Embed Size (px)
Citation preview

k. J. Med. Sc., VoL 168, No. 4 Underreporting of adverse drug reactions 2 5 7 October, November, December, 1999
Underreporting of Adverse Drug Reactions" Attitudes of Irish Doctors D. Will iams*, J. Feely
Department of Pharmacology and Therapeutics, Trinity Centre for Health Sciences, St. James's Hospital, Dublin 8.
S u m m a r y Despite the fundamenta l importance of reporting of suspected adverse drug reactions, less than
10 per cent of serious adverse drug reactions are reported. To further enhance our unders tanding of doctors' knowledge and attitudes to the current Adverse Drug React ion (ADR) report ing scheme we surveyed 158 doctors, including some 106 general pract i t ioners and 23 hospi ta l -based doctors . The response rate was 39.5 per cent. The majority had experience of reporting an ADR. Seriousness of the A D R appears to be the mos t important reason for reporting. Uncerta inty that the adverse drug react ion was definitely caused by the medicine, that the adverse drug react ion was too trivial to report or that it was too well k n o w n a reaction to report are c o m m o n reasons for not reporting. Of concern 84 per cent of doctors are unaware of the criteria of the Nat ional Drug Regulatory Agency indicat ing the need for addit ional educat ion and informat ion in this regard.
We also found considerable disagreements in doctors' understanding of the mean ing of c o m m o n , occas ional , rare, or very rare as applied to ADRs.
Introduct ion The thalidomide disaster had profound effects on the
development of new drugs, the pharmaceutical industry, and professional and public attitudes to drug safety. Despite attempts to improve the pre-marketing evaluation of new drugs, issues of safety continue to result in drug withdrawal. When a new active substance is introduced into clinical practice, experience of its effects in humans is limited. Whilst there may be confidence in the efficacy of the new drug at the time of its introduction, conclusions about its safety must remain provisional. With wider clinical experience it is possible to identify less common adverse drug reactions in different patient populations or during long-term exposure. The spontaneous reporting of adverse drug reactions (ADRs) is thus a fundamental safety net to l imit toxic i ty of marke ted medic ines . However, a problem is that less than 10 per cent of all serious and 2-4 per cent of non-serious adverse reactions are reported 1. In 1997 the regulatory authority, the Irish Medicines Board, received only 1,175 reports (35 per cent from General Practitioners, 12 per cent from hospital doctors) 2 and yet some 20 million prescription items are dispensed each yr in the General Medical Service 3 (which excludes hospital and private practice). One would expect a higher rate of reporting. In a previous study we found that spontaneous ADRs were reported in less than 1 in 500 in hosp i t a l i sed pat ients whilst more in tens ive moni tor ing involv ing review of pat ient records and collection of reports from both doctors and nurses revealed a 10 per cent occurrence 4.
To further enhance our understanding of doctors ' knowledge of the current ADR reporting scheme and whether there was any difference between doctors in hospital practice or general practice, we carried out an attitudinal survey and also recorded doctors' responses to hypothetical ADR situations.
Methods The questionnaire (Appendix A) was posted to 400
doctors drawn at random from the 1997 Irish Register of Medical Practitioners with a stamped, addressed envelope to facilitate reply. The questionnaire included information on whether the respondent ever previously diagnosed or reported an ADR. Factors discouraging reporting were also sought , as were r e s p o n s e s to ' h y p o t h e t i c a l ' A D R situations. We also quantified doctors' perceptions of ADR incidence terminology. The questionnaire was designed in such a way that respondents should have answered each part of each question. However, where respondents had answered individual questions incompletely they were removed from the analysis of that question only. A paired Chi-squared statistic was determined for a number of questions to quantify a difference in the responses between general practitioners and hospital doctors.
Results A total of 158 doctors (39.5 per cent) responded of
which 106 were in general practice and 23 were in hospital practice. The majority of doctors (87 per cent) were aged between 30 and 60 years of age.
Some 70 per cent of doctors had ever reported an ADR some time in their professional lifetime. This was higher amongst general practitioners (74 per cent) than amongst hospital doctors (50 per cent) (p<0.001). Of interest in the last 5 yr almost an equal number of doctors had reported ADRs to the pharmaceutical manufacturer (47/ 33 per cent) as to the national reporting agency (56/37 per cent). Some 90 per cent of doctors had encountered adverse drug reactions (ever diagnosed an ADR) but had not repor ted them. The pr inc ipa l reasons that discouraged ADR reporting are shown in Table I. Some 23 per cent of doctors did not know how to report an ADR and many felt that the system was too

258 Williams & Feely h-.J. Med. Sc.,Vol. 168, No. 4 October, November, December, 1999
TABLE 1 Reasons for not reporting an Adverse Drug Reaction (*p<0.05)
Reason for not reporting adverse drug reaction % of respondents
% of Total % of GPs % of Hospital Doctors
Uncertain that the reaction is definitely caused by the drug
Adverse Drug Reaction considered too trivial to report
Adverse Drug Reaction considered too well known to report Unaware of the existence of a national ADR reporting scheme
Unaware of the need to report an ADR Lack of knowledge on how to report an ADR Reporting an ADR too bureaucratic a process
Too busy to report an ADR
Concern that ADR reports may be used in a legal case for damages by the patient
72.9 72.8 73.9
69.7 71.3 61.9
85 84.6 95.2 10.9 7. l* 22.7*
13.9 11.9 27.3 22.7 22.5 22.7 43 46.3 36.8
34.7 31.3 47.6 5.7 7.22 0
bureaucratic or that they were too busy to report the reaction (Table I).
The question regarding adverse drug reactions as too trivial or already well known was tested by a series of hypothetical adverse drug reaction situations. Relatively few practitioners would report weight loss in a 44-yr old patient 8 weeks after starting a selective serotonin re- up t ake i n h i b i t o r a n t i d e p r e s s a n t (12 per cent) , a m o r b i l l i f o r m rash with a m o x y c i l l i n (21 per cent) , hypoglycaemic coma requiring hospitalisation in a well controlled insulin dependent diabetic (18 per cent) or swollen ankles associated with a calcium channel blocker (10 per cent). On the other hand more serious adverse drug react ions would be repor ted including deep venous thrombosis in a patient on the contraceptive pill (73 per cent), agranulocytosis in a patient taking spironolactone (70 per cent), angioedema one day after starting an ACE inhibitor (74 per cent), or sudden unexpected death in a patient 10 days after starting a new antipsychotic drug (88 per cent).
Doctors were asked if they were aware of the criteria of the National Drug Regulatory Agency specifying which adverse drug reactions should be reported and only 16 per cent were aware of these criteria. The majority (77 per cent) of doctors would be willing to report an ADR for a medicine prescribed for their patient by another physician and a similar number if the patient had purchased the medicine without prescription themselves.
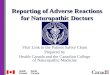
Figure 1 shows doctors understanding of expressions used to describe the frequency of adverse drug reactions. There is considerable overlap in doctors ' perceptions of occasional , rare, common or very rare adverse drug reac t ions . For e x a m p l e 1 in 1000 was cons ide red occasional by 56 per cent, rare by 19 per cent and common by 6 per cent.
Discuss ion Our finding that 70 per cent of doctors had ever reported
an ADR is similar to the reporting rate in many other EU
member states including Britain 5. It is clear that the majority of doctors encounter ADRs but only one third have reported such to the regulatory agency in the last 5 yr. The extent of underreporting is difficult to quantify but must be considerable as there is less than one ADR report per 36,000 GMS prescriptions and one per 3000 prescriptions (given that most hospitalised patients receive on average 6 medications and ADRs are reported in less than 1 in 500) in a general hospital 4. We found little difference between general practi t ioners and hospital based doctors apart f rom more general pract i t ioners reporting an ADR but this is in part explained by the g rea te r e x p e r i e n c e and mean age of the gene ra l practitioners. This is in keeping with a previous survey carried out in Ireland 6. In common with many such surveys the response rate (40 per cent) raises the question as to the validity of our sampling. Previous surveys have ident i f ied d i f f i cu l t i e s in loca t ing y o u n g e r doctors particularly when using the Medical Register allied to the fact that over a quarter of doctors registered are not in practice in Ireland 6. Also because of the temporary nature of posi t ions a poorer response f rom non-consul tan t hospital doctors is not unexpected. It was surprising to note that whilst more general practitioner have reported an ADR, they were less aware (10 per cent versus 24 per cent) of any criteria from the National Regulatory Agency for report ing ADRs as compared with their hospital colleagues.
We were somewhat surprised at the extent to which doc to r s were r e p o r t i n g ADRs to p h a r m a c e u t i c a l manufacturers. As the regulatory authority advises sending such reports directly to them it is possible that some of this reporting is by way of mention to a pharmaceutical representative which may not indicate a formal report.
Table I lists the main issues that discourage reporting. Uncertainty that the reaction was definitely caused by the medicine was a common view and appears to be the case internationally. There was no s igni f icant d i f ference between hospital doctors and general practitioners in this

Ix. J. Med. Sc., Vol. 168, No. 4 Underreporting of adverse drug reactions 2 5 9 October, November, December, 1999
regard. Also of note, adverse drug reactions considered too trivial to report and adverse reactions too well known to report are common reason for not reporting. In the hypothetical ADRs that we put by way of example to the doctors it was clear that this differentiation was present. This runs cont rary to the requi rements of the Irish Medicines Board who request reports on all ADRs 7. It appears that the response of Irish doctors is more in keeping with the requirements of the UK Committee for Safety of Medic ines , which does not encourage the reporting of trivial or well-known ADRs.
The single most important reason for reporting an ADR appears to be the seriousness of the reaction and this appears to be the case in ternat ional l / ' t Too busy to report an ADR, lack of knowledge on how to report an ADR (2 of the ' seven deadly sins ' discouraging reporting as described by Inman) and a reporting process that is too bureaucratic were other advanced reasons for not reporting adverse drug reactions. Of some concern is that some 23 per cent of doctors do not know how to report an ADR and taken in conjunction with the finding that some 84 per cent are unaware of the reporting criteria of the National Drug Regulatory Agency it does suggest that additional information and e~ducation is required in this regard. The regulatory authority needs to be more explicit
in its requirements and increase knowledge of the adverse drug reaction reporting system in order to stimulate a 'reporting culture'.
Recently, fenf luramine and dexfeni luramine were withdrawn from the marke t fol lowing concerns of a possible association between the occurrence of valvular heart disease with the use of these anorectic agents ~. In addition other new drugs associated with unexpected major adverse effects have included Mibefradil and Terfenadine. M e b e f r a d i l , a c a l c i u m - c h a n n e l a n t a g o n i s t tha t is metabolised by the hepatic enzyme CYPA4, proved toxic in patients prescribed other drugs that are metabolised by CYPA4, such as the macrolide antibiotic erythromycin, prompting its removal from the market. Serious toxic effects - torsade de points and ventricular tachycardia - were found to be a s soc i a t ed with t e r f e n a d i n e , an ant ihis tamine which is also metabol i sed by CYPA4. However this problem was not recognised until terfenadine had been on the market for 5 yr and had been taken by a significant number of patients.
It may be a poor reflection on society 's attitude to preventative measures that drug safety only became a priority following thalidomide and in Ireland is foremost following the recent hepatitis C contamination of blood products. No independent agency as such exists with the
Figure 1 - Doctors ' understanding of expres s ionsused to describe the frequency of ADRs

260 W i l l i a m s & F e e l y It. J. Med. Sc., Vol. 168, No. 4 October. November, December, 1999
respons ib i l i ty to moni to r and inves t iga te adverse events due to drugs and to p rov ide r ecommenda t ions to prevent them. A recent p roposa l has sugges ted that respons ib i l i ty for d rug s a f e t y s h o u l d be v e s t e d in an i n d e p e n d e n t au tho r i t y 9. Such i n d e p e n d e n c e w o u l d he lp to ensure objec t iv i ty and avoid confl ic ts of interest .
U n f o r t u n a t e l y , p r e v i o u s i n t e r v e n t i o n s to i m p r o v e repor t ing rates ( inc luding verbal reminders , using a fee and inc reas ing the avai lab i l i ty o f ye l l ow cards) are only shor t - l ived 4,~~ It would appear that the present repor t ing sys tem is inadequate . The present r epor t ing sys tem could be improved by using te lephone /e lec t ron ic -mai l facil i t ies. W i t h t he a d v e n t o f p h a r m a c o v i g i l e n c e n u r s e s in h a e m a t o l o g y , i t m a y we l l be a p p r o p r i a t e to a p p o i n t p e r s o n n e l w i t h e x p e r t i s e in p h a r m a c o v i g i l e n c e to hosp i ta l s . E x t e n d i n g the range o f pe r sonne l who may report A D R s by inc luding nursing s taff may also improve repor t ing rates . We have p rev ious ly shown that nurses repor ted more A D R s compared with doctors over a s imilar t i m e - p e r i o d u. G i v e n t h e i r u n i q u e p o s i t i o n in d r u g admin i s t r a t ion and record ing obse rva t ions on pat ients , nurses cou ld cont r ibu te s igni f icant ly to the repor t ing of adverse drug react ions .
Doc to r s ' unders tanding of express ions used to descr ibe the f r e q u e n c y o f A D R s a re o f i n t e r e s t . C o m m o n l y textbooks and da ta sheets, M I M S , B N F and the Speci f ics o f P r o d u c t C h a r a c t e r i s t i c s ( S P C or d a t a shee t ) use express ions l ike occas ional , c o m m o n or rare. Clear ly this
has a d i f fe ren t mean ing to d i f ferent peop le and as shown in F i g u r e 1 t he re is c o n s i d e r a b l e ove r l ap . I ndeed an occur rence o f I in 1,000 is regarded by some 6 per cent as common, by 56 per cent as occas iona l and another 19 per cent as rare. There is c lear ly need for an agreed def ini t ion of the m e a n i n g of these words, not a lone i f we are to in terpret the l i te ra ture in a mean ingfu l way but also to e xp r e s s to p a t i e n t s the r e l a t i v e r i sk o f adve r se drug react ions.
Wood et al 9 descr ibe the true safety prof i le of a drug as be ing d e p e n d e n t on the ' e x p e r i m e n t ' that necessa r i ly f o l l o w s a d r u g ' s r e l e a s e in to the m a r k e t p l a c e . Th i s exper imen t requi res adequate funding and moni tor ing to ensure that the re levan t data is co l lec ted and analysed and the conc lus ions rap id ly d i ssemina ted .
A c k n o w l e d g e m e n t
This s tudy was suppor ted by a grant to the European Pha r m acov ig i l ance Research Group, by the Commiss ion o f the E u r o p e a n C o m m u n i t i e s , u n d e r the B i o m e d 2 Program, con t rac t number PL 95 0467.
We w o u l d a lso l ike to a c k n o w l e d g e the a s s i s t ance provided by Dr. J. Bressan and M. Hal l in this study.
R e f e r e n c e s
1. Pirmohamed, M., Breckenridge, A., Kitteringham, N., Park, B. Fortnightly review. Adverse drug reactions. BMJ 1998; 316: 1295-1298.. Irish Medicines Board: Annual Report and Accounts 1997. General Medical Services (payments) Board Annual Report 1997.
4. Feely, J., Moriarty, S., O'Connor, P. Stimulating reporting
2. 3.
of adverse drug reactions by using a fee. BMJ 1990; 300: 22-3.
5. Belton, K. J., Lewis, S. C., Payne, S., Rawlins, M. D., Wood, S. M. Attitudinal survey of adverse drug reaction reporting by medical practitioners in the United Kingdom. British Journal of Clinical Pharmacology 1995; 39: 223-226.
6. McGettigan, P., Feely, J. Adverse Drug Reaction Reporting: Opinions and Attitudes of Medical Practitioners in Ireland. Pharmacoepidemiology and Drug Safety 1995; 4: 355-358.
7. Reporting adverse reactions Irish Medicines Board Drug Safety Newsletter - issue No. 3. p4. Jan. 1997.
8. Irish Medicines Board. Drug Safety Newsletter. October 1997: 5th edition.
9. Wood, A., Stein, C., Woosley, R. Making Medicines Safer - The Need for an independent Drug Safety Board. New England Journal of Medicine, 1998: 339.25; 1851-53.
10. McGettigan, P., Golden, J., Conroy, R., Arthur, N., Feely, J. Reporting of adverse drug reactions by hospital doctors and the response to intervention. British Journal of Clinical Pharmacology 1997; 44: 98-100.
11. Hall, M., McCormack, P., Arthurs, N., Feely, J. The spontaneous reporting of adverse drug reactions by nurses. British Journal of Clinical Pharmacology 1995; 40: 173- 175.
APPENDIX 1
1 Have you ever diagnosed an adverse drug reaction Yes No in a patient under your care? ~
2. Have you sent a report of a suspected adverse drug reaction to: Yes Yes No
(in the last (more than (never) years) 5 years ago)
The Irish Medicines Board O O [D 3 4 5
A pharmaceutical manufacturer? O El 6 7 8
3. Have you aver suspected an adverse drug reaction Yes No but not reported it ? [71
9 10
4.
(i[ "Yes" go to question 4, 4[ "No'" go to question 5)
If you have suspected, but not reported, an adverse drug reaction was it because: (tick as many as applicable)
Yes No You were uncertain that the reaction had been s IZI definitely caused by a drug? 11 12 You considered the adverse drug reaction to be too O [71 trivial to report? 13 14 You considered the adverse drug reaction to be too ~1 ID well known to report? 15 16 You were unaware of the existence of a national ~1 O adverse drug reaction reporting scheme? 17 18 You were unaware of the need to report CI El adverse drug reactions? 19 20 You did not know how to report adverse drug El El reactions? 21 22 Reporting adverse drug reactions is too bureaucratic O a process? 23 24 You do not have enough time to report adverse O O drug reactions? 25 26 You were concerned that your report could be used in CI El a legal case for damages by the patient? 27 28
Which of the following hypothetical situations would prompt you to report an adverse drug reaction? (Assume, in each case, that the patient has no other medical problems and is taking no other medicines).
Yes No Not Sure Deep vein thrombosis in a 22 year old patient three O 071 [D months after taking a combined oral contraceptive. 29 30 31 Hypoglycaemic coma, requiring hospitalisation, in a El CI 171 previously well controlled insulin dependent diabetic. 32 33 34

It'. J. Med. Sc., Vol. 168, No. 4 October, November, December, 1999
Acute pancreatitis in a 55 year old male 6 weeks after O starting treatment with a tricyclic antidepressant. 37
Agranulocytosis in a 65 year old patient who has been t3 taking spironolactone for three months. 40
Myalgia in a 40 year old patient who has been taking O a new statin (HMG CoA reductase inhibitor) for 43 6 months.
Weight loss in a 44 year old patient 8 weeks after O O O starting treatment with a new selective serotonin 44 45 46 reuptake inhibitor (SSRI) antidepressant.
A morbiliform rash in a patient 6 days after starting tD O a course of amoxycillin for a urinary tract infection. 47 48 49
Swollen ankles in a hypertensive patient who has O O been taking a calcium channel blocker for 4 months. 50 51 52
A sore tongue in a patient 2 weeks after starting O O treatment with a new antiepileptic agent. 53 54 55
Local hypertrichosis in a patient who has been El ~ using a new topical antifungal for 3 months. 56 57 58
Angiodema in a patient one day after starting treatment O O O with a new angiotensin-converting enzyme inhibitor. 59 60 61
Bronchospasm in an asthmatic patient after taking O O 1:3 one dose of a new selective beta blocker. 62 63 64
Temporary taste disturbance in a patient while O O O taking regular doses of paracetamol. 65 66 67
Dyspepsia in a patient taking loperamide ~1 O
Sudden unexpected death in a patient 10 days after starting treatment with a new antipsychotic drug.
Pseudomembranous colitis in a patient 3 weeks after starting treatment with a new proton pump inhibitor.
6. Are you aware of any criteria from the Irish Medicines Board specifying which adverse drug reactions you should report.
7. Would you report an adverse drug reaction if: The medicine had been prescribed for your patient by another physician?
tD O 35 36
O O 38 39
O O 41 42
68 69 70
O O C3 71 72 73
74 75 76
Yes No
77 78
Yes No O
79 80
Underreporting of adverse drug reactions 2 6 1
The patient had purchased the medicine (without ~ O prescription) themselves 81 82
8. What would yon understand by the following expressions of risk that are used to describe the frequency of ADRs in text books and prescribing literature?
Incidence Incidence Incidence Incidence Incidence Expression 1 in 10 1 in 100 I in 1,000 1 in 10,000 1 in 100,000
patients patients patients patients patients
'Occasional' tD O ~ O 83 84 85 86 87
'Rare' O I:l O ~ Ill 88 89 90 91 92
'Common' 171 O 0 ~ 0 93 94 95 96 97
'Very rare' O 0 ~ ~ 0 98 99 lO0 lO1 102
9. What is your age? O O 103 104
10. Are you principally based in:
General practice (primary health care)
Specialist or hospital practice
Other (please specify)
11. Are you currently engaged in medical practice involving the prescribing of medicines?
12. If you are a GP, do you have a GMS list?
O 105
O 106
D 107
Yes O
108
Yes tD
110
No O
109
No O
1ll
Many thanks for your help and co-operation.