequence)
Function
Elements of the Assessment
Model1. Something Sets Me Up: Also called the setting event
Examples: boredom, illness, stress, exhaustion, anxiety, depression…
2. Something Sets Me Off : Also called the trigger/antecedent
Examples: requests, told “no,” rude comment, target for teasing…
3. So I: Engage in the behavior
Examples: hit, kick, withdraw, yell, headbang, curse, cry, …
4. And I Get/Avoid: The “pay-off”/reinforcer
Examples: Attention, drama, to be alone, an object, an activity, fun, relief…
Setting events:
• Also called “slow triggers”
• “Motivating Operations” in ABA terminology
• “The things that set me up to (have a challenging behavior”
• Characteristics
• May occur hours, even days before the behavior
• May be a longstanding condition
• Doesn’t cause the behavior, but makes a behavior more likely
• Something that makes the consequence either more or less reinforcing
Some common Setting Events
16
Physical
• Pain or illness
• Physical conditions
(e.g., seizures, allergies)
• Disrupted sleep
Learning and self-
regulation
• Atypical sensory needs
• Specific disability
• Short attention span
Social-emotional
• Psychiatric illness
• Agitated or depressed
• Unusual disappointment
• Negative interaction
Environment and routines
• New schedule or setting
• Different caregiver
• Change in season or
weather

Antecedents:
• Also called
“immediate” or
“fast triggers”
• Discriminative
stimulus (SD)
17
• Characteristics
• Happen right before
the behavior
• Can predict behavior
(likely to occur when
this happens)
Common Antecedents
18
• Told to do a task
• Failure to complete task
• Reprimanded/redirected
• Presence of a person
• Target of aggression
• Being ignored/alone
• Transition from one activity
to another
• End of an interaction
• Told “no”
• End of pleasant activity
• Told to wait
• Teased – called a name
• Specific internal
need/feeling
The Function of Behavior Behaviors may persist because the individual…
• Enjoys the sensory experience – it feels better, satisfies a need or impulse (internal triggers, internal rewards)
• Experiences a decrease in an unpleasant state (e.g., decreased anger, anxiety, pain)
• Escapes or avoids demands or things he or she doesn't like to do
• Gains attention/a reaction from others
• Obtains tangible items or opportunities or access to something preferred
Mental Health Diagnoses as
Setting Events
• An individual with an anxiety disorder may experience typical life events as more anxiety provoking
• May feel very anxious around a typically neutral stimulus
• (Escape or attention/reassurance become more reinforcing)
• Individual with depression may lack motivation or interest
• They no longer engage in known tasks or activities
• (Escape from demands and/or interaction become more reinforcing)
Mood Disorders: Possible Setting
Events
• Depression: sadness, irritability, fatigue, restlessness,
loss/gain of appetite
• Lack of motivation or interest may lead to refusal,
“noncompliance”
• Might engage in challenging behavior to alleviate
unpleasant emotions
• Might engage in challenging behavior to avoid social
interaction, social activities, meals, etc.
• May engage in food-stealing or food avoidance
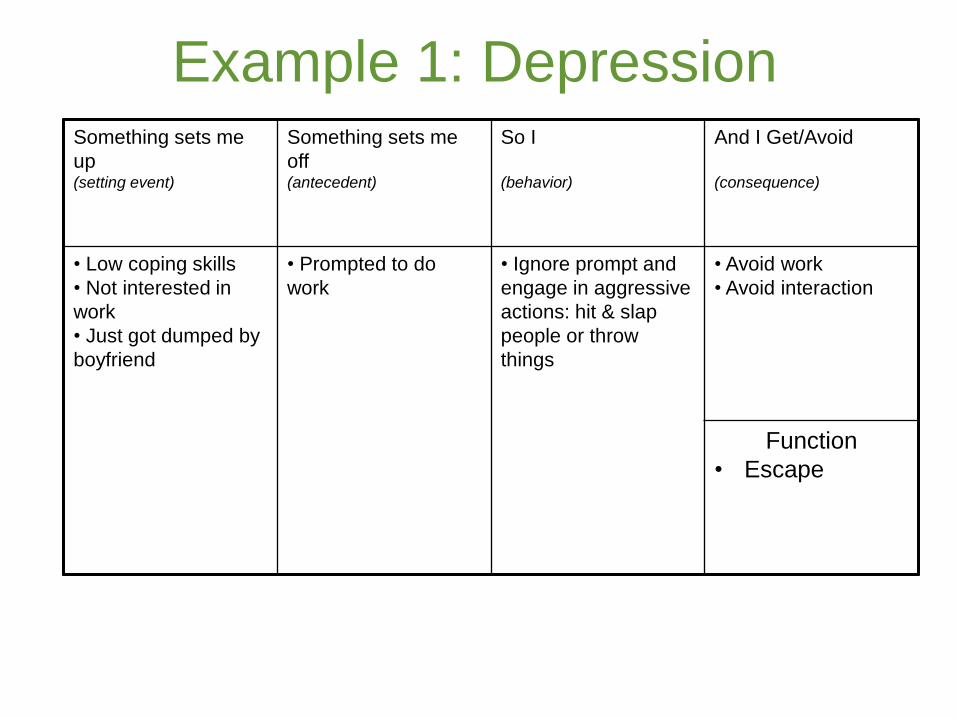
Example 1: DepressionSomething sets me
up (setting event)
Something sets me
off (antecedent)
So I
(behavior)
And I Get/Avoid
(consequence)
• Low coping skills
• Not interested in
work
• Just got dumped by
boyfriend
• Prompted to do
work
• Ignore prompt and
engage in aggressive
actions: hit & slap
people or throw
things
• Avoid work
• Avoid interaction
Function
• Escape
Anxiety Disorders
• Conditions characterized by extreme, chronic anxiety that disturbs mood, thought, behavior and/or physiological activity
• Wide variety of anxiety disorders • Generalized Anxiety Disorder
• Obsessive-Compulsive Disorder
• Panic Disorder
• Agoraphobia and Specific Phobias
• Social Anxiety Disorder
• Post Traumatic Stress Disorder
Anxiety Disorders: Possible Setting
Events
• Fear, irritability, restlessness, fatigue/muscle tension,
distractibility
• Engage in challenging behaviors to avoid people or things
that cause anxiety
• Intentionally misbehave or “get in trouble” to stay at home,
miss work, miss activity
• Become desperate to access item or source of obsessions
• May engage in self-injury to alleviate unpleasant emotions
• High level of agitation and tantrums with difficulty in
calming (fight or flight response)
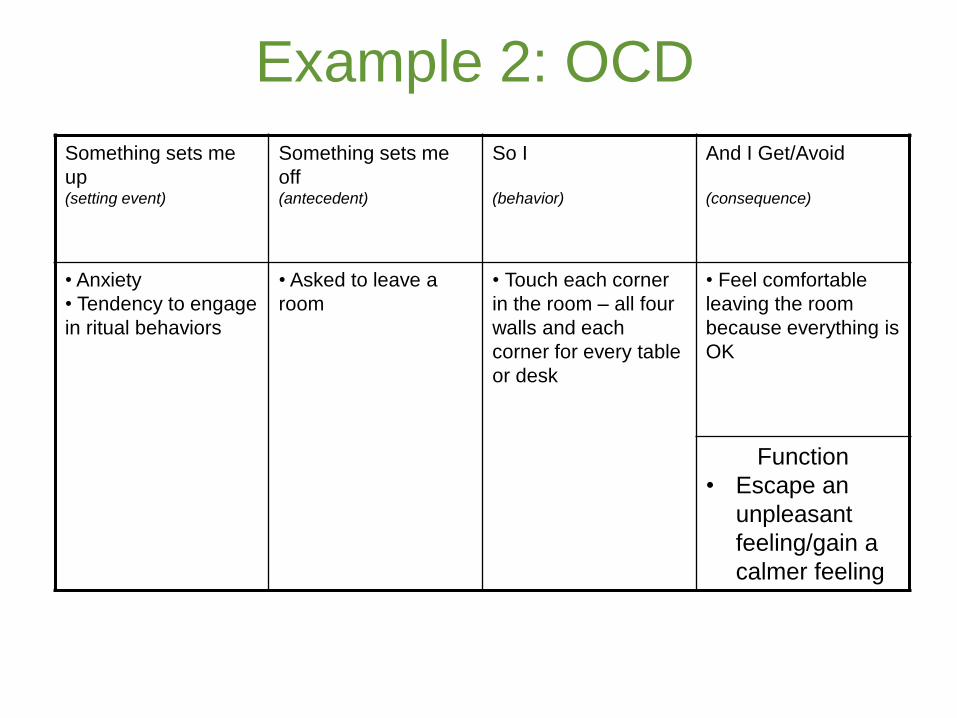
Example 2: OCD
Something sets me
up (setting event)
Something sets me
off (antecedent)
So I
(behavior)
And I Get/Avoid
(consequence)
• Anxiety
• Tendency to engage
in ritual behaviors
• Asked to leave a
room
• Touch each corner
in the room – all four
walls and each
corner for every table
or desk
• Feel comfortable
leaving the room
because everything is
OK
Function
• Escape an
unpleasant
feeling/gain a
calmer feeling
Psychotic Disorders/Schizophrenia
• Onset – late teenage years to early 20’s typical
• Characteristics:• Loss of contact with reality
• Deterioration of normal social functioning
• Symptoms:• Hallucinations
• Delusional beliefs
• Personality changes
• Disorganized thinking or speech
• Unusual or bizarre behavior
• Doesn’t trust others, isolated
• Impairment carrying out the activities of daily living
• Odd sensory experiences, rituals
Psychotic Disorders: Possible
Setting Events
• Paranoia, distorted thinking, loss of skills, distorted
sensory perceptions
• Avoid places or things that they find threatening
• Respond to stimuli only recognizable to them
• May misperceive neutral events as threatening
• Don’t respond to typical consequences for challenging behaviors
Borderline Personality Disorder
• A serious mental illness • Pervasive instability in moods, relationships, self-
image, and behavior
• Intense bouts of anger, depression and anxiety, may last only hours
• May exhibit brief psychotic episodes
• Tend to develop intense, dependent, hostile, unstable and manipulative relationships with peers, therapists and others• Their instability often disrupts family and work life,
long-term planning, and sense of self-identity
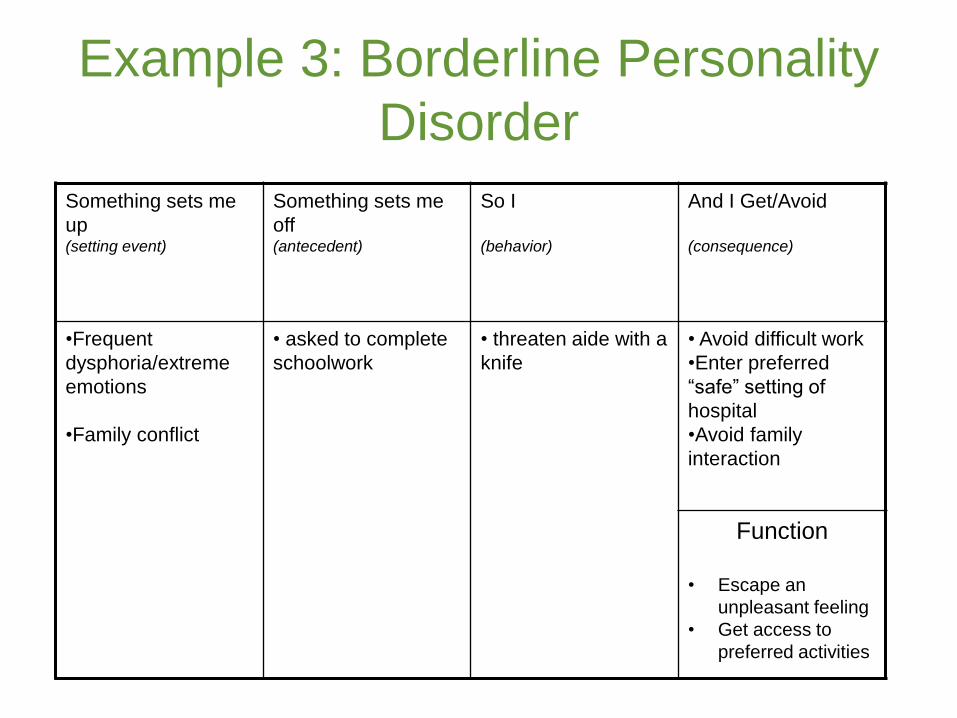
Example 3: Borderline Personality
Disorder
Something sets me
up (setting event)
Something sets me
off (antecedent)
So I
(behavior)
And I Get/Avoid
(consequence)
•Frequent
dysphoria/extreme
emotions
•Family conflict
• asked to complete
schoolwork
• threaten aide with a
knife
• Avoid difficult work
•Enter preferred
“safe” setting of
hospital
•Avoid family
interaction
Function
• Escape an
unpleasant feeling
• Get access to
preferred activities
Responding to Behaviors
• ABA historically focused on consequences for behavior
• Functional assessment allows for individualized treatment targeting specific triggers and consequences for a specific person
• Antecedent management strategies increasing in the past decade
REACTIVE PROACTIVE
• Decrease likelihood of challenging behavior by decreasing negative impact of setting events
Strategies for Prevention and
Antecedent Intervention
• Avoid the trigger• Distract the person when a trigger occurs (or even better,
just before)• Reduce or remove demands • Offer alternate places to perform tasks
• Provide extra staff attention – without a request (noncontingent attention)
• Anticipate and meet needs before problems start • Talking to the person before they get bored, providing a
snack or nap
• Take breaks – walks, movement, music
31
Supporting Long-Term Change: Teach
New Skills/Replacement
• Teach flexibility - ways to make needed variations in the routine
• Choice making
• Social skills: conversation, following directions, asking a question, asking for a break
• Understanding social expectations/use social narratives
• Self control, self-regulation, anger management, relaxation skills
• Replace: use new skills to meet the needs of the old behavior
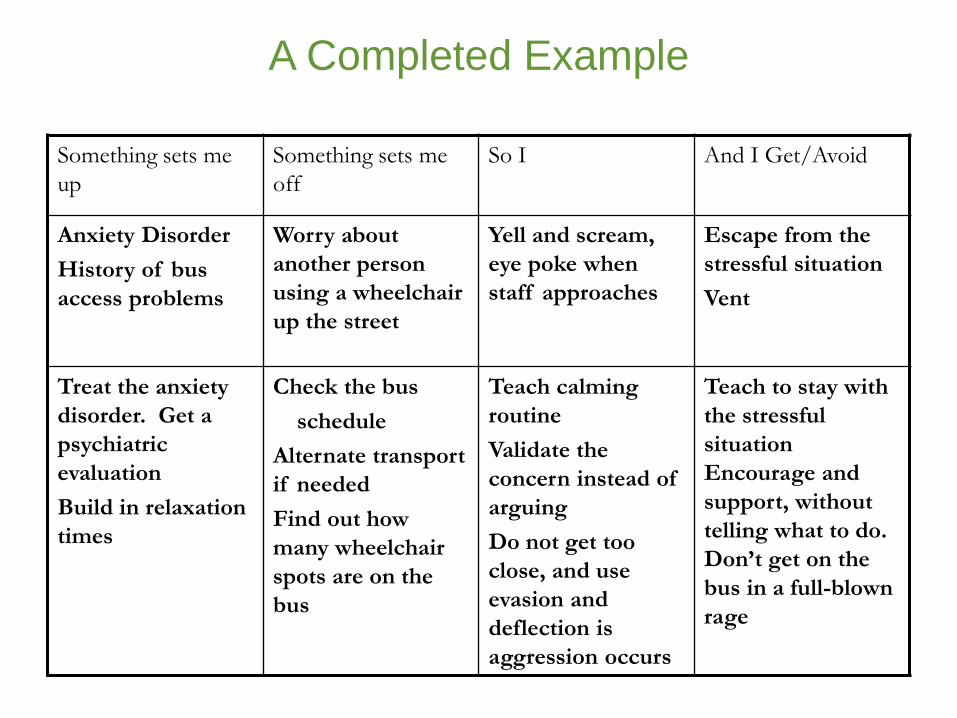
A Completed Example
Something sets me
up
Something sets me
off
So I And I Get/Avoid
Anxiety Disorder
History of bus
access problems
Worry about
another person
using a wheelchair
up the street
Yell and scream,
eye poke when
staff approaches
Escape from the
stressful situation
Vent
Treat the anxiety
disorder. Get a
psychiatric
evaluation
Build in relaxation
times
Check the bus
schedule
Alternate transport
if needed
Find out how
many wheelchair
spots are on the
bus
Teach calming
routine
Validate the
concern instead of
arguing
Do not get too
close, and use
evasion and
deflection is
aggression occurs
Teach to stay with
the stressful
situation
Encourage and
support, without
telling what to do.
Don’t get on the
bus in a full-blown
rage
Thank you for joining us
Melissa Cheplic, MPH, CHES.
Community Positive Behavior Support
The Boggs Center on Developmental Disabilities
Rutgers Robert Wood Johnson Medical School
Department of Pediatrics
Dosia Paclawskyj, Ph.D., BCBA-D, NADD-CC
Behavioral Psychology, Kennedy Krieger Institute
Assistant Professor
Department of Psychiatry and Behavioral Sciences
The Johns Hopkins University School of Medicine