Embed Size (px)
Citation preview

Undergraduate surgical teaching utilizing telemedicine
Y A Gul, A C T Wan & A Darzi
Objectives To evaluate the concept of a new telemedi-
cine orientated educational application by exposing
junior medical students to surgical teaching via video-
conferencing from the operating theatre and comparing
this to the traditional method currently employed,
which requires the presence of students in the operating
room. To determine student satisfaction with this novel
method and identify de®ciencies associated with tradi-
tional surgical teaching.
Design Students were connected by video-conferencing
equipment 2 Mbit/s permanent virtual circuits that
provided two-way picture and voice communication.
Traditional tutoring involved students attending the
operating theatre in set numbers. Video recordings
were made during the telemedicine transmission for
highlighting important factors relevant to the operative
procedure. A questionnaire was used to assess the
quality of time spent and information obtained by the
students.
Setting Telemedicine centre and operating theatre, St
Mary's Hospital, London.
Subjects Junior clinical students.
Results The median score for surgical teaching utilizing
videoconferencing was 9 (scale 0±10) compared to 5 for
traditional operating theatre surgical teaching. All 46
(100%) subjects indicated a willingness to return for
the telemedicine in¯uenced method of tutoring com-
pared to 65% of students exposed to the conventional
method.
Conclusions Our early experience with telemedicine as-
sisted surgical teaching indicate high acceptance and
satisfaction rates by clinical students. Further studies to
evaluate the objective gain in knowledge associated with
this method is required prior to its implementation in
any future medical curriculum.
Keywords Consumer satisfaction; education, medical,
undergraduate, *methods; students, medicical, psy-
chology; surgery, *education.
Medical Education 1999;33:596±599
Introduction
Medical teaching has recently undergone changes, with
continuing reforms looming on the horizon in recog-
nition of the need for a new and modern structured
educational programme. A signi®cant drive related to
this phenomenon is largely attributable to develop-
ments in information technology, which is capable of
improving upon the antiquated methods that are still
being employed in certain academic institutions.
Telemedicine encompasses a whole spectrum of
medical activities and has great potential for improving
health care delivery, including medical education.1
There has already been a number of established projects
in distance education for doctors at undergraduate and
postgraduate level. Novel teaching techniques are,
however, required to overcome the `passive viewer'
syndrome that may be associated with this system.2 We
assessed telemedicine as a teaching method for under-
graduate medical students undergoing their surgical at-
tachment by utilizing this alternative process. The main
purpose of the study was to evaluate student satisfaction
with telemedicine teaching via surgical video-
conferencing from the operating theatre and comparing
it to the established method of operating theatre surgical
teaching. An attempt was also made to identify
de®ciencies in the traditional method employed.
Subjects and methods
Undergraduate medical students in their ®rst clinical
year with no previous exposure to hospital medicine
Minimal Access Surgical Unit, Imperial College School of Medicine
and St Mary's Hospital, London, UK
Correspondence: Professor Ara Darzi, Minimal Access Surgical Unit,
4th Floor, Stanford Wing, St Mary's Hospital, Paddington, London
W2 1NY, UK
Clinical skills
596 Ó Blackwell Science Ltd MEDICAL EDUCATION 1999;33:596±599

were selected randomly to participate in the study over
a 10-week period from October to December 1997. All
46 students were attached to a general surgical ®rm at a
teaching hospital in London. Teaching venues were at
the general surgical operating theatres and the tele-
medicine centre. Conventional teaching consisted of
students (up to six at any theatre session), attending the
operating theatre during surgical procedures. Teaching
utilizing telemedicine involved up to 12 students at-
tending the telemedicine centre and viewing surgical
procedures transmitted from the operating theatre
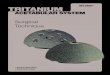
using compressed digital video signals which are con-
verted by a codec. The video network is based on 2
Mbit/s permanent virtual circuits which allows for two-
way visual transmission (625 picture lines at 25 frames
per second) and audio interaction (Fig. 1). Views ob-
tained from the operating theatre were either from an
external wall-mounted or hand-held camera which was
balanced on a tripod. Endoscopic images were trans-
mitted in the case of laparoscopic and other minimally
invasive procedures. An endoscopic camera was used to
provide a view of the internal body cavity during open
surgery whenever necessary.
The surgical procedures demonstrated included
laparoscopic cholecystectomies, inguinal hernia re-
pairs, haemorrhoidectomies and breast surgery (mas-
tectomy and axillary clearance). Operative procedures
were performed by either a consultant or senior
specialist registrar. A moderator of the grade of a
specialist registrar was present at the telemedicine
centre, conducting a short lecture prior to each op-
erative procedure. This also ensured a reduction of
unnecessary interruptions involving the operating
team, as the moderator attempted to answer some of
the questions raised by the students during the tele-
conferencing sessions.
The students participating in the study were given a
self-administered questionnaire after each teaching
session. Questions pertaining to their satisfaction and
the perceived educational value of the time spent in
theatre and the telemedicine centre were evaluated.
Items on the questionnaire were rated on a four-point
scale: 1 (poor) to 4 (excellent). Informed consent was
obtained from all the patients who were briefed fully on
the teaching methods employed.
Results
All 46 students returned the questionnaire. Students'
interpretation of telemedicine and traditional operative
surgery teaching is summarized in Tables 1 and 2. More
than 90% of students who attended the telemedicine
teaching found the audiovisual cues to be exceptional,
with all procedures clearly seen and demonstrated. Views
obtained of the surgical procedure by those who attended
the operating theatre session was considered to be poor
by 41%. Quality of tutoring was graded excellent by 96%
of the students attending the telemedicine sessions
compared with only 50% of those exposed to traditional
operating theatre teaching. Over 30% of students felt
that they were either in the way of the theatre staff or not
welcomed during their time spent in theatre.
Sixty-three per cent of students felt that valuable time
was wasted during their presence in the operating the-
atre and that 38% of time spent in theatre was squan-
dered from the learning perspective. All 46 students
Figure 1 Diagrammatic representation of telemedicine teaching from the operating theatre
Ó Blackwell Science Ltd MEDICAL EDUCATION 1999;33:596±599
Undergraduate surgical teaching · Y A Gul et al. 597

who completed the evaluation forms indicated that they
would return for similar teaching experience with tele-
medicine in¯uenced methods compared with 65% of
those who attended the operating theatre venue. Ad-
ditional positive feedback regarding the video-
conferencing method was obtained from 27 students,
who commented favourably on the interaction they had
with the operating surgeon. On a scale of 0 (worst) to
10 (best), the students surveyed gave a median score of
5 for operating theatre teaching and a rating of 9 for the
newly implemented surgical teaching. The mean period
of tutoring was 138 min (range: 120±146 min) for
telemedicine sessions and 216 min (range: 126±
326 min) for attendance at the operating theatre.
Discussion
Constraints with time and resources may have a signi®-
cant impact on the availability of clinical staff for teach-
ing. The resulting reduction in the quality and quantity of
tutoring may have a detrimental effect on our healthcare
system. The use of telecommunications in the provision
of educational services is well established and telemedi-
cine assisted teaching has been found to generate a high
level of interest from students.3
Teaching of surgery commonly relies on the use of
several media including the use of videos. The routine
attendance of medical students at the operating theatre
during their surgical attachments can be of variable ed-
ucational value. Low or infrequent levels of interaction
between medical students and the operating team is
commonplace and the random nature of this important
exercise in the undergraduate medical training pro-
gramme may have a signi®cant impact in their under-
standing of basic surgery. The frequent comment made
by clinical students of `too much time spent in theatre
with too many people around' and `not being able to see
anything' has been observed in an earlier study.4
Even though previous studies have questioned the ef-
fectiveness of teleconferencing in conducting tasks such
as information exchange and problem-solving, this form
of media is beginning to show signs of replacing routine
`face-to-face' meetings.5 We assessed videoconferencing
from the operating theatre as a complementary method
of tutoring in the discipline of surgery to determine if this
would improve the quality of surgical teaching. The
successful implementation of surgical videoconferencing
during courses held for postgraduate surgical teaching
was a driving force in conducting the study.
Our results indicate students' preference for surgical
teaching at the telemedicine centre, which involved
demonstration of live surgery rather than traditional
attendance at the theatre venue. The students' ques-
tionnaire used in this study did not measure actual gain
in knowledge, but rather their impressions of the ben-
e®t obtained and how much they had learnt. We do not
envisage this mode of teaching as a barrier to students
Table 1 Student evaluation of teaching utilizing surgical videoconferencing and traditional operating theatre attendance
Videoconferencing Operating theatre
*4 3 2 1 4 3 2 1
Clarity of procedure 42 (91) 3 (7) 1 (2) ± 17 (37) 5 (11) 5 (11) 19 (41)
Ability to ask questions freely 40 (87) 4 (9) 2 (4) ± 25 (54) 4 (9) 4 (9) 13 (28)
Quality of time spent learning 44 (96) 2 (4) ± ± 23 (50) 5 (11) 12(26) 6 (13)
Sound quality 44 (96) 2 (4) ± ± ± ± ± ±
Willingness to return for similar 100 65
teaching experience (%)
Mean overall time (%) 0 38
deemed wasted
Median score (0±10) 9 5
*Rating (4 excellent, 3 good, 2 satisfactory, 1 poor) Value in parantheses are percentages.
Table 2 Medical students' perception of operating theatre
teaching environment
Yes No Occasionally
Impression of obstructing
theatre staff
19 (41%) 11 (24%) 16 (35%)
Made to feel unwelcome
during time spent in theatre
15 (33%) 25 (54%) 6 (13%)
Time squandered while in
theatre
29 (63%) 11 (24%) 6 (13%)
Undergraduate surgical teaching · Y A Gul et al.598
Ó Blackwell Science Ltd MEDICAL EDUCATION 1999;33:596±599

attending the operating rooms. In fact, we emphasize
the importance of exposing medical students to the
operating theatre environment, especially when they are
allowed to assist and, therefore, participate closely in
the operative procedure. This is, however, only feasible
when operating during emergency hours or when there
is a low ratio or number of students attached to a sur-
gical ®rm. The latter is unfortunately not frequently
observed, especially in a teaching hospital. From the
students' perspective, a greater degree of interactive
discussion is possible with the telemedicine method
employed in our study. A possible explanation for this
®nding is probably related to the fact that the students
exhibit a lesser degree of inhibition when tutored in this
less hostile environment.
The costs of providing such a service in our institution
was limited by the already available video technology
network in place, which we utilize to conduct postgrad-
uate courses on a regular basis. Data are transmitted at
2 Mbit/s using this technology, which is ®ve times higher
than that used in standard commercial 384 kbit/s vid-
eoconferencing systems. This, however, could have
considerable implications for institutions that do not
provide such a service. Costs related to the requirements
for additional manpower in the form of audiovisual
technicians will also need to be considered if telemedi-
cine teaching sessions are held regularly. We found the
presence of a moderator necessary in minimizing com-
munications between the telemedicine centre and the
operating theatre. The moderator was also involved in
conducting a short lecture, discussing the relevant
pathophysiology and clinical aspects associated with the
operative procedure. This could be viewed as one of the
major differences in the methods compared. The pres-
ence of a similar lecturer in the operating theatre was
explored prior to commencing the study, but this was
dismissed by the operating surgeons due to the perceived
interruptions and disturbance caused by the increased
number of people in the operating room. There is no
doubt that teaching via live surgical videoconferencing
enables a greater number of students to be tutored which
could, theoretically, balance the need for separate lec-
tures on the relevant topics that are being demonstrated
and therefore sustain the manpower required to provide
such an educational service. Patient turnover time be-
tween cases probably accounts for the longer mean pe-
riod of tutoring in the operating theatre in this study.
Even though the operating surgeon or his assistant may
utilize this time to teach students, this may not always be
feasible.
It may be argued that video playback can be as ef-
fective as surgical videoconferencing to demonstrate
similar surgical procedures. The need for extensive
video editing, which can be time-consuming, may be an
essential prerequisite in utilizing this media as a
teaching aid. We feel that demonstrating surgical pro-
cedures utilizing video playback are best performed by
the operating surgeon, as the content is frequently de-
pendent on interpreting edited footage of the proce-
dure, which may be dif®cult. A comparative study is
required to con®rm the effectiveness of this media vs.
videoconferencing as a surgical teaching aid.
Students' opinions of their studies at medical school
could be used to modify educational structures and
improve upon the traditional curriculum. The students'
perception of the proportion of time they spent learning
while in theatre was low in this pilot study. We feel that
surgical teaching via videoconferencing from the oper-
ating theatre can be employed as a useful adjunct to
conventional teaching for medical students on their
surgical rotation. Acceptability of this method of tu-
toring was encouragingly high among the undergradu-
ate students, who also found it preferable to traditional
operating theatre attendance. The medical undergrad-
uates particularly enjoyed the communication they had
with the operative surgeon and the interactive nature of
the discussion that took place during the video-
conferencing teaching sessions. It would require a
greater number of subjects and objective methods of
assessment before a ®rm conclusion can be made about
the bene®t of this new method of undergraduate
teaching. Other forms of telemedicine orientated
teaching techniques, such as in the outpatient setting,
could be implemented selectively in other clinical
specialities allowing for useful dispersion of medical
information to the bene®t of undergraduate and post-
graduate students.
References
1 Wootton R. Telemedicine: the current state of the art. Minim
Invasive Ther Allied Tech 1997;5:393±403.
2 Jameson DG, O'Hanlon P, Buckton S, Hobsley M. Broadband
telemedicine: teaching on the information superhighway.
J Telemed Telecare 1995;1:111±16.
3 Gschwendtner A, Netzer T, Mairinger B, Mairinger T. What
do students think about telemedicine? J Telemed Telecare
1997;3:169±71.
4 Lockwood DNJ, Goldman LH, McManus IC. Surgical dress-
ers: the theatre experience of junior clinical students. Med Educ
1986;20:216±21.
5 Williams E. Face to face and mediated communication. Psychol
Bull 1977;84:963±76.
Received 26 June 1998; editorial comments to authors 6 August 1998;
accepted for publication 17 September 1998
Undergraduate surgical teaching · Y A Gul et al. 599
Ó Blackwell Science Ltd MEDICAL EDUCATION 1999;33:596±599